
Abstract
Background:
A recent study showed that paternal subclinical hypothyroidism adversely affects the clinical outcomes of assisted reproductive technologies (ARTs). The aim of this study was to determine whether paternal serum-free thyroxine (fT4) concentrations within the reference range are associated with ART outcomes.
Methods:
This retrospective cohort study included 4066 couples who received 4894 ART treatment cycles in our clinic between April 1, 2016 and August 31, 2021. The differences in sperm parameters and ART outcomes across the paternal fT4 concentration tertiles were compared by using generalized linear models or generalized estimation equation models. The primary outcomes were clinical pregnancy rate (CPR) and live birth rate (LBR) per oocyte retrieval after the first embryo transfer cycle.
Results:
The mean ages of the males and their female partners were 32.8 (standard deviation, 5.0) and 30.7 (standard deviation, 4.1) years, respectively. No significant differences were observed in the sperm parameters or ART outcomes between the paternal fT4 concentration tertiles of the overall population. However, a stratified analysis of men aged ≥35 showed an adjusted CPR of 0.36 [confidence interval, CI: 0.27–0.45] for the lower paternal fT4 concentration tertile relative to the middle (adjusted rate: 0.45, CI: 0.38–0.53) and upper (adjusted rate: 0.43, CI: 0.36–0.51) tertiles (p for trend >0.05). The adjusted LBRs were 0.21 [CI: 0.15–0.30] for men aged ≥35 in the lower fT4 concentration tertile (p = 0.024, with reference to the upper tertile), 0.27 [CI: 0.21–0.35] for those in the middle tertile, and 0.30 [CI: 0.23–0.38] for those in the upper tertile. No differences in these outcomes were observed in men aged <35. The nonlinear smoothing curve obtained by using fT4 concentration as a continuous variable further supported these findings.
Conclusions:
Men of older reproductive age (≥35 years old) with low-normal fT4 concentrations within the reference range are associated with a decreased LBR. Future prospective studies are warranted to confirm the detrimental effects of low-normal paternal fT4 concentrations on ART outcomes.
Introduction
Subclinical hypothyroidism (SCH) refers to thyroid dysfunction with elevated serum thyrotropin (TSH) concentrations but normal serum-free thyroxine (free thyroxine [fT4]) concentrations. SCH is the most prevalent thyroid dysfunction in women of reproductive age, with a reported prevalence of 4–13% (1 –3). Maternal SCH has been shown to be associated with increased risks of miscarriage, pre-eclampsia, placental abruption, preterm birth, and neonatal mortality (4 –6).
Our recent study showed that SCH is associated with decreased ovarian reserves in women of late reproductive age (3). However, the effect of male thyroid function on reproduction has not been adequately investigated.
Thyroid hormone receptors are present in multiple cell types of male reproductive organs, such as germ cells, Sertoli cells, and Leydig cells (7,8). Thyroid hormones are known to play important roles in testicular development, steroidogenesis, and spermatogenesis (9,10). Our previous study reported that SCH affects up to 9.1% of men who receive infertility care (11). Paternal SCH is significantly associated with decreased clinical pregnancy and implantation rates in comparison to paternal euthyroidism, after in vitro fertilization (IVF)/intracytoplasmic sperm injection (ICSI), but this detrimental effect appears to manifest only in men aged ≥35 (11). It currently remains unclear whether variations in paternal thyroid function within the normal range are associated with pregnancy outcomes.
In this study, we aimed at investigating the associations between paternal fT4 concentrations within the reference range and sperm parameters, and the outcomes of IVF/ICSI.
Materials and Methods
Study population and design
The study design was approved by the Ethics Committee of the First Affiliated Hospital of Kunming Medical University, China. As a retrospective study, it was exempt from the requirement for informed consent of patients for the publication of data. This study was conducted at the Reproductive Medical Centre of the First Affiliated Hospital of Kunming Medical University between April 1, 2016 and August 31, 2021. Couples who received IVF/ICSI treatment were potentially eligible for participation in the study.
Patients' demographic and clinical data were recorded in detail in an assisted reproductive technology (ART) database. Clinical information, such as the history of infertility, infertility diagnosis, anti-Müllerian hormone (AMH) concentration, antral follicle count, basal reproductive hormone concentrations, ovarian stimulation details, male sperm parameters, and laboratory and clinical outcomes were retrieved from the ART database.
We included patients with up to three oocyte retrieval cycles in this study. Couples (cycles) were potentially eligible if: (i) they had IVF or ICSI cycles with autologous sperm and oocytes; (ii) the females were aged ≤38 years; (iii) they underwent first embryo transfer (fresh or frozen) cycles per oocyte retrieval, or they had no available embryos to transfer; and (iv) both the male and female partners had normal concentrations of free triiodothyronine (fT3), fT4, and TSH.
Couples were excluded if (i) either partner had a systemic or chronic disease such as cancer, hypertension, diabetes, or other endocrine diseases; (ii) the IVF/ICSI cycles they underwent used frozen sperm or sperm obtained through testicular/epididymal aspiration; (iii) either the male or female partner had any chromosomal abnormalities; (iv) the female partner had a uterine abnormality; or (v) no oocytes were retrieved, fertilized, or underwent oocyte freezing cycles. Finally, 4066 couples with 4894 cycles were included in the data analysis (Fig. 1).
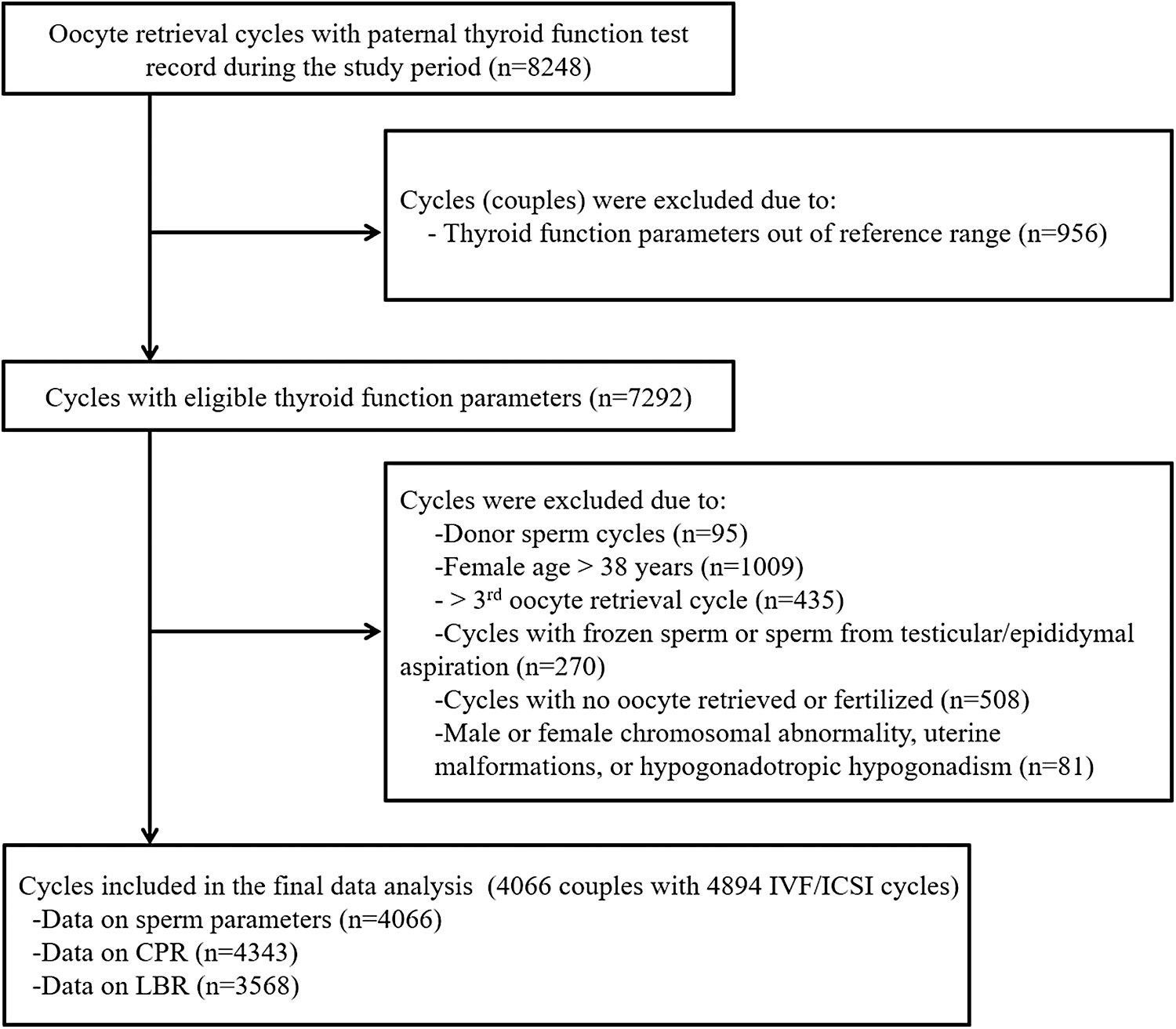
Flowchart for selection of the study population. CPR, clinical pregnancy rate; LBR, live birth rate.
We divided the cycles into three groups based on the following paternal fT4 concentration tertiles: lower tertile (12.00–15.33 pmol/L), middle tertile (15.34–18.67 pmol/L), and upper tertile (18.68–22.00 pmol/L). The differences in sperm parameters and ART outcomes between the cycles for different paternal fT4 concentration tertile groups were compared.
The primary outcomes of this study were clinical pregnancy rate (CPR) and live birth rate (LBR). The secondary outcomes were sperm parameters and the fertilization, good-quality embryo, blastocyst formation, and implantation rates. The fertilization rate was defined as the number of fertilized oocytes with two pronuclei divided by the total number of oocytes inseminated (IVF cycle) or injected (ICSI cycle). The good-quality embryo rate was calculated as the number of grade I and II embryos divided by the total number of embryos evaluated on day 3 (12).
The blastocyst formation rate was defined as the number of blastocysts divided by the number of embryos subjected to blastocyst culture. The CPR was defined as the number of pregnancies verified by the presence of an embryo with cardiac activity during early ultrasound divided by the number of embryo transfer cycles (11). Implantation was defined as a serum beta-human chorionic gonadotropin concentration >10 mIU/mL, usually measured 12–14 days after embryo transfer (13,14). The LBR was defined as the number of live birth cycles divided by the number of embryo transfer cycles.
Thyroid function test
The thyroid function parameters assessed in this study were TSH, fT3, fT4, thyroperoxidase antibody (TPO-Ab), and thyroglobulin antibody (Tg-Ab) concentrations. These parameters were measured by using an automated chemiluminescent immunoassay and a Cobas E601 analyzer (Roche Diagnostics GmbH, Mannheim, Germany), as previously described, (3,11). The following reference ranges provided by the manufacturer were used: 0.27–4.20 mIU/L, 3.1–6.8 pmol/L 12–22 pmol/L, <115.0 IU/mL, and <34 IU/mL for TSH, fT3, fT4, Tg-Ab, and TPO-Ab concentrations, respectively. Thyroid autoimmunity (TAI) was defined as having either a TPO-Ab concentration of ≥34 IU/mL or Tg-Ab concentration of ≥115 IU/mL.
Semen analysis
All male participants underwent routine semen analysis in accordance with the World Health Organization (WHO) criteria, Fifth Edition (15), before the initiation of ART. The semen analysis has been described in detail in our previous studies (11,16). Briefly, semen samples were collected by masturbation after 2–7 days of sexual abstinence. The semen volume was determined by weight. Sperm concentration and motility were examined by using a Sperm Class Analyzer (SCA-P-H-02; Microptic S.L., Barcelona, Spain). Sperm morphology was evaluated by using the Diff-Quick method, as previously described (11).
Ovarian stimulation, oocyte retrieval, fertilization, and embryo transfer
Ovarian stimulation protocols, such as gonadotropin-releasing hormone (GnRH) agonist or GnRH antagonist protocols, mild stimulation protocols, natural protocols, or progestin-primed ovarian stimulation protocols, were selected based on the age, health condition, and ovarian reserves of the women (11). After oocyte retrieval, fertilization was performed by either conditional IVF or ICSI. Embryo gradation was performed on the third day after fertilization. Blastocyst development was observed and evaluated on days 5–6 after fertilization based on the expansion degree and appearance of an inner cell mass and trophectoderm. At most, three cleavage-stage embryos or two blastocysts were transferred in a cycle. The remaining available embryos were frozen and thawed for frozen embryo transfer if the previous fresh embryo transfer cycle failed (11).
Statistical analysis
Data are presented as means (standard deviations) when normally distributed or as medians (interquartile ranges) otherwise. Demographic and clinical data were compared between patients in different paternal fT4 concentration tertiles by using analysis of variance, Kruskal–Wallis, or chi-square tests, as appropriate.
The associations between fT4 concentrations and semen parameters were analyzed by using generalized linear models. All of the semen parameters were log transformed to reduce skewness. The models were adjusted for male age (continuous), body mass index (BMI; continuous), duration of abstinence (categorical), TAI (categorical), smoking status (categorical), and alcohol consumption (categorical). The effect of paternal fT4 concentration on ART outcomes was analyzed by using generalized estimation equation models to account for patients who underwent multiple treatment cycles (17).
The laboratory outcomes (fertilization, good-quality embryo, and blastocyst formation rates) were analyzed by adjusting for parental age, BMI, male TAI, smoking, alcohol consumption, primary/secondary infertility, infertility diagnosis, ovarian stimulation protocol, and type of fertilization (IVF/ICSI). The clinical outcomes (CPR, implantation rate, and LBR) were analyzed by additionally adjusting for fresh/frozen cycles (categorical), the day of embryo transfer (cleavage or blastocyst, categorical), and the number of embryos transferred (categorical).
Our previous studies showed that the effects of thyroid dysfunction on male and female reproduction are age-dependent, in that only patients aged ≥35 were significantly affected (3,11). Therefore, we performed a subgroup analysis to investigate the effects of paternal fT4 concentration on sperm parameters and ART outcomes in men aged <35 and ≥35. Finally, generalized additive mixed models with smoothing splines were used to examine the potential nonlinear associations between paternal fT4 concentration and CPR and LBR (18,19).
Of the included couples, 14 had no data for TAI and were therefore excluded from the data analysis in all of these models. One hundred and seventy-two men had no data for sperm morphology due to severe oligoasthenospermia. Missing data for the laboratory outcomes were attributed to the failure of fertilization or lack of embryos subjected to blastocyst culture. Some data for clinical outcomes were missing due to either a lack of embryos available for transfer or ongoing pregnancies.
All of the tests were two-tailed, and p < 0.05 was considered to indicate statistical significance. SPSS v25.0 (SPSS, Inc., Chicago, IL), EmpowerStats (X & Y Solutions, Inc., Boston, MA), and R v3.6.3 (the R Foundation) were used for data analysis.
Results
Characteristics of the participants
Based on the inclusion and exclusion criteria, 4066 couples who cumulatively underwent 4894 oocyte retrieval cycles were included in the study. We allocated 446 couples (558 cycles), 1956 couples (2344 cycles), and 1664 couples (1992 cycles) to the lower, middle, and upper paternal fT4 concentration tertile groups, respectively. We obtained complete follow-up data for CPR for 4343 cycles and LBR for 3568 cycles. The mean ages of the males and their female partners were 32.8 (standard deviation, 5.0) and 30.7 (standard deviation, 4.1) years, respectively. The ages of both the men and their female partners were significantly different across the three groups (both p < 0.001). The demographic and clinical data for the included patients (cycles) are presented in Table 1.
Characteristics of Included Participants
p values in bold indicates significant difference.
Data on TAI are missing in 14 men.
Data are presented as the number of cycles.
AMH, anti-Müllerian Mullerian hormone; BMI, body mass index; fT3, free triiodothyronine; fT4, free thyroxine; ICSI, intracytoplasmic sperm injection; IQR, interquartile range; IVF, in vitro fertilization; SD, standard deviation; TAI, thyroid autoimmunity; TSH, thyrotropin.
Associations between fT4 concentration and semen parameters
After adjusting for potential confounders, we found that all sperm parameters, including semen volume, sperm concentration, total sperm count, progressive sperm motility, and normal sperm morphology, were similar across men in the different fT4 concentration tertiles, as shown in Table 2.
Associations Between Free Thyroxine Concentration and Sperm Parameters in the Overall Population
Data are missing in 172 men.
CI, confidence interval; Ref., reference.
The stratified analysis showed that, in men aged <35, the semen volume was slightly lower in men in the lower fT4 concentration tertile when using the upper tertile as reference (adjusted mean: 3.6 mL vs. 3.8 mL, p = 0.05). The proportion of men with normal sperm morphology was slightly but significantly higher in the lower fT4 concentration tertile relative to the upper fT4 concentration tertile (adjusted mean: 7.5% vs. 7.1%, p = 0.04). Other sperm parameters were similar between the tertiles. In men aged ≥35, no significant differences in any of the parameters were found between those in different fT4 concentration tertiles (all p > 0.05), as shown in Supplementary Table S1.
Associations between paternal fT4 concentration and ART outcomes
In the overall population, none of the ART outcomes were significantly different between the fT4 concentration tertiles. The CPRs for cycles associated with paternal fT4 concentrations in the lower, middle, and upper tertiles were 0.40 [confidence interval, CI: 0.35–0.46], 0.46 [0.42–0.50], and 0.43 [0.39–0.47], respectively (p > 0.05). The LBRs for these three groups were 0.29 [CI: 0.24–0.35], 0.34 [0.29–0.38], and 0.32 [0.28–0.36], respectively (p > 0.05), as shown in Table 3.
Associations Between Free Thyroxine Concentration and Assisted Reproductive Technology Outcomes in the Overall Population
ART, assisted reproductive technology.
A stratified analysis based on paternal age (Table 4) showed that none of the laboratory or clinical outcomes were significantly different between the different fT4 concentration tertiles in men aged <35. For men aged ≥35, the fertilization, good-quality embryo, and blastocyst formation rates were all similar between the different fT4 concentration tertiles. The adjusted CPRs for men in the lower, middle, and upper fT4 concentration tertiles were 0.36 [CI: 0.27–0.45], 0.45 [0.38–0.53], and 0.43 [0.36–0.51], respectively. These values were not significantly different between groups (p for trend >0.05). The adjusted LBRs were 0.21 [CI: 0.15–0.30] for men aged ≥35 in the lower fT4 concentration tertile (p = 0.024, with reference to the upper tertile), 0.27 [0.21–0.35] for those in the middle tertile, and 0.30 [0.23–0.38) for those in the upper tertile. The LBRs were not significantly different across the paternal fT4 concentration tertiles for men aged <35 (p for trend >0.05). The nonlinear smoothing curve further supported these findings, as shown in Figure 2.
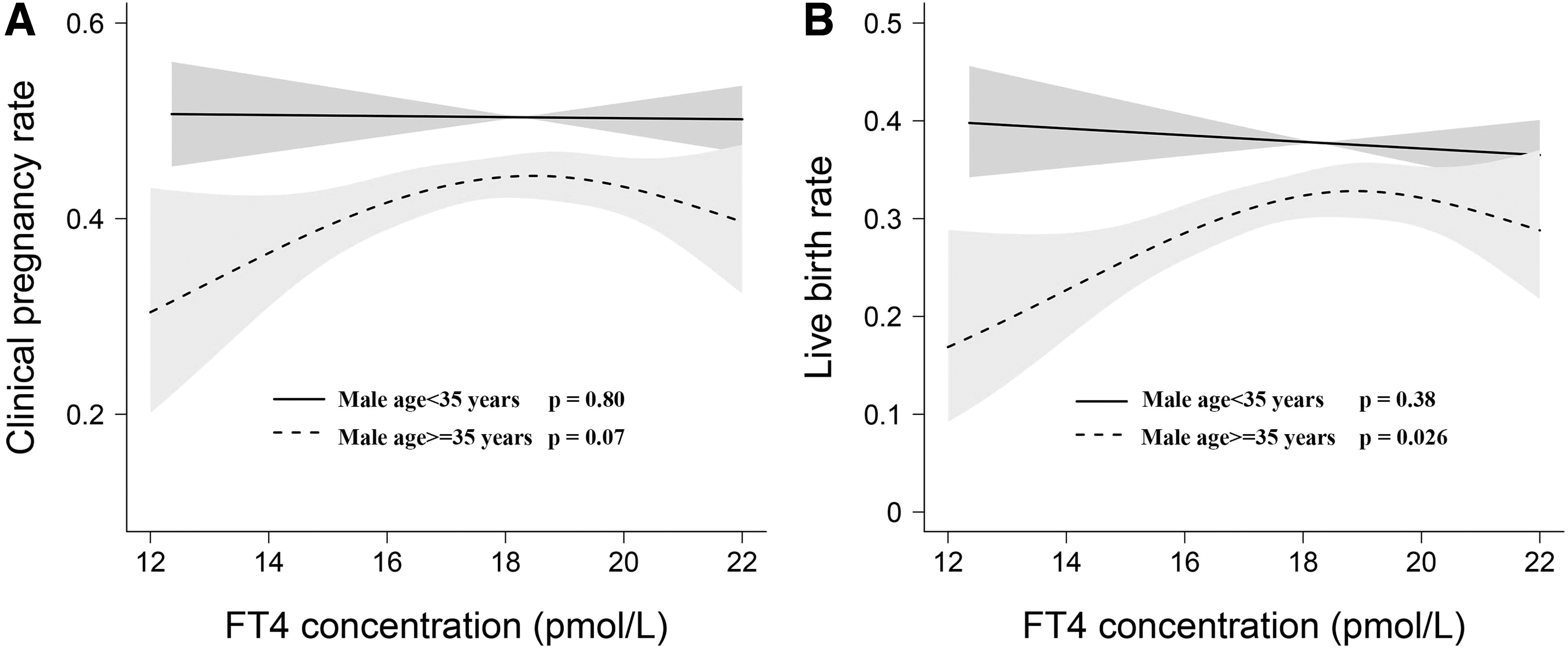
Association between paternal fT4 concentrations and ART outcomes as analyzed by using generalized additive mixed models with smoothing splines. Solid lines indicate response curves, and dotted lines indicate confidence intervals. (
Associations Between Free Thyroxine Concentration and Assisted Reproductive Technology Outcomes in Different Male Ages
p values in bold indicates significant difference.
Paternal fT4 concentration was not significantly associated with CPR in men aged ≥35 (p = 0.07) or in men aged <35 (p = 0.80; p for interaction = 0.31). Nevertheless, a significant negative association was observed between paternal fT4 concentration and LBR in men aged ≥35 (p = 0.026), but not in men aged <35 (p = 0.38; p for interaction = 0.043).
Discussion
To the best of our knowledge, this is the largest study of its kind to investigate the association between paternal thyroid function and male fertility and the first study to evaluate the association between normal-range paternal fT4 concentrations and ART outcomes. The results showed that an fT4 concentration within the reference range was not significantly associated with routine sperm parameters or ART outcomes in the overall population. However, men aged ≥35 with low-normal fT4 concentrations (lower tertile, 12.00–15.33 pmol/L) exhibited a significantly lower LBR than men with fT4 concentrations in the upper tertile (18.68–22.00 pmol/L). This association was not observed in men aged <35.
Several studies have investigated the effect of thyroid dysfunction on male reproductive function, but all of them have focused on overt thyroid dysfunction. Animal and human studies have shown that hypothyroidism has an adverse effect on spermatogenesis (20,21). A study conducted in 2015 with a small sample size showed no significant differences in sperm parameters between men with euthyroidism, SCH, and subclinical hyperthyroidism. However, they observed a positive relationship between fT4 concentration, semen volume, and seminal fructose concentration (22). Recently, Condorelli et al. conducted an in vitro study to evaluate the effects of levothyroxine (LT4) on sperm parameters, in which sperm from euthyroid men with idiopathic infertility was treated by using LT4. They found that the mitochondrial function and DNA integrity of the sperm improved after treatment (23), indicating a potential application of LT4 in treating idiopathic male infertility. In our population-based study, we did not find any significant effects of fT4 concentration on sperm parameters, barring the observation that men with lower fT4 concentrations had a slightly lower semen volume and a higher proportion of sperm with normal morphology.
In contrast to the evidence for associations between maternal thyroid dysfunction and pregnancy outcomes, evidence for the effect of paternal thyroid functional status on pregnancy outcomes is limited. Recently, our cohort study of 2511 couples showed that paternal SCH is significantly associated with decreased clinical pregnancy and implantation rates after IVF/ICSI. However, LBR was not analyzed in that study (11). In the current cohort, we found worse clinical outcomes in men with low-normal fT4 concentrations, but these effects were only observed in men aged ≥35. As the regulatory mechanisms underlying the role of thyroxine in spermatogenesis and sperm function remain largely unknown and no studies have investigated the association between normal-range thyroxine concentrations and sperm function, we hypothesize that epigenetic alterations may be a crucial modulator of the effect of thyroid hormones on sperm fecundity. Epigenetic alterations of sperm may also affect embryonic development. Indeed, studies have reported that altered thyroid hormone concentrations change the epigenetic information of the male germline, with consequences for gene expression programs in the brain, behavior, development, and hypothalamic–pituitary–thyroid axis of the progeny (24,25). DNA methylation and histone modifications have also been reported to be regulated by thyroid hormones in rat astrocytes (26). In addition, spermatozoa contain functional RNAs that are delivered to oocytes during fertilization and likely affect fertilization, embryo development, offspring phenotypes, and possibly, future generations (27 –31). However, data on the epigenetic alterations underlying the effects of thyroid dysfunction on spermatozoa are limited. Future studies are warranted to clarify this issue.
Similar to advanced maternal age, advanced paternal age has been associated with adverse outcomes in offspring, particularly with respect to psychiatric disorders, miscarriages, stillbirths, and several birth defects (32 –34). These adverse outcomes may be partially explained by an increased number of sperm DNA strand breaks, genetic imprinting errors, and chromosomal anomalies (35,36) as sperm DNA fragmentation increases with age, most likely due to decreased antioxidant capacity and increased levels of reactive oxygen species (37,38); this may impair the functional and structural integrity of sperm (39) and eventually affect fertilization, embryo quality, and implantation (40).
Therefore, aging may have an additive effect on low-normal fT4 concentrations, which may explain our observation of only men aged ≥35 showing a statistically significant difference in LBR based on fT4 concentration. Thus, the results of this study suggest that aging may amplify the negative effects of low-normal paternal fT4 concentration on pregnancy outcomes.
This study has several strengths. First, the sample size was large and strict inclusion and exclusion criteria were applied. Second, as the study was conducted in a single center, fertilization and embryo cultures were performed under the same conditions, thereby minimizing inter-assay variability. Third, a series of potential confounders were incorporated in the data analysis to account for potential bias. However, this study also has several limitations. First, due to its retrospective design, a causal relationship between paternal fT4 concentration and ART outcomes could not be established. Second, a type II error resulting from selection bias could not be excluded as all of the participants were recruited from a single center. Third, the study participants were patients who sought fertility treatment, which may have biased our results on the associations between fT4 concentration and sperm parameters. In addition, as the sample size was not large enough to perform stratified analysis based on additional paternal age subgroups (e.g., every 5 years as a subgroup), a study with a larger sample size should be conducted in the future to establish the specific range of paternal age during which reproductive function is affected.
In conclusion, the results of this study suggest that low-normal paternal fT4 concentrations within the reference range are associated with worse ART outcomes, especially a lower LBR. However, these associations were only observed in men aged ≥35. Future prospective studies are warranted to confirm the detrimental effects of low-normal paternal fT4 concentrations on ART outcomes and to evaluate whether LT4 supplementation improves the LBR for older men with relatively low-normal fT4 concentrations. Further fundamental research is also required to elucidate the molecular mechanisms underlying the regulatory effects of paternal fT4 concentration on embryo development.
Data Availability
Some or all datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions
M.R., S.Z., and L.T. designed the study. L.W., G.Y., and M.C. collected the data. S.Z. and M.R. performed the data analysis and wrote the article. All of the authors contributed intellectually to the revision of the article and approved the final version.
Acknowledgments
The authors thank all the patients who participated in their study. They acknowledge the professional article editing services of Armstrong–Hilton Ltd.
Author Disclosure Statement
All the authors have no competing financial interests.
Funding Information
This study was supported by the Basic Research Project of the Yunnan Province-Outstanding Youth Foundation (No. 202101AW070018), the “1000 Talent Plan” of Yunnan Province (No. RLQN20200001), and the Health Commission of Yunnan Province under Grant (No. D-2017021).
Supplementary Material
Supplementary Table S1