
Abstract
Background:
It is unclear if cigarette smoking and alcohol consumption are associated with thyroid cancer risk. Our aim was to explore for any associations between cigarette smoking and alcohol consumption with thyroid cancer, after adjusting for potential confounders.
Methods:
Using data from the Korean National Health Insurance database, we retrospectively identified individuals aged ≥20 years who participated in the 2009 health screening program and were followed until 2017. We estimated the adjusted hazard ratio (aHR) for the risk of thyroid cancer using a Cox proportional hazard model, adjusted for age, sex, regular exercise, monthly income, body mass index, diabetes mellitus, and dyslipidemia.
Results:
During a mean follow-up period of 8.33 ± 0.57 years, of 9,699,104 participants, 89,527 (0.9%) were diagnosed with thyroid cancer. Compared with those who never smoked, current smokers had a lower risk of thyroid cancer (aHR: 0.74, 95% confidence interval [CI]: 0.72–0.76), while ex-smokers did not (aHR: 0.98, 95% CI: 0.96–1.01). There was no significant dose–response relationship with regard to daily amount smoked, duration of smoking, or pack-years. A reduced risk of thyroid cancer was observed in subjects who reported the following categories of alcohol intake (compared with none): mild (aHR: 0.92, 95% CI: 0.90–0.93), moderate (aHR: 0.86, 95% CI: 0.84–0.89), and heavy (aHR: 0.86, 95% CI: 0.82–0.89). Inverse associations with thyroid cancer risk were observed regarding the number of drinking episodes per week and the number of drinks per occasion. A submultiplicative effect of smoking and alcohol consumption was observed (p-interaction <0.001).
Conclusions:
We observed that thyroid cancer risk was inversely associated with smoking and alcohol consumption, with a significant interaction between these variables.
Introduction
Smoking and alcohol consumption are major risk factors for various cancers. However, the association between cigarette smoking or alcohol consumption and thyroid cancer risk is unclear. An inverse association between current smoking and thyroid cancer risk has been reported in recent cohort studies, such as the United States Radiologic Technologists (USRT) cohort (282 cases from 90,713 participants; hazard ratio [HR] 0.54 for current smokers) (1), the Kangbuk Health Screening cohort (1250 cases from 96,855 participants, HR 0.58 for current smoking) (2), and the Women's Health Initiative (WHI) cohort (331 cases from 159,340 participants, HR: 0.54 for current smokers) (3). Similar results were reported in pooled analyses of studies from geographically diverse areas (2175 cases from 31 eligible studies; relative risk [RR] 0.74, 95% confidence interval [CI]: 0.64–0.86) and the United States (1003 cases from five studies, HR: 0.68, 95% CI: 0.55–0.85) (4,5). However, a study from a San Francisco Bay area cohort (196 cases from 204,964 participants) (6) did not show a significant relationship.
An inverse association with thyroid cancer incidence is not reported among past smokers (1 –4,6). Furthermore, a dose–response relationship of duration and intensity of smoking has not been consistently observed; some reports suggest a significant dose–response relationship (2,5,7), while others do not (3). One pooled analysis suggested that age did not significantly impact the association between smoking and thyroid cancer risk (5), while another study suggested that a sex effect was more prominent in men than women (although a statistical interaction was not reported) (1,2).
Regarding alcohol consumption and thyroid cancer, the results of cohort studies have been inconsistent. An inverse association has been suggested by some studies, including the National Institutes of Health–American Association of Retired Persons (NIH-AARP) cohort (370 cases from 490,159 participants; RR: 0.57 for two or more drinks/day vs. none) (8), and the Million Women study (421 cases from 1,280,296 participants) (9). However, no association was found in other studies, including the WHI cohort (3), USRT study (1), San Francisco Bay area cohort (6), or Canadian National Breast Screening Study (10). Furthermore, a positive association was found in the Korean National Health and Nutrition Examination Survey study (11). In studies showing positive results (8,9) and in pooled analysis (5,12), a dose–response relationship was noted. An interaction with age was not significant (5) or not investigated (8,12) in previous studies with positive results. Similarly, no significant (5,8) or prominent (12) interaction with sex was observed.
Previous studies may be limited by a low number of incident thyroid cancers (maximum of 1250 for a single study or 2175 for a pooled analysis), which did not allow for sufficient statistical power in the examination of a potential dose–response relationship and effect modification through stratified analyses. Moreover, while alcohol consumption and cigarette smoking are closely related habits (7), the potential interaction between the two in the development of or protection against thyroid cancer has rarely been investigated to date. The inverse association between alcohol intake and thyroid cancer was suggested to be more prominent among never-smokers compared with ever-smokers in the NIH-AARP study (8). A pooled analysis also suggested a stronger association between alcohol and thyroid cancer among never-smokers, and not among ever-smokers (5).
Our aim was to evaluate for potential associations between cigarette smoking and alcohol consumption, with thyroid cancer risk. We planned to adjust for confounders and explore for a possible interaction between the two variables.
Methods
Study design and population
We conducted a retrospective cohort study using data from the Korean National Health Insurance (KNHI) database. The profile of the database has been reported elsewhere (13 –15) and the details are described in the Supplementary Material.
Among individuals who underwent health examination, a total of 9,699,104 individuals were enrolled in this study. Figure 1 shows a summary of the process for selecting the study population. This study was approved by the Institutional Review Board (IRB) of Samsung Medical Center (IRB file no. SMC 2018-09-002). The need for informed consent from individual participants was waived as this study involved only deidentified data.
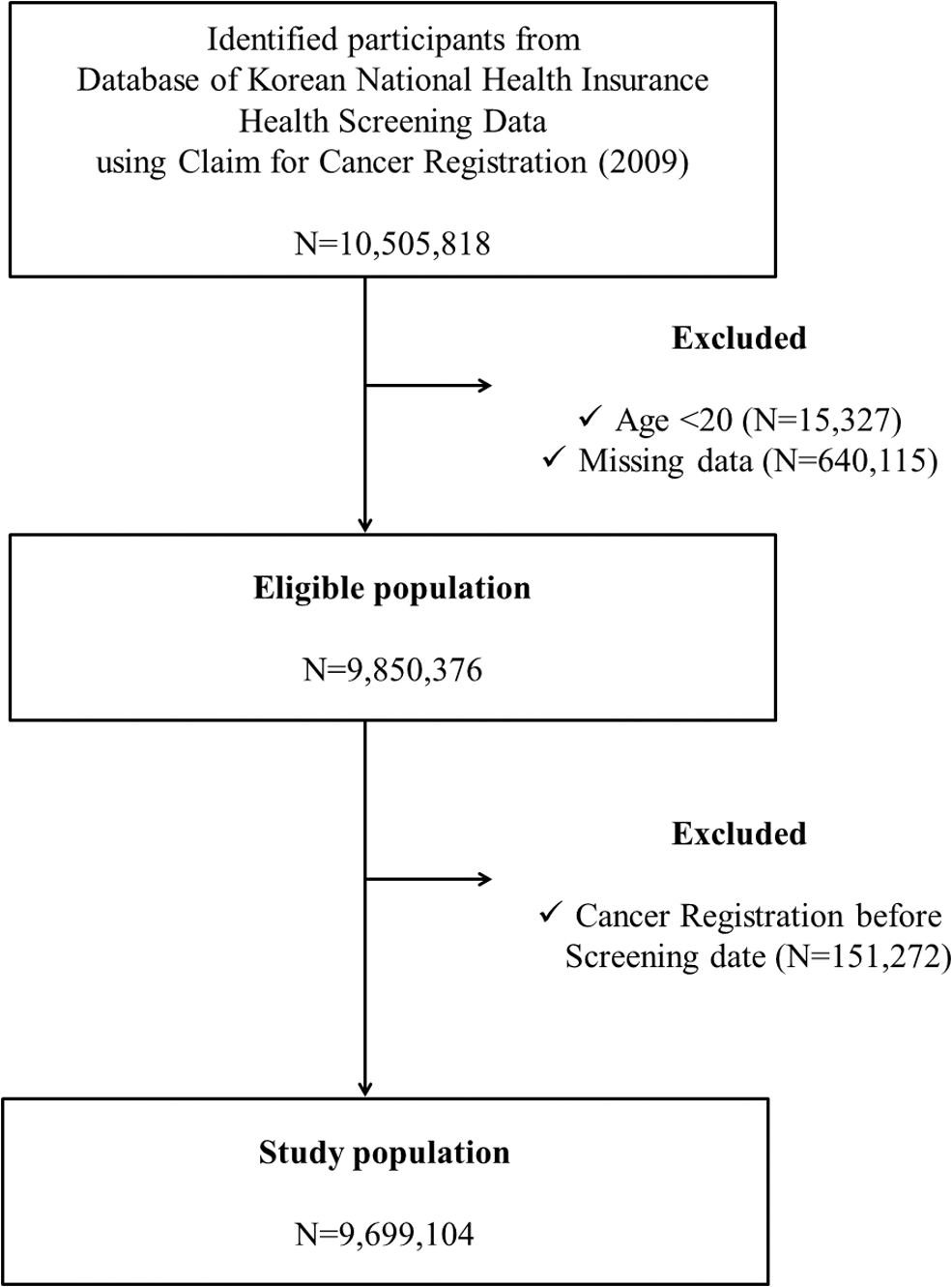
Participant flowchart.
Exposure assessment
Exposure data were self-reported, with average estimates of quantities. Smoking status was classified as follows: “never,” “past,” and “current,” respectively. The duration of smoking was categorized as follows: “less than 10 years,” “10 to 20 years,” or “more than 20 years.” Pack-years smoked were estimated by multiplying average daily cigarette smoking by the smoking duration.
Participants reported how many times per week they usually drank as well as how many glasses they drank per occasion, and the weekly amount of alcohol consumption was calculated by multiplying these values. Alcohol intake was categorized as follows: “never,” “mild” (average <15 g/day), “moderate” (15–30 g/day), or “heavy” (<30 g/day).
Potential confounders
Several variables potentially associated with thyroid cancer risk were regarded as confounders, including sex, body mass index (BMI) (16), regular exercise (1,17), monthly income (18), and chronic illnesses, including diabetes (19,20) and hyperlipidemia (21,22). Detailed information on covariates is provided in the Supplementary Material.
Outcome measurements
The incidence of thyroid cancer was defined based on the diagnosis code for thyroid cancer (i.e., C73) registered after baseline screening (23) with inclusion in a special copayment reduction program for critical illness (For details, please refer to the Supplementary Material). Participant follow-up was from the date of enrollment in the database to the first date of the following potential events: thyroid cancer diagnosis, death, or last date of follow-up (December 31, 2017).
Statistical analysis
The characteristics of the study population were summarized using descriptive statistics. We performed multivariate Cox proportional hazards regression analyses to estimate the HRs of incident thyroid cancer, relative to smoking and alcohol consumption (Supplementary Material). All analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA) and all p-values were two-sided.
Results
Study participants and their characteristics
During the mean follow-up period of 8.33 ± 0.57 years, 89,527 (0.9%) individuals were diagnosed with thyroid cancer. Baseline characteristics of the subjects are shown in Table 1. Patients who were diagnosed with thyroid cancer were older and were more often female (76.2% vs. 45.2%), compared with those who did not develop thyroid cancer. In addition, there were fewer individuals who reported themselves to be current or ex-smokers or mild-to-heavy drinkers in the thyroid cancer group.
Distribution of Selected Characteristics Among Thyroid Cancer Cases and Noncases
BMI, body mass index.
Risk of thyroid cancer mediated by cigarette smoking status
Compared with those who never smoked, current smokers had a lower risk of thyroid cancer (adjusted HR [aHR: 0.74, 95% CI: 0.72–0.76]), while ex-smokers did not [aHR: 0.98, 95% CI: 0.96–1.01] (Table 2). There was no significant dose–response relationship according to the daily amount of smoking or duration of smoking among either past smokers or current smokers. A stepwise decrease in thyroid cancer risk according to total pack-years of smoking among current smokers was not observed (Table 3).
Association of Cigarette Smoking and Alcohol Intake with the Risk of Thyroid Cancer
Incidence rate: per 1000 person-years.
Model 1: adjusted for age and sex.
Model 2: adjusted for age, sex, regular exercise, monthly income, BMI, and alcohol consumption (for analyses of smoking analyses) or cigarette smoking (for analyses of alcohol intake).
Model 3: adjusted for age, sex, regular exercise, monthly income, body mass index, alcohol consumption (for analyses of smoking analyses) or cigarette smoking (for analyses of alcohol intake), diabetes mellitus, and dyslipidemia.
aHR, adjusted hazard ratio; CI, confidence interval.
Association of Cigarette Smoking with the Risk of Thyroid Cancer
Incidence rate: per 1000 person-years.
Adjusted for age, sex, regular exercise, monthly income, body mass index, alcohol consumption, diabetes mellitus, and dyslipidemia.
Risk of thyroid cancer mediated by alcohol consumption
Compared with never-drinkers, mild (aHR: 0.92, 95% CI: 0.90–0.93), moderate (aHR: 0.86, 95% CI: 0.84–0.89), and heavy (aHR: 0.86, 95% CI: 0.82–0.89) drinkers were observed to have a lower risk of thyroid cancer (Table 2). A more prominent inverse relationship in the risk of thyroid cancer was observed according to both the number of drinking episodes per week (aHR: 0.81, 95% CI: 0.74–0.88 for daily drinkers vs. nondrinkers) and the number of glasses consumed in a single sitting (aHR: 0.87, 95% CI: 0.82–0.92 for ≥15 drinks/occasion vs. nondrinkers). Higher weekly consumption of alcohol was associated with a reduced risk of thyroid cancer compared with nondrinkers (≥40 g/week; aHR: 0.85, 95% CI: 0.81–0.89) (Table 4).
Association of Alcohol Intake with the Risk of Thyroid Cancer
Adjusted for age, sex, regular exercise, monthly income, body mass index, cigarette smoking, diabetes mellitus, and dyslipidemia.
Impact of the interaction between smoking and alcohol consumption on thyroid cancer risk
The estimated risk of thyroid cancer as mediated by combined smoking and alcohol status is displayed in Table 5. There was a statistically significant interaction between smoking and alcohol drinking on thyroid cancer risk (p-interaction <0.001); for example, the risk of thyroid cancer in those who were both current smokers and heavy drinkers (aHR: 0.62, 95% CI: 0.59–0.66) suggests a submultiplicative interaction slightly lower than that expected due to the independent effectof current smoking and heavy drinking (i.e., 0.70 × 0.80 = 0.56).
Interaction Between Smoking Status, Alcohol Intake, and Thyroid Cancer Risk
Adjusted for age, sex, regular exercise, monthly income, body mass index, diabetes mellitus, and dyslipidemia.
Effect modification by age, sex, and income status
Stratified analyses suggested that the association of cigarette smoking with thyroid cancer was present in younger individuals (aHR: 0.75, 95% CI: 0.73–0.77 for current vs. never-smokers aged <65 years; aHR: 0.89, 95% CI: 0.79–0.99 for current vs. never-smokers aged ≥65 years) (p-interaction <0.001). No significant differences were found in stratified analyses performed according to sex or income status of the study subjects (Fig. 2).

HRs estimating thyroid cancer risk according to cigarette smoking. Estimated by Cox proportional hazards model: HR adjusted for age, sex, regular exercise, monthly income, body mass index, alcohol consumption, and the presence of diabetes mellitus and dyslipidemia. HR, hazard ratio.
The inverse association of alcohol intake and thyroid cancer risk was analyzed in subgroups as follows: older than 65 years (aHR: 0.78, 95% CI: 0.65–0.95 for heavy vs. never-drinkers) and in younger people (aHR: 0.87, 95% CI: 0.84–0.91, p-interaction <0.001), women (aHR: 0.71, 95% CI: 0.65–0.78 for heavy vs. never-drinkers) and men (aHR: 0.91, 95% CI: 0.87–0.96), respectively (p-interaction <0.001). No significant effect modifications were observed in subgroup analyses performed for monthly income (Fig. 3).

HRs estimating thyroid cancer risk according to alcohol intake. Estimated by Cox proportional hazards model: HR adjusted for age, sex, regular exercise, monthly income, body mass index, cigarette smoking, and the presence of diabetes mellitus and dyslipidemia.
Discussion
To our best knowledge, this is the largest study to date investigating the potential relationship between thyroid cancer risk and cigarette smoking and alcohol intake, with explicit consideration of confounders and potential interactions. The study's strengths include the use of representative data with minimal follow-up loss. Consistent findings in previous studies from other countries support the generalizability of our findings.
Previous studies have suggested the following possible mechanisms for the association between smoking and thyroid cancer: (1) potential lowering of thyroid-stimulating hormone (TSH) (24), which could be a growth factor for thyroid cancer (25,26); (2) potential lowering of BMI, which is a risk factor for thyroid cancer (27); and (3) a potential antiestrogen effect, with the understanding that estrogen may promote thyroid cancer development through estrogen receptor or vascular endothelial growth factor pathway signaling (28,29).
Smoking intensity or duration did not show any significant trend in the reduction of thyroid cancer risk in this study. In addition, the thyroid cancer risk of past smokers did not vary from that of nonsmokers in our study. The exact explanation for our findings remains unclear. Further quantitative research exploring smoking amount, duration, and the degree of durability of this risk reduction in thyroid cancer is necessary. Our findings suggest a less prominent effect of smoking in older patients, but there we observed no significant difference in the effect of smoking by sex. Our results conflict with those of previous studies, which suggested a nonsignificant age effect (5) or a prominent sex effect (1,2). Further research is needed to reconcile these differences.
Our results demonstrate an inverse association between thyroid risk and alcohol consumption, with a linear dose–response relationship noted according to alcohol frequency, amount consumed per occasion, and total weekly amount. Previous studies suggested possible mechanisms for this association, including decreased TSH levels (26), lower odds of thyroid peroxidase (TPO) antibodies associated with alcohol consumption (30,31), and the action of polyphenols (32,33). Our data suggested the observed inverse association was more prominent in older people and women.
We identified a submultiplicative interaction between smoking and alcohol intake on thyroid cancer risk, consistent with that of a pooled analysis by Kitahara et al. (5). This could be due to common underlying biological mechanisms, such as TSH or sex hormone levels (25,34).
We found no significant effect modification by income status on the association between smoking or alcohol consumption and thyroid cancer. Overdiagnosis of thyroid cancer has been reported in Korea (18,23). In Korea, thyroid cancer screening by ultrasonography is provided at the patient's own cost (approximately US$40–US$200) mainly through a private health screening program without a referral from primary care physicians. Most thyroid cancer cases (>99%) in Korea represent papillary thyroid cancers (23), and ∼95% of thyroid cancer cases are localized or regional disease according to the Surveillance, Epidemiology, and End Results (SEER) summary stage (35). As private health screening programs are mostly utilized by individuals with high income (35 –37), a group that generally is assumed to smoke and drink less, there is a possibility that income status could explain our observed inverse association.
However, in our study, an inverse association was consistently observed from the lowest income strata to the highest income strata with similar effect sizes. Our results suggest that the inverse association between smoking/drinking and thyroid cancer incidence may represent a true biological association, even though a significant portion of thyroid cancer cases may be overdiagnosed. An inverse association between smoking and thyroid cancer risk was previously observed in a previous Korean study of wealthy individuals who participated in private health screenings (2), as well as in a meta-analysis of epidemiologic studies from different regions with variable thyroid cancer screening practices (including where thyroid cancer screening in asymptomatic persons was rarely performed) (4).
There are multiple limitations of this study. First, we lacked data on TSH or thyroid peroxidase antibody levels. Second, we lacked data on educational attainment, which could be a potential confounder. Third, we did not collect data on thyroid cancer type, stage, genomic biomarkers, nor information on individual-level data on participation in screening for thyroid cancer. Fourth, self-reported smoking habits and alcohol consumption might be not accurate and are likely to be underestimated; we did not consider any change in smoking or drinking habits in this study. The inverse association of these exposures to thyroid cancer incidence could be less prominent if participants under-reported their smoking and alcohol consumption.
In conclusion, we observed an inverse association between the risk of thyroid cancer and smoking and alcohol consumption. A submultiplicative interaction between smoking and alcohol intake with the risk of thyroid cancer was also observed. However, it should be noted that smoking or alcohol usage should not be promoted as thyroid cancer prevention strategies, given that these lifestyle choices are associated with other serious health risks.
Footnotes
Authors' Contributions
Y.Y. contributed to study conception, design, and analysis. This author contributed to article preparation, writing, and editing. D.W.S. and K.H. planned this study, had access to the data, and took responsibility for the integrity of the data and data analysis. These authors contributed to study concept and design, analysis, and article preparation. D.K., S.C., S.M.J., and Y.M.S. contributed to study concept and design and analysis. T.K. contributed to interpretation of data and critically revised and approved the final article. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data