
Abstract
Background:
Sorafenib and lenvatinib have been widely adopted to treat radioactive iodine (RAI)-refractory differentiated thyroid carcinoma (DTC). However, limited data exist regarding a direct comparison of these tyrosine kinase inhibitors (TKIs). We aimed to evaluate the clinical efficacy and safety of two TKIs as first-line therapy in patients with distant metastatic or locally advanced, progressive, RAI-refractory DTC in real-world practice.
Methods:
In this multicenter, retrospective cohort study, we evaluated 136 patients with progressive distant metastatic or locally advanced, progressive, RAI-refractory DTC or poorly differentiated thyroid carcinoma (PDTC) who received first-line sorafenib or lenvatinib treatment. The primary outcome was progression-free survival (PFS). We also evaluated the objective response rate, disease-control rate, clinical benefit rate, and safety.
Results:
The median age of the patients was 68 years, and 35% (47/136) were male. Eighty and fifty-six patients were included in the sorafenib and lenvatinib groups, respectively. The median PFS was 13.3 months [95% confidence interval, CI, 9.9–18.1 months] in the sorafenib group and 35.3 months [CI, 18.2 months to upper limit not reported as the median was not reached] in the lenvatinib group (p = 0.001). A significantly prolonged PFS was observed in the lenvatinib group (compared with the sorafenib group) after adjusting for age, sex, pathology, disease-related symptom, lung-only metastasis, cumulative RAI dose, time from diagnosis, treatment duration, and longest diameter of the target lesion (hazard ratio = 0.34, CI, 0.19–0.60, p < 0.001). The partial response rate was 24% and 59% in the sorafenib and lenvatinib groups, respectively (p < 0.001). More common grade 3–4 adverse events were hypertension (16%, 9/56 vs. 1%, 1/80, p = 0.002) and proteinuria (32%, 18/56 vs. 0%, p < 0.001) in the lenvatinib group, and hand-foot skin reaction (24%, 19/80 vs. 4%, 2/56, p = 0.001) in the sorafenib group.
Conclusion:
In our study of Asian patients, first-line lenvatinib treatment of metastatic or locally advanced, progressive, RAI-refractory DTC or PDTC was associated with a longer PFS compared with sorafenib. However, severe hypertension and proteinuria were observed more frequently after lenvatinib treatment than after sorafenib treatment.
Introduction
The overall survival rate of differentiated thyroid carcinoma (DTC) is reported to be 98% at 5 years, however, in patients with radioactive iodine (RAI)-refractory metastatic DTC, the survival rate is <10% from the time of detection of the metastasis (1 –5). Efforts to improve the survival of these patients have been made during the last decades, with options such as local therapies or systemic therapies (e.g., conventional chemotherapeutic agents, tyrosine kinase inhibitors [TKIs], immune checkpoint inhibitors, and specific inhibitors of signaling pathways) (6). According to the National Comprehensive Cancer Network (NCCN) guideline, genomic testing should be done to identify potential actionable mutations for RAI-refractory DTC, such as ALK, NTRK, and RET gene fusions and selectively inhibit cancer cell growth with minimal adverse events (AEs) (7). However, due to the rarity of these mutations, multitargeted TKIs remain the mainstay of systemic treatment.
Oral multitargeted TKIs, including sorafenib and lenvatinib, have shown efficacy in RAI-refractory DTC patients. In the DECISION trial, the median progression-free survival (PFS) of the patients who were treated with sorafenib was 10.8 months, which was significantly improved compared with that of patients receiving placebo (5.8 months) (8). In the SELECT trial, lenvatinib showed a longer PFS, which reached a median of 18.3 months (9). Both TKIs are currently approved by the US Food and Drug Administration (FDA); nevertheless, a prospective study regarding a direct comparison between the two TKIs has not been reported yet. To our knowledge, only a few studies—including a systemic review—have been conducted to compare these two TKIs (6,10).
In Korea, the pricing and reimbursement of drugs are managed by the National Health Insurance scheme, which is a single-payer system operated by the National Health Insurance Service. When patients with DTC are given a TKI covered by health insurance in Korea, the out-of-pocket money for medical services is reduced to 5%. First-line sorafenib was approved for patients with distant metastatic or locally advanced, progressive, RAI-refractory DTC in January 2014, and in November 2014, it was accepted as a reimbursable drug in Korea. Subsequently, lenvatinib was approved as first- and second-line therapy for patients with distant metastatic or locally advanced, progressive, RAI-refractory DTC in October 2015; however, reimbursement was possible only for first-line therapy starting from August 2017. Second-line sorafenib was approved in October 2020.
Therefore, previous data on these two TKIs in Korea were focused on either sorafenib as first-line treatment or lenvatinib as a salvage therapy (11 –13). The efficacy of sorafenib in real-world practice was comparable with that in the DECISION trial, and lenvatinib salvage therapy significantly improved the overall survival in patients who had progressive disease after treatment with sorafenib (11,12). Owing to the increase in the use of lenvatinib as the first-line therapy in clinical practice, sufficient real-world data were accumulated for both TKIs as first-line therapy. Therefore, we aimed to evaluate the clinical efficacy and safety of lenvatinib or sorafenib as first-line therapy in patients with metastatic or locally advanced, progressive, RAI-refractory DTC.
Materials and Methods
Study patients
In this multicenter retrospective cohort study, we included patients with distant metastatic or locally advanced, progressive, RAI-refractory DTC or poorly differentiated thyroid carcinoma (PDTC) who were treated with sorafenib or lenvatinib between April 1, 2011, and September 30, 2021, at six tertiary hospitals in Korea (Asan Medical Center, Pusan National University Hospital, Dongnam Institute of Radiological and Medical Sciences Cancer Center, Severance Hospital, Seoul St. Mary's Hospital, and Chonnam National University Hospital). Eligible patients were aged >18 years, had measurable disease according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 (14), had an Eastern Cooperative Oncology Group (ECOG) performance status of 0‒2, and had adequate bone marrow, liver, and renal function.
RAI-refractory DTC was defined by the presence of any of the following: (i) absent RAI uptake in all lesions on scintigraphy; (ii) absent RAI uptake in some lesions (not all); (iii) DTC progression despite RAI uptake; and (iv) reaching the maximum recommended cumulative RAI activity (600 mCi) (11,15). The study protocol was reviewed and approved by the Institutional Review Board of each participating institution. Informed consent was waived because of the retrospective nature of the study and the analysis used anonymous clinical data.
Treatment and follow-up protocols
The treating physicians decided on treatment and follow-up procedures, in considering the prescribing information for each drug and established local practice (16). Sorafenib or lenvatinib was self-administered, and the median initial dose of sorafenib was 800 mg per day (interquartile ranges [IQRs], 600–800) and that of lenvatinib was 20 mg per day (IQR, 20–24). All patients were treated with L-thyroxine to suppress serum thyrotropin levels (<0.1 mIU/L) and received the best supportive care. Tumor response and disease progression were assessed by computed tomography or magnetic resonance imaging at baseline and every 8–12 weeks thereafter. Physical examination, laboratory test, and safety assessments were performed at baseline, every 2–4 weeks until week 12, and then at every visit during the follow-up. Dose modification was allowed at any time as per the investigator's judgment.
Outcomes
Imaging data were retrospectively analyzed based on RECIST version 1.1. The primary outcome was the duration of PFS as determined by investigator assessments, according to RECIST. We also assessed the objective response rate (ORR), the disease-control rate, clinical benefit rate, change of target lesions, and safety. ORR was defined as the percentage of patients who achieved complete response (CR) or partial response (PR). The disease control rate and clinical benefit rate were calculated as CR plus PR plus stable disease (SD) and CR plus PR plus durable SD (duration
Safety
Safety parameters, including the presence of AEs, vital signs, hematology and clinical chemistry, urinalysis, and electrocardiograms, were evaluated at baseline and at every follow-up visit. We assessed AEs graded on a five-point scale according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0 (18). We assumed AEs to be treatment-related if a causal relationship with sorafenib or lenvatinib could not be ruled out.
Statistics
Continuous variables are presented as medians with IQRs, and categorical variables are presented as numbers with percentages. PFS curves were plotted using the Kaplan‒Meier method, and the log-rank test was used to determine their significance. A Cox proportional hazards model, with calculated hazard ratios (HRs) and at 95% confidence intervals (CIs), was used to compare the sorafenib and the lenvatinib groups for PFS analysis. In multivariate analysis, age, sex, pathology (PDTC), disease-related symptom, lung-only metastasis, cumulative RAI dose, time from diagnosis, treatment duration, and longest diameter of the target lesion were adjusted. Statistical analyses were performed using the R program (version 3.6.2, R Foundation for Statistical Computing, Vienna, Austria;
Results
Patients
We included 136 patients with distant metastatic or locally advanced, progressive, RAI-refractory DTC or PDTC. We excluded 39 patients due to no measurable lesion (n = 6); ECOG performance status score 3–4 (n = 8); abnormal bone marrow, liver, and renal function (n = 1); history of targeted therapy (n = 4); prior enrollment in trials (n = 9); and incomplete tumor response data (n = 11) (Supplementary Fig. S1). The baseline characteristics of patients in the study groups were well balanced between the sorafenib group (n = 80) and the lenvatinib group (n = 56, Table 1).
Baseline Characteristics of Patients with Radioactive Iodine-Refractory Progressive Differentiated Thyroid Carcinoma Who Underwent Sorafenib or Lenvatinib Treatment
Continuous variables are presented as median (interquartile range) and categorical variables as numbers (percentages).
Head and neck and cervical lymph nodes.
Head and neck, cervical lymph nodes, chest wall and pelvic bone mass, and metastatic skin lesion.
Adrenal, pancreas, and kidney.
Skin, subcutaneous, muscle, spleen, brain, and hypopharynx.
FTC, follicular thyroid carcinoma; PDTC, poorly differentiated thyroid carcinoma; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; RFA, radiofrequency ablation; T4, thyroxine; Tg, thyroglobulin.
There was no significant difference between the groups in terms of age, sex, pathological subtype, previous therapy, and target lesions. The median age at the initiation of TKI therapy was 68 years (IQR, 60–73 years), and 47 (35%, 47/136) patients were male. The most common pathology type was papillary (72%, 98/136), followed by follicular (13%, 17/136) and poorly differentiated carcinoma (14%, 19/136). Two patients had both papillary and follicular carcinoma. With respect to previous therapy, all patients had received prior RAI treatment, 51 (38%, 51/136) patients had received radiotherapy (head and neck, cervical and metastatic lymph nodes, metastatic lung, brain, and bone lesion), and 15 (11%, 15/136) patients had received radiofrequency ablation (head and neck, cervical lymph node, chest wall and pelvic bone mass, and metastatic skin lesion).
Majority of the patients (99%, 134/136) had distant metastasis, and the lung (66%, 90/136) was the most common target lesion, followed by lymph nodes (13%, 18/136) and head and neck (11%, 15/136). The median cumulative RAI dose was lower in the lenvatinib group (240 mCi, IQR 150–400 mCi) than in the sorafenib group (400 mCi, IQR 200–600 mCi, p = 0.014). The median time from the diagnosis of thyroid cancer to the initiation of TKIs was significantly longer in the sorafenib group (9 years, IQR 4–15 years) than in the lenvatinib group (6 years, IQR, 2–12 years, p = 0.025).
There was no significant difference in the longest diameter of the target lesion between the two groups (24 mm in the sorafenib group and 23 mm in the lenvatinib group; p = 0.539). The median maintained dose of sorafenib was 600 mg per day (IQR, 600–800 mg), and that of lenvatinib was 10 mg per day (IQR, 10–14 mg). The median treatment duration was 14 months (IQR, 5–28 months) in the sorafenib group and 12 months (IQR, 7–26 months) in the lenvatinib group. There was no significant difference in the treatment duration between groups (p = 0.909). Twenty-one patients (26%, 21/80) in the sorafenib group and two patients (4%, 2/56) in the lenvatinib group initiated TKIs after they were approved as usable drugs and before being approved as reimbursable drugs in Korea.
Efficacy
At data cutoff (September 30, 2021), RECIST-defined progression had occurred in 81 (60%) patients. The median PFS was 13.3 months [CI, 9.9–18.1 months] in the sorafenib group and 35.3 months [CI, 18.2 months to upper limit was not reported as the median was not reached] in the lenvatinib group, and it was significantly different between the two groups (p < 0.001, Fig. 1). Investigator-assessed PFS was significantly longer in the lenvatinib group than in the sorafenib group (HR = 0.41; CI, 0.24–0.70; p = 0.001, Table 2; Supplementary Table S1).
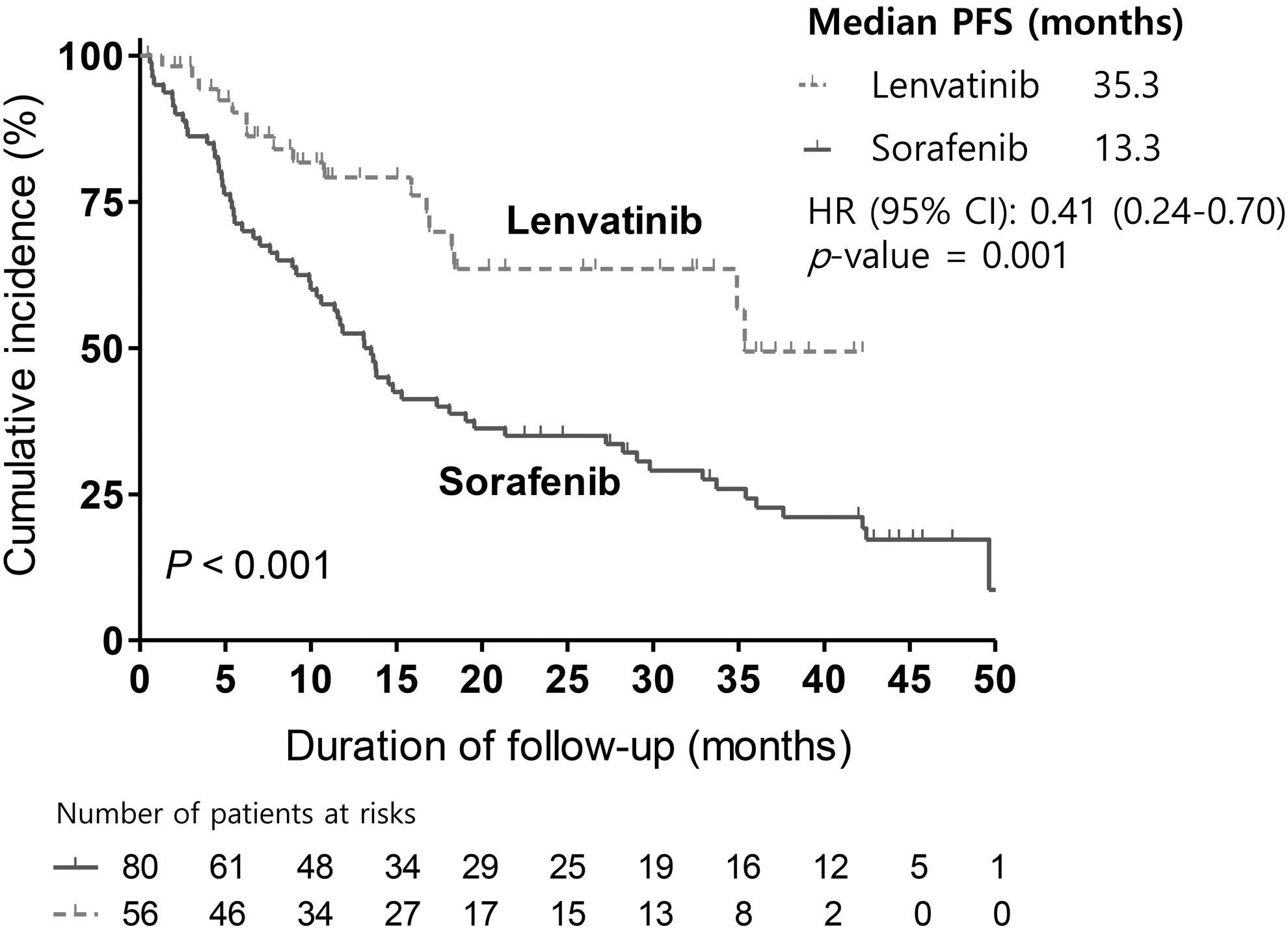
Kaplan‒Meier plot of the progression-free survival of patients with progressive refractory DTC after treatment with first-line sorafenib or lenvatinib. DTC, differentiated thyroid carcinoma.
The Hazard Ratio for Progression-Free Survival in the Lenvatinib Group Compared with the Sorafenib Group Using Multivariate Analysis
Model 1 is adjusted for age and sex. Model 2 is adjusted for age, sex, pathology (PDTC), disease-related symptom, and lung-only metastasis. Model 3 is adjusted for age, sex, pathology (PDTC), disease-related symptom, lung-only metastasis, cumulative RAI dose, time from diagnosis, treatment duration, and longest diameter of target lesion. Variables are presented as median (interquartile range). p-Values were calculated using a Cox proportional hazard model.
CI, confidence interval; HR, hazard ratio.
After adjusting for age, sex, pathology, disease-related symptom, lung-only metastasis, cumulative RAI dose, time from diagnosis, treatment duration, and longest diameter of the target lesion, the lenvatinib group was still associated with a significantly better PFS compared with the sorafenib group (adjusted HR = 0.34; CI, 0.19–0.60; p < 0.001, Model 3 in Table 2; Supplementary Table S2). The cumulative RAI dose or time from thyroid cancer diagnosis to TKI initiation was not associated with PFS (p = 0.2 and p = 0.39, respectively, Supplementary Figs. S2 and S3).
PR and SD were achieved in 19/80 (24%) and 55/80 (69%) patients in the sorafenib group, respectively, and in 33/56 (59%) and 22/56 (39%) patients in the lenvatinib group, respectively (Fig. 2 and Table 3). Eighty-three (66/80) and eighty-nine (50/56) percent of the patients exhibited reduced target lesions—from baseline—in the sorafenib and lenvatinib groups, respectively. The proportion of patients with PR and ORR was significantly higher in the lenvatinib group (59%, 33/56) than in the sorafenib (24%, 19/80) group (p < 0.001). There was no significant difference in the disease control rate (93%, 74/80 in the sorafenib group and 98%, 55/56 in the lenvatinib group; p = 0.276) and clinical benefit rate (65%, 52/80 in sorafenib group and 77%, 43/56 in the lenvatinib group; p = 0.199) between the two groups.
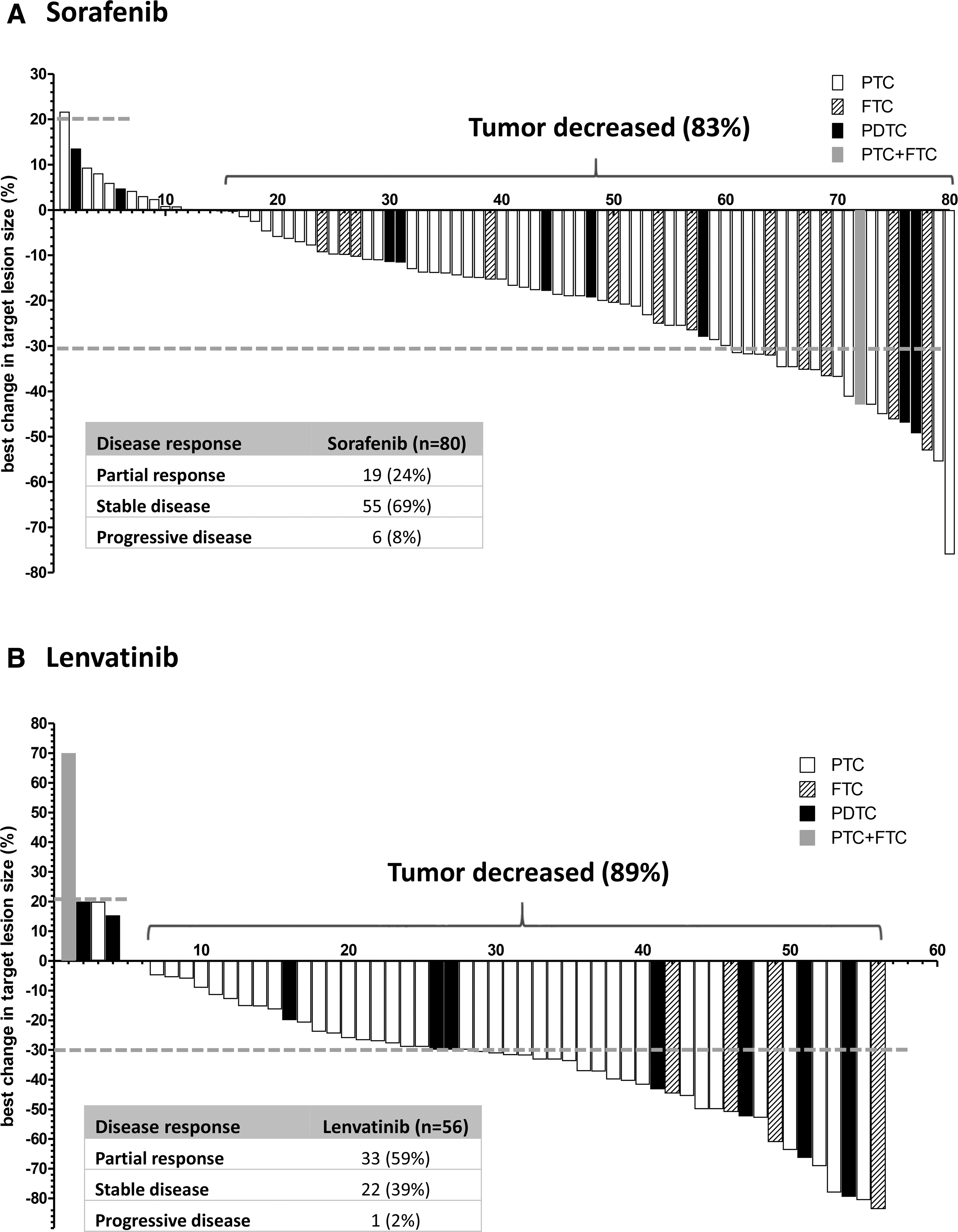
Best change of target lesions after (
Summary of Objective Responses in Patients with Refractory Differentiated Thyroid Carcinoma Who Underwent Sorafenib or Lenvatinib Treatment
Variables are presented as numbers (percentages).
Durable SD = duration of SD
Objective response rate was calculated as CR plus PR.
Disease control rate was calculated as CR plus PR plus SD.
Clinical benefit rate was calculated as CR plus PR plus durable SD.
CR, complete response; PD, progressive disease; PR, partial response; SD, stable disease.
Safety and AEs
AEs of any cause and grade occurred in 77/80 (96%) patients in the sorafenib group and in 56/56 (100%) patients in the lenvatinib group (p = 0.27). Moreover, grade 3 or 4 AEs occurred in 38/80 (48%) patients in the sorafenib group and in 26/56 patients (46%) in the lenvatinib group (p = 0.99, Table 4). The most common grade 3 or 4 AEs included hand-foot skin reaction (24%, 19/80 with sorafenib vs. 4%, 2/56 with lenvatinib), hypertension (1%, 1/80 vs. 16%, 9/56), and proteinuria (0% vs. 32%, 18/56).
Adverse Events (≥5%) Occurring in Patients with Refractory Differentiated Thyroid Carcinoma Who Underwent Sorafenib or Lenvatinib Treatment
Variables are presented as numbers (percentages). Adverse events were classified with the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0.
There were two life-threatening AEs, including pneumothorax and tracheal fistula, in patients treated with lenvatinib. One patient underwent surgery owing to pneumothorax 4 months after the initiation of lenvatinib, and restarted lenvatinib at a reduced dose. One patient developed fistula between the trachea, skin, and neck mass after 8 months following lenvatinib initiation, and died 2 weeks after lenvatinib discontinuation. Drug interruptions, reductions, and withdrawals due to AEs occurred in 14/80 (18%), 35/80 (44%), and 10/80 (13%) patients in the sorafenib group, respectively; in contrast, these occurred in 25/56 (45%), 46/56 (82%), and 6/56 (11%) patients in the lenvatinib group, respectively. The proportion of patients with dose interruptions (18%, 14/80 vs. 45%, 25/56) or reductions (44%, 35/80 vs. 82%, 46/56) was higher in the lenvatinib group than in the sorafenib group (p < 0.001, and p < 0.001, respectively).
Discussion
In this multicenter, retrospective cohort study, lenvatinib showed a potential for better efficacy than sorafenib as first-line therapy for distant metastatic or locally advanced, progressive, RAI-refractory DTC and PDTC, as reflected by a significantly longer PFS. This finding was robust after the adjustment of multiple confounding factors. We also observed that the ORR was significantly higher in the lenvatinib group compared with that in the sorafenib group. Severe hypertension and proteinuria were more commonly seen after lenvatinib treatment; however, there was no significant difference in any treatment-related AEs and grade 3 or 4 AEs between the patients treated with the two TKIs. This comparative study suggested that lenvatinib may be more effective as first-line therapy for progressive refractory DTC in clinical practice.
Overall, the efficacy of sorafenib or lenvatinib in this study was similar to that observed in phase III clinical trials and previous studies (6,8,9,11 –13,17,19 –23). The median PFS after sorafenib treatment was 10.8 months in the DECISION trial (8) and 7.2–14.4 months in previous real-world studies (12,17,19,20). In our study, the median PFS was 13.3 months in patients treated with sorafenib. So far, there have been two randomized phase III clinical trials of lenvatinib. The median PFS was 18.3 and 23.9 months in SELECT trial and study 308, respectively (9,17).
Furthermore, the updated SELECT trial analysis showed prolonged PFS (33.1 months) in lenvatinib responders (24). The proportion of Asian patients was <20% in the SELECT trial, and study 308 was done in Chinese patients with RAI-refractory DTC (17). Twenty-five percent of the patients in the two studies included patients who were previously treated with other TKIs or vascular endothelial growth factor and receptors (VEGF/VEGFRs) (8,15). In a recently published phase II study on lenvatinib, the median PFS was not reached in the 24 mg arm and was 24.4 months in the 18 mg arm (25). Previous phase II and real-world studies of lenvatinib demonstrated that PFS ranged from 9.7 to 25.8 months in RAI-refractory DTC patients (13,20 –23,26,27). The seemingly wide range of PFS may be explained by the region of patients and proportion of patients who were subjected to first-line lenvatinib therapy. In a previous multicenter cohort study, we reported that the median PFS of the patients was 21.8 months after lenvatinib treatment (13). Given that two-thirds of patients in that study were treated with lenvatinib as salvage therapy, the observed PFS of 35.3 months in this study is not unexpected. These data show promise and highlight the benefit of lenvatinib in treating patients with distant metastatic or locally advanced, progressive, RAI-refractory DTC.
The safety profile of the two TKIs was generally consistent with that in previous studies (8,9,17,28). Patients in the lenvatinib group experienced more AEs, such as hypertension (95% vs. 31%) and proteinuria (80% vs. 13%), but less hand-foot skin reaction (36% vs. 79%) compared with those in the sorafenib group. Among patients who received lenvatinib, 95% of the patients experienced hypertension, which is similar to the result obtained in study 308 (82%) and in a study from Japan (94%) (6,17). Otherwise, only 68% of the patients in the SELECT trial—with <20% of Asian individuals—experienced hypertension (9). Proteinuria was also found to have a regional difference. We saw that 80% and 32% of the lenvatinib-treated patients experienced grade or grade
Study 308 also reported a relatively high incidence of proteinuria (80% for any grade and 23% for grade
As both sorafenib and lenvatinib can be used as the first-line and salvage therapy, the selection of the first agent and the subsequent salvage therapy is crucial in clinical practice. In a few retrospective studies, salvage TKI therapy has been shown to prolong overall survival after initial TKI failure (12,30). For treatment failure with first-line sorafenib, Oh et al. demonstrated that overall survival was significantly improved in the lenvatinib salvage group compared with that in the sorafenib-only group (12). Koehler et al. also reported that lenvatinib resulted in PR in 30% of the patients in second-line treatment (20).
On the contrary, for treatment failure with first-line lenvatinib, sorafenib also showed an 11.1% ORR in a US study (21). So far, there have been no randomized controlled trials that compare directly between two kinds of sequential therapies. As a result, we had to choose the treatment sequence based on the previous studies and experience. A follow-up data from this study for patients who switched to alternative TKI after first-line treatment failure are awaited. These findings may aid clinicians in determining the best sequence of TKIs to use the best optimal time to switch to salvage therapy. Furthermore, because cabozantinib has shown efficacy in patients who have progressed after up to two prior VEGFR-targeted therapies (31), the results of different kinds of sequential therapies are expected in practice.
This study had several limitations. First, this is a retrospective cohort study, and there is a possibility of selection bias. Differences in baseline characteristics between the treatment groups suggest that the groups may not be directly comparable. However, we adjusted for age, sex, histopathology, disease-related symptoms, lung-only metastases, cumulative RAI dose, time from diagnosis, treatment duration, and longest diameter of the target lesion to minimize selection bias.
Another limitation is that the median starting dose of lenvatinib (20 mg) was lower than a recommended dose (24 mg) for RAI-refractory DTC (9). As the standard dose of 24 mg is based on data obtained from the Western population, in a post hoc analysis of the SELECT trial, a dose interruption was required in 70% of the Asian population for more than 10% of the total treatment period (32). It has been proposed that a lower starting dose of lenvatinib would provide comparable efficacy and reduced toxicity in patients with RAI-refractory DTC (32,33). Both 24 and 20 mg of lenvatinib starting doses may be reimbursed by the National Health Institute of Korea.
Since this study analyzed real-world data, all these factors were considered before administration of lenvatinib. Another limitation is that the median overall survival was not assessed due to the follow-up period for lenvatinib being relatively short. Because lenvatinib was approved as a reimbursable drug in patients with progressive RAI-refractory DTC after August 2017 in Korea, most patients in this study started lenvatinib recently. Therefore, 32 of 39 patients whose tumor did not progress in the lenvatinib group were on lenvatinib at the time of data cutoff. For this reason, the lenvatinib group had significantly better PFS than the sorafenib group, but the median treatment durations for both drugs were similar. The frequency of AEs may also be underestimated relative to prospective studies.
Despite these limitations, this relatively large multicenter cohort study was useful to compare the efficacy and AEs of sorafenib and lenvatinib in a real-world setting in patients with distant metastatic or locally advanced, progressive, RAI-refractory DTC.
In summary, in this multicenter retrospective cohort study, lenvatinib appeared to be a more effective first-line TKI in patients with progressive refractory DTC and PDTC, as reflected by a longer PFS. However, hypertension and proteinuria may be observed more commonly after lenvatinib treatment, especially in the Asian population. The selection of first-line TKI would be based on efficacy, risk of potential AEs, and strategies including rescue therapy in case of treatment failure in patients with metastatic or locally advanced, progressive, RAI-refractory DTC or PDTC.
Footnotes
Authors' Contributions
M.K. and M.J. contributed to data collection, data analysis, visualization, interpretation of the results, and wrote the article. M.J.J., E.Y.K., D.Y.S., and D.J.L. contributed to data collection, data curation, and reviewed the article. B.H.K., H.-C.K., W.B.K., and Y.K.S. provided critical input on the data analysis, reviewed the article, and contributed to the discussion. H.K.K. contributed to the design of the study, data collection, interpretation of the results, and editing of the article. W.G.K. contributed to the conception and design of the study, data curation, interpretation of the data, and editing of the article. All the authors had full access to the data, take responsibility for the accuracy of the data analysis, and approved the final version of the article.
Author Disclosure Statement
W.B.K., Y.K.S., and W.G.K. were advisory board members of Bayer, Eisai, Lilly, and Hanmi Pharmaceuticals. Otherwise, there are no competing financial interests that exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2