
Abstract
Background:
Epidemiological and experimental studies suggest that thyroid peroxidase antibody (TPOAb)- and thyroglobulin antibody (TGAb)-positive exposure during gestation may contribute to offspring's adverse neural development. However, limited knowledge is available on the association between joint exposure on TPOAb and TGAb and children's emotional and behavioral development. Furthermore, the sex-specific effect on the developmental process of preschoolers' emotions and behaviors is unknown. The present research intends to examine the sex-specific effect of TPOAb- and TGAb-positive exposure in gestation on the developmental process of preschoolers' emotions and behaviors.
Methods:
A total of 2455 mother–child pairs were included from the Ma'anshan Birth Cohort study. The serum TPOAb and TGAb of pregnant women was measured retrospectively by electrochemical immunoassay during the follow-up period. Preschoolers' emotional and behavioral development was assessed by a child behavior checklist 1.5–5. Growth mixture modeling was adopted to fit thyroid antibody (TAb) trajectories. Poisson regression models were used, stratifying by sex, to examine the association between TAb trajectories, as well as four categories of maternal TAb exposure and preschoolers' emotional and behavioral problems.
Results:
Boys born to mothers with TPOAb positivity in the first, second, and third trimesters of pregnancy had an increased risk of autism spectrum problems after adjusting for confounders, with relative risk (RR) [confidence interval, CI] of 2.01 [1.24–3.27], 2.15 [1.08–4.26], and 2.13 [1.20–3.79], respectively. Maternal TGAb positivity and TPOAb negativity in the first trimester were associated with a high risk of attention-deficit/hyperactivity problems in boys (RR = 1.74 [CI 1.01–2.99]). The prevalence of depressive problems in girls was 33.3% after exposure to TPOAb alone in the third trimester of pregnancy. Exposure to TPOAb alone in the third trimester of pregnancy was associated with an increased risk of depressive problems in girls (RR = 1.78 [CI 1.09–2.90]).
Conclusions:
Maternal TPOAb positivity in all three trimesters was associated with the risk of autism spectrum problems in boys. Isolated maternal TGAb positivity in the first trimester was associated with attention-deficit/hyperactivity problems in boys, whereas isolated maternal TPOAb positivity in the third trimester was associated with depressive problems in girls.
Introduction
Thyroid peroxidase antibody (TPOAb) positivity and thyroglobulin antibody (TGAb) positivity are indicators of autoimmune thyroid disease (AITD). Among pregnant women, the prevalence of TPOAb and TGAb positivity is 6–10%. 1 High thyroid antibody (TAb) levels are associated with elevated serum thyrotropin (TSH) levels. 2 Thyroid autoimmunity may indicate insufficient thyroid reserves, which cannot meet the physiological demand for increased thyroid hormone during pregnancy. 3 Maternal elevated TSH levels are reportedly associated with the offspring's physical and psychological development. 4,5 Moreover, our previous study showed that maternal TSH affects the behavioral development in preschool boys. 6 Therefore, it is believed that the presence of maternal TAb may affect offspring development indirectly by increasing the TSH level.
However, several studies have reported an independent association between maternal thyroid autoimmunity and the child's neurodevelopment. Pop et al 7 suggested that AITDs, rather than thyroid hormone deficiency, may affect the child's cognitive development. Ghassabian et al 8 and Brown et al 9 found that maternal TPOAb positivity was associated with children's behavioral problems after adjusting for maternal TSH levels. Therefore, it is unclear whether the effect of TAbs on the offspring's neuropsychological development is an independent effect of antibodies or due to thyroid dysfunction.
Studies on the association between maternal TAb exposure and the offspring's neurodevelopment have primarily focused on the child's cognitive development, 7,10,11 but only few examined the emotional and behavioral development. Emotional and behavioral problems are key areas that are potentially modifiable and related to later-life social development. 12
Recently, sex was confirmed as a key factor in determining behavioral and cognitive vulnerability. 13 Placentas may cause “gender dimorphism” due to the different effects of sex hormones or sex chromosomes, 14 which transmit sex-specific placental signals to the developing brain and cause different sex-related neurodevelopmental trajectories. 15 However, previous studies on the association between maternal TAb exposure and children's emotional and behavioral development did not show sex-related differences.
At present, only few studies have analyzed the effects of TAb presence during the different pregnancy trimesters on the offspring's neural development, and the critical period remains unclear. Therefore, we aimed to repeatedly measure maternal TAb levels in the pregnancy trimesters, examine the sex-specific effects of exposure to combination TAbs on the preschoolers' emotional and behavioral development, and identify the critical period of effect.
Materials and Methods
Participants
We recruited 3474 pregnant women on their first antenatal visit in the obstetric clinic of Ma'anshan Maternal and Child Health Center from May 2013 to September 2014 in the Ma'anshan birth cohort. The inclusion criteria were provision of informed consent for participation; gestational age <14 weeks; willingness to undergo prenatal checkups and childbirth at the center; no existing psychiatric disorders (assessed by self-reporting and professional evaluation); and ability to understand the questionnaires correctly. This study excluded 65 women with prepregnancy thyroid diseases (hyperthyroidism, n = 18; hypothyroidism, n = 47) and 16 with a family history of thyroid diseases. After excluding twin births, adverse pregnancy outcomes, and loss to follow-up (n = 210), 3183 singleton live births were included. Furthermore, 728 children without emotional and behavioral assessments were excluded. 2455 mother–child pairs were included in the final analysis.
Thyroid function test (TFT) data were available for 1824 pregnant women in the first trimester, 1598 in the second, and 1588 in the third. There were 1821 individuals for whom all 3 trimester TFT data were available (Fig. 1).
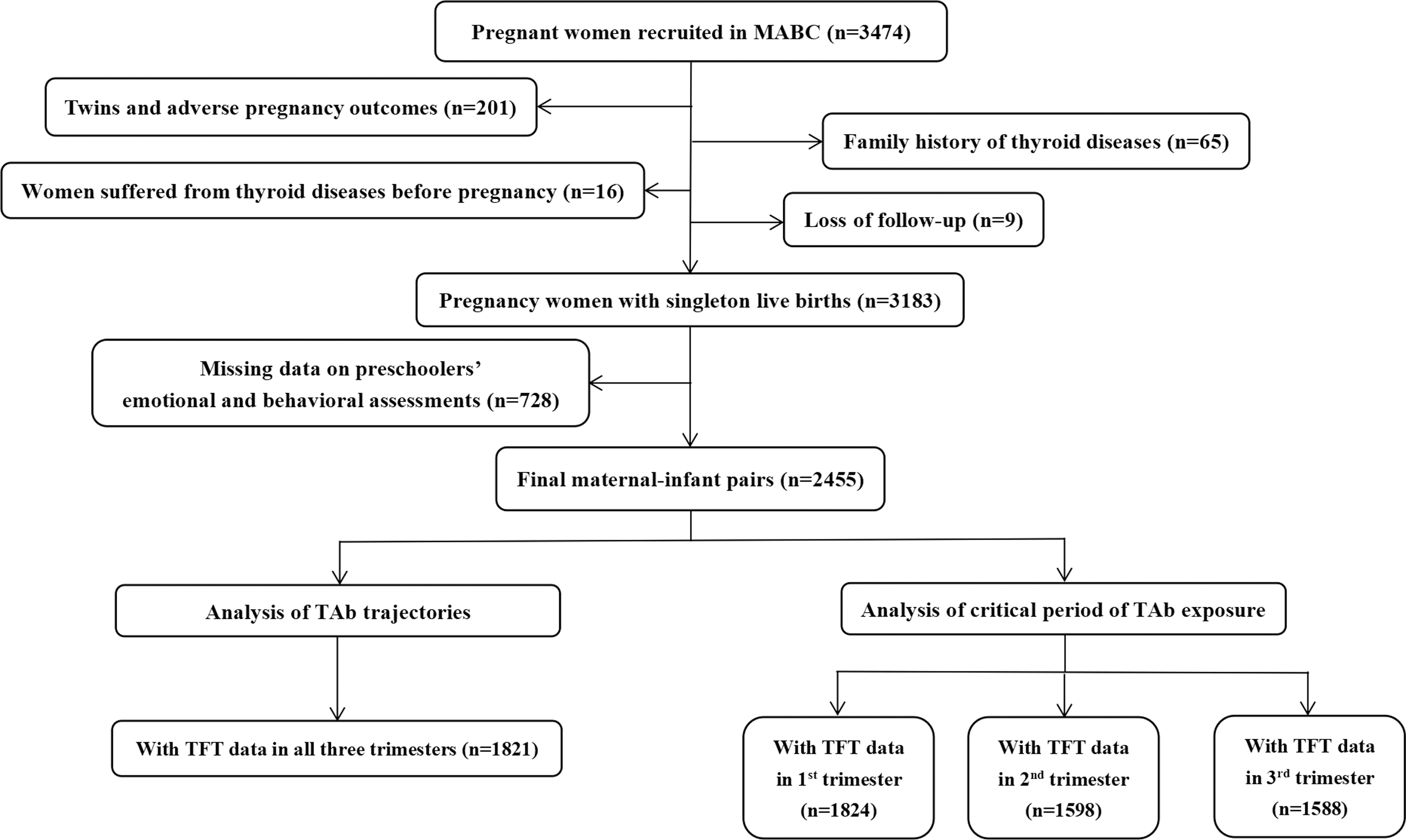
Flowchart of participant recruitment. TAb, thyroid antibody.
All participants provided written informed consent. The study protocol was approved by the Biomedical Ethics Committee of the Anhui Medical University (No. 20131401). This study reporting followed the STROBE guidelines for cohort studies (Supplementary Table S11). 16
Study procedures
Assessment of thyroid functions
Fasting blood specimens of gestational females were collected in the first trimester of gestation (mean 10 weeks), the second trimester of gestation (mean 25 weeks), and the third trimester of gestation (mean 34 weeks), respectively. Serum was stored at −80°C.
The TFT (serum triiodothyronine, thyroxine, free thyroxine, and TSH levels) and TAb (TPOAb and TGAb) of the pregnant women were measured using electrochemical immunoassays (Cobas E411 analyzer; Roche Company, Germany) during the children's follow-up. The TPOAb and TGAb status was considered positive when their serum concentrations were >34 and >115 IU/mL, respectively, based on the laboratory reference values. The upper and lower detection limits of TPOAb and TGAb were 600 and 5 IU/mL and 4000 and 10 IU/mL, respectively. The coefficient of variation between the reagent batches was <10%. 17
We then defined the positive and negative TPOAb and TGAb levels in each trimester separately as follows: TPOAb− and TGAb− (control group), TPOAb+ and TGAb−, TPOAb− and TGAb+, and TPOAb+ and TGAb+. Thus, the control group included women who tested negative for all TAbs at all time points.
Preschoolers' emotional and behavioral development
The preschoolers' emotional and behavioral development was assessed using the Diagnostic and Statistical Manual of Mental Disorders-Oriented scales (DOS) in the Child Behavior Checklist 1.5–5 for children aged 1.5–5 years, as compiled by Achenbach and Rescorla (Supplementary Methods section). 18
The 100 questions in the scale were scored 0 for “incorrect,” 1 for “somewhat or sometimes correct,” and 2 for “always correct.” According to the factor analyses in the manual, the parameters in the DOS include stress problems, depressive problems, anxiety problems, autism spectrum problems, attention-deficit/hyperactivity problems, and oppositional defiant problems. Standardized T-scores were calculated from the crude scores. A T-score ≥70 in the DOS is considered clinically significant, between 65 and 70 as borderline clinical range, and <65 as normal. 19
According to this definition, the emotional and behavioral problems of the DOS were categorized in this study as 0 indicating normal and 1 indicating borderline clinical or clinically significant. This scale has been applied in the evaluation of the emotions and behaviors of Chinese children, where the internal consistency coefficient showed α-value of 0.63–0.95. Moreover, the root mean square error of approximation in the confirmatory factor analysis, comparative fitting index, and Tucker–Lewis index was 0.055, 0.88, and 0.93, respectively, with good reliability and validity. 20
Covariates
The underlying confounding factors were determined a priori based on prior research and directed acyclic graphs (Supplementary Fig. S1). 21 Analyses were adjusted for maternal age, family income, maternal and paternal education levels, place of residence, parity, prepregnancy body mass index (BMI), and smoking and alcohol drinking during pregnancy.
The survey questions in the first trimester collected data regarding the mother's age, educational backgrounds of both parents, home address, household income, parity, prepregnancy BMI, and smoking and alcohol consumption during gestation. Prepregnancy BMI was categorized as low body weight, normal body weight, or obesity according to the Chinese Obesity Working Group criteria. 22
Data on pregnancy complications, maternal thyroid function, pregnancy-related anxiety, child's birth weight, gestational weeks, main caregivers, exclusive breastfeeding, time spent on screening, and time spent in outdoor activities were collected for sensitivity analysis. Pregnancy complications, including hypertensive disorder complicating pregnancy (HDCP), gestational diabetes mellitus (GDM), and preterm birth (PTB), were extracted from the medical records.
The women's mental health and family history of psychiatric diseases was assessed during pregnancy. A self-designed questionnaire was used to assess pregnancy-specific anxiety in the three trimesters. 23 Additional information on the questionnaire is available in the Supplementary Methods section.
The data on the child's birth weight and gestational weeks were obtained from medical records. Information on the main caregivers and exclusive breastfeeding was obtained from the questionnaires completed 6 months postpartum. Data on the time spent in screening and time spent in outdoor activities were collected from the 48-month postpartum questionnaires. Covariates were defined as shown in Table 1.
Basic Characteristics of Included and Excluded Participants
BMI, body mass index; fT4, free thyroxine; GDM, gestational diabetes mellitus; HDCP, hypertensive disorder complicating pregnancy; PTB, preterm birth; SD, standard deviation; T3, triiodothyronine; T4, thyroxine; TGAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin.
Statistical analysis
Continuous variables are described as means and standard deviations, and categorical variables as numbers (percentages). Before starting all analyses, multiplicative interactions of the TPOAb status, TGAb status, TAb exposure, and sex on the children's behavioral development were performed. DOS domains with p-values <0.15 were considered significant and examined by stratifying by sex and the four categories of maternal TAb exposure in each trimester. 24 The interaction analyses are presented in Supplementary Table S2.
Growth mixture modeling (GMM) was used to fit the TAb trajectories throughout pregnancy. Poisson regression models were used to examine the association between the TAb trajectories throughout pregnancy and the preschoolers' emotional and behavioral development. The model is a type of generalized linear regression model that is usually used to describe the distribution of the number of rare events (i.e., small probability) in a large sample population. The DOS domains were regarded as the outcome variables, and each domain was classified into two categories, 0 indicating normal (control group) and 1 indicating borderline clinical or clinical significance. Poisson regression models were adopted to understand the association of the four categories of maternal TAb exposure in each trimester with the preschoolers' emotional and behavioral problems.
Five sensitivity analyses were conducted to test the robustness of the findings. Additional information on the sensitivity analyses is available in the Supplementary Methods section. Statistical Product and Service Solutions version 26.0 (Armonk, NY) and Mplus 8.0 (Mplus, Los Angeles, CA) were utilized for data analyses.
Results
Basic characteristics of the included and excluded participants
Table 1 shows a comparison of the basic characteristics between the 2455 included mother–child pairs and 728 pairs without emotional or behavioral assessments who were excluded. In the included participants, the mean age of the pregnant women was 26.6 ± 3.6 years, and 90.7% of them were primiparous. The prevalence of GDM was higher in the women of the included group than in those of the excluded group (14.0% vs. 10.6%; p = 0.021). The birth weight of the children among the included participants was lower than that of the children among the excluded participants (p = 0.038).
Table 2 shows the basic characteristics of the participants of the TPOAb− and TGAb−, TPOAb+ and TGAb−, TPOAb− and TGAb+, and TPOAb+ and TGAb+ groups included in the analysis. Supplementary Table 1 shows the basic characteristics of the children according to the sex.
Basic Characteristics of Participants by Thyroid Antibody Grouping
Data are given as mean ± SD or n (%).
TPOAb+ was defined as >34 IU/mL; TGAb+ was defined as >115 IU/mL; TPOAb−/TGAb− group meant that women had negative TPOAb and negative TGAb at all three trimesters; TPOAb+/TGAb− group in first trimester meant that women had positive TPOAb in first trimester but had negative TGAb at all three trimesters; TPOAb−/TGAb+ group in first trimester meant that women had positive TGAb in first trimester but had negative TPOAb at all three trimesters; TPOAb+/TGAb+ group in first trimester meant that women had positive TPOAb and positive TGAb in first trimester. Four groups, TPOAb−/TGAb− group, TPOAb+/TGAb− group, TPOAb−/TGAb+ group, and TPOAb+/TGAb+ group in the second trimester and third trimester, were defined in the same way.
Missing data in second trimester: 19 in education level, 23 in prepregnancy BMI, 142 in pregnancy-related anxiety, 11 in main caregivers, and 31 in exclusive breastfeeding within 6 months after birth.
Missing data in first trimester: 13 in education level, 32 in prepregnancy BMI, 739 in pregnancy-related anxiety, 1 in children's birth weight, 11 in main caregivers, and 34 in exclusive breastfeeding within 6 months after birth.
Missing data in third trimester: 4 in prepregnancy BMI, 165 in pregnancy-related anxiety, 11 in main caregivers, and 31 in exclusive breastfeeding within 6 months after birth.
TAb trajectories during pregnancy and emotional and behavioral problems in preschoolers
In total, 1821 pregnant women with 3 complete measurements of TFT data were included. The best fit was categorization into low-level and high-level TAb trajectory groups. Figure 2 shows the trajectory of the maternal TAb during pregnancy in women birthing boys (n = 945). High-level trajectory was observed in 3.7% of the pregnant women, characterized by high levels of TAb at baseline and a gradual decline in the second trimester, with a slight decline in the TPOAb levels and slight increase in the TGAb levels in the third trimester. Furthermore, 96.3% of the women showed a low-level trajectory.

Maternal TAb trajectory grouping during pregnancy in boys.
The same tendency was observed in women birthing girls (n = 876). High-level trajectory was observed in 3.7% of the women, and low-level trajectory in 96.3% (Fig. 3).
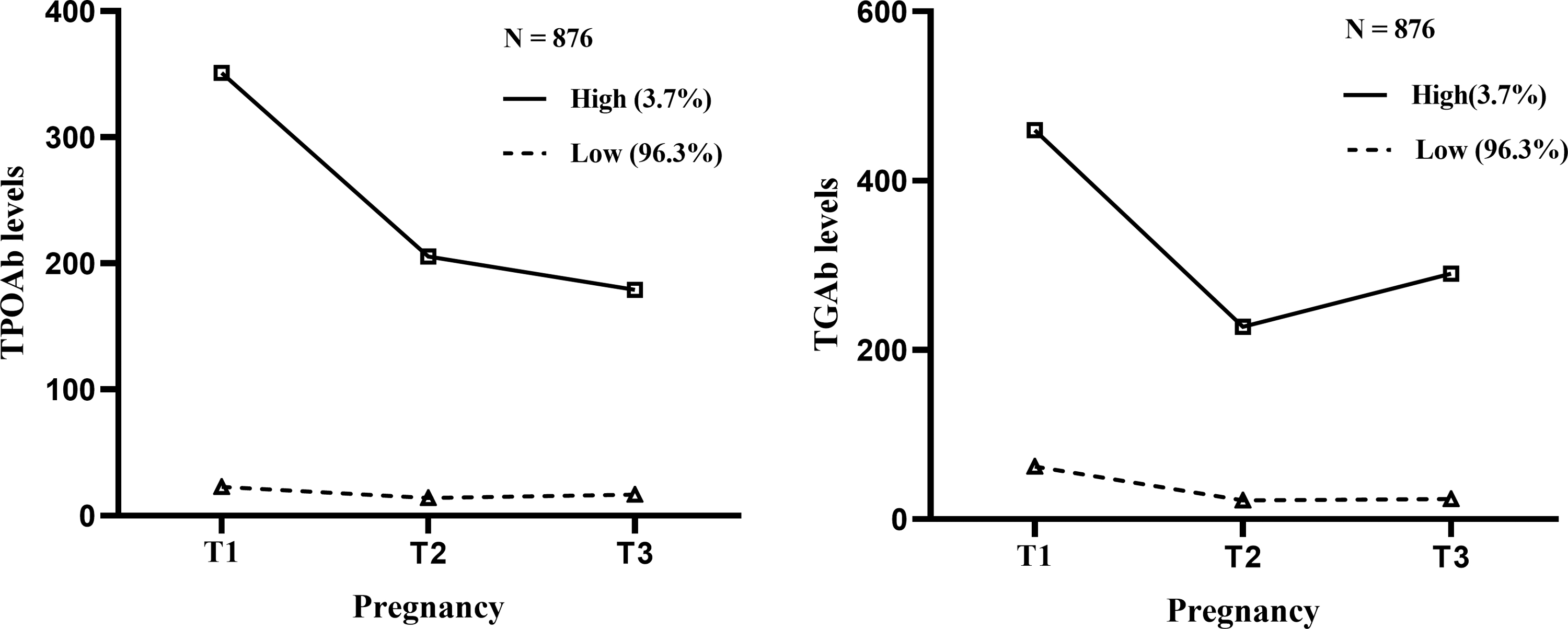
Maternal TAb trajectory grouping during pregnancy in girls.
The prevalence of depressive problems among the girls was 20.7% and 34.4% among the low-level and high-level TAb trajectory cases, respectively (p = 0.064). Girls born to women with high TAb levels during pregnancy had an increased risk of depressive problems after adjusting for confounders (relative risk, RR = 1.70 [confidence interval, CI 1.03–2.81]) (Table 3). The sensitivity analysis did not fundamentally change the results of the main analysis (Supplementary Tables S8 and S9).
Association Between Maternal Thyroid Antibody Trajectories and Preschoolers' Emotional and Behavioral Problems (Relative Risk and [Confidence Interval])
Model 1: unadjusted model.
Model 2: adjusted for maternal age, family income, maternal education level, paternal education level, place of residence, parity, prepregnancy BMI, and smoking and alcohol drinking situation during pregnancy.
p < 0.05; — no results due to the limited cases with emotional and behavioral problems.
ref, reference variable; TAb, thyroid antibody.
Prevalence of emotional and behavioral problems in preschoolers exposed to maternal TAbs
The prevalence of autism spectrum problems in boys born to mothers with TPOAb+ and TGAb− in the first, second, and third trimesters of pregnancy was 30.8%, 30.0%, and 30.0%, respectively, which was higher than that in boys born to mothers with TPOAb+ and TGAb+, TPOAb− and TGAb+, and TPOAb− and TGAb− in the same period.
The prevalence of depressive symptoms in girls born to mothers with TPOAb+ and TGAb− in the first, second, and third trimesters of pregnancy was 27.3%, 28.1%, and 33.3%, respectively, which was higher than that in girls born to mothers with TPOAb+ and TGAb+, TPOAb− and TGAb+, and TPOAb− and TGAb− in the same period.
The respondents of the DOS in this study included mothers (70.8%), fathers (20.9%), grandparents (7.5%), and others (0.8%).
Association between maternal exposure to TPOAb and TGAb and preschoolers' emotional and behavioral problems
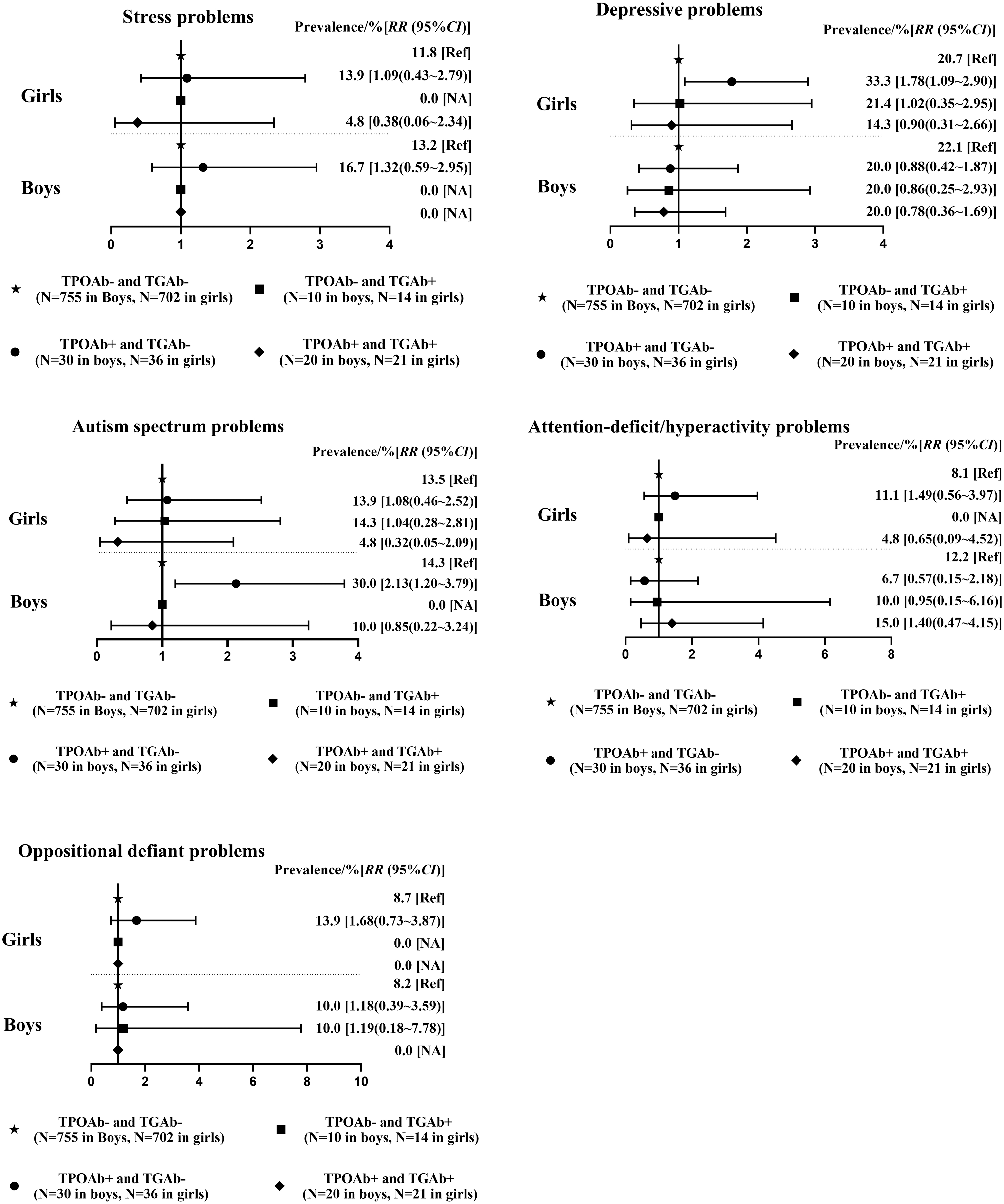
Boys born to mothers with TPOAb positivity in the first, second, and third trimesters of pregnancy had an increased risk of autism spectrum problems after adjusting for confounders, with RR [CI] of 2.01 [1.24–3.27], 2.15 [1.08–4.26], and 2.13 [1.20–3.79], respectively (Figs. 4 –6).
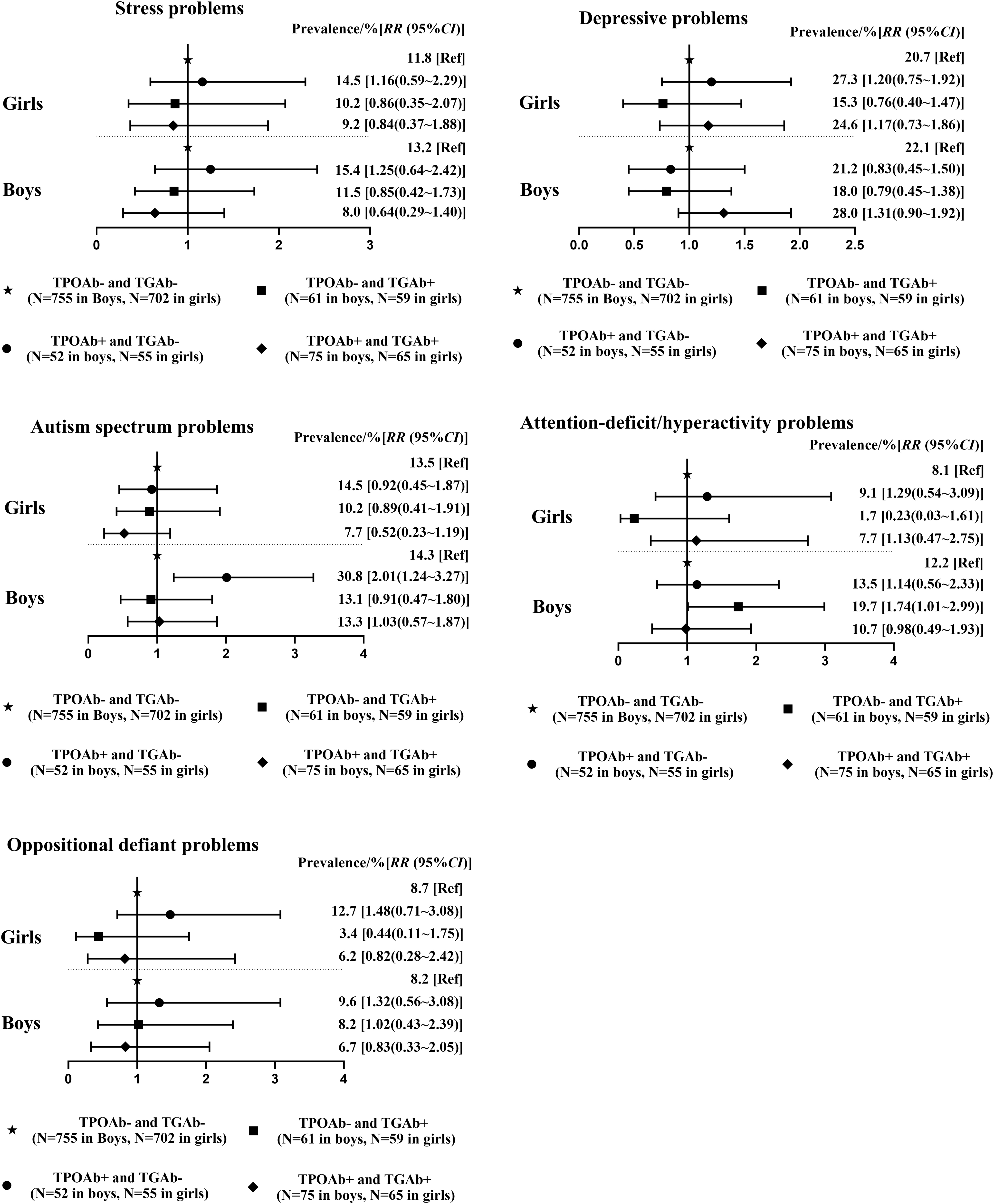
Poisson regression analyses on the correlation between maternal exposure of TPOAb and TGAb in the first trimester of pregnancy and preschooler's emotional and behavioral problems. TPOAb+ was defined as >34 IU/mL; TGAb+ was defined as >115 IU/mL; TPOAb−/TGAb− group meant that women had negative TPOAb and negative TGAb at all three trimesters; TPOAb+/TGAb− group meant that women had positive TPOAb in first trimester but had negative TGAb at all three trimesters; TPOAb−/TGAb+ group meant that women had positive TGAb in first trimester but had negative TPOAb at all three trimesters; TPOAb+/TGAb+ group meant that women had positive TPOAb and positive TGAb in first trimester. Negative TPOAb and negative TGAb as the control group; adjusted for maternal age, family income, maternal and paternal education levels, place of residence, parity, prepregnancy BMI, and smoking and alcohol drinking during pregnancy. Each group above the cutoff value N = 5 is considered reasonable. BMI, body mass index; TGAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody.
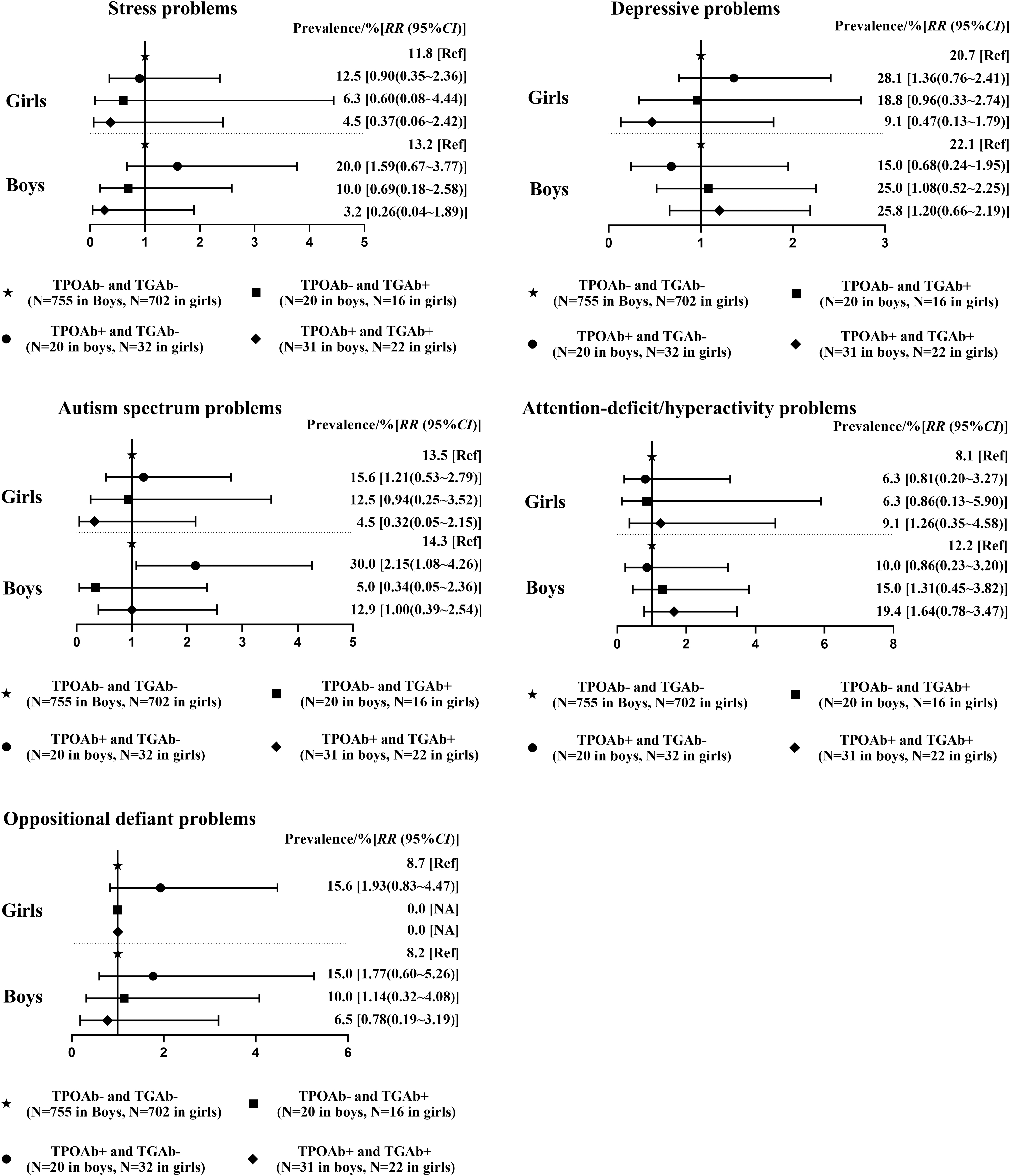
Poisson regression analyses on the correlation between maternal exposure of TPOAb and TGAb in the second trimester of pregnancy and preschooler's emotional and behavioral problems. TPOAb+ was defined as >34 IU/mL; TGAb+ was defined as >115 IU/mL; TPOAb−/TGAb− group meant that women had negative TPOAb and negative TGAb at all three trimesters; TPOAb+/TGAb− group meant that women had positive TPOAb in second trimester but had negative TGAb at all three trimesters; TPOAb−/TGAb+ group meant that women had positive TGAb in second trimester but had negative TPOAb at all three trimesters; TPOAb+/TGAb+ group meant that women had positive TPOAb and positive TGAb in second trimester. Negative TPOAb and negative TGAb as the control group; adjusted for maternal age, family income, maternal and paternal education levels, place of residence, parity, prepregnancy BMI, and smoking and alcohol drinking during pregnancy. Each group above the cutoff value N = 5 is considered reasonable.
Poisson regression analyses on the correlation between maternal exposure of TPOAb and TGAb in the third trimester of pregnancy and preschooler's emotional and behavioral problems. TPOAb+ was defined as >34 IU/mL; TGAb+ was defined as >115 IU/mL; TPOAb−/TGAb− group meant that women had negative TPOAb and negative TGAb at all three trimesters; TPOAb+/TGAb− group meant that women had positive TPOAb in third trimester but had negative TGAb at all three trimesters; TPOAb−/TGAb+ group meant that women had positive TGAb in third trimester but had negative TPOAb at all three trimesters; TPOAb+/TGAb+ group meant that women had positive TPOAb and positive TGAb in third trimester. Negative TPOAb and negative TGAb as the control group; adjusted for maternal age, family income, maternal and paternal education levels, place of residence, parity, prepregnancy BMI, and smoking and alcohol drinking during pregnancy. Each group above the cutoff value N = 5 is considered reasonable.
After adjusting for potential confounders, maternal TGAb positivity and TPOAb negativity in the first trimester were associated with a high risk of attention-deficit/hyperactivity problems in boys (RR = 1.74 [CI 1.01–2.99]) (Fig. 4). Maternal TPOAb positivity and TGAb negativity in the third trimester of pregnancy were associated with depressive problems in girls, with RR [CI] of 1.78 [1.09–2.90] (Fig. 6).
The sensitivity analysis did not fundamentally change the results of the main analysis (Supplementary Tables S3–S7 and 10).
Discussion
This cohort study showed that maternal TPOAb positivity in the pregnancy trimesters was associated with the risk of autism spectrum problems in boys. Isolated maternal TGAb positivity in the first trimester was associated with attention-deficit/hyperactivity problems in boys, whereas isolated maternal TPOAb positivity in the third trimester was associated with depressive problems in girls.
Whether the presence of maternal TAbs affects the neuropsychological development of the offspring remains controversial. The inconsistency in the findings could be attributed to the differences in the methods, sample sizes, 25 definition of antibody positivity, 26 and instruments used for assessing the offspring's neuropsychological development. 27 We observed that maternal TAb exposure correlated differently with the emotional and behavioral problems in boys and girls. Williams et al 28 found that the motor and perceptual abilities of the children of TGAb-positive mothers were lower than those of the children of TGAb-negative mothers. We also observed an isolated effect of maternal TGAb positivity on attention-deficit/hyperactivity problems in boys. A study from Belgium showed that women with isolated TGAbs had significantly higher serum TSH levels than those without thyroid autoimmunity. 28
Imaizumi et al 29 detected 12 fetal male cells with Y chromosome loci in the thyroid of 26 thyroglobulin-immunized pregnant mice. This indicates that the Y chromosome is related to the sex-related autoimmune response of thyroglobulin and may highlight the role of maternal TGAb exposure in boys.
The mechanism underlying the association between maternal TPOAb exposure and autism spectrum problems in boys and depressive problems in girls is unclear. Brown et al 9 found that the prevalence of maternal TPOAb positivity was significantly higher in children with autism spectrum disorders than in controls. Zhou et al 30 found that increased TPOAb levels in mice before pregnancy could increase the risk of postpartum depression by reducing the levels of brain-derived neurotrophic factors and serotonin in the prefrontal lobe. Some studies have indicated that the TPOAb may pass through the blood–brain barrier. 31,32 The Fc-γ receptor in the placenta primarily mediates the mother-to-infant transmission of immunoglobulin G (IgG) antibodies. 33,34 TPOAb belongs to the IgG class of antibodies, which can pass through the placental barrier. Therefore, it is speculated that the TPOAb passing through the placental barrier may reach the fetal brain through the circulation and affect the child's neurodevelopment.
However, further animal experiments are warranted to verify this.
This study has several strengths. To our knowledge, this is the first study that comprehensively examined the effects of the exposure to a combination of maternal TAbs on the children's emotional and behavioral development. In addition, based on a large-sample birth cohort study, information on exposure, outcome, and potential confounders was collected prospectively and accurately. Second, maternal TAbs were measured repeatedly during the pregnancy trimesters. Currently, few studies have focused on changes in the TAbs during pregnancy by conducting repeated assessments in the trimesters, which is the strength of our longitudinal study. GMM was adopted for fitting trajectories of TAbs throughout pregnancy to understand the dynamic TAb exposures better during pregnancy progression. It must be acknowledged that exploratory post hoc analyses are hypothesis generating.
To examine the association between TAb trajectories throughout pregnancy and the preschoolers' emotional and behavioral development, a post hoc analysis was performed using GMM that included the same covariates as those in the Poisson regression models.
This study has some limitations. First, the limited sample size made it difficult to stratify the participants with normal thyroid function according to various TAb exposures. However, we fully considered the possible effects of the thyroid hormone levels during each pregnancy trimester on the child's development. Sensitivity analyses, only including women with normal TSH levels according to trimester-specific reference ranges, were conducted to consider the possible effects of the thyroid hormone levels.
Second, researchers have found an association between TPOAb positivity and miscarriage. 35 –37 When we examined the association between maternal TAbs and children's behavioral development, including the live births was the only choice for sample selection. Nevertheless, the potential impact of TPOAb positivity cannot be ignored, as it might lead to severe diseases and subsequent miscarriage, which could cause bias in our data set. Moreover, this study did not distinguish women with assisted reproductive technology (ART), although some studies have suggested that ART can affect neurodevelopment in the offspring to a certain extent. 38
Third, caregivers with psychiatric disorders may easily report poor behaviors in children, 39 and major diseases of caregivers may affect the children's behavioral development. 40 However, there was a lack of emotional assessment and information on major diseases among the responders, that is, the main caregivers. Furthermore, adverse life events after birth, such as parental divorce/death, and serious illnesses in children may also affect their behavioral development. 41,42 A lack of such data may decrease the accuracy of the findings. Finally, the homogeneity between the comparison groups was not significant due to the limited sample size. Moreover, the findings should be cautiously explained in clinical applications.
In conclusion, exposure of maternal TAbs may be associated with emotional and behavioral development in children. Particularly, maternal isolated TPOAb positivity in all three trimesters of pregnancy may be associated with autism spectrum problems in boys. There may exist critical time windows of maternal TAb exposure on depressive problems in girls and attention-deficit/hyperactivity problems in boys.
Footnotes
Authors' Contributions
Y.T.: Study design, execution, analysis, article drafting, and critical discussion. P.L.: Study design and critical discussion. M.Y.: Study design and analysis. Y.H. and Y.X.: Data collection. S.Y., F.T., and K.H.: Study conception and design, interpretation of data, and critical discussion. We declare that all authors participated sufficiently in the work and take public responsibility for its content.
Acknowledgments
We thank the cohort field investigators Leijing Mao, Sanhuan Huang, and Zijian Liu for the entry of the questionnaire and the technicians Hong Gan and Yang Xie for technical assistance. In addition, we are grateful to Fu Zhang and Shanshan Zhang for laboratory measurements. We also thank Editage for English language editing.
Author Disclosure Statement
The authors including Y.T., P.L., M.Y., Y.H., S.Y., Y.X., F.T., and K.H. declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
The National Natural Science Foundation of China (81872630), The University Synergy Innovation Program of Anhui Province (GXXT-2020-067), Sci-tech Basic Resources Research Program of China (2017FY101107), the Special Project “Reproductive health, prevention and control of major birth defects” of National Key Research and Development Program (2016YFC1000204-2), the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2019PT310002), and the Research Fund of Anhui Institute of translational medicine (ZHYX2020A001).
Supplementary Material
Supplementary Data S1
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Table S11