
Abstract
Background:
Metastatic anaplastic thyroid cancer (ATC) has a poor prognosis. This pilot study aims to evaluate tremelimumab plus durvalumab with stereotactic body radiotherapy (SBRT) to improve overall survival (OS).
Methods:
Eligible patients received up to 4 doses tremelimumab (75 mg) given q4 weeks and up to 1 year of durvalumab (1500 mg) given q4 weeks. SBRT at 9 Gy × 3 fractions was given within the first 2 weeks of the start of treatment. Paired biopsies (pretreatment and between 3 and 10 weeks after the first dose of the drug treatment) were done in the medically qualified patients. Major inclusion criteria are metastatic ATC, Eastern Cooperative Oncology Group (ECOG) performance status 0–2, no prior immunotherapy, and last anticancer treatment >7 days before starting the study. The primary endpoint was 1 year OS with the combination of durvalumab, tremelimumab, and SBRT in metastatic ATC patients with a target of 1 year OS in ≥2 out of 12 patients.
Results:
A total of 13 patients signed consent but only 12 patients ultimately participated in this trial. One patient who consented to the protocol became ineligible for this study due to continued decline in performance status. Patient characteristics were as follows: male (n = 6) with a median age of 71 years (range: 49–82), and ECOG = 1. Nine patients had prior neck radiation and nine patients had prior chemotherapy. Next-generation sequencing and PD-L1 staining were done in the nine patients where tissue was available. High microsatellite instability (MSI) corresponding to mismatch repair defect was noted in two patients. There were zero confirmed responses and only one patient had stable disease and was treated with ≥4 cycles of study drugs. The median time that the patients were under treatment was 11 weeks (1–28 weeks). MSI status did not affect treatment response. High MSI patients were on treatment for 8–14 weeks before disease progression. The median OS was 14.5 weeks with only 1 patient alive beyond 1 year. The presence of a BRAF or p53 mutation did not appear to affect treatment outcome.
Conclusions:
Tremelimumab and durvalumab with SBRT did not improve OS for ATC. Future research is needed to examine other novel immunotherapy combinations with or without radiotherapy in the treatment of ATC. Clinical Trial Registration: NCT03122496.
Introduction
Anaplastic thyroid cancer (ATC) is a rare and highly aggressive cancer. The median survival is ∼6 months for localized nonmetastatic disease with a reported 1-year overall survival (OS) rate ranging between 20% and 40% from the time of diagnosis (1,2). A high variability in ATC OS may be attributed to a mixture of poorly differentiated tumors that are sometimes misdiagnosed as having ATC, the former having the better prognosis.
Within the ATC family, the prognosis of an incidental finding of ATC in a background of papillary thyroid cancer at the time of surgery is far more superior than the ATC that is the result of multiple thyroid cancer recurrences or the de novo ATC cases that have the worse prognosis (1 –4). The American Thyroid Association has an updated guidelines for the management of ATC, advising individualized care to optimize patient outcomes (5).
Patients with metastatic ATC have an extremely poor prognosis, where <10% of patients are alive at 1 year (6). The National Comprehensive Cancer Network guidelines recommend a limited number of treatment options that include doxorubicin, paclitaxel, and platinum-based agents, however, responses to these treatments are not durable and have not been shown to affect OS (7). Despite activity in differentiated thyroid cancer, multikinase angiogenesis inhibitors in ATC have demonstrated only modest activity in phase II studies (8 –10). In particular, only 2 of 15 patients treated with sorafenib responded, 1 of 2 patients treated with axitinib, and none of 14 patients treated with pazopanib responded.
Lenvatinib has shown mixed response for metastatic ATC, with one study reporting an objective response rate of 24% while another reporting the response being short lived (11,12). Recently, however, targeted treatment for the 20–50% of patients with BRAFV600 mutations has been reported to show promising efficacy, with an overall response rate of 56% (13). The 12-month progression-free and OS rates were reported to be 43.2% and 51.7%, respectively, and the 24 months OS rate was 31.5% (13). In one series, metastatic BRAF mutant ATCs experienced a remarkable 69% (11 of 16; confidence interval, 41–89%) overall response rate when treated with BRAF inhibitor dabrafenib (150 mg twice daily) plus the MEK inhibitor trametinib (2 mg once daily).
Median duration of response, progression-free survival, and OS were not reached as a result of a lack of events, with 12-month estimates of 90%, 79%, and 80%, respectively. In a recent publication of ATC patients including those with stage IVC disease, Maniakas et al. also demonstrated an improved OS with the use of dabrafenib and trametinib for their BRAF mutant ATC patients (14).
The thyroid is one of the most immunogenic organs in the body and often affected by diseases of autoimmunity. Checkpoint blockade with anti-CTLA-4 and programmed death ligand 1 (anti-PD-1) may commonly lead to thyroiditis (15). Antithyroid autoimmune thyroiditis is often observed in patients with metastatic melanoma treated with ipilimumab, a monoclonal antibody against CTLA-4 (16). PD-L1 and PD-L2 receptors are also expressed in aggressive thyroid cancer (15). Capdevila et al. reported a remarkable response rate of 19% for locally advanced and metastatic ATC with the use of single agent spartalizumab that is a PD-1 inhibitor (17).
Of note, only 90% of the enrolled patients truly were ATC and >40% of the patients did not have prior lines of therapy (17). However, others have reported that the response to single agent PD-1 antibody can be delayed for ATC (18). A phase II study of ipilimumab (antibody to CTLA-4) and nivolumab (antibody to PD-1) was reported to show a 30% response rate but only in 10 patients (19). Due to the aggressive and rapidly growing nature of ATC, targeting both CTLA-4 and PD-L1 may augment the response rates. This combination has been shown to be beneficial in melanoma, where higher and quicker response rates are observed, compared with either agent alone (20,21).
Lastly, there is also unpublished data that suggest ATC with high mutation load and high tumor t-cell infiltrate may respond better to checkpoint inhibitors. We have previously reported that ATC has a tumor mutational burden (TMB) of ∼6 mutations/Mbp, which is not unusually high in solid malignancies, but is high in relationship with other thyroid cancers (22,23).
In mice, an abscopal response was observed by Deng et al. (24) when an anti-PD-L1 antibody was given either one day before or on the same day of high dose stereotactic body radiotherapy (SBRT). Golden et al. (25) demonstrated an abscopal effect seen with the combination of ipilimumab and radiation in NSCLC adenocarcinoma. In this study, radiotherapy was delivered one day before the ipilimumab treatment.
In a phase II randomized lung cancer trial of pembrolizumab with or without SBRT, the study's prespecified endpoint criteria for meaningful clinical benefit were not met, however, a doubling of overall response rate was observed (26). McBride et al. (27) did not observe enhanced response rates in a phase II randomized trial for metastatic head and neck squamous cell carcinoma treated with nivolumab with or without SBRT.
Recognizing the poor prognosis and the paucity of immunotherapy data for metastatic ATC, we initiated this pilot study. We hypothesized that PD-L1 inhibition using durvalumab (MEDI4736) and CTLA-4 inhibition using tremelimumab, targeting two nonredundant pathways combined with SBRT, could lead to an OS benefit for metastatic ATC. The benefit of the addition of SBRT to checkpoint inhibition to augment response may currently be considered questionable, however, we initiated this trial in 2017. Furthermore, at the time this trial was initiated, it was unknown that BRAF and MEK inhibition could lead to improved survival for mutant ATC. Our study was presented both at the 2019 American Society of Clinic Oncology and at the 2019 American Society of Therapeutic Oncology Convention (28,29).
Methods
Patient inclusion and exclusion criteria
This phase I study was approved by Memorial Sloan-Kettering Cancer Center IRB, MSKCC IRB#17-108 (
Patients were required to have an absolute neutrophil count ≥1.5 × 109/L, hemoglobin ≥9.0 g/dL, platelet count ≥100 × 109/L, serum bilirubin ≤1.5 × upper limit of normal, AST and ALT within the parameters of ≤2.5 times the upper limit of normal without liver metastases, or ≤5 times the upper limit of normal with adequate renal function with known liver metastases. Prior RT was permitted, so long as it was not the same lesion that received SBRT.
Patients were excluded if they had previous treatment with an anti-CTLA4, anti-PD-1, or anti-PD-L1 agent, current or prior use of immunosuppressive medication within 28 days before the first dose of durvalumab or tremelimumab; any prior Grade ≥3 immune-related adverse events as a result of any immunotherapy agent; active or prior autoimmune disease within 2 years of study entry; active or prior documented inflammatory bowel disease; confirmed pneumonitis or interstitial lung disease; and history of leptomeningeal carcinomatosis or active brain metastases receiving concurrent treatment inclusive of but not limited to surgery, radiation, and/or corticosteroids.
Treated brain metastases were permitted if there had been no evidence of progression for at least 8 weeks after treatment on magnetic resonance imaging (MRI). Intranasal and inhaled or systemic corticosteroids at physiological doses ≤10 mg/day or any corticosteroids for >4 consecutive days were allowed. Patients were recruited by the principle investigator (PI) (N.Y.L.) and Co-PI (E.S.) who knew the study well and only approached patients who were deemed eligible for this study.
Treatment
Patients received durvalumab and tremelimumab given together every four weeks (one cycle). Image-guided SBRT at 9 Gy for 3 fractions were delivered, in line with standard treatment guidelines, to 1 metastatic lesion within 2 weeks after the start of the first cycle of durvalumab and tremelimumab to allow flexibility in scheduling and radiation planning. After 4 cycles of durvalumab and tremelimumab, patients continued with single agent durvalumab every 4 weeks until disease progression or unacceptable toxicity for a total of 12 months from date of initial treatment (Fig. 1).
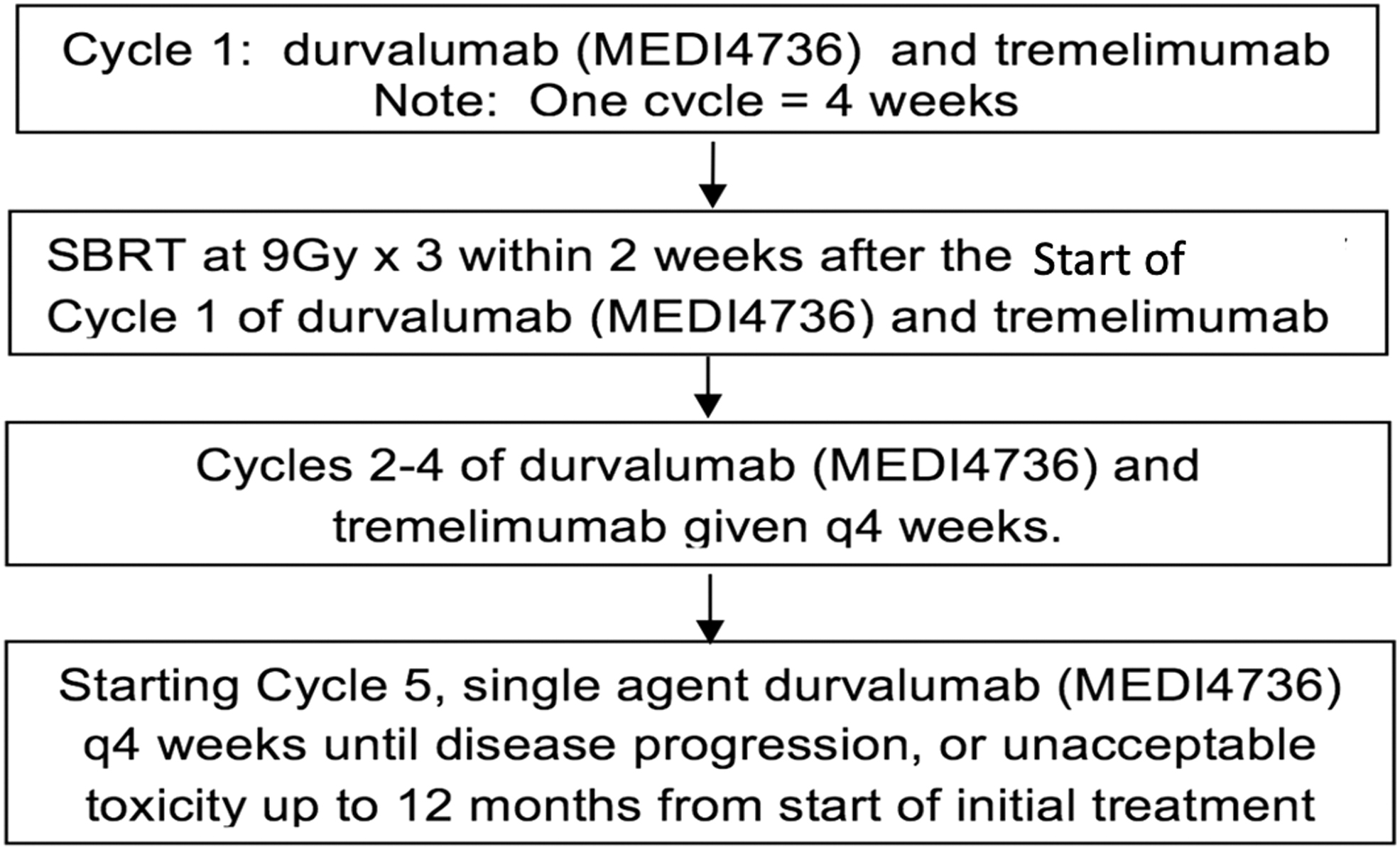
Treatment schema.
Restaging scans were performed every two cycles. If progression of disease was observed, patients could remain on study treatment for an additional cycle with another scan and, if at that time progression of disease was not seen, patients could continue on study. Furthermore, if all lesions are progressing, and up to five separate lesions were amenable to palliative RT, the patient remained on study while these areas were being irradiated.
If a patient completed 12 months of treatment and later developed progression of disease, treatment with durvalumab only could be restarted, as long as additional informed consent was provided. A flat dose of 1500 mg durvalumab for patients >30 kg intravenous (IV) was administered. For patients ≤30 kg, dose will be 20 mg/kg. A flat dose of 75 mg tremelimumab for patients >30 kg was administered IV. For patients ≤30 kg, dose will be 1 mg/kg.
Primary and secondary endpoints
The primary endpoint was OS at one year with the combination of durvalumab, tremelimumab, and standard-of-care SBRT in patients with metastatic ATC. OS was defined as the time from initiation of therapy to the date of death from any cause. For patients who are alive, their survival time will be censored at the date of last contact. Our preplanned hypothesis stated that this combination regimen would be worthy of further evaluation if at least 2 out of 12 patients were alive and still under observation at 12 months. Metastatic ATC has poor prognosis of <10% 1-year OS.3
We hypothesize that 1-year OS will be improved 25% with this combination of treatment. This decision rule has the following probabilities of missing an effect (observing 0 or 1 survivors out of 12 patients and thus declare failure of the protocol) at the various true 1-year rates of success (i.e., being alive and still under observation).
Overall response rate is defined as the number of patients with a best overall response of complete response or partial response in nonirradiated lesions during the one-year period after initiation of treatment divided by the total number of patients on the study. Response was evaluated using Response Evaluation Criteria in Solid Tumors (RECIST) 1.1. Another secondary endpoint was progression-free survival. Treatment-related adverse events were assessed using Common Terminology Criteria for Adverse Events version 4.0 (CTCAE v4.0).
Next-generation sequencing and PD-L1 staining
Patients with sufficient tumor material underwent targeted next-generation sequencing of their tumors with Memorial Sloan Kettering-integrated mutation profiling of actionable cancer targets (MSK-IMPACT), which has been previously described in detail (30). In brief, MSK-IMPACT is a hybridization and capture-based assay that for patients in this cohort captured all exons and selected introns in 468 cancer-related genes. Sequencing was performed in a Clinical Laboratory Improvement Amendments environment with both tumor and matched normal to identify somatic related cancer alterations and compute TMB. Microsatellite instability (MSI) status was determined by using MSI-Sensor (31) in tumors that had a TMB of at least 10 mutations.
PD-L1 immunostaining was also performed on patients with sufficient material using clone E1L3N (dilution 1:400; Cell Signaling Technologies, Danvers, MA). PD-L1 staining was quantified separately on tumor and immune cells, and then a combined positivity score (CPS) was determined. PD-L1 staining was quantified separately on tumor and immune cells, and then a CPS was determined.
Results
Patient characteristics/treatment compliance
From April 28, 2017, to October 5, 2018, 13 patients signed consent to MSKCC IRB 17-108 but only 12 patients were eligible and underwent protocol treatment. One patient who consented to the protocol was admitted to urgent care before starting protocol treatment and was deemed no longer eligible for protocol due to decreased performance status. See Table 1 for details of the 12 patients including prior lines of therapies. During this time, all consecutive potentially eligible patients were approached by the PI and the co-PI and were consented to the study. Furthermore, there were no other competing protocols at the same time when this trial was open for patient enrollment.
Patient Characteristics
ECOG, Eastern Cooperative Oncology Group; F, female; M, male; RT, radiation therapy.
See Figure 2 for a flow chart of patients enrolled. The median age was 71 years (range, 49–88); 50% of the patients were male. ECOG performance was as follows: 0, n = 5; 1, n = 6, 2, n = 1. Nine patients had previously received definitive RT to the neck with a median dose of 70 Gy (range: 40–70 Gy) with chemotherapy of whom all received doxorubicin except for 2 patients who received carboplatin/paclitaxel. Five patients (42%) received prior systemic therapy (not including those getting chemotherapy with RT only). Two patients also received prior palliative radiation: stereotactic radiosurgery for a brain metastasis, palliative radiation to a bony painful lesion.
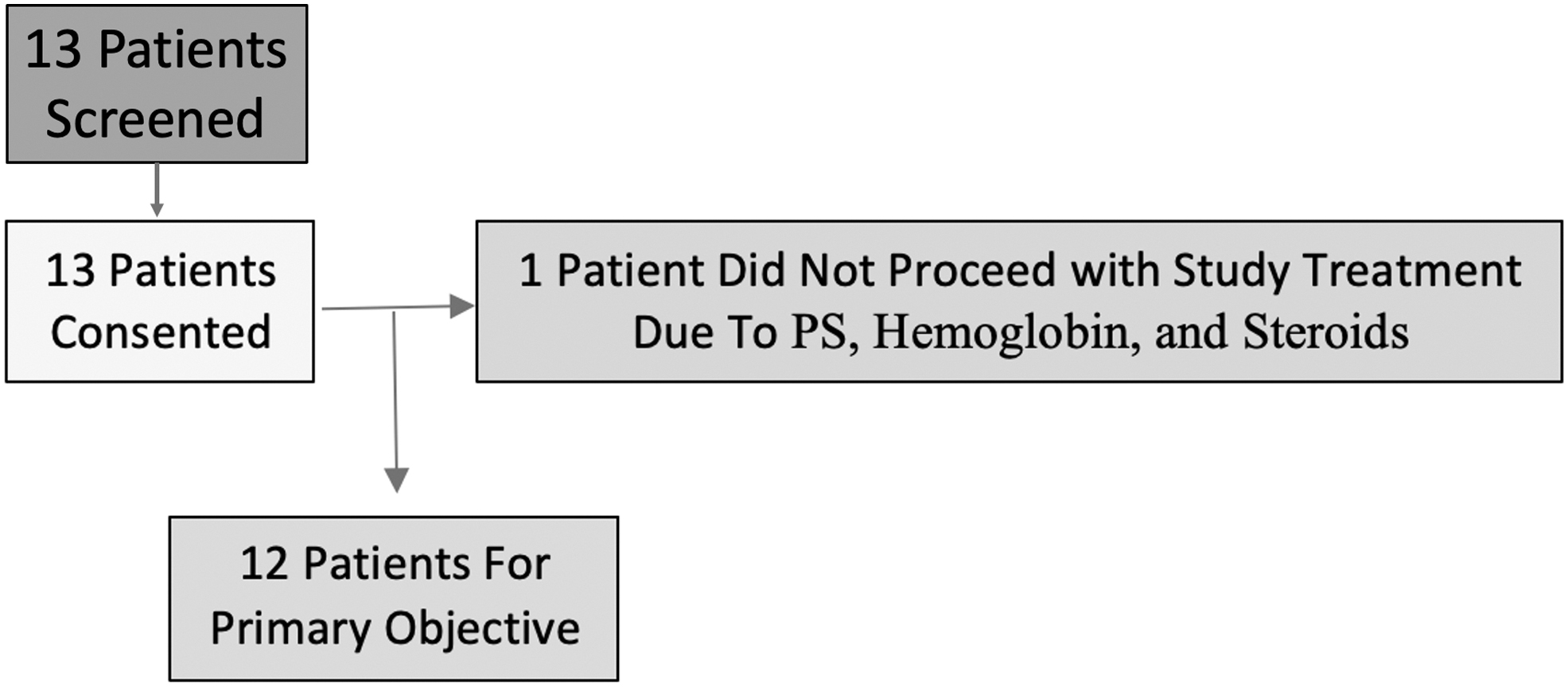
Patient flow chart.
Patients were able to tolerate treatment and none was removed from the study due to toxicities of treatment. SBRT sites were as follows: lung, n = 5; bone, n = 4; lymph node, n = 2; liver, n = 1. The median time patient was on treatment was 11 weeks (range 1–36 weeks). One patient required SBRT to a brain metastasis while on therapy (Fig. 3).

Median duration of treatment.
Toxicities patients experienced were dysphagia, fatigue, dyspnea, hypertension, cough, constipation, and edema. Every patient experienced at least ≥ grade 2 toxicities. Seven patients had ≥ grade 3 toxicity and 2 patients experienced grade 4 events, including 1 patient with respiratory failure largely due to progression of disease and 1 patient with pancreatitis (with increased lipase and amylase levels).
Treatment outcomes
The median OS was 104 days (range was 12–622 days). Two-thirds of the patients survived 3 months, 25% survived 6 months, and 17% survived 9 months. Only 1 patient lived beyond 1 year. RECIST reads were not done for those who came of the study before the formal first follow-up RECIST reads were done. One patient had an unconfirmed partial response at the first follow-up but then progressed on the second follow-up due to a new nontarget lesion.
Only 1 patient had stable disease beyond 15 weeks. The median time on treatment was 11 weeks, with a range of 1–36 weeks. All reported adverse events can be found in the Supplementary Table S1. Treatment was overall well tolerated with most adverse events being grade 1 or 2, most notably cough and constipation. Table 2 gives all the reported serious adverse events with one grade 4 respiratory failure that could also be attributed to disease.
Serious Adverse Events
Correlative analysis
Nine patients underwent next-generation sequencing and nine had sufficient material for PD-L1 staining. Exploratory analysis of the mutational profile, TMB, and PD-L1 staining (CPS) with clinical outcomes is illustrated in Figure 4. Of note, two patients were noted to have MSI status, although neither patient had a response. One patient with MSI lived the longest but was noted to have modest radiographic increase in tumor on his first scan and developed intracranial progression of disease.
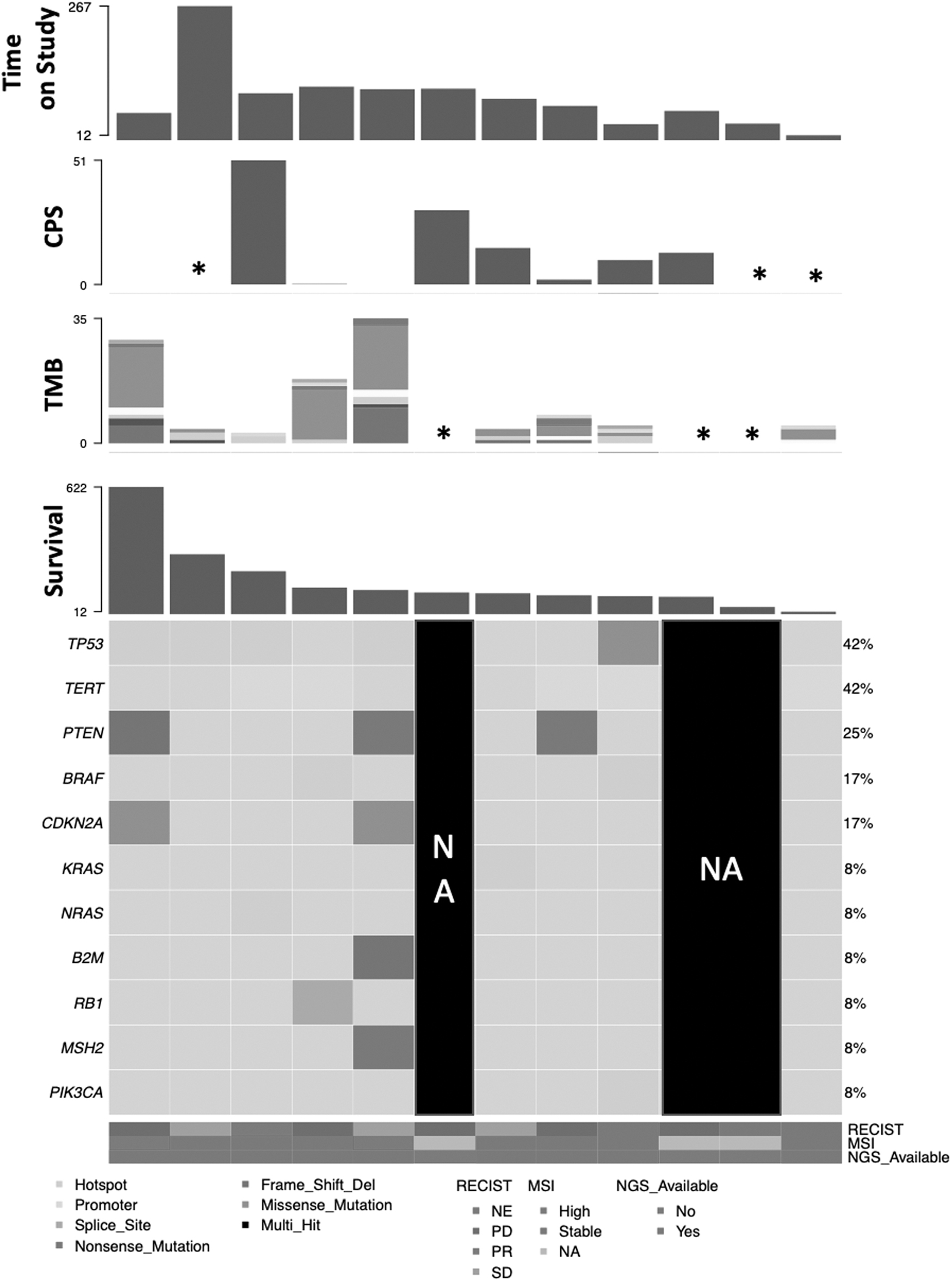
Onco-print of cohort with TMB, PD-L1, and MSI status. Patients organized by duration of survival. *Indicates cases wherein data are unavailable for either TMB or CPS. Note all 12 patients are visualized, but next-generation sequencing and PD-L1 status were available for 9 of 12 patients. CPS, combined positivity score (PD-L1 staining); MSI, microsatellite instability; TMB, tumor mutational burden.
The second patient with high MSI notably had ATC develop from a prior treated poorly differentiated (Hurthle cell) thyroid cancer. Interestingly, this patient had a concurrent B2M mutation, which has previously been suggested to be associated with immune evasion (32). One patient with an unconfirmed partial response had the highest CPS in the cohort. Lastly, patients with >10 mutations/Mb (N = 3 patients) (33) survived on average 290 days compared with 138 patients with ≤10 mutations/Mb (n = 6 patients). Two patients had Foundation One sequencing that showed 1 BRAF mutant and 1 BRAF wild type. A third patient underwent BRAF mutation testing and was found to have BRAF wild type.
Discussion
This is the first pilot clinical study in metastatic ATC evaluating the combination of antibodies to CTLA-4 and PD-L1 with SBRT. The study did not show activity in a small group of patients with metastatic ATC, including three patients with tumors that were high MSI and had a high TMB. Furthermore, three patients had high CPS. Median OS for this cohort was low (∼3.5 months) that is similar to other reported series (34). Only 1 patient in this cohort lived longer than 1 year.
To date, there have been very little published data evaluating the role of immunotherapy in ATC. In one published study, spartalizumab was reported to yield a 19% response rate in 42 patients, although all responses were seen in tumors that expressed PD-L1 (17). This study did exclude patients at short-term risk for life-threatening complications, so it is very likely that our study cohort did have more advanced disease than was studied in the study of spartalizumab.
All other studies with immunotherapy in the management of ATC have been only presented as abstracts, so there is more limited information available for these studies including the ability to compare with the current study population. The phase II study of ipilimumab (antibody to CTLA-4) and nivolumab (antibody to PD-1) was reported to show a 30% response rate in 10 patients (19). Authors from MD Anderson evaluated atezolizumab with vemurafenib/cobimetinib (BRAF mutant ATC), cobimetinib alone (RAS or NF1 mutant ATC), bevacizumab (other), or paclitaxel (not qualified for the first three) (35).
Only the cobimetinib arm was observed to have a response rate (17%), which was greater than expected from the nonimmunotherapy drugs alone. Furthermore, this study allowed earlier disease and surgery, neither of which was part of our current durvalumab/tremelimumab SBRT study. The ATLEP study is currently investigating a combination of lenvatinib and pembrolizumab for treatment of ATC (36). To date, the authors have reported a 30% response rate in 20 patients, but little is known to date concerning the study population or review of the pathology (36). The study is still ongoing.
Since this study was completed, the landscape for the management of ATC has changed. Significant benefit in treating metastatic ATC has been reported with targeted treatments, such as those targeting BRAFV600E mutations (37), TRK fusion genes (38), and RET fusions genes (39). All of these studies have been small and, in some cases, have led to FDA approval for treatment with dabrafenib/trametinib, entrectinib/larotrectinib, and selpercatinib, respectively. In current practice, ATC testing for BRAFV600E mutation is required and, if positive, immediate treatment with dabrafenib and trametinib may be considered (13,14,37). Other gene alterations may also be targetable and require further study.
The results of this study are very disappointing, especially since three of the cases had high MSI and a high TMB. There are several potential explanations for our results. The first is that durvalumab and tremelimumab, despite being directed at appropriate targets, may not be the best combination of drugs in the treatment of ATC compared with other immunotherapy combinations. The second possibility is that the population evaluated was more advanced than what was evaluated in these other studies. This is highly likely given we only screened for and enrolled on this study the patient with confirmed widely metastatic ATC. A third possibility is that immunotherapy alone does not really work well and both the spartalizumab and ipilimumab data need further validation.
Preclinical data suggest that PD-1/PD-L1 antibodies alone have little effect in ATC models, possibly due to tumor-associated macrophages or Tregs. Either the inhibition of the MAPK pathway (40) or the use of a multitargeted therapy like lenvatinib (41) with a checkpoint inhibitor can overcome this resistance. A fourth possibility, although less likely, is that while SBRT was used to enhance the effects of the checkpoint inhibitor through an abscopal effect, in reality RT acted as an immunosuppressant and decreased the activity of the checkpoint inhibitors.
The JAVELIN study in head and neck squamous cell cancer that randomized patients to concurrent chemotherapy and RT with or without avelumab (42) did not meet its primary endpoint of improving progression-free survival with the addition of immunotherapy to the backbone of chemoradiation. If anything, the addition of the checkpoint may have caused a worse outcome, although preclinical data note otherwise.
Conclusions
The combination of durvalumab and tremelimumab with SBRT should not be studied further for metastatic ATC based on the results of this study. Consideration of checkpoint inhibitors with other agents may still be promising and should continue to be studied in this highly fatal disease with very limited options.
Footnotes
Authors' Contributions
All authors contributed to concept, article writing, editing, and patient contribution.
Author Disclosure Statement
N.Y.L. is on the advisory board—Merck, Merck EMD, Mirati, Elsie. N.R.: Research support: Repare, Repertoire, Invitae, Pfizer; Consulting paige. C.J.T. is on the Varian Advisory Board. All other authors have no conflict of interest.
Funding Information
This study was supported by P30 Grant (P30 CA016042). Additional funding was provided by Astra Zeneca.
Supplementary Material
Supplementary Table S1