
Abstract
Background:
Thyroiditis and Graves' disease have been reported after coronavirus disease 2019 (COVID-19) vaccination. We evaluated the risks of adverse events after COVID-19 vaccination among patients treated for hypothyroidism.
Methods:
In this retrospective population-based cohort study of Hong Kong Hospital Authority electronic health records with the Department of Health vaccination records linkage, levothyroxine (LT4) users were categorized into unvaccinated, vaccinated with BNT162b2 (mRNA vaccine), or CoronaVac (inactivated vaccine) between February 23, 2021, and September 9, 2021. Study outcomes were dosage reduction or escalation in LT4, emergency department (ED) visit, unscheduled hospitalization, adverse events of special interest (AESI) according to the World Health Organization's Global Advisory Committee on Vaccine Safety, and all-cause mortality. Inverse probability of treatment weighting for propensity score was applied to balance baseline patient characteristics among the three groups. Hazard ratios (HR) were estimated using Cox regression models. Patients were observed from the index date until the occurrence of study outcome, death, or censored on September 30, 2021, whichever came first.
Results:
In total, 47,086 LT4 users were identified (BNT162b2: n = 12,310; CoronaVac: n = 11,353; and unvaccinated: n = 23,423). COVID-19 vaccination was not associated with increased risks of LT4 dosage reduction (BNT162b2: HR = 0.971 [confidence interval; CI 0.892–1.058]; CoronaVac: HR = 0.968 [CI 0.904–1.037]) or escalation (BNT162b2: HR = 0.779 [CI 0.519–1.169]; CoronaVac: HR = 0.715 [CI 0.481–1.062]). Besides, COVID-19 vaccination was not associated with a higher risk of ED visits (BNT162b2: HR = 0.944 [CI 0.700–1.273]; CoronaVac: HR = 0.851 [CI 0.647–1.120]) or unscheduled hospitalization (BNT162b2: HR = 0.905 [CI 0.539–1.520]; CoronaVac: HR = 0.735 [CI 0.448–1.207]). There were two (0.016%) deaths and six (0.062%) AESI recorded for BNT162b2 recipients, and one (0.009%) and three (0.035%) for CoronaVac recipients, respectively.
Conclusions:
BNT162b2 or CoronaVac vaccination is not associated with unstable thyroid status or an increased risk of adverse outcomes among patients treated for hypothyroidism in general. These reassuring data should encourage them to get vaccinated against COVID-19 for protection from potentially worse COVID-19-related outcomes.
Introduction
As of November 1, 2021, coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has infected nearly 250 million people globally and resulted in more than 5 million deaths (1). The inter-relationship between thyroid disease and COVID-19 has been increasingly observed, such as SARS-CoV-2-related subacute thyroiditis and the occurrence of nonthyroidal illness syndrome in COVID-19 (2,3). Hypothyroidism is a common condition worldwide, with the prevalence of overt hypothyroidism estimated to be 0.2–5.3% (4). Hashimoto's thyroiditis is the most probable etiology of primary hypothyroidism (5). There are suggestions that hypothyroidism is associated with worse prognosis in COVID-19 patients, (6) which may be explained by the possible role of thyroid hormones in the immune system (7). Vaccination against SARS-CoV-2 may enhance population immunity and protection against COVID-19 hospitalization and mortality. COVID-19 vaccines, developed based on different technology platforms, have shown efficacy in reducing severe COVID-19 (8).
The thyroid gland is a potential target of attack by SARS-CoV-2 because of the expression of angiotensin converting enzyme 2, the entry receptor for SARS-CoV-2 (9). Cases of subacute thyroiditis and Graves' disease have been described among infected patients (2). Similar concerns have been raised regarding the potential of COVID-19 vaccination in inducing thyroid dysfunction, as evidenced by case reports of subacute thyroiditis (10) and Graves' disease (11) occurring after COVID-19 vaccination. These concerns are amplified by the fact that this is the first time that any mRNA vaccine has been approved for human use. Patients with hypothyroidism due to various etiologies may be at risk of these thyroid-specific outcomes.
Recently, we have also reported a patient who developed Graves' disease after COVID-19 vaccination on a background of eight-year history of hypothyroidism requiring levothyroxine (LT4) replacement (12). Moreover, patients who have undergone radioactive iodine or thyroidectomy to an extent less than total thyroidectomy may still have normal thyroid tissue, thus potentially at risk of thyroid-specific outcomes after COVID-19 vaccination. Currently, the Hong Kong Government vaccination program provides two authorized COVID-19 vaccines: CoronaVac (inactivated whole-virus vaccine) and BNT162b2 (mRNA vaccine). It is time to conduct a population-based cohort study to systematically evaluate whether COVID-19 vaccines are associated with increased risks of adverse events, focusing on the at-risk group of patients treated for hypothyroidism.
Materials and Methods
Data source
This retrospective cohort study used linked data, a collaboration between the Department of Health (DH) of Hong Kong with anonymized, population-wide COVID-19 vaccination records and the Hong Kong Hospital Authority (HA) with electronic medical records (EMRs) of patients. HA provides health care services to a population of more than 7.47 million through 42 public hospitals and institutions, specialist outpatient clinics (SOPCs), and general outpatient clinics (13). Centralized medical records are generated during public health care services, including demographics, date of registered death, drug dispensing records, diagnoses, procedures, and laboratory tests. Thyroid diseases are managed by the HA SOPCs. HA prescriptions can only be dispensed by HA pharmacies.
Vaccination records of all Hong Kong residents included the date of administration and the type of vaccine. This vaccine safety data linkage has been widely used to conduct population-based pharmacovigilance studies of COVID-19 vaccines on Bell's palsy, arthritis flare-up, myo-/pericarditis and whether patients with various diseases are at a higher risk of experiencing adverse events (14 –18).
The study protocol was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 21-149 and UW 21-138) and the Department of Health Ethics Committee (LM 21/2021). Informed patient consent was not required as the data used in this study were anonymized.
Study design and population
The study cohort included all adults (age 18 years or older) who were LT4 users, continuously for at least three months, at the time of the first-dose vaccination (for the vaccinated group) and at the pseudoindex date (for the unvaccinated group) between February 23, 2021, and September 9, 2021 (inclusive).
We identified all LT4 prescriptions by the British National Formulary (BNF) code 6.2.1 and drug names from EMRs. The daily reference dosage was defined as the daily dosage of LT4 in the most recent prescriptions before the index dates. Patients were excluded if none of their prescription records (except the most recent prescriptions before the index dates) had the same daily dosage value as the daily reference dosage in the three months before the index dates. Patients who had been prescribed antithyroid drugs in the three months before the index date were excluded as these were likely patients treated for hyperthyroidism using a block-and-replace regimen.
Patients with thyroid cancer were also excluded as patients with differentiated thyroid cancer require thyroid hormone suppressive therapy with different target thyrotropin (TSH) levels from patients without thyroid cancer, and different targets according to risk categories of the thyroid cancer (19). The data linkage and selection procedure are shown in Figure 1.
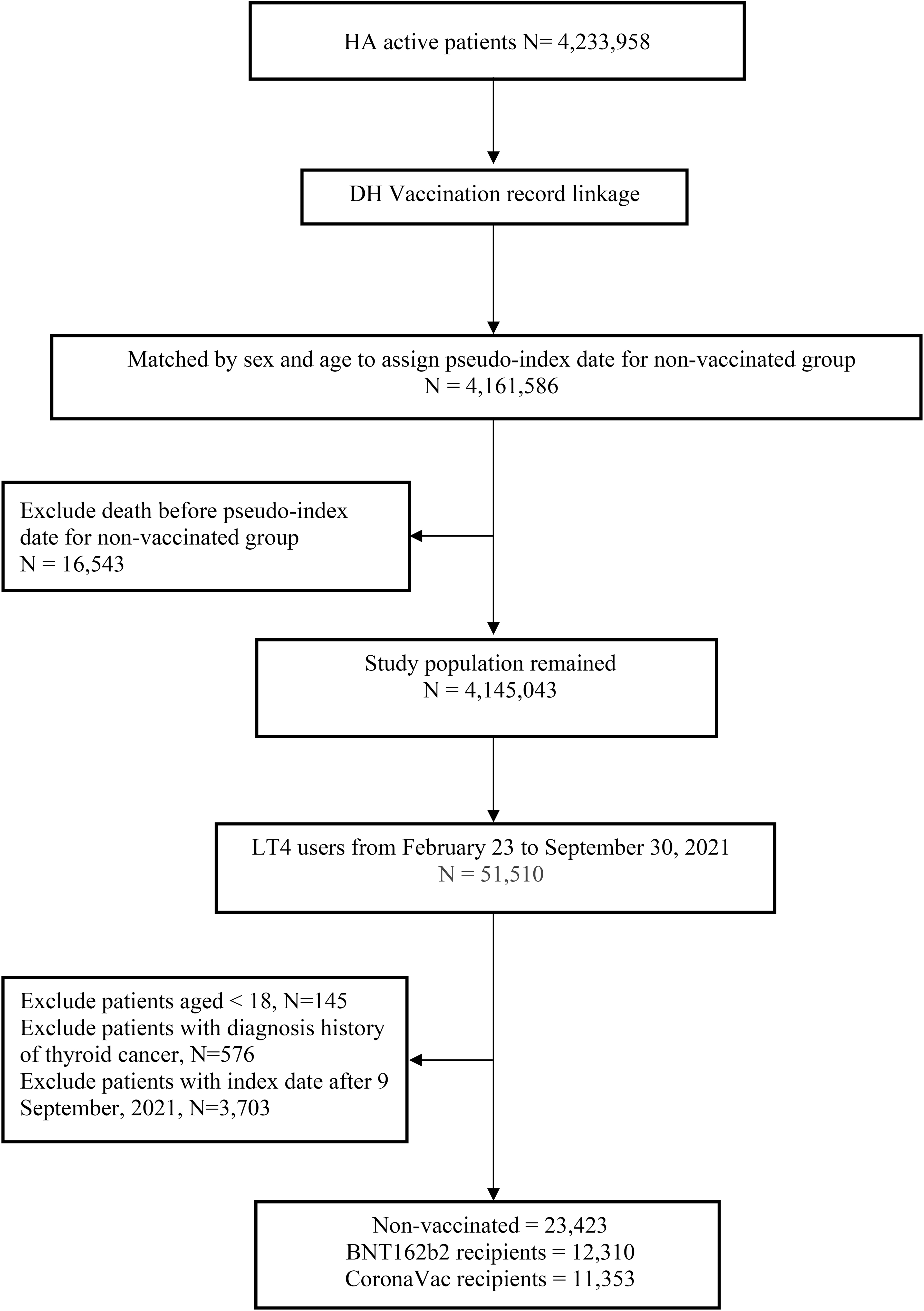
Flowchart of record linkage and selection procedures for LT4 users from February 23, 2021, to September 9, 2021, in Hong Kong. The figure shows record linkage and selection procedure for LT4 users from February 23, 2021, to September 9, 2021, in Hong Kong. After applying the inclusion and exclusion criteria, there were 47,086 LT4 users eligible for inclusion. A total of 23,423 did not receive vaccination, 12,310 received the BNT162b2 vaccine, and 11,353 received the CoronaVac vaccine. LT4, levothyroxine.
The index date was defined as the date of first-dose vaccination for the vaccinated people or the assigned pseudoindex date for the unvaccinated people. The follow-up for each patient commenced from the index date until the outcome occurrence, death, or end of the study period (September 30, 2021), whichever came first.
Outcome definition
The primary outcomes were the following thyroid-specific outcomes: (1) dosage reduction in LT4 and (2) dosage escalation in LT4. Dosage reduction in LT4 was chosen in view of case reports of subacute thyroiditis (10) and Graves' disease (11) after COVID-19 vaccination presented as thyrotoxicosis, where dosage reduction would imply a thyrotoxic state. Dosage reduction in LT4 was defined as a decrease in the daily dosage after the index date when compared with the daily reference dosage. On the contrary, dosage escalation in LT4 was chosen in view of case reports of Hashimoto's thyroiditis after COVID-19 (20), where dosage escalation would imply a hypothyroid state. Dosage escalation in LT4 was defined as an increase in the daily dosage after the index date when compared with the daily reference dosage.
The secondary outcomes were emergency department (ED) visits, unscheduled hospitalizations (admission through ED) 21 days after the index date, adverse events of special interest (AESI) resulting in hospitalization or specialist outpatient visit, and all-cause mortality. Unscheduled hospitalization was identified by ED visits, which required subsequent hospitalization for urgent diagnostic workup and in-patient management. Patients hospitalized at index date were excluded from the analysis of ED visits and unscheduled hospitalization. AESI have been widely used for the safety surveillance of COVID-19 vaccines, defined by the WHO Global Advisory Committee on Vaccine Safety (21). The Hong Kong Government has adopted these AESI for the pharmacovigilance program of COVID-19 vaccines. The list of AESI investigated in this study is shown in Supplementary Table S1. Each AESI was defined by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9) Diagnosis and Procedure codes, and the International Classification of Primary Care (ICPC).
Propensity score weighting
The propensity score (PS) was estimated by multinomial logistic regression to predict the probability of a patient receiving one type of COVID-19 vaccine or not getting vaccinated using covariates: demographics including age and sex, history of COVID-19 (positive SARS-CoV-2 polymerase chain reaction results), health care utilization, comorbidities (Charlson comorbidity index, medical history of myocardial infarction, peripheral vascular disease, cerebrovascular disease, chronic obstructive pulmonary disease, dementia, paralysis, diabetes with/without chronic complication, chronic renal failure, mild/moderate-severe liver disease, ulcers, and cancer), baseline TSH level (within the 6 months before the index date), and recent use (within the 90 days before the index date) of the renin-angiotensin-aldosterone system inhibitors, beta blockers, calcium channel blockers, diuretics, nitrates, lipid-lowering agents, antidiabetic drugs, antiepileptic drugs, antidepressants, nonsteroidal anti-inflammatory drugs (NSAIDs), drug for gout, and antibiotics.
Inverse probability of treatment weighting (IPTW) using the PS was applied, followed by truncation of 1st and 99th percentiles of the observed PS weighting distribution to account for extreme weights (22). The maximum absolute standardized mean difference was used to assess the difference in each covariate among the three groups, of which a value of less than 0.2 was considered acceptable (23).
Statistical analyses
Descriptive statistics of the baseline characteristics among unvaccinated people, and BNT162b2 and CoronaVac recipients before and after PS weighting were presented as proportions for categorical variables, and means with standard deviations (SDs) for continuous variables. IPTW-weighted Cox regression models were fitted to estimate the hazard ratios (HR) and corresponding confidence intervals [CIs] of dosage reduction in LT4, dosage escalation in LT4, ED visits, and unscheduled hospitalization among the three groups, in which the unvaccinated group was treated as a reference group. Separate models were conducted to assess risk of outcomes by subgroups (age <65 years vs. ≥65 years, sex, and prevaccination thyroid status). A two-sided significance level of p < 0.05 was considered statistically significant. To account for multiple testing for subgroups, Bonferroni correction was used, and so, the results were considered statistically significant if p < 0.05/56 (number of subgroup analysis) = 0.0009 (24).
All statistical analyses were performed using the STATA Version 16.0 (StataCorp LP, College Station, TX, USA).
Results
Baseline characteristics
We obtained 4,233,958 records of HA active patients with affirmed vaccination status from February 23, 2021, to September 30, 2021 (Fig. 1). Among 47,086 LT4 users eligible for inclusion, 23,423 did not receive vaccination, 12,310 received the BNT162b2 vaccine, and 11,353 received the CoronaVac vaccine. Comparing with the 23,423 unvaccinated individuals, both BNT162b2 and CoronaVac vaccine recipients were younger (age—BNT162b2: 55.2 ± 13.4 years, CoronaVac: 59.9 ± 11.7 years; unvaccinated: 66.6 ± 15.3 years [p < 0.001 vs. BNT162b2 and CoronaVac, respectively]) and less likely to have preexisting medical comorbidities overall. There were 84 COVID-19 survivors, more than half of them were vaccinated (BNT162b2: 0.3% [37]; CoronaVac: 0.1% [16]; unvaccinated: 0.1% [31]). After PS weighting, all baseline characteristics had standardized differences of less than 0.2 (Table 1 and Supplementary Table S2), implying a balance of covariates among the three groups. The mean baseline daily dosages of LT4 (SD) were 76.7 (26.8), 81.5 (25.4), and 80.2 (24.5) mcg among the unvaccinated, and the BNT162b2, and CoronaVac groups, respectively.
Baseline Characteristics of Levothyroxine Users Who Were Unvaccinated, Received BNT162b2 or CoronaVac Vaccine from February 23, 2021, to September 9, 2021, in Hong Kong SAR, China
ASMD, maximum absolute standardized mean difference; COVID-19, coronavirus disease 2019; ED, emergency department; NSAID, nonsteroidal anti-inflammatory drug; SD, standard deviation; TSH, thyrotropin.
Thyroid-related outcomes following vaccination
Regarding dosage reduction in LT4, there were 2357 (19.1%) cases among BNT162b2 recipients (before weighting: incidence of 913 per 1000 person-years) with a median follow-up of 66 days (IQR: 45–98), and 2280 (20.1%) cases among CoronaVac recipients (before weighting: incidence of 875/1000 person-years) with a median follow-up of 72 days (IQR: 48–105). When compared with unvaccinated individuals, receiving the first dose of BNT162b2 (median time to dosage reduction in LT4: 51 days vs. 44 days, HR 0.971 [CI: 0.892–1.058], p = 0.503) or CoronaVac (median time to dosage reduction in LT4: 56 days vs. 44 days, HR 0.968 [CI: 0.904–1.037], p = 0.349) was not associated with an increased likelihood of dosage reduction of LT4 (Table 2).
Cumulative Incidence and Incidence Rate of Dosage Reduction/Escalation of Levothyroxine, Emergency Department Visits, and Unscheduled Hospitalization for People Who Were Unvaccinated, Received BNT162b2 or CoronaVac Vaccine, and Hazard Ratio of Events for BNT162b2 or CoronaVac in Comparison with Unvaccinated People
Unvaccinated group was treated as reference category.
CI, confidence interval; HR, hazard ratio; LT4, levothyroxine.
Regarding dosage escalation in LT4, there were 138 (1.1%) cases among BNT162b2 recipients (before weighting: incidence of 47/1000 person-years) with a median follow-up of 76 days (IQR: 51–111), and 134 (1.2%) cases among CoronaVac recipients (before weighting: incidence of 45/1000 person-years) with a median follow-up of 84 days (IQR: 55–118) before weighting. When compared with unvaccinated individuals, receiving the first dose of BNT162b2 (median time to dosage escalation in LT4: 54 days vs. 52 days, HR 0.779 [CI: 0.519–1.169], p = 0.228) or CoronaVac (median time to dosage escalation in LT4: 64 days vs. 52 days, HR 0.715 [CI: 0.481–1.062], p = 0.097) was not associated with an increased likelihood of dosage escalation of LT4 (Table 2).
Health care utilization, AESI, and all-cause mortality following vaccination
We did not observe increased likelihood of unscheduled health care utilization among the vaccinated group compared with the unvaccinated group: ED visits (BNT162b2: HR 0.944 [CI: 0.700–1.273], p = 0.708; CoronaVac: HR 0.851 [CI: 0.647–1.120], p = 0.249); unscheduled hospitalization (BNT162b2: HR 0.905 [CI: 0.539–1.520], p = 0.707; CoronaVac: HR 0.735 [CI: 0.448–1.207], p = 0.224) (Table 2).
Five (0.041%) cases of Hashimoto's thyroiditis, five (0.041%) cases of Graves' disease, two (0.016%) deaths, and six (0.062%) AESI (two cases of narcolepsy, two cases of Bell's palsy, one case of arrhythmia, and one case of anaphylaxis) were observed among BNT162b2 recipients. Meanwhile, one (0.009%) case of Hashimoto's thyroiditis, three (0.026%) cases of Graves' disease, one (0.009%) death, and three (0.035%) AESI (one case of hemorrhagic disease, one case of Bell's palsy, and one case of narcolepsy) were identified among CoronaVac recipients. In comparison, 10 (0.043%) cases of Hashimoto's thyroiditis, 15 (0.064%) cases of Graves' disease, 155 (0.662%) deaths, and 26 (0.202%) AESI were observed among unvaccinated individuals. There was no report of subacute thyroiditis after vaccination.
Subgroup analyses
We repeated the analyses stratifying the groups according to age, sex, and prevaccination thyroid status, which were largely consistent with the main analysis (Supplementary Table S3).
Discussion
To our knowledge, our current study represents the first to evaluate the safety of COVID-19 vaccination specifically among patients treated for hypothyroidism. Results showed that the COVID-19 vaccination, with either CoronaVac or BNT162b2, was not associated with a higher likelihood of dosage reduction or escalation in LT4, suggesting that COVID-19 vaccination did not lead to instability in thyroid status. Furthermore, we provided reassuring real-world data to clarify potential safety concerns by showing that unscheduled ED visits or hospitalizations did not increase after COVID-19 vaccination among patients treated for hypothyroidism.
In this study, vaccine recipients were observed to be younger and less likely to have preexisting comorbidities. This observed difference did not stem from a specific regulation of the vaccine campaign. In fact, elderly patients with medical comorbidities are encouraged to receive COVID-19 vaccines to protect themselves from COVID-19-related morbidities (25). Nevertheless, in the early phase of the vaccine campaign, people with chronic illness were less willing to receive COVID-19 vaccines (17), which may be due to their concerns about the potential side effects, as illustrated in a study in Hong Kong that family doctors were less likely to recommend COVID-19 vaccines to patients given their worry about vaccine side effects on chronic illness patients (26).
We showed that COVID-19 vaccination was not associated with unstable thyroid status. As case reports of COVID-related thyroiditis and autoimmune thyroid disorders such as Graves' disease are accumulating (27), it is reasonable to postulate that COVID-19 vaccination can also be associated with a spectrum of thyroid dysfunction. In line with this, case reports of subacute thyroiditis and Graves' disease after COVID-19 vaccination have been published (10,11). Molecular mimicry and “autoimmune/inflammatory syndrome induced by adjuvants” (ASIA) have been proposed to be the mechanisms for the thyroid dysfunction after COVID-19 vaccination.
A recent study has demonstrated the cross-reactivity of SARS-CoV-2 spike protein, nucleoprotein, and membrane protein with thyroid peroxidase, and the sequence homology/similarity between many thyroid peroxidase peptide sequences and sequences in various SARS-CoV-2 proteins (28). Furthermore, the adjuvants in the vaccines, such as the aluminum salts in CoronaVac, may have the potential to cause ASIA (29). Hence, people with preexisting thyroid disorders such as hypothyroidism may be worried about the possible unstable thyroid status after COVID-19 vaccination and avoid vaccination. Although some vaccine trials that demonstrated safety and efficacy have included patients with autoimmune disorders (30), this group of patients was the minority and the nature of the autoimmune disorders was not necessarily thyroid specific.
Based on these trials, professional bodies such as the European Society of Endocrinology have issued statements suggesting that patients with stable endocrine disorders, including thyroid disorders, should follow the same recommendations as for the general population and receive COVID-19 vaccination accordingly (31,32). Our population-based study provided important reassuring real-world data that COVID-19 vaccination did not lead to thyroid status instability or increased risks of overall adverse outcomes. Our results further provide solid ground for the statements published by the professional bodies and encourage patients treated for hypothyroidism to proceed with COVID-19 vaccination, particularly if stable on LT4, to protect themselves from possibly worse COVID-19-related outcomes.
Apart from Graves' disease and subacute thyroiditis, Hashimoto's thyroiditis presented with hypothyroidism has also been reported after COVID-19 (20). Nevertheless, to date, Hashimoto's thyroiditis after COVID-19 vaccination has not been reported. Consistent with that, our results did not show a higher risk of dosage escalation in LT4 among vaccine recipients.
The prevalence of Hashimoto's thyroiditis—the leading cause of hypothyroidism and an autoimmune thyroid disorder—varies with age and sex. Autoimmune thyroiditis is much more common in women than in men. Furthermore, thyroid autoantibodies increase with age (5). As we did not have access to the thyroid autoimmunity status of the cohort, we performed subgroup analyses to evaluate if there is any differential impact of COVID-19 vaccination especially on thyroid-specific outcomes. Importantly, we did not observe any adverse impact on the stability of thyroid status and health care utilization outcomes across age and sex groups. The results further supported the safety of COVID-19 vaccination on patients treated for hypothyroidism, be it due to autoimmune or not. Moreover, across different categories of baseline thyroid status, we did not observe any adverse safety signal after COVID-19 vaccination.
The exact proportion of post-thyroidectomy patients in this cohort of 47,086 LT4 users was not known, as we did not have the details of etiologies of hypothyroidism in this database. Indirect data from a previous study in Hong Kong showed that 5364 patients received total thyroidectomies for benign pathologies over 20 years from 1995 to 2014 (33), meaning that post-thyroidectomy hypothyroidism probably accounted for a certain proportion of our study cohort. This also meant that patients with nonthyroidectomy hypothyroidism probably still accounted for a major portion of our study cohort.
Published case reports of thyroiditis and Graves' disease after COVID-19 vaccination referred to patients with thyroid gland present (12). Although post-total thyroidectomy patients would be expected to be at a lower risk of vaccine-related thyroid dysfunction, it is still clinically relevant to assess the safety of COVID-19 vaccination in all patients with hypothyroidism including post-thyroidectomy. People with chronic illness such as history of thyroidectomy might be less willing to receive COVID-19 vaccines because of their concerns about the potential side effects.
Indeed, in a study in Hong Kong, family doctors' willingness to recommend COVID-19 vaccines to patients correlated with their worry about vaccine side effects on patients with chronic illness (26). Given the lack of details of etiologies of hypothyroidism, sensitivity analyses have been performed according to age and sex, as the prevalence of different etiologies of hypothyroidism varies with age and sex. For example, Hashimoto's thyroiditis has been reported to be more common in women, and thyroid antibodies increase with age (5). Sensitivity analyses revealed no signal of increase in thyroid-related events or unscheduled health utilization across different age, sex, and even prevaccination thyroid status categories, suggesting that our results are likely generalizable to patients treated for hypothyroidism due to various etiologies.
Our study addressed the vaccine safety of two different technology platforms with a relatively large sample size and a median follow-up of 10 weeks after vaccination. A review of published case reports on subacute thyroiditis and Graves' disease after COVID-19 vaccination shows that the time of onset of these adverse events varies from a few days (10,11) to eight weeks postvaccination (34,35). Hence, it is likely that our study should have covered most of these thyroid-specific outcomes postvaccination.
However, results from our study should be interpreted bearing certain limitations. First, as discussed above, the details about the etiologies of hypothyroidism were not available. Second, our study used LT4 dosage as the surrogate to gauge the thyroid status, where thyroid function measurement may be preferred. Nonetheless, adjustments in LT4 dosage have taken into consideration both the patient's clinical status and thyroid function, which may be a more clinically relevant outcome. Third, similar to all large-scale pharmacovigilance studies using EMR databases, drug adherence could not be ascertained. Lastly, despite our attempts in balancing a range of patient demographics, comorbidities, and concurrent medications, in common with all epidemiological studies, residual confounders could not be completely excluded in this retrospective database analysis.
Conclusions
Among patients treated for hypothyroidism in general, COVID-19 vaccination with CoronaVac or BNT162b2 was not associated with instability in their thyroid status or an increased risk of adverse outcomes. These important reassuring data align with the positional statements from professional bodies, and should encourage patients treated for hypothyroidism to proceed with vaccination against SARS-CoV-2 infection to protect themselves from potentially worse COVID-19-related outcomes as no thyroid-related repercussions of vaccine should be expected.
Footnotes
Acknowledgments
The authors thank the Hospital Authority and the Department of Health for the generous provision of data for this study. F.T.T.L. and I.C.K.W.'s post were partly funded by D24H; hence, this work was partly supported by AIR@InnoHK administered by the Innovation and Technology Commission.
Authors' Contributions
D.T.W.L., C.K.H.W., and X.X. reviewed the literature, designed the statistical analysis, conducted analyses, and wrote the article. X.X., C.K.H.W., D.T.W.L., and K.T.K.L. reviewed the literature, contributed to the interpretation of analysis, and wrote the article. X.X. and I.C.H.A. conducted the analyses. C.K.H.W., F.T.T.L., X.L., E.Y.F.W., C.S.L.C., E.W.Y.C., F.W.T.C., C.H.L., Y.-C.W., D.T.W.L., and I.C.K.W. contributed to the interpretation of the analysis, and critically reviewed and revised the article. All authors contributed to the interpretation of the analysis, critically reviewed and revised the article, and approved the final article as submitted. The corresponding author attests that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted.
Author Disclosure Statement
C.K.H.W. reports receipt of research funding from the EuroQOL Group Research Foundation, the Hong Kong Research Grants Council, and the Hong Kong Health and Medical Research Fund. F.T.T.L. has been supported by the RGC Postdoctoral Fellowship under the Hong Kong Research Grants Council. X.L. has received research grants from the Food and Health Bureau of the Government of the Hong Kong SAR, research and educational grants from Janssen and Pfizer; internal funding from the University of Hong Kong; consultancy fee from Merck Sharp & Dohme, unrelated to this work.
E.Y.F.W. has received research grants from the Food and Health Bureau of the Government of the Hong Kong SAR, and the Hong Kong Research Grants Council, outside the submitted work. C.S.L.C. has received grants from the Food and Health Bureau of the Hong Kong Government, Hong Kong Research Grant Council, Hong Kong Innovation and Technology Commission, Pfizer, IQVIA, and Amgen; personal fee from PrimeVigilance Ltd.; outside the submitted work.
E.W.Y.C. reports honorarium from Hospital Authority, grants from Research Grants Council (RGC, Hong Kong), grants from Research Fund Secretariat of the Food and Health Bureau, grants from the National Natural Science Fund of China, grants from Wellcome Trust, grants from Bayer, grants from Bristol-Myers Squibb, grants from Pfizer, grants from Janssen, grants from Amgen, grants from Takeda, and grants from Narcotics Division of the Security Bureau of HKSAR, outside the submitted work. I.C.K.W. reports research funding outside the submitted work from Amgen, Bristol-Myers Squibb, Pfizer, Janssen, Bayer, GSK, Novartis, the Hong Kong RGC, and the Hong Kong Health and Medical Research Fund, the National Institute for Health Research in England, European Commission, National Health and Medical Research Council in Australia, and also received speaker fees from Janssen and Medice in the previous three years.
Funding Information
Research Grant from the Food and Health Bureau, The Government of the Hong Kong Special Administrative Region (Ref. No. COVID19F01). The funders did not have any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3