
Abstract
Background:
Thyroid autoimmunity (TAI) has a high prevalence among women of reproductive age. Investigating its possible impact on ovarian function and fertility is, thus, of utmost relevance. The aim of this systematic review and meta-analysis was to elucidate the effect of TAI on both assisted reproductive technology (ART) outcomes and ovarian reserve.
Methods:
This systematic review and meta-analysis was restricted to two groups of research articles investigating the association between TAI and: (1) autologous ART outcomes (i.e., fertilization rate [FR], implantation rate, clinical pregnancy rate [CPR], miscarriage rate, and live birth rate), (2) markers of ovarian reserve (i.e., anti-Müllerian hormone, basal follicle stimulating hormone, antral follicle count, and number of oocytes retrieved). Studies including women affected by overt hypo/hyperthyroidism were excluded. Relevant studies were identified by a systematic search in PubMed, MEDLINE, ClinicalTrials.gov, Embase, and Scopus, from database inception to May 1, 2022.
Results:
From a total of 432 identified publications, 22 studies were included in Group 1 and 26 studies in Group 2. The presence of TAI was associated with a higher risk of miscarriage (7606 participants, odds ratio [OR] 1.52, confidence interval [CI 1.14–2.01], p = 0.004, I 2 = 53%), lower chance of embryo implantation (7118 participants, OR 0.72, [CI 0.59–0.88], p = 0.001, I 2 = 36%), and live birth (11417 participants, OR 0.73, [CI 0.56–0.94], p = 0.02, I 2 = 71%). These associations were no longer observed in a subgroup analysis of patients who exclusively underwent intracytoplasmic sperm injection (ICSI). The FR and CPR as well as the mean values of surrogate markers of oocyte quantity appeared not to be affected by TAI.
Conclusions:
This data synthesis suggest a higher risk of adverse ART outcomes in women with positive TAI. However, the reliability of these findings is hampered by the relatively low quality of the evidence and significant heterogeneity in many of the meta-analyses. The possible protective effect of ICSI is promising but should be confirmed in controlled prospective clinical trials.
PROSPERO Registration ID
: CRD42021236529.
Introduction
Ovarian reserve is the number of oocytes that a woman possesses at a particular time in her life and inversely correlates with age. 1 Both follicular atresia and ovulation over time cooperate in determining the slow depletion of the initial pool of non-growing follicles. 1 Ovarian reserve may be evaluated by measuring biochemical (i.e., Anti-Müllerian hormone [AMH], basal follicle stimulating hormone [FSH], estradiol [E2], or inhibin B serum concentration) and ultrasound (i.e., antral follicle count [AFC] and ovarian volume) parameters or by assessing the response to controlled ovarian hyperstimulation (COH) for in vitro fertilization (IVF) (i.e., number of oocytes retrieved [NOR]). 1,2 Serum AMH, which is produced by granulosa cells of gonadotropin-independent early follicles, and AFC are considered the most sensitive and reliable markers of oocyte quantity. 1 However, they have only a weak association with reproductive outcomes such as clinical pregnancy rate (CPR), and live birth rate (LBR). 1
Ovarian senescence is also characterized by a progressive impairment of oocyte quality, which relates to the potential of a fertilized oocyte to result in a live birth. 2 This process determines an ineluctable reduction of fecundity and reproductive potential. 2,3 The extent and speed of the decline in both ovarian reserve and oocyte quality with aging vary among women and mainly depend on genetic characteristics. 2 Importantly, there are other contributing factors. Among these, ovarian surgery certainly plays a role. Evidence from studies investigating the modification in AMH serum concentration after surgical excision of ovarian endometriomas showed a surgery-related damage to ovarian reserve. 4,5 Other authors claimed a role for an autoimmunity-mediated damage. 6 In particular, an association between thyroid autoimmunity (TAI) and diminished ovarian reserve (DOR) has been hypothesized. 7
The available data also suggest a detrimental effect of TAI on oocyte quality. Monteleone et al demonstrated the presence of thyroid antibodies in the follicular fluid of women with TAI. Further, they observed a decreased chance of oocyte fertilization and top-quality embryo development in women with positive TAI compared with negative controls. 7 On this basis, they speculated that the presence of thyroid antibodies within the follicle may damage the maturing oocyte. 8
The impact of thyroid antibodies on the ovarian reserve can be easily assessed by comparing the earlier mentioned surrogate markers between TAI-positive and -negative women. However, investigating their effect on oocyte quality is more challenging. To date, assisted reproductive technology (ART) is considered the most reliable study model since it is well known that oocyte quality considerably influences its outcomes (i.e., fertilization rate [FR], implantation rate [IR], CPR, miscarriage rate [MR], and LBR). 3,9
Although the premises support a possible negative impact of TAI on both the quantity and the quality of the remaining oocyte pool, the available evidence is inconclusive. 10,11 In a previous meta-analysis, we showed a detrimental impact of TAI on the course of pregnancy achieved through ART. 7 However, our findings have been questioned by subsequent systematic reviews. 12,13 As for quantitative outcomes, information is often hidden among the baseline characteristics and does not attract the reader's attention. Considering the relatively high prevalence of TAI among women of reproductive age, such uncertainties and lack of knowledge are particularly frustrating for both clinicians and their patients.
The aim of this systematic review and meta-analysis was to provide an updated data synthesis about the effect of thyroid antibodies on both ovarian reserve and the reproductive potential of women undergoing ART.
Materials and Methods
Protocol registration and guidelines
This systematic review of the published literature was reported according to the PRISMA guidelines, 14,15 and the meta-analysis was reported according to the MOOSE guidelines. 16 This study was, thus, exempt from institutional ethics review. The protocol was registered with PROSPERO (CRD42021236529).
Eligibility criteria
This systematic review and meta-analysis were restricted to two groups of published research articles:
Studies that investigated the association between TAI and ART (including IVF, intracytoplasmic sperm injection [ICSI], intrauterine insemination [IUI], or ovulation induction [OI] with timed intercourses) outcomes (i.e., FR [i.e., percentage of transformation of micro-injected oocytes into two pronuclei], IR [i.e., the number of gestational sacs observed divided by the number of embryos transferred], CPR (i.e., the number of clinical pregnancies [defined as a pregnancy diagnosed by ultrasonographic visualization of one or more gestational sacs or definitive clinical signs of pregnancy] divided by the number of women who started an ART cycle [only one cycle per patient included]), MR (i.e., the number of spontaneous loss of an intra-uterine pregnancy before 22 completed weeks of gestational age divided by the number of clinical pregnancies), and LBR (i.e., the number of deliveries that resulted in at least one live birth divided by the number of women who started an ART cycle [only one cycle per patient included])
17
; Studies that investigated the association between TAI and surrogate markers of ovarian reserve (i.e., AMH serum concentration, basal FSH serum concentration, AFC and NOR after COH for IVF or ICSI).
Information sources and search strategy
We systematically searched PubMed, MEDLINE, ClinicalTrials.gov, Embase, and Scopus from database inception to May 1, 2022. Searches were limited to studies in humans and written in English. Search strings are shown in Supplementary Appendix SA1. All pertinent articles were retrieved, and the relative reference lists were systematically reviewed to identify further reports that could be included in the meta-analysis. Moreover, review articles and meta-analysis that focused on the impact of TAI on both ART outcomes and ovarian reserve were consulted and their reference list searched for potential additional studies.
No attempt was made to identify unpublished studies. Two authors (A.Bus. and C.B.) independently evaluated the title and abstract of all articles and excluded those deemed irrelevant by both observers. Reports were classified according to the study design into case-control studies, prospective and retrospective cohort studies. In the event of multiple publications from the same group or overlapping study populations among studies, data from the most recent study were included.
Selection of studies
Studies examining TAI and ART outcomes (Group 1) were eligible for inclusion only if: (1) the FR, IR, CPR MR, and LBR were separately reported for women with and without TAI; (2) the participants were involved in autologous cycles; and (3) the outcomes were reported per patient and not per cycle. Studies on TAI and surrogate markers of ovarian reserve (Group 2) were eligible for inclusion only if the authors reported: (1) the AMH or basal FSH serum concentration or the AFC or the NOR separately for women with and without TAI, or (2) the rate of women with positive TAI according to the ovarian reserve level (i.e., DOR, normal ovarian reserve, and high ovarian reserve). We considered the use of median and interquartile range (IQR) as an indicator that the data distribution was skewed.
We did not convert median and IQR into mean ± standard deviation (SD). 18 Studies that reported continuous data (i.e., surrogate markers of oocyte quantity) as median and IQR were, thus, included only in the qualitative synthesis. Finally, studies could be included only if participants were in their reproductive age (i.e., between 15 and 49 years old), had a basal serum thyrotropin (TSH) within the normal range as defined by each single study, were not affected by overt hypothyroidism (i.e., increased TSH and/or decreased thyroxine [T4 level]) or hyperthyroidism, and were not taking medications to treat thyroid diseases.
Risk of bias and quality assessment
Two authors (A.Bus. and F.C.) independently critically appraised the included studies for risk of bias using the Newcastle-Ottawa Quality Assessment Scale. 19
To account for potential confounders (i.e., basal TSH serum level, women's age, type of thyroid antibodies, method of conception), the following subgroup analyses were conducted: (1) studies reporting data about the difference in age and/or TSH between groups; (2) studies including only subjects with basal TSH ≤2.5 mIU/L; (3) studies including only women with proven thyroperoxidase antibodies (TPO-Abs) positivity (i.e., studies that included women who were positive for TPO-Abs but who were not tested for thyroglobulin antibodies [Tg-Abs] as well as for other thyroid antibodies); (4) studies including only women who underwent ICSI; and (5) pooling of only risk estimates adjusted for age.
To evaluate the effect of women's age and basal TSH values on both MR and LBR, a meta-regression analysis was also performed. To evaluate for potential publication bias, funnel plots were generated and both Egger's test and Begg's test were performed. 18 A.Bus. and F.C. graded the quality of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. 20 The quality of evidence was downgraded by one level in case of serious concerns and by two levels in case of very serious concerns for risk of bias, inconsistency, indirectness, imprecision, and publication bias.
Data extraction and statistical analysis
Two authors (A.L. and A. Bul.) independently analyzed all articles and extrapolated their data on respective standardized forms. A final official report was compiled from these reports after resolving all discrepancies in discussion with the remaining authors. The year of publication, location, study design, characteristics of the included subjects, thyroid antibodies detected (i.e., TPO-Ab and/or Tg-Ab), thyroid function tests assessed (i.e., TSH, free T4 [fT4], free triiodothyronine [fT3]), surrogate markers of oocyte quantity (AMH, AFC, basal FSH and NOR), and ART outcomes quality (FR, IR, CPR, MR, and LBR) were recorded.
The difference in surrogate markers of oocyte quantity as well as in covariates (i.e., serum TSH concentration and age) was expressed using a mean difference (MD) with confidence interval [CI]. The risk estimate was expressed using an odds ratio (OR) with CI. If spurious data were not reported, the MD and the OR were extracted from original studies and combined in meta-analysis using the generic inverse variance method with the DerSimonian and Laird random-effects model. 15,18
The inconsistency of the studies' results was evaluated using Cochrane Q and the I 2 statistic. 18 Risk estimates were combined in a meta-analysis using a fixed-effects model when the statistical heterogeneity among the studies was absent to moderate (0% ≤ I 2 < 30%). When it was moderate, substantial, or considerable (I 2 ≥ 30%), the DerSimonian and Laird method was used for a random-effects model. 15,18 All analyses were performed using Review Manager (RevMan) [Computer program], Version 5.4, The Cochrane Collaboration, 2020. The effect of both woman's age and basal serum TSH level on MR and LBR was assessed through restricted maximum likelihood random effects meta-regression. The meta-regression analysis was performed using the “metareg” macro (Stata Statistical Software: Release 15 [Computer program; Stata Corp., 2017]).
Results
Results of search and description of studies
Figure 1 summarizes the process of study identification and selection. 12 Our literature searches yielded 435 studies, from which 19 duplicates were removed. After a review of the titles and abstracts, 30 and 32 studies were identified as potentially eligible for inclusion in group 1 and 2, respectively. After a full review, we excluded 5 reviews, 21 –25 7 systematic reviews and/or meta-analyses, 7,11 –13,26 –28 and 6 studies because they included hypothyroid and/or hyperthyroid women. 29 –34 The exact reasons for exclusion are reported in Supplementary Table S1. 33,34
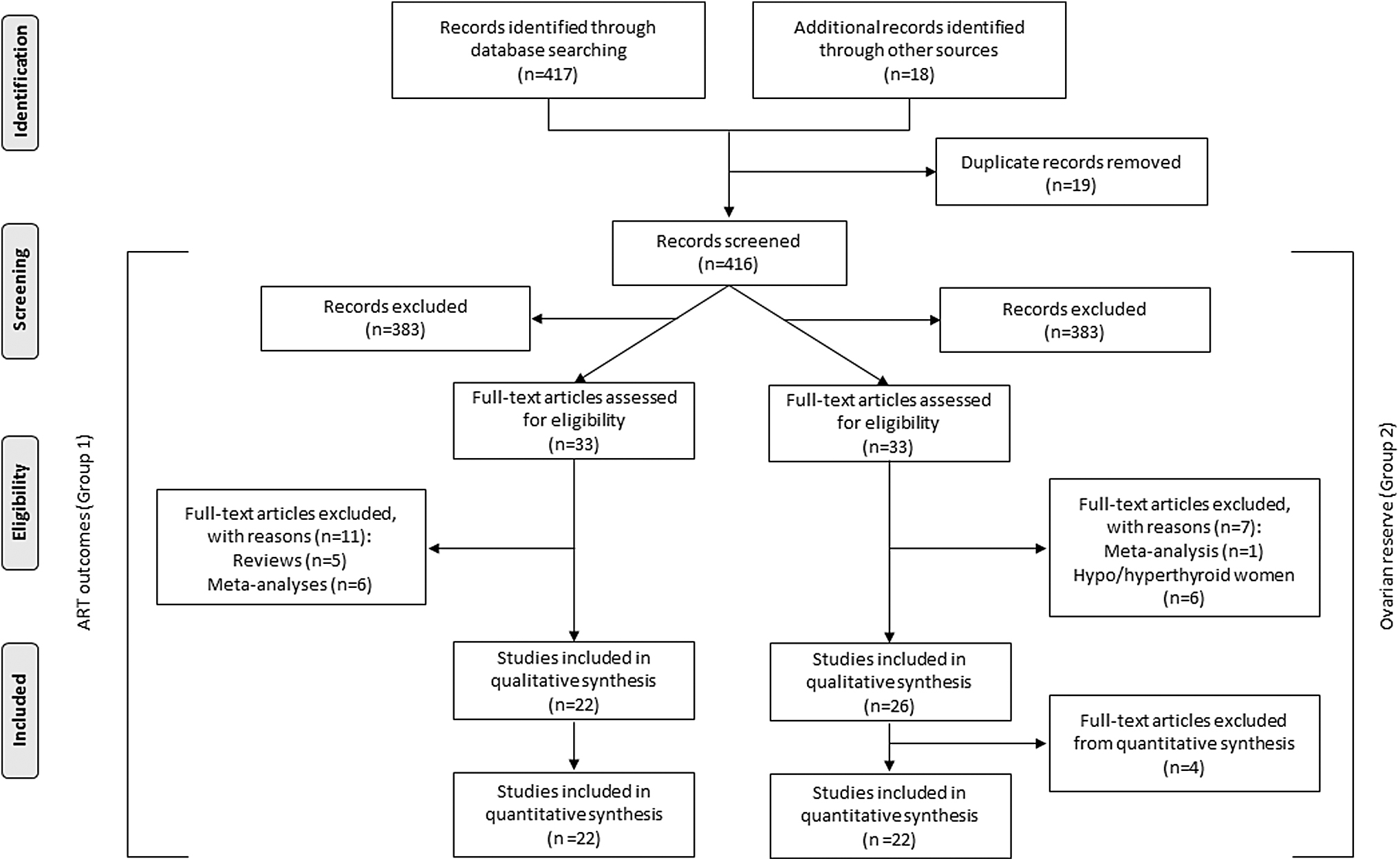
Selection of studies. Group 1 includes studies selected to investigate the association between TAI and ART outcomes. Group 2 includes studies selected to investigate the association between TAI and surrogate markers of ovarian reserve. ART, assisted reproductive technology; TAI, thyroid autoimmunity.
Data on the association between TAI and ART outcomes were extracted from 22 studies 35 –56 (Group 1). Data on the association between TAI and surrogate markers of ovarian reserve were extracted from 26 studies 10,35 –48,52,54,57 –65 (Group 2). Of these, four were excluded from the quantitative synthesis since they reported surrogate markers of ovarian reserve as median and IQR. 35,36,52,54 None of the included studies have overlapping participants for the same outcome. Characteristics of included studies are reported in Table 1.
Characteristics of the Included Studies
AFC, antral follicle count; AMH, anti-Mullerian hormone; ART, assisted reproductive techniques; CPR, clinical pregnancy rate; fT3, free triiodothyronine; fT4, serum free thyroxine; FR, fertilization rate; FSH, follicle-stimulating hormone; ICSI, intracytoplasmic sperm injection; IR, implantation rate; IUI, intra-uterine injection; IVF, in vitro fertilization; LBR, live birth rate; MR, miscarriage rate; NOR, number of oocytes retrieved; OI, ovulation induction; TAI+, positive thyroid autoimmunity; TAI−, negative thyroid autoimmunity; Tg-Ab, thyroglobulin antibodies; TPO-Ab, thyroid peroxidase antibodies; TSH, thyrotropin.
Association between TAI and ART pregnancy outcomes
Fertilization rate
Five studies reported the FR in women with TPO-Abs and/or Tg-Abs that underwent IVF/ICSI and in negative controls. 40,41,43,54,55 The FR was not significantly different among the two groups of women (random-effects model, OR 0.87, [CI 0.62–1.24], p = 0.44, I 2 = 92%) (Table 3) (Supplementary Fig. S1).
Association Between Thyroid Autoimmunity and Surrogate Markers of Ovarian Reserve
GRADE's approach to rate the quality of evidence in observational studies: Initial quality of evidence: Low. The quality rate was downgraded if: risk of bias −1 serious, −2 very serious; inconsistency −1 serious, −2 very serious; indirectness −1 serious, −2 very serious; imprecision −1 serious, −2 very serious; publication bias −1 likely, and −2 very likely. The quality of evidence was upgraded if: large effect +1 large, +2 very large; dose response +1 evidence of a gradient; all plausible residual confounding +1 would reduce a demonstrated effect, +2 would suggest a spurious effect if no effect was observed.
Implantation rate
Six studies reported the IR in women with TPO-Abs and/or Tg-Abs who underwent IVF/ICSI and in negative controls. 35,40,41,44,47,54 A significantly lower chance of embryo implantation was observed in TAI-positive women (random-effects model, OR 0.72, [CI 0.59–0.88], p = 0.001, I 2 = 36%) (Table 3) (Supplementary Fig. S1).
Clinical pregnancy rate
Twenty studies reported the CPR in women with TPO-Abs and/or Tg-Abs who underwent ART and in negative controls. 3 –47,49,51 –54,56,64 No differences in CPR emerged (random-effects model, OR 0.88, [CI 0.76–1.01], p = 0.07, I 2 = 44%) (Table 3) (Supplementary Fig. S1).
Miscarriage rate
Twenty-one studies reported the MR in women with TPO-Abs and/or Tg-Abs who underwent IVF/ICSI and in negative controls. 3 –46,48,49,51 –55,56,64 The MR was observed to be significantly higher in TAI women (random-effects model, OR 1.52, [CI 1.14–2.01], p = 0.004, I 2 = 53%) (Table 3) (Supplementary Fig. S1).
Live birth rate
Fifteen studies reported the LBR in women with positive TAI and in negative controls. 35 –38,42 –46,51 –54,56 Pooling of their results showed a significantly higher LBR in negative women (random-effects model, OR 0.73, [CI 0.56–0.94], p = 0.02, I 2 = 71%) (Table 3) (Supplementary Fig. S1).
Confounding variables assessment
Results about the influence of possible confounding variables (i.e., female age and serum TSH concentration) on the reproductive outcomes as well as sensitivity analysis according to the method of conception and the restriction to studies including only women with proven TPO-Abs are reported in Table 2.
Association Between Thyroid Autoimmunity and Reproductive Outcomes
GRADE's approach to rate the quality of evidence in observational studies: initial quality of evidence: low. The quality rate was downgraded if: risk of bias −1 serious, −2 very serious; inconsistency −1 serious, −2 very serious; indirectness −1 serious, −2 very serious; imprecision −1 serious, −2 very serious; publication bias −1 likely, and −2 very likely. The quality of evidence was upgraded on the basis of: i) magnitude of the effect (+1 if the magnitude of the effected was deemed ‘large’, +2 if the magnitude of the effect was deemed ‘very large’; ii) dose response gradient (+1 if there was evidence of a dose response gradient); iii) all plausible residual confounding (+1 if they would reduce a demonstrated effect, +2 if they would suggest a spurious effect if no effect was observed). Since the present meta-analysis included only observational studies, particularly relevant in rating up quality were the magnitude of the effect estimate and the presence of a dose-response gradient.
CI, confidence interval; cIVF: conventional in vitro fertilization; GRADE, Grading of Recommendations Assessment, Development and Evaluation; OR, odds ratio; MD, mean difference.
Meta-regression analysis
Seventeen 29 –33,35 –37,39,41,43,44,50,53,54,56,58 and 11 studies 29 –32,37,39,41,43,44,54,56 could be included in the meta-regression analysis exploring the possible influence of women's age on MR and LBR, respectively. Eleven 30,31,33,36,37,39,44,50,53,56,58 and 6 30,31,37,39,44,56 studies could be included in the meta-regression analysis focusing on the impact of basal TSH values on MR and LBR, respectively. No significant relationship between women's age and log OR for both MR (p = 0.12) and LBR (p = 0.09) was observed. Similarly, basal serum TSH seems to not have an effect on both MR (p = 0.24) and LBR (p = 0.11).
Association between TAI and surrogate markers of ovarian reserve (i.e., basal FSH and AMH serum concentration, AFC and NOR)
Three studies reported FSH serum concentration as median and IQR. None reported a significant difference between TAI-positive and -negative women. 35,36,54 Fifteen studies reported enough data to calculate the mean basal FSH difference between women with TPO-Abs and/or Tg-Abs and negative controls. 39,40,42,45 –48,57 –62,64,65 Pooling of results showed the absence of a significant difference (Table 3) (Supplementary Fig. S1).
Two studies reported AMH serum concentration as median and IQR and did not show any difference between TAI-positive and -negative women. 36,54 Pooling of results of studies reporting the mean ± SD AMH failed to show a difference between women with TPO-Abs and/or Tg-Abs and negative controls. 42,43,45,46,48,58 –60,62,64 (Table 3) (Supplementary Fig. S1). Two studies compared the prevalence of TPO-Abs according to the AMH serum concentration category. 10,61 No differences emerged (low ovarian reserve vs. normal ovarian reserve) (random-effects model, OR 1.38 [CI 0.89–2.15], p = 0.15, I 2 = 59%).
One study reported the bilateral AFC as median and IQR without showing any difference between TAI-positive and -negative women. 36 Pooling of results of studies reporting the mean ± SD AFC confirmed the absence of a difference between women with TPO-Abs and/or Tg-Abs and in negative controls (Table 3) (Supplementary Fig. S1). 43,45,57,60,63,64
Two studies compared the median NOR between women with positive and negative TAI without observing any difference. 52 The meta-analysis of studies reporting the mean ± SD NOR did not show any difference between women with TPO-Abs and/or Tg-Abs and negative controls (Table 3) (Supplementary Fig. S1). 37 –39,40,41,43,44,47,48,56,64
Confounding variables assessment
Results about the influence of possible confounding variables (i.e., female age and serum TSH concentration) on the difference in ovarian reserve surrogate markers between groups as well as the findings of studies that included only women with proven TPO-Abs are reported in Table 3.
Risk-of-bias and quality assessment results
Risk-of-bias assessment for observational studies is summarized in Supplementary Table S2. Overall, included studies showed a moderate or low risk of bias. Among the nine applicable stars assessing the three main categories of selection, comparability, and outcomes, the eligible studies received between six and eight stars. Visual evaluation of Funnel Plots and the Egger's test results suggest the reliability of the association between TAI status and NOR; MR and LBR might be hampered by publication bias (Supplementary Fig. S2).
The quality of evidence evaluated according to the GRADE system is summarized in Tables 2 and 3. Owing to the retrospective design of the included studies, the lower boundaries of CIs of risk estimate measures being close to 1, and the inability to properly adjust for the effect of possible confounding factors, the quality of evidence was between low and very low.
Discussion
Main findings
The present systematic review and meta-analysis showed that TAI-positive women undergoing ART cycles had a higher risk of miscarriage and a lower chance of live birth. Both sub-analyses and meta-regression suggest that the association between thyroid antibodies and MR was not significantly influenced by age or serum TSH concentration. However, a confounding role of age in the association between TAI and LBR cannot be excluded. Although both meta-regression and meta-analysis of adjusted risk estimates did not show a significant effect, the restriction of meta-analysis studies providing the mean (±SD) women's age showed that TAI-positive patients were significantly older. We also observed a reduced rate of embryo implantation in women with thyroid antibodies. However, the reliability of this finding can be questioned as the association disappeared after limiting the analysis to studies including only women with proven TPO-Abs. Moreover, the CPR was not significantly associated with the presence of TAI.
The increased risk of adverse pregnancy outcomes in TAI-positive women had already been observed in a previous meta-analysis and prompted many authors to formulate theories to explain the possible effect of thyroid antibodies on fertility. 7,12,66 –68 The most accepted one considers TAI as a marker of generalized immune imbalance, possibly leading to the failure of fertilization, implantation, and sustained pregnancy. 66 –68 Alternatively, TAI might have a direct pathogenic effect on ovarian tissue. Monteleone et al hypothesized that thyroid antibodies may pass the “blood-follicle” barrier and cause mediated cytotoxicity in the growing ovarian follicle. 8,66 –68
According to other authors, TAI causes a degree of relative hypothyroidism that adversely impacts the reproductive function. Importantly, ART can facilitate the development of this condition. In a systematic review and meta-analysis, we demonstrated a significant increase in the serum TSH concentration in subjects undergoing COH for IVF/ICSI. In particular, approximately one out of four euthyroid women are expected to exceed the serum TSH level threshold of 2.5 mIU/L during or immediately after COH. 66 –70 On this basis, it has been hypothesized that the supplementation of levothyroxine (LT4) before the initiation of ART cycle could reverse the negative impact mediated by TAI. 71,72 Unfortunately, data published so far are not reassuring. A recent Cochrane review demonstrated that treatment with LT4 neither increased LBR nor decreased the MR in euthyroid TAI-positive women undergoing ART. 73 These findings indirectly refute the third mentioned theory. 7
Our subgroup analyses also provided useful insights. In women who exclusively underwent ICSI, no association between the presence of thyroid antibodies and any of the considered reproductive outcomes was observed. The interpretation of these findings is suggested by the previous evidence that showed that zona pellucida may be a target for thyroid antibodies. 71 –74 Accordingly, in women with TAI, the interaction between the oocyte and the sperm cell and, as a consequence, the normal embryogenesis process could be hampered. 74 –77 The ICSI, which involves the direct injection of a single spermatozoon into the ooplasm, might thus overcome the detrimental effect mediated by TAI. 12
As for the hypothesized association between TAI and oocyte quantity, we observed that the mean values of surrogate markers of ovarian reserve (i.e., basal FSH serum concentration, AMH serum concentration, AFC and NOR after COH) did not significantly differ between women with and without thyroid antibodies. Restriction to studies including only women with proven TPO-Abs positivity confirmed these findings.
We also did not observe a difference in the proportion of women with TAI between the various ovarian reserve categories defined on the basis of the AMH serum level. Unfortunately, data from only two studies could be pooled and our findings do not allow reliable conclusions to be drawn. 10,61
Our results partially conflict with the previous literature. Some studies showed a high prevalence of thyroid antibodies positivity in patients with premature ovarian insufficiency (POI). 78 –80 Specifically, TAI was reported in 37% of POI women with Turner Syndrome and in 15% of POI patients with 46, XX karyotype. 71,81 Accordingly, the European Society of Human Reproduction and Embryology (ESHRE) suggests TAI screening in all women diagnosed with spontaneous POI. 82 Since DOR in young women and POI have been hypothesized to share at least a part of their pathophysiological mechanism, the recent guidelines published by the European Thyroid Association recommend to screen women with DOR not only for thyroid dysfunction but also for TAI. 83
In a recent meta-analysis, Hasegawa et al reported a lower AMH level in adult TAI-positive women. Although statistically significant, the calculated MD entity (0.12 ng/mL) is likely of modest clinical importance. However, adolescent girls with thyroid antibodies were shown to have a higher AMH serum concentration when compared with negative controls. 28 Our approach differs from the previous ones, as it is aimed at investigating the impact of TAI on different ovarian reserve markers. Interestingly, our findings suggest that the presence of TAI in women seeking fertility care should not be considered a risk factor for DOR and for poor ovarian response to COH.
Limitations and reason for cautions
Some limitations should be considered in the interpretation of our results. First, the reliability of the evidence could be undermined by possible confounders (e.g., woman's age and BMI, basal TSH value, indication to ART, etc.) and we rated most of the evidence as of a relatively low quality. Many of our meta-analyses were subject to statistically significant heterogeneity, and there was some concern about publication bias.
Another limitation concerns the type of thyroid antibody tested in the included studies. Some investigators included TPO-Abs- and/or Tg-Abs-positive subjects without providing separate data for women with one or both positive antibody titers. To minimize the interference of this factor, we conducted a sub-analysis that included only patients who were positive for TPO-Abs that has been defined as the most sensitive marker of TAI and linked to the risk of (sub)clinical hypothyroidism. 67 In the great majority of cases, restriction to such studies confirmed the results of the principal analysis.
Further, some studies have included subjects with TSH values >2.5 mIU/L. Although the impact of minimally increased serum TSH levels (i.e., 2.5 mIU/L < TSH ≤4.0 mIU/L) on both natural fertility and ART outcomes is still debated, the European Thyroid Association guidelines suggest treatment with LT4 in infertile women with TAI and TSH >2.5 mIU/L. 83 Even in the absence of a difference in mean TSH values between the two study groups, a negative effect determined by the concomitant presence of TSH levels >2.5 mIU/L and thyroid antibodies cannot be ruled out. We, therefore, conducted a sub-analysis including only women with a TSH value below 2.5 mIU/L, which confirmed the results of the main one.
Finally, by pooling the results of non-spontaneous pregnancy outcomes regardless of the method of conception, we might have introduced a source of heterogeneity. To overcome this issue, we performed sub-analyses taking this variable into account. Unfortunately, studies including only women selected for conventional IVF or IUI/OI are still very few and prevent clinical inferences from being made. The reliability of the evidence regarding ICSI, although supported by a larger sample size, is weakened by other factors. In particular, the use of ICSI, despite the available evidence., 84 has increased substantially in couples with non-male factor infertility.
The absence of a shared vision regarding ICSI indications makes its adoption rate extremely variable from one Fertility Unit to another, introducing a relevant confounding factor above all in retrospective studies.
Conclusions
In conclusion, in the present systematic review and meta-analysis, we observed an association between TAI and adverse ART outcomes. However, considering the extent of the calculated risk estimates and the reported limitations, a causal relationship cannot be determined. 85 Noteworthy, the possible protective effect of ICSI is promising and reassuring. This technique could potentially be a simple solution to limit the widely spread trend toward pharmacological overtreatment of TAI-positive women undergoing ART. In this regard, randomized controlled trials comparing the reproductive outcomes in TAI-positive women treated with either classical IVF or ICSI should be a research priority. Importantly, we also demonstrated the absence of a difference in surrogate markers of ovarian reserve between women with positive and negative thyroid antibodies.
These findings tend to refute the theory of a damaging process on the residual oocyte patrimony mediated by TAI. At the current state of knowledge, considering our results and the absence of treatments of proven efficacy, testing euthyroid infertile women selected for ART for thyroid antibodies is questionable.
Footnotes
Authors' Contributions
A.Bus. and C.B. conceived and designed the study. A.Bus. and F.C. independently assessed the included studies for risks of bias and graded the quality of evidence. A.Bul. and A.L. evaluated all articles and extrapolated the data on a standardized form. A.Bus. and C.B. performed the statistical analysis. A.Bus. and P.E.L.-S. drafted the first version of the article. All authors revised it critically and approved the final version to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2