
Abstract
Background:
Combination therapy with liothyronine (LT3) and levothyroxine (LT4) is used in patients with persistent symptoms, despite being administered an adequate dose of LT4. LT3 may also be used in some thyroid cancer patients preparing for radioactive iodine therapy. However, there is a controversy regarding the safety of LT3 use, and there has been no definite evidence of long-term safety of LT3 therapy in Asian populations. The aim of this study was to examine the long-term safety of LT3 therapy using the Common Data Model (CDM).
Methods:
We conducted a retrospective multicenter study across four hospital databases encoded in the Observational Medical Outcomes Partnership (OMOP) CDM. LT3 users were defined as those who received an LT3 prescription for at least 90 days (with or without LT4), and their safety outcomes were compared with those in LT4-only users after 1:4 propensity score matching. Safety outcomes included the incidences of osteoporosis, cardiovascular disease, cancer, anxiety disorder, and mood disorder.
Results:
We identified 1434 LT3 users and 3908 LT4-only users. There was a statistically significant difference in the incidence rate of safety outcomes between LT3 users and LT4-only users. The risks of heart failure (incidence rate ratio [IRR] = 1.664, 95% confidence interval [95% CI] 1.002–2.764, p = 0.049) and stroke (IRR = 1.757, CI 1.073–2.877, p = 0.025) were higher in LT3 users than in LT4-only users. When subgroup analysis was performed according to the presence/absence of thyroid cancer history and duration of thyroid hormone replacement, the risk of heart failure was higher in LT3 users with a history of thyroid cancer and those who underwent ≥52 weeks of LT3 therapy. In addition, the risk of stroke was higher in LT3 users without thyroid cancer history and those who underwent ≥52 weeks of LT3 therapy.
Conclusions:
The use of LT3 was associated with increased incidence of heart failure and stroke in patients with a longer duration of LT3 use and history of thyroid cancer. Therefore, clinicians should consider the risk of heart failure and stroke in thyroid cancer patients with long-term use of LT3. These findings require confirmation in other populations.
Introduction
Levothyroxine (LT4) is the standard treatment for thyroid hormone replacement in patients with hypothyroidism, commonly due to autoimmune thyroiditis or post-ablative therapy such as surgical treatment and radioiodine therapy. However, some patients treated with LT4 monotherapy have persistently complained of impaired psychological well-being and hypothyroid symptoms, even though they achieved a normal serum thyrotropin (TSH) level. 1 –3
Patients with LT4 monotherapy have shown stable low-normal triiodothyronine (T3) level and elevated free thyroxine (T4)/free T3 ratio. 4 –6 Therefore, the normalization of TSH in LT4 monotherapy does not always lead to the normalization of T3, and T3 replacement could be useful for hypothyroidism patients with unsatisfactory results. 7
Previous clinical trials of LT4/liothyronine (LT3) combination therapy did not reveal significant superiority, compared with LT4 monotherapy, in managing hypothyroidism symptoms; thus, clinical practice guidelines do not support the routine use of LT4/LT3 combination therapy. 8,9 Despite the lack of evidence on benefits, the prescription of and the interest in LT4/LT3 combination therapy has increased. 10,11 The proportions of physicians in the United States and Europe who considered using LT4/LT3 combination therapy in patients with persistent symptoms have been reported to range from of 18% to 59%. 12 –16 In addition, some reports suggest that patient hypothyroidism satisfaction or preference may be higher for desiccated thyroid extract or LT4/LT3 combination treatment than for LT4 monotherapy. 17,18
Due to the increase in the prescription rate of LT4/LT3 combination therapy, concerns have been raised regarding the long-term safety outcomes of LT3 therapy in heart and bone diseases. However, these outcomes have not been widely studied. Recently, two observational studies reported long-term safety outcomes in LT3 users. 19,20 One study showed no increased risk of cardiovascular disease, atrial fibrillation, and fractures. 19
Interestingly, the incidence of breast cancer was reported to be increased non-significantly in LT3 users. 19 However, the other study showed no increase in the incidence and mortality rates of breast cancer. 20 The use of LT3 was not associated with an increased risk of adverse safety outcomes in the two previous observational studies; however, these studies were conducted in European populations. Therefore, it is difficult to generalize these previous findings to other ethnic groups and races.
In addition, the target serum TSH levels are reportedly lower in patients with a history of thyroid cancer due to TSH suppression. Therefore, there is a need to assess the safety outcomes of LT3 usage according to a history of thyroid cancer.
The aim of this study was to evaluate the association of LT3 treatment with the incidences of osteoporosis, atrial fibrillation, cardiovascular disease, malignant tumors other than thyroid gland, anxiety disorder, and mood disorder, compared with LT4 monotherapy in the Korean population. We also evaluated the incidence of safety outcomes according to the presence/absence of thyroid cancer history.
Materials and Methods
Data sources
We conducted a retrospective study comparing LT3 users with LT4-only users for hypothyroidism treatment, using four hospital data sources encoded in the Observational Medical Outcomes Partnership (OMOP) Common Data Model (CDM) version 5 from the distributed research network of the Observational Health Data Sciences and Informatics (OHDSI) community. 21,22 The data sources are electronic health records from four hospitals located in different regions: Ajou University Hospital (AUMC, 2.7 million; January 1994 to May 2020), Daegu Catholic University Hospital (DCMC, 1.7 million; January 2005 to December 2018), Myongji Hospital (MJH, 0.88 million; September 2003 to August 2021), and Pusan National University Hospital (PNUH, 0.79 million; February 2011 to August 2018).
All records of each hospital were mapped to the OMOP CDM standard vocabulary concepts (drug ingredient or disease condition) and placed in the OMOP CDM schema; the OMOP CDM provides a homogeneous format for health care data and standardization of underlying clinical disease coding systems. The OHDSI network studies are conducted via a federated model, where access to data and statistical testing is run within the firewall of the research partners' infrastructure on de-identified patient information. 21,22 The entire code used to perform this study can be shared in any database in the format of the OMOP CDM to allow analysis by applying the same method used in this study.
Study design
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting a retrospective observational study, with special attention to the propensity score (PS) analysis. 23 We included patients aged older than 18 years receiving thyroid hormone replacement therapy and divided them into two cohort groups according to LT3 use. The target cohort (LT3 users with or without concurrent LT4 use, hereinafter referred to as LT3 users) consisted of patients treated with LT3 (ingredients concept ID: 1505346) or a combination of LT3 and LT4 for at least 90 days, and the reference cohort (LT4-only users) consisted of patients treated with LT4 (ingredients concept ID: 1501700) for at least 90 days and those who had not previously used LT3.
The index date was indicated by the first observed prescription for LT3 or LT4 in the patients. We excluded patients who were pregnant (concept ID: 36803580), those with cardiac arrhythmia (ingredients concept ID: 44784217), and those in whom safety outcomes were identified before the date of treatment initiation from the cohort. Continuous drug exposures are evaluated from the available longitudinal data by considering sequential prescriptions that have fewer than 30 days gap between prescriptions.
Safety outcomes included osteoporosis (including osteoporotic fractures), atrial fibrillation, heart failure, ischemic heart disease, stroke, malignant tumors other than the thyroid gland, breast cancer, anxiety disorder, and mood disorder. Each safety outcome was identified using OMOP CDM standard vocabulary concepts. Details on the safety outcomes, including concept IDs, are provided in Supplementary Table S1. New onset safety outcomes were defined as newly identified safety outcomes or initiation of medication for osteoporosis after the index date. We set the time-at-risk to start on the day the cohort study started and to stop 3650 days from the cohort study start date.
Ethical consideration
This study complies with the principles laid by the Declaration of Helsinki. This study was approved by the Institutional Review Board of PNUH (IRB No. 2102-021-100). Since the data sources were de-identified, the need for informed consent was waived by the board.
Statistical analysis
Statistical analysis of the incidence of safety outcomes was executed using an analysis tool from the OHDSI's ATLAS tool version 2.7.6 (
We used a caliper of 0.2 PS scale and set the 90-day time window for the time bound era covariates in days relative to the cohort index. The preference score distribution is shown in Supplementary Figure S1. Incidence rate ratio (IRR) and 95% confidence interval (95% CI) were calculated. A forest plot was produced to visually assess IRRs and CIs. The analysis was carried out using R version 4.0.5. Negative control outcomes using a data-rich algorithm were applied for measured residual bias due to systematic errors and unmeasured confounders, and these negative outcomes were not considered to be caused by LT3 and LT4 treatment. 25,26 Statistical significance was defined by a p-value of <0.05.
Results
Baseline characteristics and crude analysis
From the four hospital data sources, we identified 1887 LT3 users and 30,303 LT4-only users. More than half of the patients in each group were in their forties (29.0% in LT3 users and 25.5% LT4-only users) to fifties (28.1% in LT3 users and 26.3% in LT4-only users), and most of the patients in each group were females (84.0% in LT3 users and 82.4% in LT4 users). Half of the patients in each group underwent ≥1 year of thyroid hormone replacement (Table 1 and Supplementary Fig. S2).
Baseline Characteristics
LT3, liothyronine; LT4, levothyroxine.
Incidence rate ratio of safety outcomes, comparing LT3 users with LT4-only users
After applying 1:4 PS matching, 1434 LT3 users and 3908 LT4-only users were selected to analyze safety outcomes (Fig. 1 and Supplementary Table S2). The incidence rate (IR) of each safety outcome was calculated as events per 1000 person-years: 8.88 for osteoporosis, 2.12 atrial fibrillation, 3.13 heart failure, 3.65 ischemic heart disease, 3.40 stroke, 5.56 malignant tumors other than those of the thyroid gland, 0.50 breast cancer, 3.80 anxiety disorder, and 4.03 mood disorder among LT3 users.
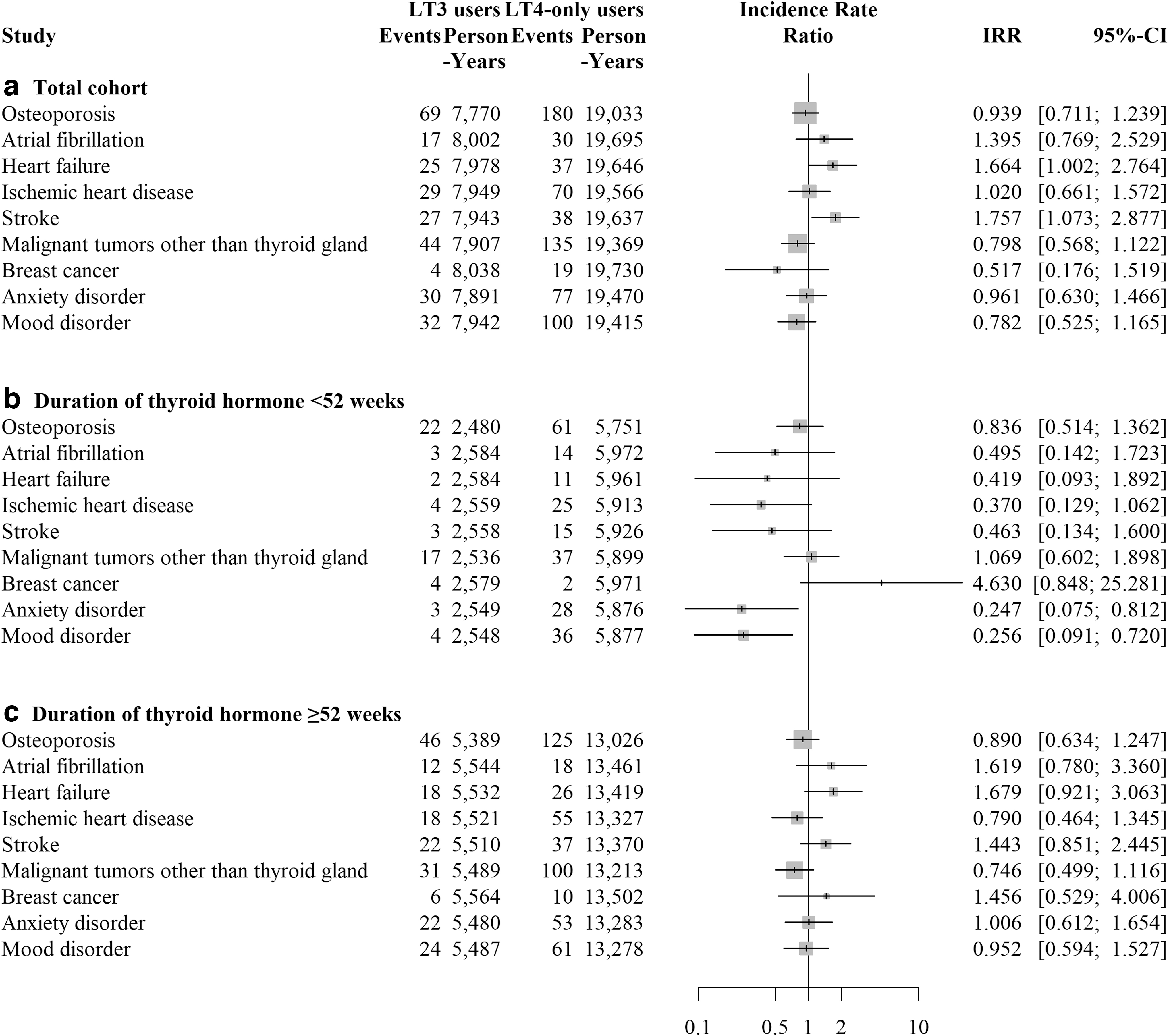
Forest plot, the IRR of safety outcomes. (
There were statistically significant differences between LT3 users and LT4-only users in the IRs of heart failure (IRR [CI] 1.664 [1.002–2.764], p = 0.049) and stroke (IRR [CI] 1.757 [1.073–2.877], p = 0.025). When analyzing according to thyroid hormone replacement duration (≥52 weeks or not), although not significant, the risk of heart failure (IRR [CI] 1.679 [0.921–3.063], p = 0.091) and stroke (IRR [CI] 1.443 [0.851–2.445], p = 0.173) increased in LT3 users compared with LT4-only users when the duration of thyroid hormone replacement was ≥52 weeks. The IRs of anxiety (IRR [CI] 0.247 [0.075–0.812], p = 0.021) and mood disorder (IRR [CI] 0.256 [0.091–0.720], p = 0.010) were significantly lower in LT3 users with a duration of <52 weeks.
IR ratio of safety outcomes according to history of thyroid cancer
The entire cohort was divided into two groups according to the presence/absence of thyroid cancer history. One third of LT3 users (727 patients) had a history of thyroid cancer, and after applying 1:4 PS matching, 457 LT3 users and 1064 LT4-only users were selected in the group of those with a history of thyroid cancer. In the group of those without thyroid cancer history, 924 LT3 users and 2573 LT4-only users were selected after applying 1:4 PS matching.
In the group of those with a history of thyroid cancer, the IRs of safety outcomes were not statistically significantly different, except that of heart failure. The IR of heart failure in LT3 users was higher than that in LT4-only users (2.39 vs. 0.54 per 1000 person-years, IRR [CI] 4.401 [1.101–17.599], p = 0.036). When analyzing according to the duration of thyroid hormone replacement, the IR of heart failure was statistically higher in LT3 users with a duration of ≥52 weeks than in LT4-only users (3.48 vs. 0.63 per 1000 person-years, IRR [CI] 5.551 [1.435–21.465], p = 0.013).
The IR of heart failure was not statistically significantly different between LT3 users and LT4-only users when the duration of thyroid hormone replacement was <52 weeks (IRR [CI] 1.343 [0.027–67.703], p = 0.883). In addition, the risk of mood disorder was higher in LT3 users with a duration of ≥52 weeks (IRR [CI] 2.203 [1.005–4.828], p = 0.049). (Fig. 2 and Supplementary Table S3).

Forest plot, the IRR of safety outcomes in the subgroup with history of thyroid cancer. (
The IR of heart failure in the group without a history of thyroid cancer was not statistically significantly different (3.13 vs. 4.31 per 1000 person-years, IRR [CI] 1.211 [0.656–2.235], p = 0.255). However, the IR of stroke was statistically significantly different between LT3 users and LT4-only users when the duration of thyroid hormone replacement was ≥52 weeks (p = 0.008).
The IR of stroke in LT3 users was 5.37 per 1000 person-years, and IRR [CI] was 2.480 [1.266–4.858]. In addition, the risk of anxiety disorder was lower in LT3 users without a history of thyroid cancer (IRR [CI] 0.461 [0.256–0.833], p = 0.010) (Fig. 3 and Supplementary Table S4).
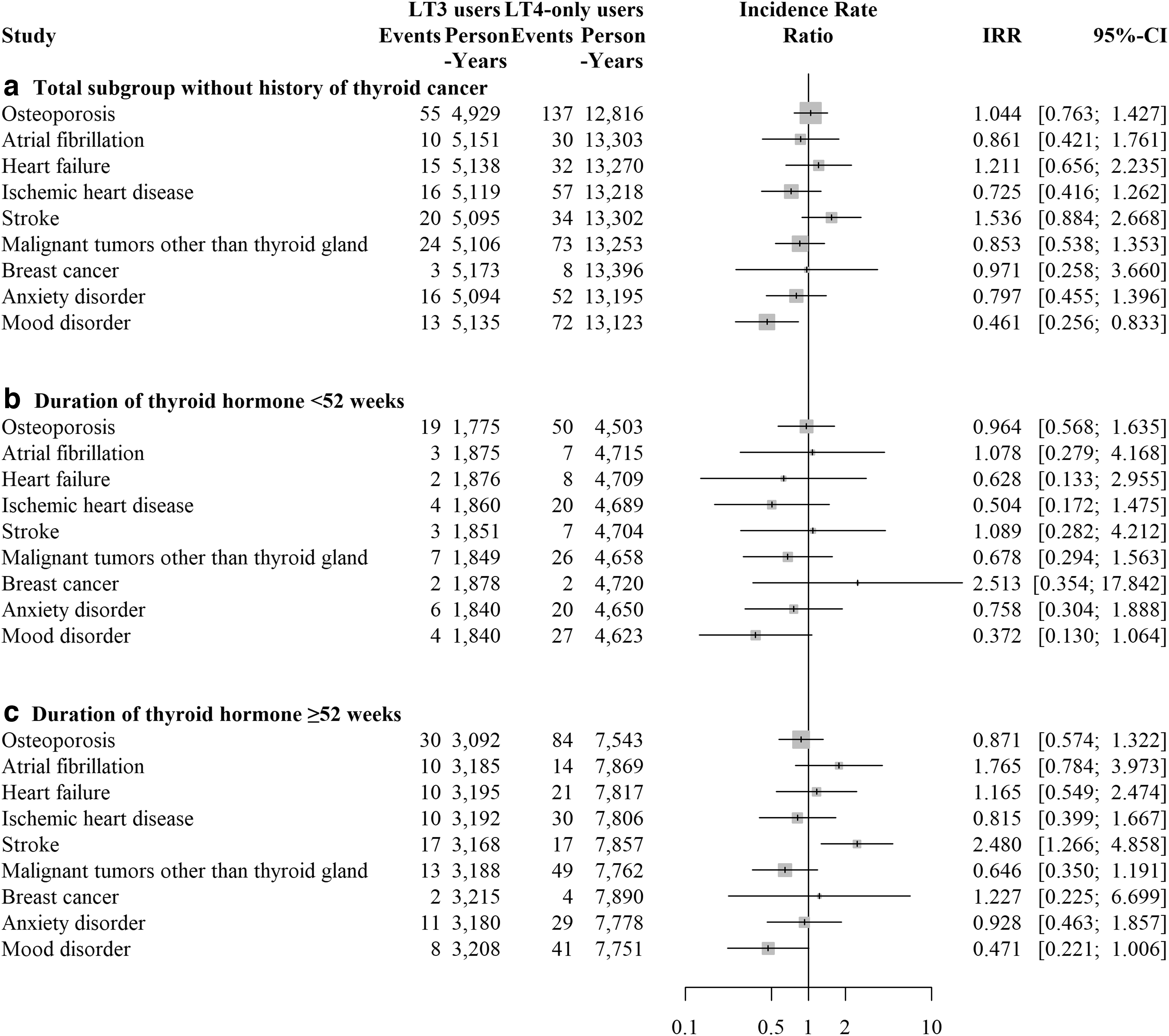
Forest plot, the IRR of safety outcomes in the subgroup without history of thyroid cancer. (
Discussion
In this retrospective multicenter study of a Korean population, there were no statistically significant differences in the IRs of atrial fibrillation, osteoporosis, breast cancer, and malignant neoplasm other than that in the thyroid gland between LT3 users and LT4-only users. However, we found that long-term use of LT3 was associated with increased incidence of heart failure in patients with a history of thyroid cancer and increased incidence of stroke in patients without a history of thyroid cancer.
Thyroid hormones regulate body homeostasis and metabolism, and cardiovascular and musculoskeletal systems are especially sensitive to the change in thyroid hormone levels. 27,28 Excessive level of T3 as a biologically active thyroid hormone causes atrial fibrillation and heart failure through an increase in cardiac contractility and cardiac hypertrophy, and it is associated with reduced bone mass and fragility fractures due to a high bone turnover. 29,30 The safety concerns associated with excessive serum T3 levels are the main issue in LT4/LT3 combination therapy. However, recent observation studies comparing LT3 therapy with LT4 therapy showed that there were no additional risks of atrial fibrillation, cardiovascular disease, osteoporosis, and cancer. 19,20,27
Consistent with previous studies, LT4/LT3 combination therapy lasting less than 52 weeks did not increase the incidence of safety outcomes such as cardiovascular disease, osteoporosis, and any cancer in this study. However, our findings regarding safety outcomes such as heart failure and stroke in long-term LT3 users were different from a previous report of longitudinal safety outcome of LT3 treatment. 19
One possible hypothesis is the effect of LT3 fluctuation. Regarding the pharmacodynamics of LT3, serum T3 levels fluctuate, increasing up to 40% after LT3 administration in patients with LT4/LT3 combination therapy and serum T3 reach a level above normal reference range according to LT3 dose. 31,32 At the serum T3 peak after LT3 administration, patients complained of palpitation and chest tightness, and recent clinical trials have reported minimally increased heart rate and systolic blood pressure in patients who received LT4/LT3 combination therapy. 18,27 Therefore, prolonged transient hypertriiodothyroninemia would occur in LT3 users, and it could result in tachycardia-related effects on cardiac function. Further studies are required to evaluate the effect of T3 fluctuations on cardiovascular disease.
Another potential explanation for the observed increased incidence of heart failure and stroke in LT3 users in our study could be ethnicity. The nationwide epidemiology study in Korea showed higher serum TSH reference levels in the Korean population than in the Western population; thus, a higher dose of LT3 may be required to achieve normalization of serum TSH levels in Korean hypothyroidism patients. 33 In addition, the risk of cardiovascular disease associated with thyroid hormone replacement differed by race and ethnicity.
A recent retrospective study showed different hazard ratios for the incidence of atrial fibrillation and stroke in thyroid hormone replacement therapy according to race and ethnicity. 34 Therefore, the difference in ethnicity of our study population may have contributed to the observed safety outcomes in this study.
The cause of hypothyroidism also affects safety outcomes of LT4/LT3 combination therapy. The IRR of heart failure was significantly different in long-term LT3 users with a history of thyroid cancer, and the IRR of stroke was significantly different in long-term LT3 users without a history of thyroid cancer. For high- or intermediate-risk thyroid cancer patients, recommended target serum TSH levels were lower than the normal value (below 0.5 mIU/L). 35
TSH suppression therapy for thyroid cancer patients leads to a state of subclinical hyperthyroidism and is associated with increased risk of cardiovascular diseases, including atrial fibrillation and heart failure. 36 One observational study showed increased risk of heart disease and decreased risk of cerebrovascular disease in thyroid cancer survivors with but not without TSH suppression. 37
Thus, low serum TSH level caused by TSH suppression therapy may explain the difference in the risk of heart failure and stroke according to the presence/absence of thyroid cancer history. However, due to the nature of the CDM database, we could not analyze the association between the TSH suppression therapy and cardiovascular disease. Further evaluation of the association between long-term LT3 use and cardiovascular disease in thyroid cancer patients would be required.
Previously, the Thyroid Epidemiology, Audit, and Research Study (TEARS) showed an increased prescription of antipsychotics in LT3 users, but mental disorder prevalence was not significantly different between LT3 users and LT3 non-users. 19 In the current study, the risk of mood disorder was higher in long-term LT3 users with a history of thyroid cancer, and LT3 users without a history of thyroid cancer had a lower incidence of mood disorder. LT4/LT3 combination therapy is usually applied in patients with sustained hypothyroidism symptoms despite receiving adequate LT4 therapy; therefore, the diagnosis of mood disorder may increase in LT3 users.
In addition, the diagnosis and treatment of thyroid cancer was associated with an increased risk of mood disorder. 38 A lower incidence of mood disorder in LT3 users without a history of thyroid cancer compared with LT4-only users may be related to improved symptoms of hypothyroidism. However, there were no data on hypothyroidism symptoms in this study; thus, further study is required.
There are some limitations in this study, including its retrospective nature. First, we analyzed safety outcomes using de-identified patient information from the CDM database; therefore, the clinical data of the patients were lacking in this study. 21,22 We excluded previously diagnosed comorbidities such as cardiovascular disease and bone disease, but clinical factors associated with safety outcomes such as age, body mass index, and serum lipid profile could not be considered in this study.
It is also important to consider the limitations of diagnostic accuracy and accurate case identification, as they rely on diagnostic codes for disease identification. Second, our study had no data on LT3 dose, LT3 compliance, and serum thyroid hormone levels. Serum TSH and T3 levels were mainly treated to target in LT3 users, and higher serum T3 levels were associated with increased adverse event in LT3 users. 39 Thus, it is important to consider the relationship between increased safety outcomes and un-identified abnormal thyroid hormone levels.
Finally, heart failure and stroke events were relatively uncommon and multiple statistical analyses were conducted; thus, the possibility of a type 1 error should be considered. There was an increased risk of safety outcomes (heart failure and stroke) in long-term LT3 users; thus, we believe that LT4/LT3 combination therapy should be discontinued when there is no beneficial effect on hypothyroidism symptoms at 6 months of treatment.
In conclusion, LT4/LT3 combination therapy was not associated with increased IRs of atrial fibrillation, osteoporosis, and malignant tumors other than thyroid cancer, compared with LT4 monotherapy. However, the incidence of heart failure and stroke was found to be increased in patients who uses LT3 for a longer duration and those with a history of thyroid cancer. Therefore, clinicians should consider the risk of heart failure and stroke associated with long-term LT3 use, including in patients with LT3 use for a history of thyroid cancer.
Footnotes
Authors' Contributions
W.Y. researched the data and drafted the article; J.K. provided the statistical analysis and edited the article; M.I. and S.R. researched the data; E.H.K. edited the article; Y.K.J., S.S.K., and I.J.K. supervised drafting of the article; and M.K., B.H.K. designed the article. All authors revised the article and approved the final version.
Author Disclosure Statement
No competing interests exist.
Funding Information
This study was supported by Biomedical Research Institute Grant (202100070001), PNUH.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4