
Abstract
Background:
Evidence of the efficacy of laser thermal ablation (LTA) in benign thyroid nodules is abundant. However, little is known about the effect on quality of life (QoL) of this treatment.
Methods:
Prospective cohort study investigating the effect of LTA before, three, and six months after LTA on QoL using the thyroid-specific patient-reported outcome (ThyPRO) measure. Patients receiving LTA (laser group [LG]) was compared with a well-characterized control group (CG) from the Danish civil registry.
Results:
The LG comprised 54 patients, with no age or sex differences compared with the CG (n = 739). Sixty-nine percent of the patients had a recurrent cystic thyroid nodule, 6% had a solid nodule, while the remaining 25% were of mixed character. The median nodule volume was 6.8 mL (interquartile range [IQR]: 4.0–11.1) before LTA, and 1.8 mL (IQR: 0.6–4.1) at 6 months post-LTA (p < 0.001), corresponding to a median reduction of 78%. All cystic fluid (median: 6 mL; IQR: 2.0–9.0) was aspirated before LTA. Median treatment time was 400 seconds (IQR: 300–600), applying a median energy of 823 J (IQR: 600–1200). At baseline and according to the ThyPRO scales, the LG differed significantly from the CG by having more goiter symptoms, hyperthyroid symptoms, tiredness, and cognitive complaints (p < 0.05 for all variables), but only the difference in the goiter symptom scale was of a clinically important magnitude. At three months, the LG experienced a large improvement in goiter symptoms (effect size [ES] = 1.05), a moderate improvement in cosmetic complaints (ES = 0.50), and a moderate improvement in the overall QoL (ES = 0.64). Only the improvements in the goiter symptom and the cosmetic complaint scales were clinically important. Six months after LTA, the anxiety scale showed further improvement of moderate size (ES = 0.52). At 6 months, the results above were maintained, and 79% of patients experienced a large and clinically important improvement in the goiter symptom scale and no clinically important differences were found between the LG and the CG.
Conclusions:
In this unblinded, prospective observational study, measures of disease-specific QoL were significantly improved compared with preprocedure levels, in patients with solid-cystic nodules.
Introduction
Laser thermal ablation (LTA) and other thermal ablation therapies for benign solid, mixed, or cystic thyroid nodules are increasingly used, with local neck symptoms being the primary indication for treatment. The European Thyroid Association guidelines for their use, in benign and malignant thyroid nodules, have recently been published, as the first major international thyroid society guidelines (1 –3). Further advocacy for implementing minimally invasive nonsurgical thermal treatment for thyroid nodules is provided by a recent international multidisciplinary consensus statement (4). First-line therapy of cystic thyroid nodules is most often cyst aspiration, and many patients will be cured using this treatment alone (5).
However, a significant proportion, that is, 60–90%, of patients have recurring cysts and warrant reaspiration, surgery, or other treatments such as LTA or other thermal ablation options (5). LTA has demonstrated efficacy in reducing nodule-related pressure symptoms with minimal side effects in comparison with percutaneous ethanol injections, however, at increased health care cost and reduced accessibility (6). In a retrospective multicenter study including 1531 patients, the mean nodule volume reduction by LTA was 72% ± 11% (standard deviation [SD]) after 12 months (7). Eighty-three percent of patients were treated with a single session, and both small and large nodules showed similar relative volume reduction (7). Only eight patients experienced complications, such as transient voice changes, but no patients required surgical repair (7).
Few long-term studies offer data on the treatment efficacy of LTA. In cystic-solid nodules, one study found a 15% conversion rate to surgery within 6 months of treatment (8). In patients with scintigraphically cold nodules, 8% were referred to surgery within 6 months of LTA therapy, due to inadequate treatment effect (9).
Apart from small single-center studies with limited follow-up (6,10) showing post-LTA improvements, the effect of LTA treatment on quality of life (QoL) is largely unknown. Thyroid surgery of benign thyroid nodules reduces compressive symptoms and improves QoL (11). However, compared with LTA, surgery has a higher risk profile with postoperative bleeding in 4.2% (12), short-term voice changes in up to 40% (13 –16), and recurrent laryngeal nerve paralyses in 2.1% (13,17) of patients. The disadvantages of LTA, as opposed to surgery, are its poor availability (3), lack of a histological diagnosis, and incomplete removal of the target tissue, implying risk of regrowth.
To establish the role of LTA as an alternative to thyroid surgery, awaiting head-to-head comparative studies, more data related to the effect on QoL are needed (1). Thus, we aimed to investigate, in consecutive patients with a symptomatic benign solid-cystic thyroid nodule, how QoL measured by the thyroid-specific patient-reported outcome (ThyPRO) questionnaire is affected.
Materials and Methods
This was a cohort study that, by a paired design, investigated symptom improvement and health-related QoL three and six months after LTA of benign thyroid nodules. The laser group (LG) was compared with a historical control group (CG), comprising 739 individuals randomly selected from the Danish background population, but stratified for age and sex to resemble the distribution of patients with benign thyroid disorders (18). The CG had previously completed the ThyPRO questionnaire, as described in detail elsewhere (18).
Patient cohort
All patients at the Odense University Hospital undergoing first time LTA for purely cystic, mixed cystic-solid-, or solid thyroid nodules, causing pressure symptoms and/or cosmetic concerns, were offered participation in this study in the period from September 2019 to November 2020. Fine needle or cystic fluid aspiration of the nodule showing benign cytology was mandatory in all patients. Furthermore, all patients with a cystic component had recurrence of the cystic fluid after the initial diagnostic complete aspiration. The following exclusion criteria were applied: age younger than 18 or older than 80 years, any previous neck surgery except thyroid surgery, previous thyroid LTA, previous head, neck, or thyroid malignancy, pregnancy, overt hyperthyroidism, or high-risk ultrasound (US) features (EU-TIRADS class 4–5) (19). Patients offered surgery after LTA and those who were lost to follow-up were excluded from the study, but collected data until that point were included for analyses.
Laser thermal ablation
All LTA procedures were performed by one of the authors (H.D.) who has more than 20 years of experience in LTA, neck US, and US-guided diagnostic outpatient procedures. LTA was performed under sterile conditions. After injection of local subcutaneous anesthesia, an 18G needle was inserted into the center of the thyroid lesion under real-time US monitoring. The technique has previously been described in detail (6,8,9). Any nodule fluid content was removed completely through a syringe, and the laser fiber (0.4 mm) inserted through the needle to the far end of the cystic nodule cavity or the most distant part of the solid nodule. Hereafter the needle was withdrawn, and energy applied through the laser fiber. The output power was between 1.5 and 3.0 W for ∼600 seconds. The laser power source was a continuous-wave infrared (820 nm) diode (model 15; Diomed, Cambridge, England) laser.
Pre- and post-treatment volume of the thyroid lesion and the thyroid gland was determined by US at baseline, three, and six months post-LTA, and measured as the three largest perpendicular diameters (width*length*depth/2). In addition, the volume of aspirated cystic fluid was registered at baseline and at later visits. If indicated (due to insufficient nodule volume reduction and/or persistent symptoms), an additional LTA was performed at the visit at three months. Complete cure was defined as a volume of the treated nodule of <1.0 mL at 6 months after LTA (6).
Disease-specific QoL
Treatment efficacy, in terms of change in symptoms and QoL, was evaluated by the ThyPRO (20 –22). This instrument has been thoroughly validated for use in multiple languages, including Danish (21). The ThyPRO is an 85-item patient-reported outcome measure evaluating aspects of QoL relevant for patients with benign thyroid disease. Each item is assigned into 13 multi-item scales, that is, goiter symptom, hyperthyroid symptom, hypothyroid symptom, eye symptom, tiredness, cognitive complaint, anxiety, depressivity, emotional susceptibility, impaired social life, impaired daily life, impaired sex life, and cosmetic complaint scales, as well as a 22-item composite score representing the overall QoL (20,23,24). All items are scored on a 0–4-point Likert scale, summarized and linearly transformed to a scale of 0–100 points in each scale, with 100 points representing more symptoms.
The “eye symptom scale” was not included, as it was not relevant for this patient group in accordance with the principles of the questionnaire (24). The ThyPRO has been used to monitor QoL after treatment of benign thyroid disease by surgery, ethanol sclerotherapy, and radioactive iodine (11,25 –27). Recently, the minimal important changes (MIC) for groups (MICg) as well as for individuals (MICi) have been defined and represent clinically important differences (28).
The questionnaire was sent electronically to the patients approximately two weeks before treatment. Informed consent was obtained to ensure further participation in the study. The questionnaire was sent again two weeks before the follow-up visits at three and six months, respectively.
The project has been evaluated by the local ethics committee with identification number S-20190028 and was completed in accordance with the Declaration of Helsinki as revised in 2013.
Statistics
Data on patient characteristics, thyroid volume reduction, and ThyPRO are presented. Based on data from our previous cohort undergoing thyroid surgery (11), the sample size was calculated to a minimum of 45 patients, to obtain a score change of 6 ± 14 (SD) points on the goiter symptom scale. To allow for loss to follow-up and conversion to thyroid surgery, inclusion of a minimum of 54 patients was considered relevant. Descriptive data were reported as means with standard deviations, medians with interquartile range (IQR), or numbers and percentages.
A nonpaired t-test was used to compare the LG and the CG. Cohen's effect size (ES)/Glass' delta was calculated based on mean change divided by the standard deviation at baseline for the ThyPRO data. An ES of 0.2–0.5 is considered small, 0.5–0.8 is moderate, and values >0.8 as large (29). Observed mean differences between and changes within groups of patients were categorized as clinically important, if values were above the previously determined scale-specific MICg; changes in scores within individual patients were categorized as clinically important if above the scale-specific MICi (28).
A linear mixed model was used to evaluate the effect of LTA on the ThyPRO scales during follow-up. Age, sex, and volume of the thyroid lesion were independent variables in the model. Next, a multiple regression analysis was used to evaluate the effect of age, sex, and volume of the thyroid lesion on the ThyPRO scales. Finally, patients needing more than one LTA treatment were compared with patients cured by the initial treatment using post hoc multiple linear regression analyses with age, sex, nodule volume, nodule characteristics, and goiter symptoms as independent variables.
Results
Patient characteristics
Consecutively, 105 patients were assessed for eligibility (Fig. 1). The patients were referred for LTA from the Departments of Internal Medicine, Departments of Otolaryngology, private practicing ENT specialists, and general practitioners in Denmark. Thirty-five patients (31%) were ineligible for treatment, and 16 (15%) declined to participate, leaving 54 patients (77% of those eligible) to be enrolled. The median age of the patients was 52 (range, 18–76) years. Baseline characteristics did not differ significantly between the LG and CG (Table 1).

Flowchart of patient inclusion and follow-up.
Characteristics of Patients with a Benign Thyroid Nodule/Cyst (n = 54) and the General Population (n = 739)
LTA, laser thermal ablation; n, number; SD, standard deviation; TSH, thyrotropin.
Forty-six of 54 patients (85%) completed all US examinations and ThyPRO questionnaires. Eight patients (15%) had their US examination canceled at 3 months, and 3 patients (5%) at 6 months, as a consequence of the national lockdown (March 11, 2020, to April 26, 2020) caused by either the COVID-19 pandemic or as a consequence of a strike among nurses during the summer of 2021. These cancelations reduced the number of US examinations, but did not affect the ThyPRO data collection, which 96% of the participants completed. Forty-five patients (83%) had 1 LTA treatment only, while the remaining 9 patients (17%) underwent 2 treatments, with 8 patients at 3 months and 1 patient at 6 months after initial LTA. One patient was referred to thyroid surgery 4 weeks after a first time LTA, and 1 patient at 6 months after the second LTA. One patient was lost to follow-up.
Effect of LTA on thyroid and nodule volume
The total thyroid volume diminished from a median of 19.5 mL (IQR 14.3–23.6 mL) at baseline to 14.6 mL (IQR 10.0–19.6 mL) at 3 months post-LTA (p < 0.001), corresponding to a median volume reduction of 22% (IQR 8–44%). Thus, at 6 months, the median thyroid volume of 15.2 mL (IQR 9.9–18.8 mL) versus 19.5 mL (IQR 14.3–23.6 mL) at baseline (p < 0.001) corresponded to a reduction of 18% (IQR 2–45%).
The median nodule diameter was 30 mm (IQR 25–36 mm) at baseline, 19 mm (IQR 15–26 mm) at 3 months (p < 0.001), and 17 mm (IQR 13–24 mm) at 6 months (p < 0.001) (Table 2). The median total nodule volume was 6.8 mL (IQR 4.0–11.1 mL) at baseline and 1.8 mL (IQR 0.6–4.1 mL) at 3 months (p < 0.001), that is, a reduction by 70% (IQR 44–90%) when including patients receiving 1 and 2 LTA treatments. At 6 months, the nodule volume was 1.6 mL (IQR 0.6–3.0 mL) (p < 0.001), corresponding to a reduction of 78% (IQR 51–91%).
Ultrasound Characteristics of Cystic, Mixed, and Solid Thyroid Nodules at Baseline, Three Months, and Six Months After Laser Thermal Ablation (n = 54)
IQR, interquartile range.
At baseline, the median volume of aspirated cyst fluid was 6.0 mL (IQR 2.0–9.0 mL), at 3 months 0.0 mL (IQR 0.0–1.0 mL), and 0.0 mL (IQR 0.0–0.0 mL) at 6 months after LTA. At 3 months after LTA, patients in need of a second LTA (n = 8) had the cystic part of 3.0 mL (IQR 2.0–6.3 mL) aspirated before the LTA procedure. The median remaining solid part was 1.1 mL (IQR 0.2–1.9 mL) at baseline, 1.1 mL (IQR 0.3–2.5 mL) at 3 months, and 1.0 mL (IQR 0.4–2.0 mL) at 6 months after LTA. At 6 months, the rate of complete cure, that is, reducing the volume of the treated nodule to less than 1.0 mL, was 46% (n = 23), which probably reflects a change in nodule morphology rather than complete elimination of the nodule or cyst.
Considering only the cystic part, complete cure (cystic volume <1 mL) was obtained in 50% (n = 25) of the patients. At 3 and 6 months, the recurrence rate, that is, nodules with increased volume compared with previous measurements, was 4% (n = 2) and 24% (n = 12). In all, nine patients required a second LTA due to insufficient nodule reduction or persistent symptoms. Four of these nine individuals requiring a second LTA showed no reduction in nodule volume at six months, and one patient was referred for surgical treatment. Patients requiring retreatment were younger (age 40 ± 14 years, p = 0.005), while there was no significant difference in sex, nodule volume, nodule characteristics, or pressure symptoms at baseline compared with those requiring only a single LTA treatment.
Patients with the need for a second LTA were treated for a longer time during LTA (300 seconds [IQR range 300–600 seconds], p = 0.04) compared with patients only having one LTA treatment (Supplementary Table S1; comparison of patients needing retreatment with LTA compared with those needing only one treatment).
Median amount of applied energy was 823 J (IQR 600–1200 J) with a median treatment time of 300 seconds (IQR 300–600 seconds). The median pain score, evaluated immediately after completion of LTA, was 2 points (IQR 1–4 points) on a verbal rating scale (0–10 points).
QoL at baseline compared with the general population
Compared with the CG, the LG had more goiter symptoms, hyperthyroid symptoms, tiredness, and cognitive complaints (all p < 0.05), while no differences were seen on the hypothyroid symptom, anxiety, depressivity, and emotional susceptibility scales (Fig. 2 and Table 3). The remaining scales were not applicable, as these questions are asked with attribution to thyroid disease and therefore not applicable to the general population. The goiter symptom scale showed the largest difference (i.e., 30 points) between the LG and the CG. The hyperthyroid, tiredness, and cognitive complaint scales showed differences below 10 points between the two groups. According to the MICg level, only the score on the goiter symptom scale of the LG was clinically different compared with the scores among the CG.
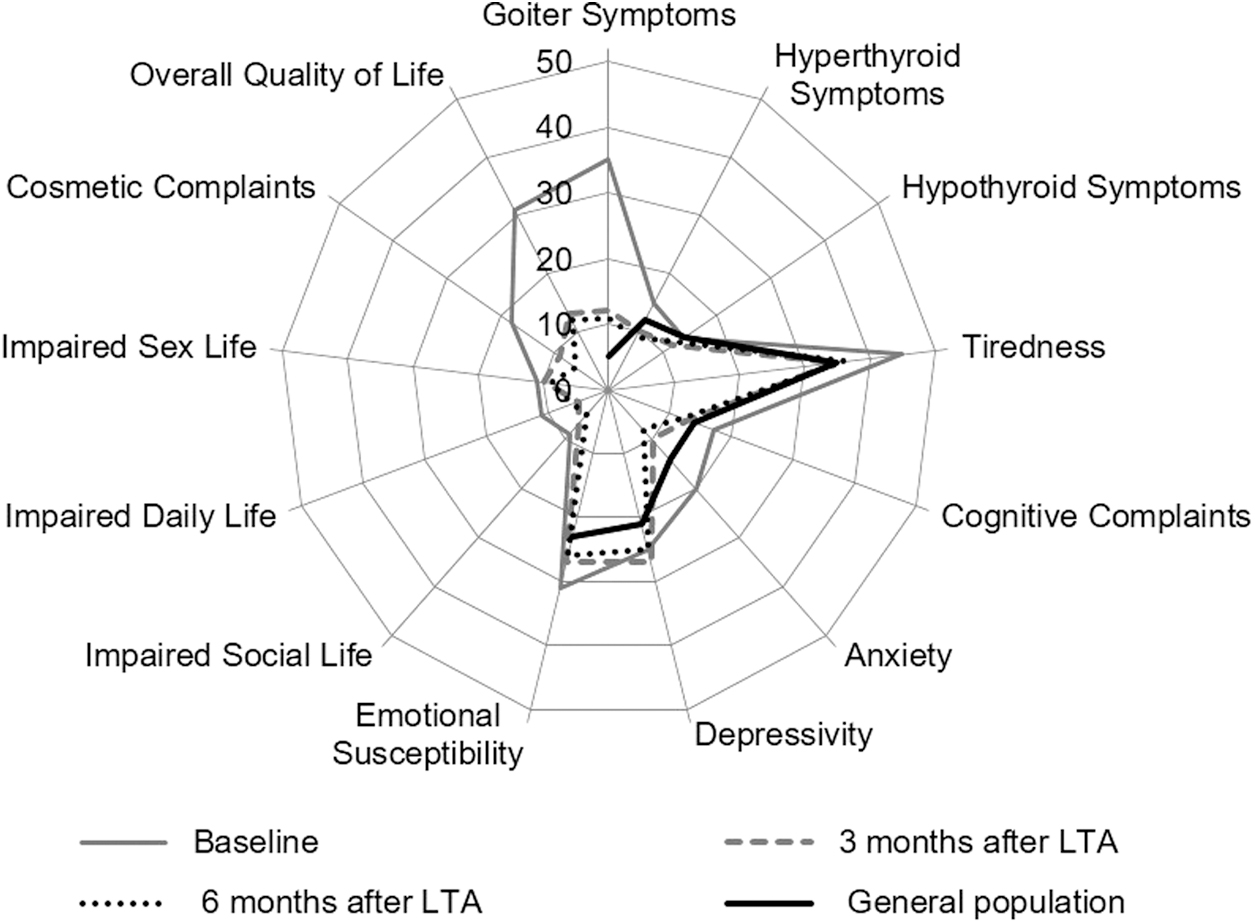
Radar plot of ThyPRO scale scores at baseline, and at three and six months after LTA of patients with a symptomatic thyroid lesion (n = 54), in comparison with the general population (n = 739). LTA, laser thermal ablation; ThyPRO, thyroid-specific patient-reported outcome.
Mean Thyroid-Specific Patient-Reported Outcome Scale Scores for the General Population and for Patients with Solid-Cystic Thyroid Nodules Undergoing Laser Thermal Ablation
The MICg are given, according to Ref. (25). ThyPRO scores above MICg are marked with bold.
CG versus LG, using a nonpaired t-test.
LG baseline versus six months after LTA, using a linear mixed model.
CG versus LG at 6 months after LTA, using a nonpaired t-test.
CG, control group; LG, laser group; MICg, minimal important change levels for groups; ThyPRO, thyroid-specific patient-reported outcome.
Effect of LTA on QoL
At 3 months after LTA, the LG experienced a large decrease (improvement) on the goiter symptom scale (ES = 1.05), a moderate decrease on the cosmetic complaint scale (ES = 0.50), and a moderate decrease on the overall QoL scale (ES = 0.64; Table 3). Small, but statistically significant, improvements were seen on the hyperthyroid, tiredness, anxiety, and impaired daily life scales (ES <0.50).
At 6 months after LTA, the anxiety scale showed a further moderate improvement (ES = 0.52, p < 0.001), while cognitive complaints, emotional susceptibility, and impaired social life now showed minor (ES <0.50), but statistically significant, improvements. Only the scores on the goiter symptom and the cosmetic complaint scales reflected clinically important mean changes (i.e., above the MICg level) at both 3 and 6 months after treatment (Fig. 3), while the remaining changes were below the MICg threshold.
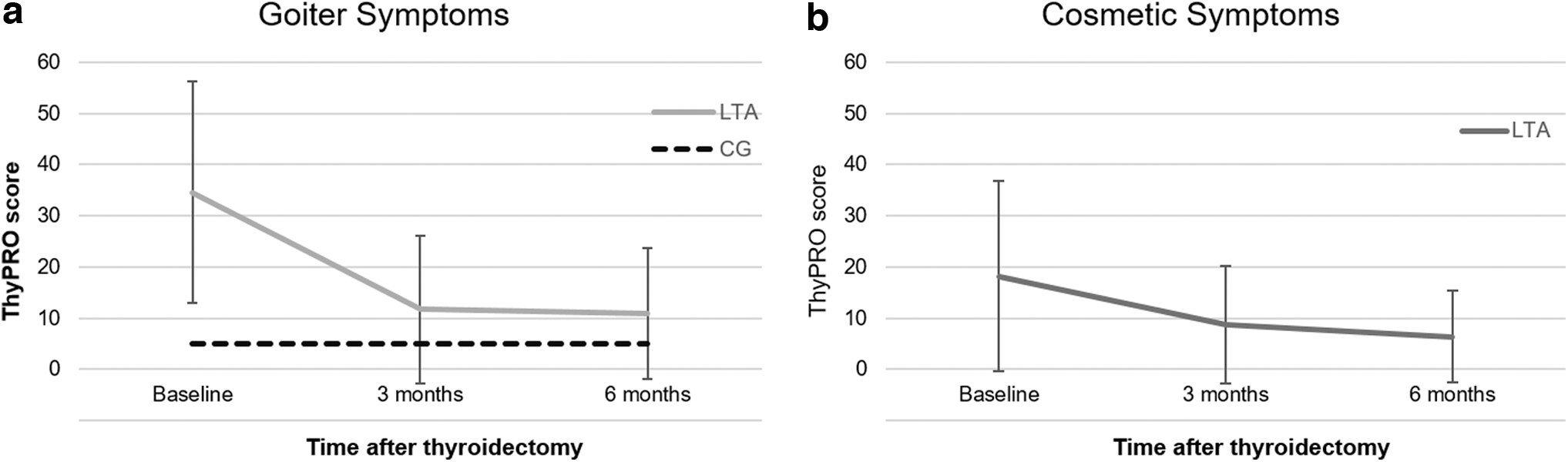
Profile plot of changes in the scales with clinically significant changes, that is, the goiter symptom scale (
The proportion of individual patients experiencing a clinically important change for each scale is presented in Supplementary Table S2. As shown, 75% of the patients experienced a clinically important improvement in goiter symptom scores, which increased to 79% at 6 months.
The regression analyses revealed no impact of age, sex, and volume of the thyroid lesion on the ThyPRO scores at baseline. Regarding the change in QoL from baseline to end of follow-up, the improvement in cosmetic complaints was positively correlated with the baseline volume of the thyroid lesion (p = 0.005, 11-point decrease in cosmetic complaints pr. logarithmic value of nodule volume), and also with changes of the nodule volume (p = 0.005, 10-point decrease in cosmetic complaints pr. logarithmic value of nodule volume). At 3 months, the cosmetic complaint score was higher (i.e., worse) among patients requiring retreatment with LTA than those who needed only one LTA (coefficient 8.0 points, p = 0.01). None of the remaining ThyPRO scores was associated with the need for retreatment.
QoL after LTA compared with the general population
Six months after LTA, the LG experienced significant relief of symptoms. Although the scores on the goiter symptom scale improved, patients still had more goiter symptoms compared with the CG (11 ± 13 points vs. 5 ± 9 points; p = 0.04), but not of clinical relevance according to MIC levels. The LG also had higher (worse) scores on the depressivity and emotional susceptibility scales, compared with the CG, despite no significant differences at baseline. No significant differences were found on the remaining ThyPRO scales.
At three months after LTA, the goiter symptom scale was the only one with higher scores in the LG than in the CG, when taking the MICg levels into consideration. Such difference between the two groups was absent at six months.
Discussion
For a number of patients, LTA and other thermal ablation methods are attractive options instead of thyroidectomy, ethanol treatment, or repeated aspirations of cyst fluid (1,3,30,31). In this study, we confirmed that LTA is very effective in achieving a reduction of the thyroid nodule volume, with a median reduction of 78% after 6 months, which is in line with previous findings (7,8). In parallel, four out of five of the patients experienced a clinically important reduction in goiter symptoms.
Our study is the first to use the thyroid-specific ThyPRO questionnaire for evaluation of LTA of thyroid nodules, adequately powered, and with the inclusion of a CG. Before treatment, and compared with the general population, patients had significantly more goiter symptoms, hyperthyroid symptoms, tiredness, cognitive complaints, and anxiety. Only the difference in goiter symptoms was clinically relevant when considering MIC levels. Most symptoms were ameliorated by LTA, and the patients obtained a QoL similar to that in the general Danish population matched for gender and age. An exception was that goiter symptoms remained statistically more prevalent among patients, which is in accordance with persistent symptoms in other thyroid phenotypes such as hypothyroidism (32) and hyperthyroidism (33).
However, the difference in goiter symptoms was of limited clinical relevance according to the MIC. The improvement in the anxiety scale may rely on the fact that suspicion of malignancy was ruled out by fine needle aspiration and US examinations during follow-up (34,35).
The use of ThyPRO allows comparing our results with other treatment modalities using the same tool for QoL measurement. In addition, Cohen's ESs were used to convert the results into standard units, to compensate for differences in cohort composition. We previously published a study of 106 patients with benign thyroid nodules and the effect of surgery on QoL measured with ThyPRO (11). In that study, the baseline scores were very similar to those in the present study, despite the fact that the patients had much larger thyroid glands, that is, a median volume of 35 mL versus 19 mL (11).
However, it is well known that goiter symptoms and the thyroid volume are poorly correlated variables (13), but change in nodule volume, more specifically, did correlate to symptom improvement in 10 of the 13 ThyPRO scales. The location of the nodule within the thyroid gland and growth rate are probably more important (11,36). However, all examinations should be made with focus on avoiding unnecessary treatments, as thyroid nodules in the majority of the population are an incidental finding (37). This is, in our study, reflected by 25% of referred patients not receiving LTA treatment.
The present study demonstrates an overall restoration of QoL, reaching a level similar to that in the general Danish population (11). Importantly, this should be seen in the context of LTA being an outpatient treatment associated with fewer complications and shorter time of convalescence in comparison with thyroid surgery. However, an LTA and a surgical cohort are not fully comparable as LTA treatment is not feasible in very large goiters or in cases with multiple thyroid nodules. A definitive comparison of efficacy would require a prospective randomized controlled study, including adequate follow-up and an evaluation of the socioeconomic consequences of the two treatments.
Some limitations of our study need to be addressed. Obviously, patients were highly selected by referral and were treated at a tertiary university center. LTA was provided by a specialized team with years of experience with LTA, which may reduce the external validity of our data. Some patients were lost to follow-up, but since this number was low, we believe that our results were not affected to any significant extent. Lastly, there is a well-known clinically significant placebo effect regarding needle intervention procedures focusing on pain relief (38,39).
However, this study evaluated a technique that offers a lasting effect following cyst aspiration with low risk of complications when compared with aspiration alone or combined with ethanol injection in recurrent cystic nodules. Even though the primary treatment for cystic thyroid lesions is cyst aspiration, all of the patients had been treated according to current guidelines before referral for LTA. Simple aspiration is the treatment of choice, but the recurrence rate is 60–90% and positively correlated with the number of aspirations and cyst volume (5,6,40,41). The use of ethanol injection may be associated with pain, mostly mild, and a minor risk of ethanol leakage causing tissue necrosis and fibrosis (40). We did not include a sham-intervention group, as LTA was, according to current guidelines, a relevant treatment option for all included patients (1).
The nodules treated in this study were heterogeneous. The majority of lesions were primarily cystic, and we cannot exclude that some of the improvement in QoL following LTA was achieved by the cyst aspiration alone. The study was not powered to analyze the effect of LTA in individual subtypes of nodules. Such a stratification is relevant to compare LTA with other minimally invasive therapies. Thus, LTA treatment and other US-guided interventions are known to be very effective for volume reduction of cystic nodules after aspiration, especially in the case of a residual solid component postaspiration (42,43). Surgical series mostly include patients with multinodular goiter and thyroid malignancy, and such individuals are with few exceptions not candidates for LTA (1,2).
We conclude that LTA of cystic, semisolid, and solid thyroid nodules is effective, not only for shrinkage of the thyroid lesion, but also for reducing thyroid-related symptoms in this unblinded, prospective observational study. Importantly, after treatment, QoL was restored to a level similar to that in the general population. Such information is important when guiding the patient in choice of treatment and addressing realistic expectations in relation to goiter treatment.
Footnotes
Authors' Contributions
J.R.S. participated in writing the protocol, data collection, data analyses, and writing of the article; H.D. and T.W. participated in the study design, data collection, data analyses, and writing of the article; P.C. and L.F. participated in the study design, data collection, data analyses, and writing of the article; L.H. and S.J.B. participated in the study design, data analyses, and writing of the article.
Author Disclosure Statement
L.F. received payment or honoraria for lectures, presentations, speakers' bureaus, article writing, or educational events from Gedeon Richter Nordics AB. All other authors have no competing financial interests.
Funding Information
The study has been funded by the University of Southern Denmark, Denmark, and Odense University Hospital, Denmark.
Supplementary Material
Supplementary Table S1
Supplementary Table S2