
Abstract
Background:
Stereotactic radiosurgery (SRS) is the standard of care for patients with a limited number of brain metastases. Despite the fact that the seminal studies regarding SRS for brain metastases were largely tissue agnostic, several current national guidelines do not uniformly recommend SRS in thyroid cancer. We therefore investigated oncological outcomes in a cohort of patients with brain metastases from thyroid cancer who received radiotherapy (RT) at our institution as well as those in a nationally representative cancer cohort, the National Cancer Database (NCDB).
Materials and Methods:
We identified patients with thyroid cancer and brain metastases treated with RT at our institution from 2002 through 2020. For the NCDB cohort, the national database of patients with thyroid cancer was screened on the basis of brain-directed RT or brain metastases. For the institutional cohort, the cumulative risk of local failure (LF), distant intracranial failure, and radiation necrosis were calculated, adjusted for the competing risk of death. Overall survival (OS) in both cohorts was analyzed using the Kaplan–Meier method. Univariate analysis was accomplished via clustered competing risks regression.
Results:
For the institutional cohort, we identified 33 patients with 212 treated brain metastases. OS was 6.6 months. The 1-year cumulative incidences of LF and distant intracranial failures were 7.0% and 38%, respectively. The 1-year risk of radiation necrosis was 3.3%. In the NCDB cohort, there were 289 patients, and the median survival was 10.2 months. NCDB national practice patterns analysis showed an increasing use of SRS over time in both the entire cohort and the subset of anaplastic patients. Univariate analysis was performed for OS, risk of LF, risk of regional intracranial failure, and risk of radiation necrosis.
Conclusions:
SRS is a safe, effective, and increasingly utilized treatment for thyroid cancer brain metastases of any histology and should be the standard of care treatment.
Introduction
Thyroid cancer is the 12th most common cancer, accounting for an estimated 44,280 new cases in 2021 (1). Generally, thyroid cancer is associated with an excellent prognosis, with a 5-year overall survival (OS) estimated at 98% (1). Owing to this generally favorable biology, brain metastases are a relatively rare event in thyroid cancer, estimated to occur in 1–2% of cases (2,3). Consequently, there is a paucity of data regarding the management of brain metastases from thyroid cancer.
Radiotherapy (RT) approaches, including stereotactic radiosurgery (SRS), have emerged as standard of care treatments in patients with brain metastases (4 –7). Importantly, SRS has been associated with excellent local control in treating limited number of brain metastases (4 –7). Although thyroid cancer patients were eligible for randomized clinical trials, which established a role for SRS for brain metastases, the applicability of these data to thyroid cancer patients remains an open question (4 –7). Additionally, although there are several small retrospective studies reporting outcomes for thyroid cancer brain metastases, these studies are limited by several factors including small numbers of patients, absence of reported local control rates, and the lack of inclusion of anaplastic histology (3,8 –11). Consequently, there is no clear consensus in national guidelines regarding the management of these patients. While the American Thyroid Association (ATA) Guidelines generally favor SRS, the National Comprehensive Cancer Network (NCCN) guidelines currently do not support such a universal role for SRS in thyroid cancer brain metastases, specifically in treatment of anaplastic tumors (12 –14).
To address this knowledge gap, the current study represents the largest patient cohort of thyroid cancer brain metastases to include anaplastic histology and sought to test the hypothesis that RT was an effective modality in this patient population using both institutional data and registry data from the National Cancer Database (NCDB). Additionally, utilization of per-lesional analysis has allowed for a robust local control analysis and treatment outcomes.
Materials and Methods
Institutional patient cohort
In this institutional review board-approved retrospective study, we reviewed the records of patients with thyroid cancer brain metastases treated at our institution with RT from 2002 through 2020. Patients were identified using the STARR Cohort Discovery Tool, which has been described previously (15), using thyroid cancer diagnosis codes (a denominator of 7885 patients with thyroid cancer) and search terms for SRS and whole brain radiotherapy (WBRT) (16). Patient charts were then exported from the STARR interface, and charts were manually reviewed and screened for having received RT directed to brain metastases. Demographic data, Karnofsky performance status (KPS), recursive partitioning analysis (RPA) class, and data on additional cancer-directed treatments were obtained for each patient. Data on lesions and SRS planning characteristics were obtained from the electronic medical record. Planning target volume was defined as the actual radiation target volume (in patients who received SRS) and as calculated metastasis volume (in patients who received WBRT).
NCDB patient cohort
For the NCDB cohort, we obtained the Participant User File (PUF) for patients with thyroid cancer (total of 453,778 patients) and then screened by patients who had brain metastases at diagnosis (METS_AT_DX_BRAIN coded 1) and/or who received brain-directed RT (PHASE_I_RT_VOLUME, PHASE_II_RT_VOLUME, PHASE_III_RT_VOLUME coded as 12 or 13). Of note, METS_AT_DX_BRAIN was available in the database starting in 2016. SRS was defined as PHASE_(I, II or III)_BEAM_TECH coded as 6–8, with any other brain-directed RT modality referred to as Brain radiation. The NCDB is a joint project of the Commission on Cancer of the American College of Surgeons and the American Cancer Society. The data used in the study are derived from a de-identified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the investigator. The PUF for thyroid cancer was obtained from the NCDB (for patients diagnosed from 2004 to 2017) in accordance with all institutional and organizational regulations.
Outcome measures and statistical analyses
This study was conducted in compliance with the STROBE criteria (17). The NCDB data were processed in SAS, and then, all analyses for both cohorts were conducted using R studio and Prism.
For both institutional and NCDB cohorts, OS was calculated from the date of RT to the date of death or censoring at last clinical follow-up and analyzed with the Kaplan–Meier and Cox proportional hazard methods. The median follow-up was calculated using the inverse Kaplan–Meier method (18 –20). We assessed if the following variables were prognostic for OS: anaplastic histology, single fraction equivalent dose, and systemic therapy. For the NCDB cohort, trends in practice patterns over time were analyzed using the Mann–Kendall nonparametric test (21).
For the institutional cohort (the following data were unavailable for the NCDB cohort), local failure (LF) was defined as evidence of radiographic progression in the radiation target (planning target volume). Distant intracranial failure was defined as new parenchymal tumor and/or leptomeningeal disease (22). For the neurological death endpoint (as described previously), a determination of the cause of death for each patient was attempted. For the death to be considered neurological, patients had to (a) have died with stable systemic disease with progressive neurological dysfunction, (b) died of intercurrent illness with neurological disability, or (c) those who had rapidly progressive systemic disease and loss of neurological function. Radiation necrosis was determined as described previously (22).
Time to LF, distant intracranial failure, and radiation necrosis were measured from date of RT and calculated with competing risk analysis with death as a competing risk, censored at the last imaging follow-up (R package, “crrSC”). Data were analyzed per lesion (LF and necrosis endpoints), per course of radiation (regional intracranial failure endpoint), and per patient (OS endpoint). Competing risk regression was performed with variables with alpha equal to 0.05 on univariate analysis clustered by patient to account for patients who were treated for multiple lesions (23). Univariate analysis was performed for the following endpoints: OS, LF, regional failure (RF), and risk of radiation necrosis. For these endpoints, increased hazard ratio (HR) refers to increased mortality, failure rate, or rate of necrosis, depending on the endpoint. Variables included in this analysis were number of metastases, systemic therapy, prior craniotomy, anaplastic histology, BRAFV600E status, single fraction equivalent dose, and late (>1 year) diagnosis of brain metastases after initial diagnosis.
Missing data were handled by using complete case analysis. For the institutional cohort, 1 patient had no available follow-up, cavity status was unknown for 3 patients who received WBRT, and BRAF mutation status was missing for 14 patients. For the NCDB cohort, 65 patients had no available follow-up and brain RT dose was missing for 68 patients who received such radiation, and 8 patients were missing systemic therapy data. Patients were censored at last follow-up.
Results
Patient, tumor, and treatment characteristics
Detailed demographic data for the institutional cohort are outlined in Table 1. The cohort consisted of 33 patients (including 8 with anaplastic cancer) with 212 treated brain metastases. The median age of the cohort was 71 years old and 64% were female. Seventy-six percent of patients were white, 12% were Latino, and 3% were Asian. One hundred sixty-eight (83%) lesions were of differentiated histology; the remainder were anaplastic histology. 29.4% of patients were positive for BRAFV600E mutation. Five patients received WBRT, while 28 patients received SRS (single fraction equivalent dose 22 Gy, interquartile [IQ] range 20–22 Gy). Patients receiving SRS or WBRT did not differ in terms of RPA (2.2 vs. 2.0, respectively, p = 0.41) or KPS (76 vs. 80, respectively, p = 0.53). The median number of lesions for patients receiving WBRT was 15 (compared with 2 for SRS). The median size of treated metastases across all modalities was 0.33 cc (IQ range 0.069–2.16). Twenty-six (78.8%) patients received radioactive iodine and 19 (57.6%) received another form of systemic therapy.
Institutional Cohort Demographic and Treatment Data
RAI, radioactive iodine treatment; SRS, stereotactic radiosurgery; WBRT, whole brain radiotherapy.
For the NCDB cohort, we identified a cohort of 289 patients (Table 2). The median age was 63 years (range 19–90 years), and 56% were female. Sixty-nine percent of patients were white, 14% were black, and 11% were Latino. Seventeen percent were treated with SRS, 55.0% were treated with other brain-directed RT, and 28.4% were treated with no brain-directed RT. The most common histologies included papillary (46%) and anaplastic (15%).
National Cancer Database Cohort Demographic and Treatment Data
RT, radiotherapy.
Overall survival
The median follow-up among survivors of the institutional cohort was 32.3 months. In this cohort, the median survival was 6.6 months. Patients with anaplastic thyroid cancer had a trend to worse survival, with median survival of 3.6 months, while patients with differentiated thyroid cancer had a median survival of 10.7 months (p = 0.06) (Fig. 1). Additionally, patients treated with SRS had a longer median survival of 10.7 months than the 1.8 months observed in patients who received WBRT (p < 0.001) (Fig. 1), although the number of patients who received WBRT was small (five).
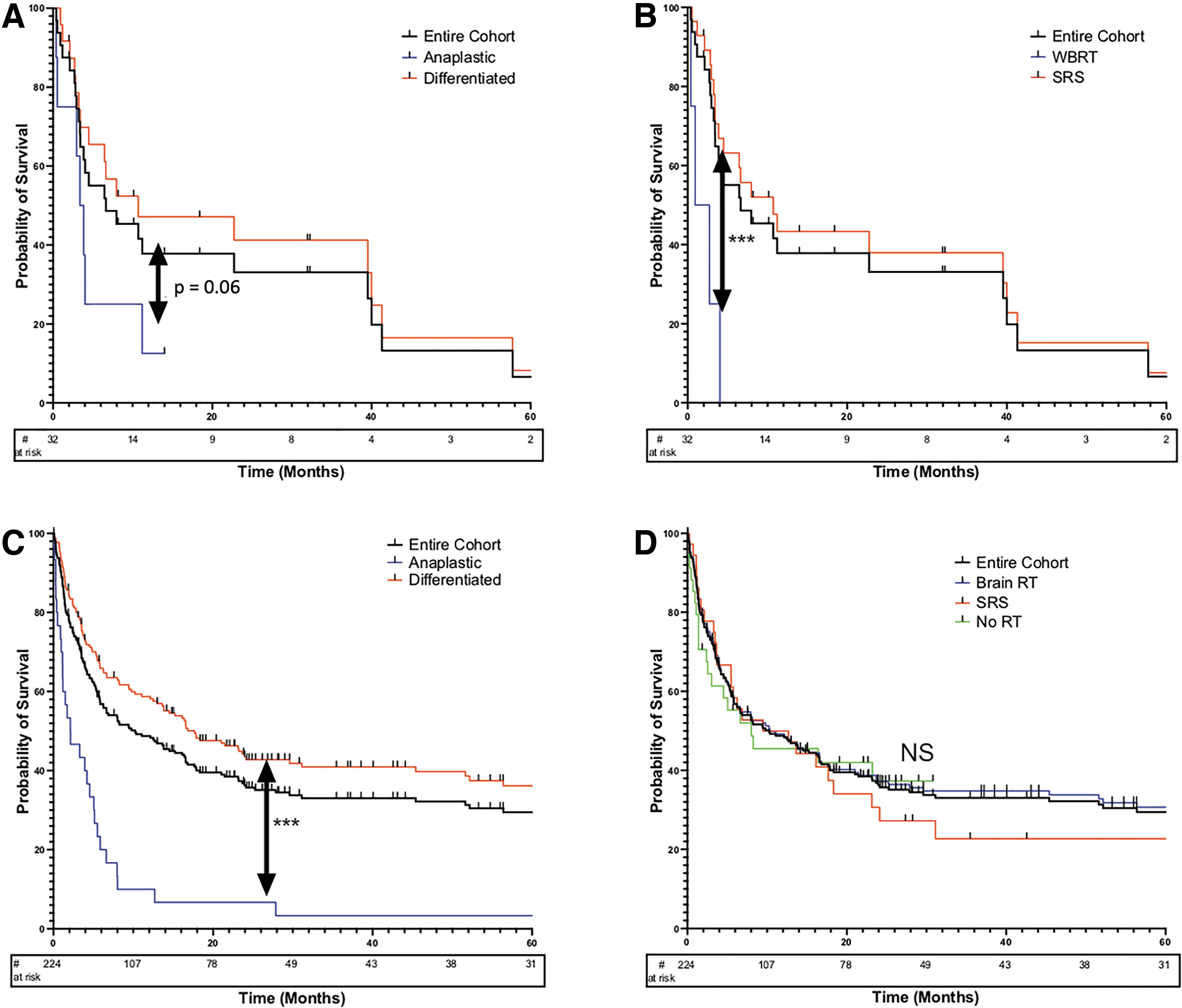
Overall survival. (
In the NCDB cohort, the median follow-up among survivors was 53.3 months, and the median survival was 10.2 months. Anaplastic histology was again associated with worse OS of 2.1 months compared with 17.7 months in patients with differentiated disease (p ≤ 0.001) (Fig. 1). In the NCDB cohort, SRS modality was not significantly associated with improved OS (p = 0.73) (Fig. 1). Kaplan–Meier for anaplastic cancer stratified by treatment modality was analyzed on an exploratory observational basis, which showed no difference in OS between the groups (Supplementary Fig. S1).
Intracranial failure, radiation necrosis, and neurological death (institutional cohort)
The 1-year cumulative incidence of LF and distant intracranial failure for the entire institutional cohort (including WBRT and SRS patients) was 6.5% [95% confidence interval, CI, 3.8–9.2] and 36.8% [CI 16.6–57], respectively (Fig. 2). In patients with differentiated thyroid cancer, the 1-year cumulative incidence of LF and distant intracranial failure was 6.8% [CI 3.6–10.0] and 38% [CI 13.6–62.4], respectively. The 1-year cumulative incidence of LF and distant intracranial failure for anaplastic tumors was 6.4% [CI 0–30.5] and 17.9% [CI 0–100], respectively. Two patients in the cohort had leptomeningeal disease; one patient had a small number of nodular dural deposits, which were the targets for SRS treatment while another SRS patient with prior craniotomy developed nodular meningeal disease at 44 weeks post-treatment.
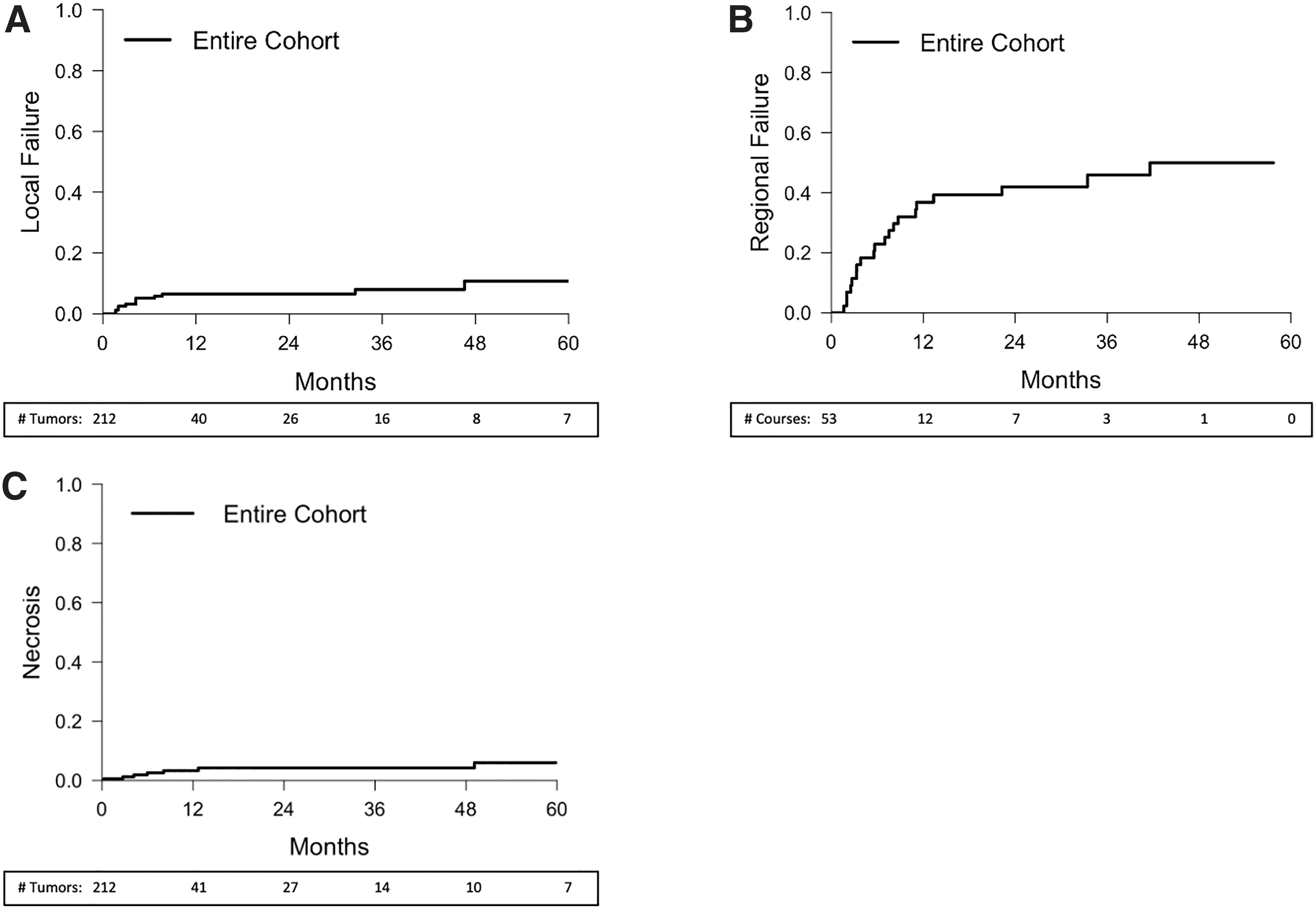
Institutional cohort: cumulative incidence curves. (
The 1-year cumulative incidence of radiation necrosis for the entire cohort on a treated-lesion basis was 3.3% ([CI 0–23.2]; Fig. 2), which were all observed in the SRS subset of patients. Most were grade 2 (57%); 3 (43%) were grade 4 (there were no grade 1 or 3 events). Neurological death was observed in 6 (18%) patients, representing 24% of total deaths. Of these 5 were observed in the SRS subset (of 28 total patients) and 1 in the WBRT subset (of 5 total patients).
Factors associated with outcome
For the institutional cohort, anaplastic histology (HR = 2.49 [CI 1.02–6.09], p = 0.046) and increasing number of metastases (HR per 1 metastasis increase = 1.1 [CI 1.01–1.11], p = 0.012) were associated with worse OS (Table 3). For LF, patients with prior resection (cavity SRS) had an increased risk of LF (HR = 4.7 [CI 1.3–17], p = 0.02) while single fraction equivalent dose (HR per 1 Gy = 0.81 [CI 0.75–0.88], p < 0.001) and number of metastasis in the same treatment course as the index lesion (HR = 0.87 [CI 0.78–0.98]) were associated with lower risk of LF. For RF, increasing planning target volume (HR per 1 cc increase = 1.01 [CI 1.0–1.02], p = 0.006) was associated with increased RF. Number of treated metastases in the same treatment course as the index lesion was associated with decreased risk of radiation necrosis (HR = 0.88 [CI 0.78–0.98], p = 0.02).
Univariate Analysis
Analyses are shown for various variables alpha threshold = 0.05, specifically for LF (per lesion), regional intracranial failure (per course), radiation necrosis (per lesion), and overall survival (per patient). For these endpoints, increased HR refers to increased mortality, failure rate, or rate of necrosis, depending on the endpoint.
Late CNS diagnosis defined as diagnosis of brain metastases >1 year after initial diagnosis of cancer.
CI, 95% confidence interval; CNS, central nervous system; Gy, Gray; HR, hazard ratio; LF, local failure; NCDB, National Cancer Database; OS, overall survival; RF, regional failure.
For the NCDB cohort, anaplastic histology (HR = 3.52 [CI 2.2–5.5], p < 0.001) and systemic therapy (HR = 2.1 [CI 1.6–2.9], p < 0.001) were associated with worse OS while single fraction equivalent dose (HR per 1 Gy increase = 0.97 [CI 0.934–1.0], p = 0.018) was associated with improved OS (Table 3).
National practice patterns
To determine if practice patterns changed over the course of our study period, we analyzed the practice patterns of SRS use as well as Brain RT over time. On the level of the entire cohort, we observed a significant increase in SRS use over time (tau = 0.734; p = 0.000532), but there was no such trend for Brain RT (tau = 0.271; p = 0.204). Next, we similarly looked at practice pattern trends in the management of the subset of patients with anaplastic thyroid cancer. Given that this represented a much smaller subset of patients, we conducted an exploratory one-sided analysis to determine if the anaplastic cohort exhibited a similar increase in RT modality utilization as was observed in the entire cohort analysis. In that context, we observed a significantly increased use of SRS in patients with anaplastic cancer (tau = 0.422; p = 0.0497), but not Brain RT (tau = 0.250; p = 0.174). The practice pattern trends are represented in Supplementary Figure S2.
Discussion
Brain metastases are a rare presentation of this disease, and there is a paucity of data regarding their management, particularly in patients with anaplastic histology. The present study reports both a national database of patients with thyroid cancer as well as our institutional experience in brain metastases from thyroid cancer treated with RT. Together, these cohorts represent a significant number of patients, including a large cohort of those with anaplastic histology, which are understudied in the literature.
The observed OS in the present study was consistent with prior studies and significantly worse in patients with anaplastic histology (3,8 –11). Local and regional intracranial control was comparable to other histologies in our institutional cohort, underscoring the role for RT in treatment of these patients. The toxicity profile was also favorable, with only a small percentage of patients experiencing radiation necrosis, with no grade >3 toxicity. In the institutional cohort, SRS modality exhibited improved OS, although the small number of patients receiving WBRT and possible selection bias limit potential conclusions about survival benefit. Although this OS improvement was not observed in the NCDB cohort, univariate analysis showed that increasing single fraction equivalent dose was correlated with improved survival. However, rather than representing treatment efficacy, these findings likely represent selection biases involving underlying reasons for which patients are treated with SRS versus WBRT.
In addition to dose and modality, anaplastic patients exhibited worse OS in both cohorts, in agreement with the limited published literature for this rare presentation. Increasing number of metastases was associated with worse OS in the institutional cohort. Interestingly, systemic therapy was associated with worse OS in the NCDB cohort, but this may be due to confounding by indication in the same way as discussed above with WBRT versus SRS as patients with worse prognoses may be the ones selected for systemic therapy. Although our patient numbers were too small for robust multivariable or propensity score analyses, it is worth noting that patients receiving SRS and WBRT had similar RPA and KPS scores, suggesting balance between the cohorts in underlying functional status. It is therefore worth noting that due to these biases, our study cannot assess superiority of SRS over WBRT, but rather provides supporting evidence to complement prior tissue agnostic studies, which have established SRS as an acceptable practice standard in brain metastases from any cancer histology (4 –7).
For our institutional cohort, we were able to accomplish clustered univariate regression for LFs and intracranial RFs. We found that increasing single fraction equivalent dose was associated with decreased LFs, suggesting that a dose response exists and thus potentially favoring SRS, which can deliver higher ablative doses than WBRT. Interestingly, increasing number of treated metastases was also associated with decreased LFs, although this finding is perhaps the result of selection bias rather than true tumor biology. Similarly, the poorer LF outcomes associated with cavity SRS may represent similar confounding. Additionally, increasing radiation target volume (also called planning target volume or PTV) was associated with an increased incidence of LF, suggesting a relationship between lesion size and occult metastatic disease. Increasing number of lesions in the same treatment course as the index lesion was associated with reduced incidence of radiation necrosis, likely reflecting a bystander effect of dose or another confounding phenomenon.
To the best of our knowledge, the present report is the largest study of anaplastic patients with brain metastasis in the literature, underscoring the limited evidence that exists for guiding the management of this rare presentation. While SRS has become the standard of care for brain metastases in most situations, it is worth noting that the current NCCN guidelines do not support SRS in managing brain metastases from anaplastic thyroid cancer (12). One concern underlying this decision is the widely held hypothesis that anaplastic brain metastases are more likely to rapidly fail intracranially out of the treatment field as microscopic metastases blossom, therefore putatively favoring WBRT for broader dose coverage. In that context, our observation that anaplastic brain metastases exhibit comparable LF and regional intracranial failure to differentiated tumors is potentially provocative. Although the competing risk of mortality observed was high, these patients still lived long enough to potentially experience neurocognitive side effects of WBRT (which is routinely observed as early as 3–4 months) (24).
Additionally, our exploratory analysis of national practice patterns of anaplastic brain metastasis management showed significantly increased use of SRS in these patients. Taken together, these findings begin to crystallize a role for SRS in anaplastic brain metastases (a rare presentation that makes prospective study unlikely) as a potentially less toxic but oncologically effective modality which is (perhaps not coincidentally) being increasingly used over time. In any case, appropriate management of this rare presentation should be approached with the best interest of the individual patient in mind and as part of a multidisciplinary team with involvement of neurosurgery and radiation oncology expertise, as exemplified by the ATA guidelines (13,14).
Conclusions
The present study provides strong rationale for treatment of thyroid cancer brain metastases with RT, and more specifically with SRS. Leveraging these data and extrapolating from the existing literature on brain metastases in other cancers, SRS should be considered the standard of care for thyroid cancer brain metastases. As advances in systemic therapy continue to improve outcomes in all histologies of thyroid cancer (including anaplastic cancers), the increased utilization of SRS as a standard of care for brain metastases is a forward-looking approach to improve the neurological outcomes in longer term survivors.
Footnotes
Acknowledgments
We would like to acknowledge the two scientific meeting poster presentations and associated abstracts resulting from the present study. This work was made possible by the CyberKnife Stereotactic Radiosurgery Program at Stanford University Hospitals, as well as the NCDB from the American College of Surgeons.
Authors' Contributions
E.B.: Project inception, database construction, data generation and analysis, and article preparation. S.B., D.G., and N.S.: Database construction, data generation and analysis, and article preparation. N.H.: Data analysis and article preparation. A.M., M.B., C.H., and T.C.: Database construction, data analysis, and article preparation. K.D., S.C., S.S., and E.P.: Project oversight and mentorship, data generation and analysis, and article preparation.
Author Disclosure Statement
E.B., S.B., N.H., D.G., A.M., M.B., C.H., T.C., N.S., K.D., S.C., and E.P. have no pertinent disclosures. S.S. is a consultant for Inovio Pharmaceuticals, Inc.; has a speaker honoraria for Zap Surgical, Inc.; has research funding from Novocure, Inc.; and is on the advisory board for Accuray, Inc. There are no other disclosures.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2