
Abstract
Background:
Medullary thyroid cancer (MTC) is a neuroendocrine tumor arising from parafollicular C-cells of the thyroid gland that, in rare cases, can cause a paraneoplastic ectopic Cushing's syndrome (ECS). The development of Cushing's syndrome (CS) in MTC patients is generally associated with advanced disease and poor prognosis.
Summary:
We described a case of severe CS due to MTC in a young male. We performed a systematic review to identify cases of ECS due to MTC. We searched PubMed, Scopus, and Web of Science for publications between database inception and February 2022 and we collected the patient characteristics, disease presentation, employed treatment strategies, and disease outcomes. In addition to our patient, we identified 96 cases of ECS due to MTC reported in literature. Mean age at diagnosis was 44.4 years (range 10–84), and there was a male predominance (male:female [M:F] = 1.8:1). Most patients (51%) presented with metastatic disease at diagnosis and showed severe hypercortisolism. Seventeen patients developed distant metastasis and hypercortisolism during follow-up. Interestingly, in 48% of patients, the diagnosis of CS followed the diagnosis of MTC with a median time of 48 months but, among patients in whom the diagnosis was concomitant (38%), symptoms due to hypercortisolism were frequently the reason for seeking medical advice. Pathology results showed evidence of adrenocorticotropic hormone (ACTH) or corticotropin releasing hormone (CRH) positive cells in 76% of patients in whom they were tested. The management of hypercortisolism was challenging in most patients with 48% requiring, eventually, definitive treatment with bilateral adrenalectomy (BLA). Recently, some limited evidence has emerged regarding tyrosine kinase inhibitors (TKIs) treatment for hypercortisolism in patients with ECS due to MTC. Despite limited information on survival, prognosis was generally poor and the main causes of death were either complications of CS or disease progression.
Conclusions:
Despite its rarity, MTC should be considered in the differential diagnosis of ECS. Management of hypercortisolism is a key factor to improve the patient's symptoms but it is often challenging and BLA is frequently required. Further studies are needed for investigating the role of TKIs in patients with MTC with ECS.
Introduction
Medullary thyroid cancer (MTC) is a rare neuroendocrine tumor arising from the parafollicular C-cells of the thyroid. The term “medullary” was definitively adopted in 1959, after Hazard et al. presented the distinctive histological features of this tumor (1). Despite its incidence slightly increasing in the past decades, it only accounts for 1–2% of all thyroid cancers, which is also due to the more consistent incidence and increase of papillary thyroid cancer (PTC) (2,3).
The MTC is usually more aggressive than differentiated thyroid cancer (DTC: PTC and follicular thyroid cancer), with the main prognostic factors being age (worse for patients ≥45 years old) and disease stage at diagnosis (4,5). The prognosis of early stage disease is still very good, with an estimated 10-year overall survival of 100% and 93% for patients with stage I and stage II disease, respectively. Unfortunately, more than 70% of patients with palpable disease at diagnosis have cervical lymph node metastases and 10% have distant metastases with a 10-year survival of 71% and 21% for stage III and stage IV disease, respectively (5,6).
About 75% of MTC are sporadic and the rest of them are hereditary as a component of autosomal dominant disease such as multiple endocrine neoplasia (MEN) type 2A and 2B or familiar MTC (FMTC), generally considered a variant of MEN 2A. Almost all patients with inherited MTC have germline mutations in the protooncogene RET, while only half of the sporadic cases have somatic RET mutations. Germline mutations in inherited MTC show a genotype–phenotype correlation. Germline mutations in MEN 2A and FMTC syndromes have been described in exons 10, 11, 13, 14, and 15 of RET, while germline mutation in exon 16 (M918T) is responsible for more than 95% of unrelated MEN 2B cases (7). Some mutations in sporadic MTC (e.g., M918T) are associated with a more aggressive disease course and a worse prognosis (8,9).
Calcitonin and carcinoembryonic antigen (CEA) are the main tumor markers in MTC but C-cells can also secrete several bioactive hormones that rarely give rise to a paraneoplastic syndrome, the most common of which is Cushing's syndrome (CS) due to corticotropin releasing hormone (CRH) or adrenocorticotropic hormone (ACTH) secretion. In 1932, Harvey Cushing described a group of patients affected by a “polyglandular syndrome,” which he ascribed to the presence of a basophil adenoma of the pituitary gland.
This syndrome was, therefore, called “pituitary basophilism” but it soon became referred to as “Cushing's syndrome” (10). The evidence that certain “nonendocrine” tumors could give rise to CS through ACTH secretion was first presented in the works of Christy and of Liddle's groups in the early 1960s (11,12). It very soon became clear that nonpituitary endocrine tumors also could cause CS and the term “ectopic ACTH syndrome” was, therefore, coined (13).
In 1968, Donahower et al. reported for the first time two cases of MTC associated with CS in which ACTH assays of the tumors confirmed ectopic ACTH production (14). Until then, only 11 other cases of CS supposedly due to thyroid cancer had been reported, with 7 of them probably of medullary type, but without clear evidence of ACTH production by the MTC (15 –21).
Ectopic Cushing's Syndrome (ECS) is an uncommon cause of CS that accounts for 5–10% of cases of ACTH-dependent CS. The most frequent causes of ECS are small cell lung cancer and other neuroendocrine tumors of the lung, thymus, and pancreas. The MTC is a rare and less frequent source of ECS (22), and the development of CS in MTC patients is generally associated with advanced disease and poor prognosis. Together with primary cancer treatment, the control of hypercortisolism has a key role in the management of these patients as the complications of CS worsen quality of life and prognosis and may prevent adequate cancer management.
The main treatment strategies of hypercortisolism include tumor debulking, steroidogenesis inhibitors, and bilateral adrenalectomy (BLA). Recently, tyrosine kinase inhibitors (TKIs) have been proposed as a new treatment strategy to manage ECS in MTC.
In this article, we present a systematic review of ECS due to MTC, starting from a new case report. We also discuss the role of laparoscopic BLA and of TKIs in this setting.
Case Presentation
In September 2020, a 32-year-old male was referred to our Endocrinology department for suspected Cushing's disease with central hypothyroidism and a suspicious thyroid nodule. The patient reported marked fatigue, proximal muscle weakness, and weight loss in the past 3 months. Physical examination showed moon face, facial plethora, proximal muscle atrophy, and easy bruising. Buffalo hump and striae rubra were not present. Blood pressure and blood glucose levels were normal. Initial blood tests showed marked hypokalemia, inappropriately low thyrotropin associated with low free thyroxine, and free triiodothyronine and severe ACTH-dependent hypercortisolism.
Both 8 mg-dexamethasone suppression test and CRH stimulation test were performed, and the results were indicative of ECS. All the test results are available in Supplementary Table S1. Pituitary magnetic resonance imaging (MRI) was performed and showed a normal gland. The alteration in thyroid functions tests, mimicking central hypothyroidism, was considered secondary to the inhibitory effects of glucocorticoids on the Hypothalamus-Pituitary-Thyroid axis (23) and thyroxine replacement was not judged useful.
Thyroid ultrasound showed a thyroid nodule suspicious for thyroid cancer (American College of Radiology Thyroid Imaging, Reporting and Data System score: TR5) with bilateral cervical lymph nodes metastasis. The MTC diagnosis was confirmed by cytology and serum calcitonin levels of >20,000 pg/mL (normal value [n.v.] <10), and CEA of 3054.2 ng/mL (n.v. <5). Serum calcium and urinary catecholamines, metanephrines, and normetanephrine were normal. Genetic testing excluded both germinal and somatic RET mutations. 68Ga-DOTATOC positron emission tomography (PET)/contrast-enhanced computed tomography revealed metastasis in every bone segment and in cervical and mediastinal lymph nodes with moderate tracer uptake and a miliary distribution of metastasis in the lungs and liver.
During hospitalization, the patient developed worsening hypokalemia, despite 120 mEq/day I.V. KCl replacement and I.V. canrenone 200 mg bid, and severe psychiatric symptoms non-responsive to medical therapy. Due to these complications and the rapid worsening in general conditions, the patient required urgent simultaneous BLA that was personalized by the surgeons based on the patient's clinical needs. Indeed, a modified anterior transabdominal laparoscopic approach was used to reduce the risk of patient's positioning related to multiple bone metastasis especially at the spine level.
Intraoperative liver biopsy showed localization of MTC with ACTH expression at immunohistochemistry. After surgery, the patient started hydrocortisone and fludrocortisone replacement therapy and had a rapid recovery with a significant improvement in the general conditions. The patient was discharged home 13 days after surgery with the plan to perform thyroidectomy soon and in the meantime lanreotide 120 mg/28 days was started. Five weeks later, he underwent total thyroidectomy with central and bilateral cervical lymph node dissection to control the disease locally. Histology confirmed the diagnosis of multifocal MTC with infiltration of the left laryngeal recurrent nerve (pT4aN1b).
Due to the high disease burden, systemic therapy with lanreotide 120 mg/28 days was continued and vandetanib 300 mg/day was initiated 2 weeks after the thyroid surgery. After 6 months, total-body computed tomography (CT) scan showed stable disease. The patient is now in good clinical conditions; he resumed work and light physical activity and is continuing treatment without severe side effects. Considering the diffuse bone metastasis with a high risk of skeletal-related events, zolendronic acid 4 mg/28 days was initiated in May 2021.
Systematic Review of the Literature
Methods
Search strategy and selection criteria
We performed a systematic review to identify cases of ECS due to MTC and synthesize the patient characteristics, disease presentation, employed treatment strategies, and disease outcomes.
We searched PubMed, Scopus, and Web of Science for publications between database inception and February 7, 2022 using the following as keywords and MeSH terms: (“medullary thyroid cancer” OR “medullary thyroid carcinoma” OR “medullary carcinoma” OR “medullary cancer” OR “thyroid cancer” OR “thyroid carcinoma”) AND (“cushing syndrome” OR “ACTH” OR “hypercortisolism” OR “paraneoplastic syndrome” OR “paraneoplastic” OR “ectopic cushing”). No language restrictions were used. In the attempt to identify any relevant manuscript not already found in this search, the references of the retrieved articles were also screened and relevant studies were included.
After duplicate articles were removed, two reviewers (A.C., V.R.) selected relevant articles independently first by title and abstract and then by reviewing the full text of the remaining articles. All articles reporting new cases of ECS due to MTC were considered relevant, and studies in which individual participant data were reported were included. Two reviewers (A.C., V.R.) evaluated independently the final selected studies using the Joanna Briggs Institute (JBI) critical appraisal checklist for case reports and case series (24); disagreement was solved by discussion. No study was excluded on the basis of quality since the available evidence was already limited.
This research was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (25).
Data extraction and analysis
For each included manuscript, available data regarding patient demographic characteristics, disease stage, clinical presentation, biochemical tests, CS treatment, MTC treatment, immunohistochemistry results, and disease outcome were extracted independently by two reviewers (A.C., V.R.). Data were then cross-checked, and any discrepancies were discussed and mediated by a third reviewer (P.L.). Both reviewers and abstractors worked independently.
The significant heterogeneity of the included studies, especially in terms of outcome measures, did not allow us to perform a meta-analysis. Therefore, we conducted a narrative synthesis without additional statistical analysis.
Results
Included articles
Database search yielded 1029 results, of which 130 were selected after titles and abstracts screening. Twelve articles were excluded, because the full text was not available. Sixteen articles were excluded because they were in a non-English language. The list of these potentially relevant articles that were excluded can be found in Supplementary Data.
The full text of 102 articles were screened, and 70 were included (Fig. 1). The 70 included articles contained data on 96 patients with ECS due to MTC. To this group we added the patient we described in the present report for a total of 97 patients. Of note, 11 out of 97 cases have been retrieved from a recent matched case series (26) and are not included in the results of this article as data regarding each single case were not reported. Nonetheless, the key findings of this matched case series are discussed in the “Discussion” section.
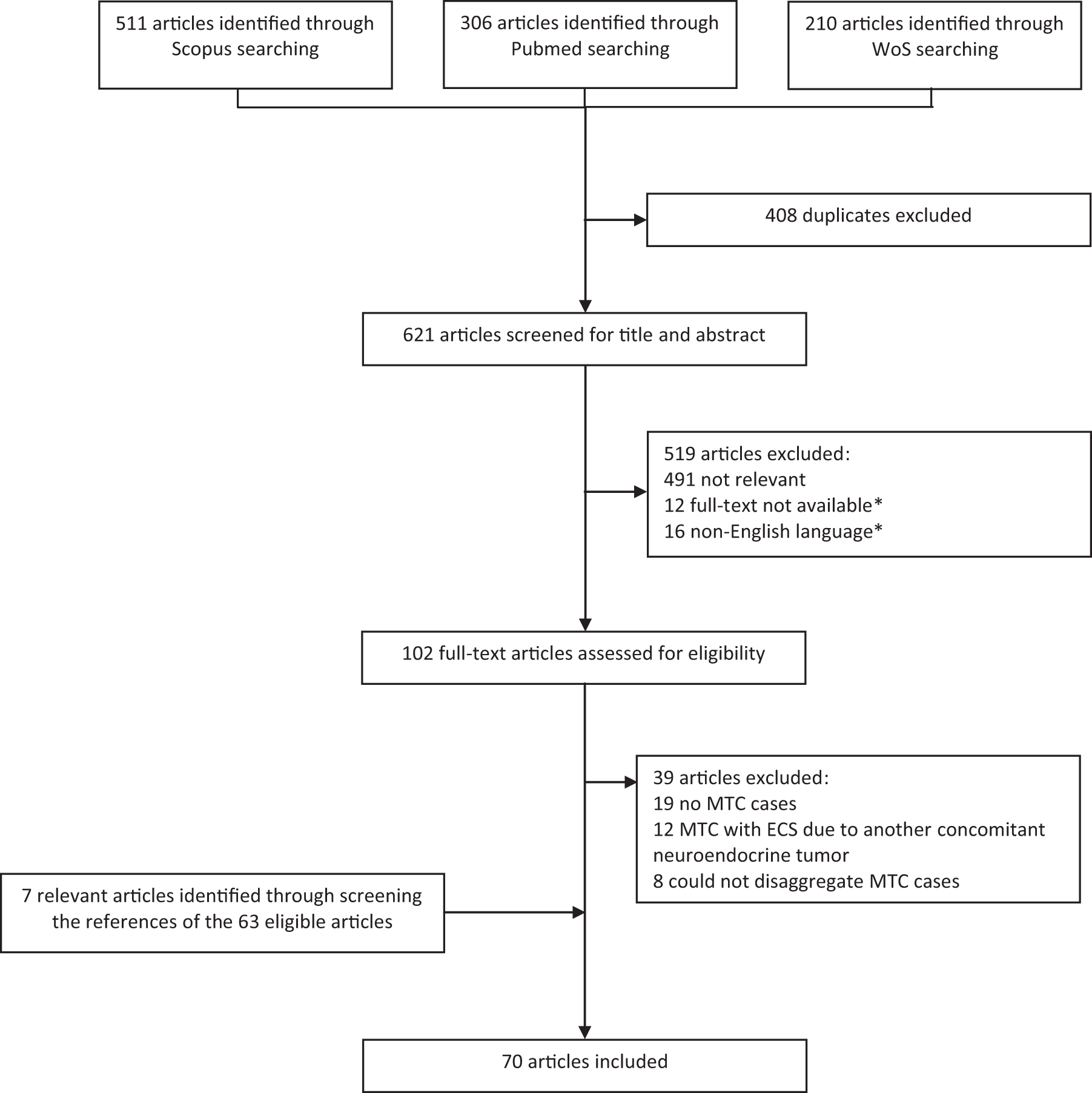
Flowchart of literature search and study selection. Adapted from PRISMA. *The full list of potentially relevant articles excluded due to lack of full-text availability and/or language (non-English) can be found in Supplementary Data. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; WoS, Web of Science.
Overall, despite a significant variation across quality domains, the quality of the included articles was acceptable. In particular, among the case reports, the domains with the highest quality were those regarding the description of the demographic characteristics and the diagnosis and treatment; the domains with the lowest quality were those regarding the outcome and the reporting of adverse effects. The results of the quality assessment according to the JBI checklist can be found in Supplementary Tables S2 and S3 and Supplementary Figures S1 and S2.
Patients' characteristics
The mean age at diagnosis was 44.4 years (range 10–84). There were 55 males (64%) and 31 females (36%). The MTC was sporadic in 34 patients (39%), hereditary in 11 patients (13%) and the disease form was not available in the remaining 41 patients (48%).
Among patients with hereditary MTC, four cases were MEN 2A, four were MEN 2B, and three were not better specified.
The most common clinical presentation at diagnosis was either a new onset neck mass and/or sign and symptoms suggestive for CS. At diagnosis, distant metastasis was already present in 44 patients (51%); 16 patients had only lymph node metastasis (19%), and 17 patients had local or locally advanced disease (20%). The disease stage at diagnosis was not available for nine patients (10%).
Among the 33 patients with non-metastatic disease at diagnosis, 17 (52%) developed distant metastasis between 2 months and 24 years. Overall, the most common site of metastasis was the liver followed by lung and bone (Table 1).
Clinical Characteristics of Patients and Disease Stage at Diagnosis
Patient ID number is a patient identifier number assigned consecutively for this study. Probably sporadic = no specific indication on disease form but history suggestive for sporadic. Probably hereditary = no specific indication on disease form but history suggestive for hereditary. Probably metastatic = no specific indication on disease stage at diagnosis but history suggestive for metastatic disease at diagnosis.
CS, Cushing's syndrome; F, female; LN, lymph nodes; M, male; MEN, multiple endocrine neoplasia; MTC, medullary thyroid cancer; N+, lymph nodes metastases; NA, not available.
CS in MTC
As expected, most patients with CS due to MTC showed severe hypercortisolism with a marked increase in serum cortisol and ACTH and in 24 hours urinary-free cortisol. Cortisol was not suppressed by high-dose dexamethasone in 36 out of 39 patients (92%), and there was no response to CRH in 6 out of 6 patients (100%). PET/CT using 68Ga-labeled somatostatin receptor ligands was employed only in 4 patients and showed uptake in lymph nodes, lung, liver, and bone lesions (Supplementary Table S4).
Hypokalemia was present in most patients, and it was often severe and difficult to treat. As in other cases of ECS, the clinical presentation was variable, and the signs and symptoms typical of Cushing's disease were not always present. The full list of signs and symptoms of CS that characterized these patients is summarized in Table 2. The diagnosis of MTC preceded that of CS in 41 out of 86 patients (48%; median time = 42 months), was concomitant with CS in 33 out of 86 patients (38%), and followed CS only in 2 out of 86 patients (2%).
Signs and Symptoms of Cushing's Syndrome
The presence of a sign or symptoms was derived from the description of the case reports and it was not possible, in most cases, to define the severity. Moreover, as in most studies it was not always specified when a symptom was not present, we preferred to include “No” and “NA” in the same field.
IGT, impaired glucose tolerance.
In 10 out of 86 patients (12%), the timing between MTC and CS diagnosis was not specified (Table 3). Of note, among patients in whom the diagnosis of MTC and CS was concomitant, the reason for seeking medical advice was frequently symptoms or signs associated with hypercortisolism.
Time Between Cushing's Syndrome and Medullary Thyroid Cancer Diagnosis, Treatment, and Follow-Up
Patient ID number is a patient identifier number assigned consecutively for this study. Combination therapy is identified with a “+” sign between the different drugs employed. Sequential therapy is identified with a “→” sign between the different treatment employed.
CHT, chemotherapy; LFN, regional lymphadenectomy (distinction between central and laterocervical compartment lymphadenectomy was not available from most studies); MIBG, metaiodobenzylguanidine; RT, radiotherapy; SSA, somatostatin analogues; TT, total thyroidectomy.
Immunohistochemical results
Calcitonin-positive cells were detected in the vast majority of patients in whom it was tested, including in our case (Supplementary Table S5).
Different techniques have been employed to confirm that the MTC primary tumor or its distant metastasis was, indeed, the source of ACTH and/or CRH. Results of this investigation were available for 41 patients (Supplementary Table S5). Overall, including radioimmunoassays, immunofluorescence, immunohistochemistry, arteriovenous gradients, and messenger RNA (mRNA) in situ hybridization, ACTH in MTC lesions was detected in 24 patients (59%); evidence of CRH secretion was observed in 6 patients (15%), and proopiomelanocortin (POMC) mRNA expression was detected in 1 patient (2%). In the remaining 10 patients (24%), no evidence of ACTH was observed in tumor tissues.
Treatment and evolution
Regarding MTC treatment, 52 patients (60%) underwent thyroid surgery. In particular, 28 out of 52 patients (54%) underwent total thyroidectomy with regional lymphadenectomy, 16 out of 52 (31%) total thyroidectomy, 5 out of 52 (9%) hemithyroidectomy or subtotal thyroidectomy and 3 out of 52 (6%) neck surgery not better specified. After surgery, especially in the earlier reports, some patients underwent external neck radiotherapy and systemic chemotherapy. Differently, in the most recent reports, patients with significant disease burden after surgery were mainly treated with TKIs in line with current guidelines.
Information regarding CS treatment was available for 65 patients. Obtaining a good control of CS turned out to be challenging in most patients. Indeed, 31 out of 65 patients (48%) eventually required BLA. Interestingly, in 19 out of 31 patients, BLA was used as the first-line treatment for CS while for the remaining 12 patients it was a “rescue treatment” after failure of medical therapy with steroidogenesis inhibitors.
Among the 34 patients who did not undergo BLA, 6 (18%) were cured by total thyroidectomy, in 4 (12%) a good control of hypercortisolism was obtained with steroidogenesis inhibitors (2 patients on metyrapone, 1 on mitotane and 1 on “anticortisolic drugs” not better specified), in 8 (23%) a good control was obtained with TKIs (4 on Vandetanib, 1 on sorafenib, 1 on subitinib, and 2 on selpercatinib), 8 (26%) did not achieve a good control with steroidogenesis inhibitors, 6 (18%) did not receive any treatment, 1 (3%) had already undergone previous BLA for pheochromocytoma and 1 (3%) did not achieve a good control of hypercortisolism despite combination treatment with sorafenib and mifepristone (Table 3).
Although information on survival was limited due to the nature of the studies (case reports or case series with a relatively short-term follow-up), overall the prognosis was relatively poor with overall survival ranging between a few days and 24 years (291 months). The main causes of death were related either to complications of CS (including respiratory tract infections, peritonitis due to intestinal perforations, sepsis) or to MTC progression (Table 3).
Discussion
MTC is a rare thyroid tumor and one of the least frequent causes of ECS. It has been estimated that only 0.7% of patients with MTC develop ECS (59) and that, in turn, 2–8% of all ECS cases are caused by MTC (90).
After a systematic literature review, we collected the clinical characteristics of 86 cases of ECS due to MTC reported between 1959 and February 2022. We observed, in line with previous case series, a male predominance and the mean age at diagnosis was 44.4 years. Most patients were affected by sporadic MTC with only 11 cases of familial MTC reported although in about half of the reports, and especially in the earliest ones when genetic analysis was not routinely available, the disease form was not specified.
In most patients, MTC preceded ECS diagnosis by several months. However, the time between MTC diagnosis and ECS presentation was variable with some cases of ECS diagnosed even before MTC diagnosis and others more than 20 years later, suggesting that tumor cells may acquire the ability to produce ACTH or CRH at any time of the cancer natural history. Interestingly, in some patients, the diagnosis of hypercortisolism was concomitant with the development of metastatic disease. In line with this, the prevalence of distant metastasis at diagnosis in this cohort is relatively high (around 50%) when compared with that of MTC not associated with paraneoplastic syndrome (10–15%) (6).
A possible and tempting explanation is that the process leading to metastization and/or the tumor microenvironment at the metastatic site might play a role in the acquisition of the ability to produce ACTH or CRH by the tumor cells as a result of tumor dedifferentiation, as already hypothesized for other neuroendocrine tumors (91,92). Another possible explanation is that ACTH or CRH secretion is present since disease onset but it is the increase in tumoral burden associated with metastatic disease that leads to clinically significant hypercortisolism. A schematic representation of the hypothalamus-pituitary-adrenal axis in normal conditions and in patients with MTC secreting ACTH or CRH is shown in Figure 2.

Regulation of the hypothalamus-pituitary-adrenal axis in normal conditions and in patients affected with Cushing's syndrome due to MTC. (
The clinical presentation of CS was variable and in most cases it was not helpful in distinguishing between Cushing's disease and ECS. The biochemical investigations, on the other hand, documented severe hypercortisolism in almost every patient, there was no suppression by high-dose dexamethasone in 36 out of 39 patients, and there was no response to CRH in 6 out of 6 patients, suggesting the ectopic source. Therefore, we believe that the application of the validated algorithm for the diagnosis of CS would correctly point to an ectopic source and MTC should be considered at that point among the differentials (93). On the other hand, when a patient with progressive MTC shows clinical and laboratory findings suggestive of hypercortisolism ECS due to MTC should be strongly considered.
ACTH- or CRH-positive cells were detected in the majority, but not all, of patients in whom they were tested. Negative ACTH and CRH immunostaining despite clear evidence for tumor causing CS has been reported by several authors. One of the most feasible proposed explanations is that the tumor has a high hormonal secretion rate with a consequently low storage concentration of ACTH or CRH that can be found in tumor tissue (59,94). Another possible explanation is that extrapituitary tumors tend to have an abnormal processing of POMC with increased production of ACTH precursors. In line with this, POMC mRNA in situ hybridization has been proposed as a useful tool to identify the source of ectopic ACTH production (58,95).
MTC treatment and CS management must be addressed at the same time. Indeed, the complications of hypercortisolism are often debilitating and have a significant impact on prognosis being one of the main causes of death in these patients. In the setting of locoregional or oligometastatic disease, curative surgery should be considered the first line of treatment.
However, this approach is feasible in a minority of patients and only 6 out of 86 (7%) patients were cured by surgery without the need for further treatment. Since most patients presented with or developed diffuse metastatic disease, the first treatment goal was to prevent the complications due to hypercortisolism and improve the patient general conditions to initiate as soon as possible systemic therapy for MTC. Steroidogenesis inhibitors are considered first line in ECS due to unresectable or metastatic tumors and they were often employed in patients with ECS due to MTC. However, the control of hypercortisolism was often not satisfactory and BLA was, indeed, employed as rescue treatment in a good proportion of patients.
BLA is the most effective treatment of hypercortisolism but in ECS it is generally considered a rescue treatment, when steroidogenesis inhibitors are ineffective or not tolerated, because of the mortality and morbidity risks especially in patients with severe CS. With the advent of laparoscopic BLA, which has reduced morbidity and hospital stay (96), the choice between medical therapy and BLA in the setting of severe hypercortisolism has become debated and a shift toward BLA can be considered, especially in patients who need to start immediate treatment with antineoplastic drugs.
Since this review of the literature includes cases that have been managed in a wide range of decades, we have tried to observe whether there were some temporal trends explaining differences in diagnosis, treatment, and outcome. Regarding MTC treatment, there is a clear change in the surgical approach with more conservative surgeries (i.e., hemithyroidectomy and subtotal thyroidectomy) performed almost exclusively in the earliest reports (until the 1980s). Also, the “adjuvant treatment” approach radically changed during time with radiotherapy and chemotherapy being the only option up until 2013 when Baudry et al. reported a case of reversal of CS in MTC by the recently approved TKI Vandetanib (66).
Similarly, a temporal trend can be observed in the management of CS. Indeed, in the earliest reports, BLA was often the only treatment employed while starting from the late 1980s, steroidogenesis inhibitors were usually the first line of treatment, and BLA was reserved as a “rescue treatment.”
Recently, a multicenter case series investigated the overall survival (OS) in 11 MTC patients with ECS compared with 22 matched MTC patients without ECS. The results showed, as expected, that the presence of the paraneoplastic syndrome worsened the outcome of MTC patients (OS in patients with ECS vs. without ECS = 87 months [confidence interval, CI: 64–111] vs. 190 months [CI: 95–285]). In line with our results, MTC usually preceded the diagnosis of ECS and ECS occurred mainly in patients with advanced disease (26).
Interestingly, also in this case series, hypercortisolism was severe and BLA was performed in half of the patients who received treatment and proved to be safe and effective.
In the last few years, some authors showed that TKIs may be a new treatment option in patients with ECS due to MTC. Since the first report by Baudry et al. (66), 13 cases have been reported describing the role of TKIs to manage hypercortisolism in patients with MTC (Table 3). The TKIs were initiated due to progressive MTC in 9 out of 13 patients and to control hypercortisolism after failure of steroidogenesis inhibitors in 4 out of 13 patients.
In most of these cases (9/13), treatment with TKIs (including vandetanib, sorafenib, sunitinib, cabozantinib, and selpercatinib) showed an amelioration of CS, with a reduction of cortisol levels since the first days of treatment. Interestingly, some authors reported that often the control of hypercortisolism did not correspond to a reduction in tumor burden and it sometimes persisted even in patients with disease progression, suggesting that TKIs might have a direct antisecretory effect on MTC cells that may be independent from their antineoplastic effect (70).
Therefore, if a significant antisecretory effect is confirmed, TKIs in patients with ECS due to MTC could theoretically represent the best treatment strategy, allowing us to address MTC and hypercortisolism simultaneously.
In patients with metastatic disease, thyroid surgery is often performed but is usually less extensive as the goal is palliative debulking while trying to minimize complications and maintaining the patient's functions of speech and swallowing.
The case we presented underlines the effectiveness of emergency BLA for prompt management of severe hypercortisolism with marked and rapid improvement in patient conditions that allowed the initiation of systemic therapy for MTC.
We present the reasoning behind the choice of treatment for our patient, as we believe it may be applicable to a good proportion of patients with ECS due to MTC.
All available treatment strategies were thoroughly discussed in a multidisciplinary meeting.
Among steroidogenesis inhibitors, mitotane was the first to be excluded due to the delay in the control of CS that is in the range of several months (97). On the opposite, etomidate, a short-acting intravenous anesthetic agent that suppresses steroidogenesis by inhibiting 11β-hydroxylase, was a possible treatment option since it allows a rapid control of hypercortisolism (within hours) (98) but it needs intensive care unit monitoring and it is not a useful strategy for the long-term control of hypercortisolism.
The use of ketoconazole and metyrapone either alone or in combination was proposed and deeply evaluated (99). Among the main side effects of metyrapone, there is the possible worsening of hypokalemia but this effect is attenuated when used in combination with ketoconazole. On the other hand, ketoconazole treatment necessitates close monitoring of liver function as it may lead to hepatic toxicity and this was a further concern for our patient considering the diffuse hepatic involvement.
The use of somatostatin analogues was not considered useful in this acute setting, as the effect on CS control is often suboptimal but it was employed later on as a cytostatic agent considering the 68Ga-PET/CT results. Similarly, mifepristone was not considered an option as evidence in the treatment of ECS is limited (99).
TKIs are one of the newest proposed treatment strategies to manage CS in patients with MTC. Among the different TKIs, treatment with vandetanib was considered the preferred one since it is readily available in our center, it is approved for the treatment of metastatic MTC, and the results regarding its efficacy are consolidated. However, the patient's clinical conditions did not allow a safe initiation of this treatment.
BLA was finally taken in consideration. Although it carries a not negligible risk of morbidity and mortality in patients with severe CS, it is the most effective and immediate treatment for hypercortisolism (96,100). The decision came down to either combination therapy with ketoconazole and metyrapone or BLA, and these were also discussed with the patients' wife. BLA was preferred because our goal was immediate and definitive control of hypercortisolism to establish further MTC treatment as soon as possible.
Among the different advantages of BLA, the prevention of possible drug interactions, especially between steroidogenesis inhibitors and vandetanib, was judge significant. Although different approaches are available (posterior retroperitoneoscopic, lateral transabdominal, open) (101) in the present case a modification of the laparoscopic transperitoneal approach via an anterior route was adopted, to avoid the need of patient positioning, which cannot be feasible in patients with multiple bone metastasis and severely reduced bone density. Despite being more technically demanding, the absence of positioning time allows for a faster operation and lowers the risk of bone fractures.
To the best of our knowledge, this is the first systematic review collecting evidence regarding ECS due to MTC. However, there are several limitations to this review. First, all the included studies were case reports or cases series with a relatively low number of patients. Second, all the studies except for one excluded matched case series (26) do not include a control group so it is difficult to judge treatment outcomes and prognosis. Third, the wide time range of the included studies limits the consistency of the comparison of labs, treatment, and outcomes. Finally, this systematic review was not registered in Prospero.
Conclusions
The MTC is a rare cause of ECS, with 97 cases reported so far in the literature. Most of these patients present with advance disease and develop significant complications due to the CS. The control of CS is a priority to facilitate the initiation of antineoplastic treatment but these patients may poorly respond to conventional pharmacological treatments of hypercortisolism. Indeed, BLA is frequently required, and it is important not to delay this intervention as it may not improve management and survival if it is employed too late in the disease course.
Laparoscopic BLA is considered a safe procedure when performed by experienced surgeons in high-volume centers and the anterior approach might have some advantages, especially in patients with bone disease due to either the hypercortisolism and/or metastatic localizations. There are some promising recent reports on the use of TKIs in managing CS due to MTC, but more research is needed to inform the mechanism of action as well as potential treatment utility.
Footnotes
Authors' Contributions
A.C., V.R., P.L., R.M.P., M.R., and S.M.C. contributed to the study design, literature search, data collection and interpretation, writing, and approval of the article. G.P., E.D.R., A.P., and C.D.C. contributed to writing and approval of the article. F.T. contributed to reviewing and approval of the article.
Author Disclosure Statement
All authors have no conflict of interests to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5