
Abstract
Background:
Active surveillance (AS) has been established as an alternative to immediate surgery for low-risk papillary thyroid microcarcinoma (PTMC). Nonetheless, it remains difficult to decide between AS and immediate surgery, since limited objective evidence exists regarding risks and benefits. The aim of study is to compare the cumulative costs of AS and immediate surgery.
Methods:
To estimate cumulative costs, a hypothetical model is simulated based on the Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Micro-Carcinoma (MAeSTro) study, a multicenter prospective cohort study of AS for PTMC. Direct and indirect costs are estimated from diagnosis to the treatment decision and follow-up for 10 years and a longer period. In the case of the scenarios, AS, AS to surgery due to changing their mind, and lobectomy (analyzed regardless of levothyroxine [LT4] treatment, as well as subdivided into lobectomy/LT4[−] and lobectomy/LT4[+]) are considered. A sensitivity analysis is performed using different discount rates to address uncertainties in future time costs. To compare the cumulative costs, we referred to previous research conducted in Hong Kong, the United States, and Japan.
Results:
The initial cost of AS is estimated to be 5.6 times lower than that of lobectomy (regardless of LT4 use), while the 10-year cumulative costs of AS ($2545) and lobectomy regardless of LT4 ($3045) are similar under a discount rate of 3%. However, in the long-term follow-up period, immediate surgery is going to be estimated more economical than AS. The costs of the two management approaches are similar in Hong Kong, but substantially different in the United States and Japan, implying that it could be affected by each country's national health insurance coverage and the thyroid ultrasound interval during follow-up.
Conclusion:
Considering both direct and indirect costs, the cumulative costs of AS and immediate surgery in low-risk PTMC patients are similar during 10 years, and surgery could be more economical for patients with a life expectancy in long-term follow-up. However, careful interpretation is needed for long-term follow-up and the country's health care system and environment. Nevertheless, considering the representative protocols and objective costs in South Korea, it is expected to be a key to suggest the appropriate treatment for PTMC patients.
Introduction
Papillary thyroid cancer (PTC) is the most common histologic subtype of thyroid cancer. The overall incidence of PTC has increased worldwide during the last three decades, especially that of papillary thyroid microcarcinoma (PTMC), which is defined as a 1 cm or smaller tumor (1,2). However, the rapidly increasing incidence of PTMC has not led to changes in morbidity or mortality rates; instead, its primary effect has been an increased socioeconomic burden.
A study analyzing the U.S. cancer statistics reported that the total medical costs of thyroid cancer substantially increased from 2010 ($1.4 billion) to 2019 ($2.38 billion) (3). These observations have raised the clinical question of whether immediate surgery should be performed for PTMCs. Due to the low disease progression rate, in 2015, the American Thyroid Association (ATA) discussed considering active surveillance (AS), defined as regular monitoring, as an alternative for low-risk PTMC patients without clinically evident metastases, local invasion, or cytological evidence of aggressive disease (4,5).
AS is now established as one of the standard management strategies for low-risk PTMC patients. Nonetheless, it remains difficult for patients to decide between AS and immediate surgery, although the medical indications for AS have been defined (6). An evidence-based tool has been developed to present the treatment options for PTMCs and facilitate optimal decision-making (7). However, the currently available evidence of clinical outcomes comparing AS versus immediate surgery is still limited because of the relatively short follow-up periods or retrospective design of previous studies (8,9). In addition, several economic evaluation studies that have compared AS and surgery only considered direct costs (10 –12). Therefore, determining the appropriate management for PTMC patients requires a detailed economic evaluation study considering the life-long socioeconomic burden based on representative costs between AS and immediate surgery (13).
If two interventions are equally effective, a cost-minimization analysis could be conducted to select a more economical intervention in a resource-limited environment (14). This is important in countries, such as South Korea, that operate a national health insurance system. As for effectiveness, recurrence, progression, and thyroid cancer-specific mortality rate can be considered in PTMC patients.
Therefore, the aim of study is to estimate the cumulative costs, including both direct and indirect costs, of AS and immediate surgery from the perspective of the South Korean health care system. A cost-minimization analysis is conducted for a 10-year follow-up, assuming that both AS and immediate surgery have equivalent effectiveness, and an additional simulation is conducted for 10–30 years of follow-up.
Materials and Methods
Standard treatment models for AS and immediate surgery
The standard treatment protocol of AS and immediate surgery is adopted from the Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Micro-Carcinoma (MAeSTro) study, a multicenter prospective cohort study of AS for PTMC comparing the long-term prognosis, quality of life, and medical costs between AS and immediate surgery in low-risk PTMC patients at three tertiary referral hospitals in South Korea
This study protocol was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1603-044-747). Supplementary Figure S1 demonstrates the standard clinical procedure for the diagnosis and treatment of PTMC under the MAeSTro protocol. The intervention selection between AS and surgery is made using a “decision-making node” (diagonal pattern) and a “chance node” for the type of immediate surgery. The scenarios used in this analysis are described below and they are constructed as a hypothetical model for economic evaluation. All processes of economic evaluation are reported according to the Consolidated Health Economic Evaluation Reporting Standards guideline 2022 (16).
Detailed scenarios of AS and immediate surgery
First visit to thyroid cancer diagnosis
At the first visit, diagnostic tests for thyroid cancer include thyroid ultrasonography (USG), USG-guided fine needle aspiration (FNA), and thyroid function tests (Supplementary Table S1). At the second visit, the diagnosis of PTMC is confirmed and as the third visit, patients are confirmed as having low-risk PTMC and decide on either AS or immediate surgery (Fig. 1). After thyroid cancer is diagnosed, this model is intended to simulate the follow-up period from 10 to 30 years. It is based on the peak-incidence age of thyroid cancer (the early 40s) (17) and the life expectancy of the world population (72.4 years in 2017 (18).
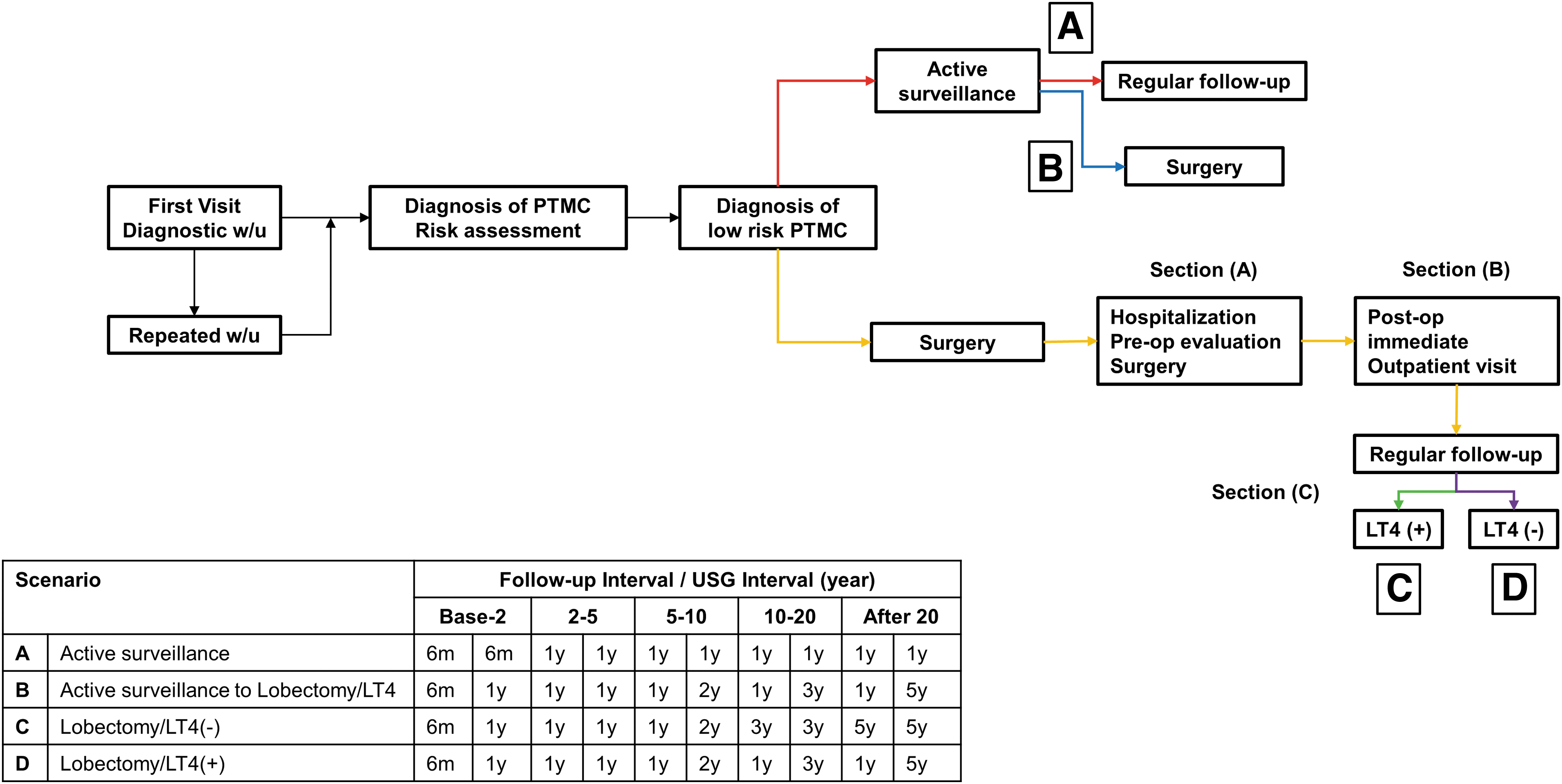
Detailed scenarios and follow-up interval between AS and surgery for cumulative cost estimation.
The detailed scenario of AS
In the case of AS group, it can be divided into two scenarios (Fig. 1). First, the AS group is followed every 6 months with USG at the initial 2 years, and then every year (Supplementary Table S2). In this scenario, thyroid function is included as a fixed direct cost along with USG. We hypothesized that AS patients may cross over to surgery due to the changing their mind.
In the MAeSTro data, about 19% of the initial AS group changed their mind and crossed over to surgery, and therefore, this is established as the additional scenario in the model. In MAeSTRo, the time period for crossover to occur is within 1.3 years, and the follow-up interval is thus set at 1-year intervals every year, and USG intervals are different according to the follow-up time (2–5 years, 1-year interval; 5–10 years, 2-year interval; 10–20 years, 3-year interval; 20 years later, 5-year interval, Fig. 1).
The detailed scenario of immediate surgery
For the immediate surgery group, it is divided into two scenarios. The first scenario is lobectomy, which did not treat with levothyroxine (LT4) during the follow-up and the second scenario is lobectomy, which treated with LT4. As detailed protocol, it is divided into three sections. The first section consisted of preoperative examination, hospitalization, and surgery. In the MAeSTro protocol, as preoperative risk assessment, blood test and laryngoscopy are conducted. With regard to hospitalization for surgery, the cost is estimated based on 4 days (Supplementary Table S3). Next, postoperative immediate and regular follow-up can be conducted in the surgery group (Supplementary Table S4). In the immediate follow-up, blood test and laryngoscopy could be conducted according to the clinical status, and as regular follow-up, thyroid function test, USG, and LT4 could be conducted. For LT4 treatment, we hypothesized a 50% probability of LT4 treatment, and the rationale of 50% is referred from the previous studies in Korea (19,20).
For the lobectomy/LT4(−) group, follow-up is performed at 6-month intervals for the first 2 years and at 1-year intervals for until 10 years. In addition, for 10–20 years and 20 years afterward, follow-up was regularly performed every 3 and 5 years, respectively (Fig. 1). For the lobectomy/LT4(+), follow-up is performed at 6-month intervals for the first 2 years and then at 1-year intervals thereafter. For all surgery groups, USG examinations are performed at 1-year intervals for the first 5 years and at 2-year intervals for the 5–10 years. After 10 years, USG examinations are performed every 3 and 5 years for the periods of 10–20 and 20–40 years, respectively (Fig. 1). In addition, the following major complications from surgery are considered (Supplementary Table S5): (1) postoperative hypoparathyroidism, (2) vocal cord palsy, and (3) wound problem (infection).
Cost estimation
For cost estimation, both direct and indirect costs are analyzed. To estimate direct medical costs, both outpatient and inpatient medical expenses are calculated based on the 2017 publication of the Health Insurance Review and Assessment Service (HIRA) (21). As direct nonmedical costs, round trip transportation costs are calculated by reflecting the consumer price index of the transportation sector based on the Korean National Health and Nutrition Examination Survey in 2005 (22). For indirect costs, the loss of productivity corresponding to time spent in the hospital is estimated. Time spent on outpatient visits, including the waiting time, is calculated based on the National Medical Care Resources and Utilization Survey in 2000 (23).
For the immediate surgery group, the length of the in-hospital stay is set to 4 days. Productivity loss is calculated as the average wage of workers from Statistics Korea in 2017 (24) corresponding to the time spent in the hospital. All costs are calculated in Korean Republic won (KRW) and converted into United States dollars (USD) by applying the exchange rate of 1 USD to 1143 KRW (June 30, 2017) (25).
To calculate the cumulative costs, a discount rate—an interest rate used to determine the present value of future cash flows—is applied (26). A discount rate of either 3% or 5% is used based on previous studies, and 5% corresponds to the current HIRA guidelines (27). A sensitivity analysis is conducted to assess the uncertainty that may arise during the economic evaluation. We also compared cumulative costs with previous PTMC studies, which only analyzed the direct costs of AS and immediate surgery. The previous studies used a hypothetical model of a 40-year-old patient with low-risk PTMC and compared only direct medical costs for 10 or 20 years between the AS and immediate surgery groups. In the U.S. and Hong Kong studies, direct medical costs are estimated using literature reviews and Medicare reimbursement from the Centers for Medicare and Medicaid Service data (11,12).
In a Japanese study, direct medical costs for 10 years are calculated for all PTMC patients who visited one hospital (10).
Results
Cost estimation: from first visit to thyroid cancer diagnosis
In the period from diagnosis to the decision of treatment, direct medical cost items include outpatient medical consultation fees, thyroid function tests, thyroid USG, FNA, and cell block with liquid aspiration (Supplementary Table S1). The estimated direct medical costs in this phase are $208 (Table 1). The direct nonmedical costs for transportation and the indirect costs are $52 and $44 for two visits with basic examinations, respectively. Finally, the sum is $304 (Table 1).
Estimated Cost Description from the Scenarios from the MAeSTro Study
The cost was set as the standard cost by the Korea HIRA in 2017 using Korean currency and converted it USD (1$, 1143 won).
Cumulative cost was estimated under discount rate (3%).
Ultrasound was conducted differently for each period under FU period (until 5 years, annually; 5–10 years, biannually; every 3 years; 20–40 years every 5 years).
AS, active surveillance; FU, follow-up; HIRA, Health Insurance Review and Assessment Service; LT4, levothyroxine; MAeSTro, Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Micro-Carcinoma; USG, ultrasonography.
Cost estimation for AS and immediate surgery
After the treatment decision for low-risk PTMC, subjects are classified into the AS or the immediate surgery group. Under the MAeSTro protocol, the fixed direct cost for the AS group at each follow-up point is $86 (Table 1). This cost includes thyroid USG, thyroid function tests, and the outpatient medical consultation fee (Supplementary Table S2). The total sum of each visit of the AS group is $134. Those who changed their mind from AS to surgery are assumed to have two visits as part of the AS protocol, and after that are followed as per the surgical group protocol.
In the immediate surgery group, total costs are divided into three stages. Stages (A) and (B) correspond to the process of the surgical treatment, and stage (C) is the regular follow-up (Fig. 1). In stage (A), preoperative examination, hospitalization, and surgery would be conducted, and the sum of the direct costs is $773 for lobectomy (Table 1). Supplementary Table S3 summarizes the detailed items related to the examinations for preoperative risk assessment, hospitalization, and surgery, and their costs. Stage (B) includes immediate visits to confirm the postoperative pathologic diagnosis and check for surgical complications, as well as long-term regular follow-up. During this stage, the total cost is $66 (Table 1 and Supplementary Table S4).
In the regular follow-up visits, each surgery group is associated with differing costs, according to LT4 treatment and USG examination. The regular follow-up visit costs for the lobectomy with the USG group are $134 (non-LT4) and $145 (LT4 treatment) (Table 1 and Supplementary Table S4). If complications occur, an additional one to three visits to medical institutions and treatments are assumed. For postoperative hypoparathyroidism, calcium, active vitamin D treatment, and blood test for calcium and phosphorus are needed (Supplementary Table S5). For vocal cord palsy, laryngoscopy is additionally needed. For wound problems, detailed treatments such as (1) wound dressing, (2) USG neck aspiration, and (3) wound suture will be conducted depending on the type of problem.
Cumulative cost comparison between AS and immediate surgery
In the 10-year follow-up, the cumulative costs between AS and immediate surgery do not differ substantially (AS: discount rate 0%, $2323; 3%, $2545; 5%, $2712; lobectomy [regardless of LT4]: discount rate 0%, $2958; 3%, $3045; 5%, $3145). With no discount rate, the curve of the AS crosses that of lobectomy (regardless of LT4) at 22 years (Fig. 2A). With a discount rate of 3%, the corresponding cross-point is found at 17 years (Fig. 2B), and with a discount rate of 5%, it is found at 15 years (Fig. 2C). In the case of AS to surgery, the 10-year cumulative cost is $3108 (discount rate 0%), $3245 (discount rate 3%), and $3347 (discount rate 5%).
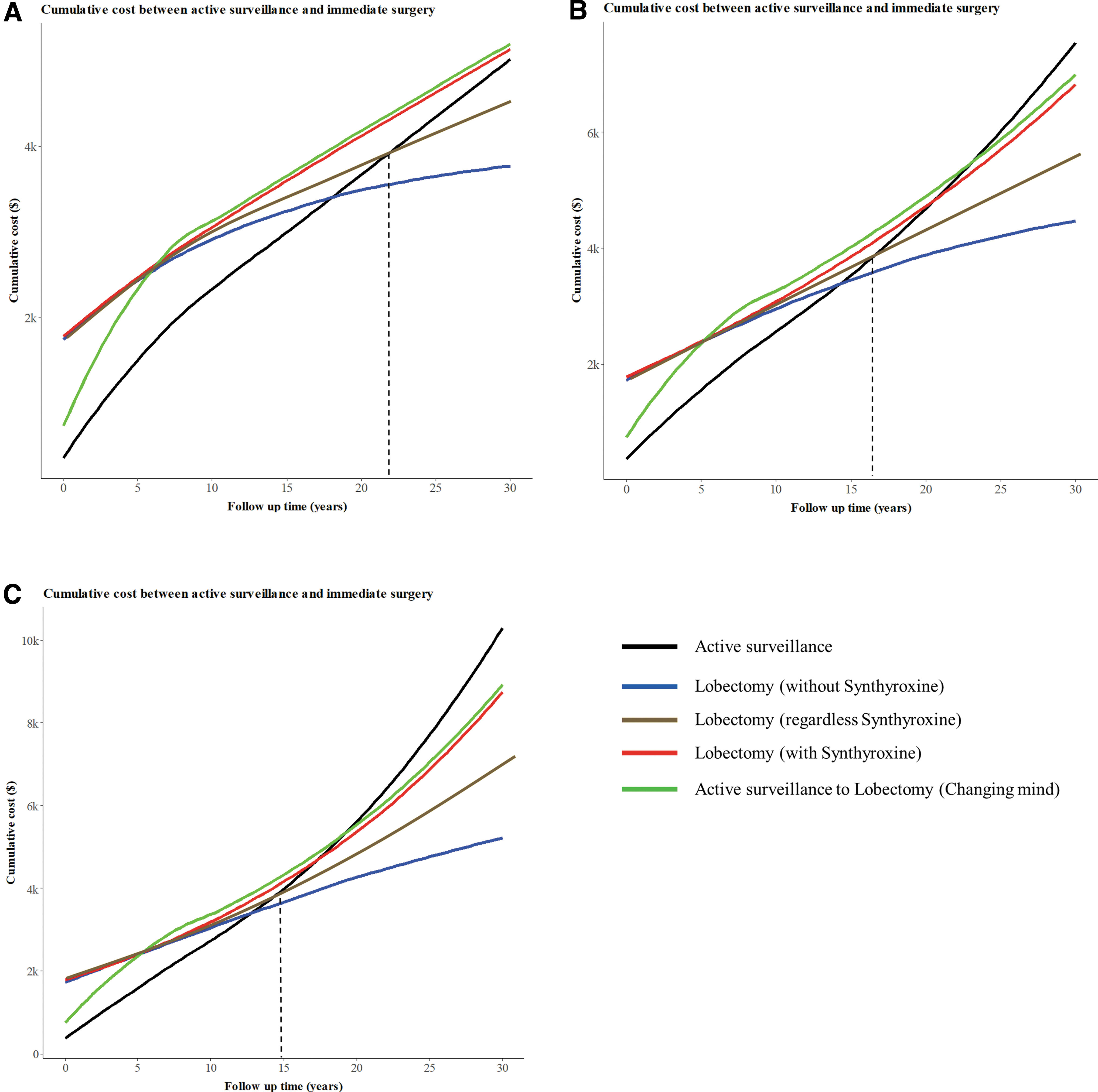
Cumulative cost between AS and immediate surgery group. (
We also compared the estimated costs of AS and immediate surgery with previous studies from other countries (Table 2) (10 –12). The cumulative 20-year cost is $6678 for AS and $7377 for surgery in Hong Kong, and $5724 and $13866 for surgery in the United States. In Japan, the cumulative 10-year costs of AS are $1525 (for no recurrence) and $2052 (for recurrence), and those of surgery are $7225–$8616 (for no recurrence) and 8437 (for recurrence). The costs of AS in South Korea estimated in this study are 1.84 times lower than those in Hong Kong and 1.89 times lower than those reported by the U.S. study.
Comparative Summary of 10- and 20-Year Follow-Up Costs of Active Surveillance in Thyroid Cancer
Examination costs derived from ultrasound, thyroid function test, fine needle aspiration, computer tomography, blood test [Kim et al. (13)], ultrasound [Lang and Wong (11)], and ultrasound, blood test, outpatient consultation [Venkatesh et al. (12)]; The costs of treatment include costs from lobectomy [Kim et al. (13), Venkatesh et al. (12)] and lobectomy/central node dissection [Lang and Wong (11)]. The costs of hospitalization include costs from hospitalization room and meals. The costs of complication include the costs from vocal cord palsy, hypoparathyroidism, hematoma formation, and chyle leakage.
Won to dollar exchange rate: using dollar = won/1143 and yen to dollar exchange rate: using dollar = yen × 0.009.
Changed to surgery from AS during the FU.
NR, not reported; PTMC, papillary thyroid microcarcinoma.
Discussion
In this study, the cumulative costs of AS and immediate surgery for the treatment of low-risk PTMC are estimated in a cost-minimization analysis considering life expectancy. A hypothetical model of a 40-year-old low-risk PTMC patient with a 10-year follow-up period is simulated based on both direct and indirect costs. Additional costs are also estimated from 10 to 30 years. With a 10-year follow-up time, the cumulative costs of AS and immediate surgery are similar, but when follow-up is extended longer, immediate surgery seemed to be more economical.
We compared our findings with those of previous economic evaluation studies based on direct costs (examinations, surgery, and hospitalization) for AS and lobectomy in 40-year-old low-risk PTMC patients (11,12). In the Hong Kong study, the cost of surgery is 1.1 times higher than that of AS, with a cost difference of only $700 (i.e., $35 per year) (11). However, in the U.S. study, surgery is 2.4 times more expensive than AS (12). In the Japanese study, which is based on 10 years of follow-up at one institution, surgery is 4 times more expensive than AS (10). However, this study found that the cost of lobectomy (regardless of LT4) is 1.06 times lower (discount rate, 3%) or 1.09 times (discount rate, 5%) lower than AS during a 20-year follow-up.
The discrepancy between the present study and previous research may be due to differences between countries in the initial cost of surgery, insurance coverage from the national health care system, and the timing of USG. For example, in the United States and Japan, the USG follow-up interval is 1 year, but in Hong Kong, it is every 6 months (10 –12).
Despite the findings of this study, in terms of cost minimization, other considerations should be kept in mind regarding the choice of management for PTMC patients under limited resources. Patients who receive AS may suffer anxiety and fear due to the nonremoval of thyroid cancer, while those who undergo surgery may experience difficulty in swallowing, the discomfort of the surgical wound, and a weak voice (28,29). Second, the severity of the patients' condition should be considered in relation to their quality of life and costs. Patients who develop surgical hypothyroidism require LT4 treatment, which may be associated with poor quality of life and imposes additional costs (30). Third, as suggested in this study, the follow-up period should also be considered, because surgery is more economical than AS in patients who will receive long-term follow-up.
Lastly, individual economic circumstances and the country's health insurance system must be considered due to the differing treatment costs (31).
Considering the characteristics, trends, and the current status of PTMC in each country, it is necessary to consider robotic surgery as the standard treatment in PTMC patients. Although robotic surgery was introduced to South Korea in 2007, it still requires higher costs than other surgical treatments. It is a big burden on patients from an economic perspective. Despite the high cost, many patients have been choosing robotic surgery due to the low complication incidence and improved quality of life. However, compared with other surgical treatments, robotic surgery lacks evidence as a standard treatment, and so, a detailed evaluation through cost-effectiveness or cost-utility analysis is necessary.
In addition, an understanding of the country's health care system or environment is needed. In Korea, more than 90% of medical institutions perform thyroidectomy in general hospitals (32). Accordingly, many patients require hospitalization for thyroidectomy. In addition, the proportion of radioactive iodine therapy among the overall thyroid cancer patients who are surgically treated patients has been gradually decreasing since the late 2000s, until reaching 62% in 2012. It is understood that overdiagnosis of thyroid cancer may be a contributing factor (32). Thyroid cancer overdiagnosis may be suspected for tumor size, which is <0.5 cm (33,34). Compared to the past, 16% of the surgery group and 26% of the AS group had a tumor size of less than 0.5 cm. Therefore, suspected overdiagnosis of PTMC patients appears to be decreasing compared with the past.
In South Korea, thyroid surgery requires 4 days of hospitalization, but in the United States or some other countries, it is performed as an outpatient procedure or is subject to 1 day of hospitalization. Some tests utilized in this study are not concordant with the current ATA Differentiated Thyroid Cancer guidelines (4,35) (routine computed tomography imaging, biopsy of subcentimeter thyroid nodules, and some preoperative diagnostic tests). Also, there is a medicolegal consideration, because AS is not a definite standard alternative treatment compared with surgery in all countries.
This study has some limitations. First, the costs of AS and surgery are different across medical institutions and health care delivery systems; furthermore, postoperative maintenance (e.g., complementary and alternative medical treatment/procedures) may vary (36). However, we could not directly consider those factors in this study. As further analysis, research on our cohort of thyroid cancer patients (37) it will be possible to accurately investigate costs including postoperative maintenance. Second, when only costs are analyzed, AS is observed to be more economical, in accordance with previous studies, but the cost-utility analysis found surgery to be more cost-effective than AS (10,11).
Additional economic evaluations such as cost-effectiveness and cost-utility analyses considering quality adjusted life year, disability-adjusted life years, and health behaviors should be conducted. Although cost uncertainty is estimated based on the discount rate, there would be cost variation in the long-term follow-up period, and so, careful interpretation is needed. The risk of secondary clinical outcome (e.g., death and other diseases related to thyroid cancer) according to age based on MAeSTro data is not included in this study due to the need for long-term follow-up. Therefore, we are preparing a further economic evaluation study to assess the risk of noncancer and old-age mortality rates based on long-term follow-up data.
Despite these limitations, there are some strengths of this study. First, the economic burden of thyroid cancer throughout the world would be expected to rise steadily due to its high incidence and good prognosis (38). In this context, this study proposes management strategies for thyroid cancer patients based on their life expectancy and their economic status. Second, unlike previous studies, we considered both direct and indirect costs with a much larger sample (39). Furthermore, the costs and protocols are representative because the estimations are made according to the standard clinical treatment flow of PTMC considering life expectancy. Although lobectomy is assumed when calculating the costs of surgery in other studies, we also estimated the costs considering lobectomy both with and without LT4, as well as total thyroidectomy.
Another strength is that while other studies estimated the cost based on 10 or 20 years of follow-up (10 –12), we estimate the costs with long-term follow-up (up to 30 years), assuming that patients diagnosed with thyroid cancer at 40 years of age may normally survive until 70 years of age. Because PTMC has a good prognosis, survival for longer than 10 or 20 years is routine, and longer survival and follow-up periods may lead to higher costs (39).
There is no significant difference in the cost of AS and immediate surgery based on direct and indirect costs for 10 years in Korea, whereas immediate surgery is found to be more economical for PTMC patients requiring long-term follow-up. Therefore, it would be desirable to make a clinical judgment by integrating other information such as the patient's clinical condition and preferences when choosing between surgery and AS. Our results suggest that the identification of a more economical disease management strategy may depend on the patient's life expectancy, which impacts the expected follow-up period. However, it is necessary to interpret these findings carefully, due to the known differences in the health care systems according to the country, cost value, and variations in the long-term follow-up period. Our findings may be utilized to provide resource allocation information for medical providers or health policy makers regarding PTMC management options.
Footnotes
Authors' Contributions
Study design: E.K.L., J.H.M., Y.J.P., and S.K.P. Data acquisition: J.Y.C., S.K., E.K.L., Y.K.L., J.S.R., K.E.L., Y.J.P., and S.W.C. Data analysis: K.K. and S.W.C. Data interpretation: K.K., S.K., E.K.L., Y.J.P., S.W.C., and S.K.P. Drafting the article and critical review of revisions: K.K., Y.J.P., S.W.C., and S.K.P. Final approval to submit: K.K., S.W.C., Y.J.P., and S.K.P. Obtaining funding: E.K.L., J.H.M., Y.J.P., and S.K.P.
Acknowledgment
We would like to express our gratitude to Hojoon Sohn (Professor of Department of Preventive Medicine, Seoul National University College of Medicine), for giving some advice in presenting the methodology and description of the economic evaluation study.
Author Disclosure Statement
No potential conflict of interest relevant to this article is reported.
Funding Information
This research is supported by a grant of the Patient-Centered Clinical Research Coordinating Center funded by the Ministry of Health & Welfare, Republic of Korea (grant Nos. HI19C0481, HC19C0103).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5