
Abstract
Background:
Anaplastic thyroid carcinoma (ATC) is an aggressive thyroid malignancy that is associated with poor prognosis. Current treatment options include surgery, radiation, cytotoxic chemotherapy, and multikinase inhibitor therapy. The role of immunotherapy in ATC is an area of active interest and recent evidence suggests that it may be a potentially effective treatment option.
Methods:
We report a case series of 13 patients with locally advanced or metastatic unresectable ATC who received immune checkpoint inhibitor therapy (pembrolizumab or nivolumab) at a single institution.
Results:
The patients' median age was 70 years, 54% (7/13) were male, and 85% (11/13) had stage IVC disease with lungs and lymph nodes being the most common sites of metastases. Ten patients had tumor tissue available for programmed death-ligand 1 (PD-L1) expression testing, all of which were positive for PD-L1, and seven of these patients also had a BRAFV600E mutation. The median progression-free survival was 1.9 months and median overall survival (OS) was 4.4 months. The objective response rate was 16% (2/13). Two patients had partial response (PR), and three patients had durable stable disease. Among patients with a clinical benefit, after a median follow-up of 13.5 months, median OS had not been reached (range 4+ to 29+ months). Responses were ongoing in four subjects. The one-year survival rate was 38% (5/13). Six patients (46%) experienced an immune-related adverse event, and 15% (2/13) experienced a grade 3 or higher adverse event, including one patient with grade 5 immune checkpoint-related thyroiditis.
Conclusions:
Immune checkpoint blockade was well tolerated with a toxicity profile consistent with published literature on PD-1/PD-L1-targeting therapies. For ATC patients, immune checkpoint inhibition may represent an effective treatment option with robust sustained responses seen in a subset of patients.
Introduction
Anaplastic thyroid carcinoma (ATC) is a rare and aggressive subtype of thyroid cancer representing ∼1% of all thyroid cancer cases (1). Despite its rarity, ATC disproportionately accounts for 20% to 50% of thyroid cancer deaths (2). The median overall survival (OS) ranges from three to eight months with a one-year survival rate of 20%. Response rates to conventional chemotherapy and radiotherapy are low (3). Due to the rapid development of resistance to existing therapies, there is an urgent unmet need for new treatments especially in the metastatic setting.
For patients with unresectable or metastatic ATC, recent advances in targeted therapies have expanded the arsenal of systemic treatment options beyond cytotoxic chemotherapy in patients with constitutively activated mitogen-activated protein kinase (MAPK) signaling. Approximately 40% of ATC patients express a BRAFV600E mutation that is susceptible to combination BRAF/MEK inhibition with dabrafenib and trametinib (2). Treatment with this regimen is based on a phase II open-label trial that reported a 69% overall response rate (ORR) and 80% one-year survival rate (4).
Another targeted therapy option is NTRK inhibition with larotrectinib and entrectinib in patients with NTRK gene fusion-positive tumors. The data supporting these agents are based on studies of patients with NTRK gene fusion-positive tumors, of which a small subset of patients had thyroid cancer (5,6). Pooled data from three phase I/II trials of larotrectinib reported an objective response rate of 29% (2/7) among patients with ATC (7).
In an analysis of patients who received entrectinib, one of the five patients with thyroid cancer achieved a partial response (PR) (6). Multiple receptor tyrosine kinase inhibitors (TKIs) such as sorafenib, pazopanib, and lenvatinib have been studied in trials with generally limited efficacy. In an open-label, multicenter phase II trial of lenvatinib in ATC patients, the confirmed ORR was 0% (0/20). However, more than half of the patients experienced a brief period of tumor shrinkage, indicating some short-lived activity.
The median progression-free survival (PFS) was 2.6 months and median OS was 3.2 months (8). Pembrolizumab is a guideline-recommended option for patients with high tissue tumor mutational burden (TMB-H), defined as at least 10 somatic mutations per megabase based on the results of the Keynote-158 trial (9).
The role of checkpoint blockade in treating ATC patients without TMB-H is presently unclear. Eleven to 29% of ATC tumor samples express programmed death-ligand 1 (PD-L1), which suggests a role for anti-PD-L1/PD-1 therapy (10,11). Multiple case reports of robust responses to single-agent checkpoint blockade exist in the literature (12,13).
A multicenter, international phase II trial of the PD-1 inhibitor, spartalizumab, enrolled 42 patients with ATC regardless of PD-L1 or TMB status. The ORR was 19%, with three patients achieving a complete response and five patients demonstrating a PR. The duration of response ranged from 16.7 weeks to 1.6 years. The median OS was 5.9 months with a 1-year survival rate of 40%.
Additionally, in a subgroup analysis of 28 patients with positive PD-L1 expression (≥1% positive in tumor cells), the median OS was not reached. The median PFS was 1.7 months with no significant difference in patients with positive PD-L1 expression (14).
As evidence supporting the use of immune checkpoint blockade in ATC patients continues to grow, we sought to evaluate the real-world benefit of utilizing available immune checkpoint inhibitors at a major academic medical center.
Methods
Patients
This was a single-center, retrospective case series of patients with histologically confirmed ATC at The Ohio State University Comprehensive Cancer Center (OSUCCC). This study was approved by The Ohio State University Institutional Review Board with waiver of consent documentation (IRB Approval No. 2021C0074).
Patients were required to be 18 years of age or older and have received at least one infusion of pembrolizumab or nivolumab. Patients who received concomitant BRAF and/or MEK inhibitors were included. However, patients who received any other targeted therapeutic agents or concomitant chemotherapy while on immunotherapy as well as protected populations such as prisoners and pregnant women were excluded. In addition, patients treated with pembrolizumab or nivolumab as a component of a clinical trial were not included in the analysis.
All patients received their first dose of immune checkpoint inhibitor between June 2016 and June 2021. Patients who were alive without disease progression were censored at last follow-up through August 25, 2021.
Retrospective data were reviewed using the electronic medical record system. Baseline demographics and characteristics were obtained and included age, sex, ethnicity, stage of disease, presence of metastases, and treatment with prior surgery, radiation, chemoradiation, and/or systemic chemotherapy. Tumor biomarker analyses were performed on the majority of biopsies. Tumor biomarker (such as PD-L1, TMB, BRAF, KRAS, and NRAS mutation status) and immunotherapy-related adverse events were collected.
PD-L1 immunohisto/cytochemistry was done with the 22C3 pharmDx (Dako Autostainer Link 48 platform) and the combined positive score (CPS) was reported. The morphological characteristics, immunohistochemical staining, and immune infiltrate were reviewed by an experienced head and neck pathologist (A.L.L.). Genomic DNA was extracted and polymerase chain reaction was performed. Products were analyzed by pyrosequencing for mutations in codons 600 and 601 of BRAF and codons 12, 13, and 61 of NRAS and KRAS, as well as codons 117 and 146 of KRAS, with a lower threshold of detection of the variant mutant allele of ∼5%.
In select cases with adequate tissue sample, DNA was extracted from 40-μM formalin-fixed paraffin-embedded sections, and comprehensive genomic profiling was performed on hybridization-captured, adaptor ligation-based libraries to a mean coverage depth of × 650 for 315 cancer-related genes plus select introns from 28 genes frequently rearranged in cancer (Foundation One). All classes of genomic alterations were identified, including base substitutions, insertions/deletions, copy number alterations, and rearrangements.
In addition, time points of date of diagnosis, immunotherapy initiation and discontinuation, disease progression, and death were collected. Patients received either a fixed dose of nivolumab (240 or 480 mg given intravenously (IV) every two or four weeks, respectively) or pembrolizumab (200 or 400 mg administered IV every three or six weeks, respectively). All infusions were administered over 30 minutes in an outpatient infusion center.
Patients had follow-up imaging assessments performed at intervals as per the discretion of the treating clinician. The endpoints collected were OS, PFS, response rate, and frequency of adverse events. Response was determined according to the response evaluation criteria in solid tumors (RECIST), version 1.1. All adverse effects were assessed using the National Cancer Institute's Common Terminology Criteria for Adverse Events (CTCAE), version 5.0.
OS was defined as the time from the first infusion of pembrolizumab or nivolumab to death from any cause or censoring, and OS from diagnosis was defined as the time from collection of the first sample that reported pathology/cytology consistent with ATC to death from any cause or censoring. PFS was the time from first infusion to disease progression, death from any cause, or censoring.
The clinical benefit rate (CBR) for the purpose of this study included patients who achieved a complete response, PR, or durable stable disease based on RECIST, v1.1. Durable stable disease was defined as no progressive disease or response for ≥4 months.
Statistical analyses
Baseline demographics and characteristics were summarized using descriptive statistics. Survival outcomes were determined based on the Kaplan–Meier method. Kaplan–Meier survival analyses were performed using GraphPad Prism, version 8.0.0 for Windows, GraphPad Software (San Diego, CA). For the key descriptive analyses, response rates, overall benefit rates, and OS rates were summarized by frequencies, percentages, and confidence intervals [CIs]; OS and PFS were summarized by median and interquartile range.
CIs were calculated based on the exact binomial test using R 4.10 (R Core Team, 2021) (15).
Results
Patients
A total of 22 patients were eligible for inclusion based on treatment orders entered in the electronic medical record to initiate immune checkpoint blockade (Fig. 1). Three patients were excluded because they did not have ATC and another four patients were not included since they did not receive the planned dose of immune checkpoint inhibitor.

Patient flow chart. ATC, anaplastic thyroid carcinoma; ICI, immune checkpoint inhibitor.
Additionally, two patients were excluded because they were enrolled in clinical trials containing an immune checkpoint inhibitor. Among the remaining 13 evaluable patients, 12 received pembrolizumab and 1 patient received nivolumab. The median age was 70 years. Thirty percent, 15%, and 54% of patients had stage IVA–IVC disease, respectively (Tables 1 and 2).
Patient Characteristics
ATC, anaplastic thyroid carcinoma; PD-L1, programmed death-ligand 1.
Pertinent Clinical Data of Individual Patients
CCRT, concurrent chemoradiation; CPS, combined positive score; D+T, dabrafenib+trametinib; IHC, immunohistochemistry; N, no; N/A, not available; PCR, polymerase chain reaction; RT, radiation; SBRT, stereotactic body radiation therapy; TPS, tumor proportion score; Y, yes.
Tumor genetics and immune marker characterization
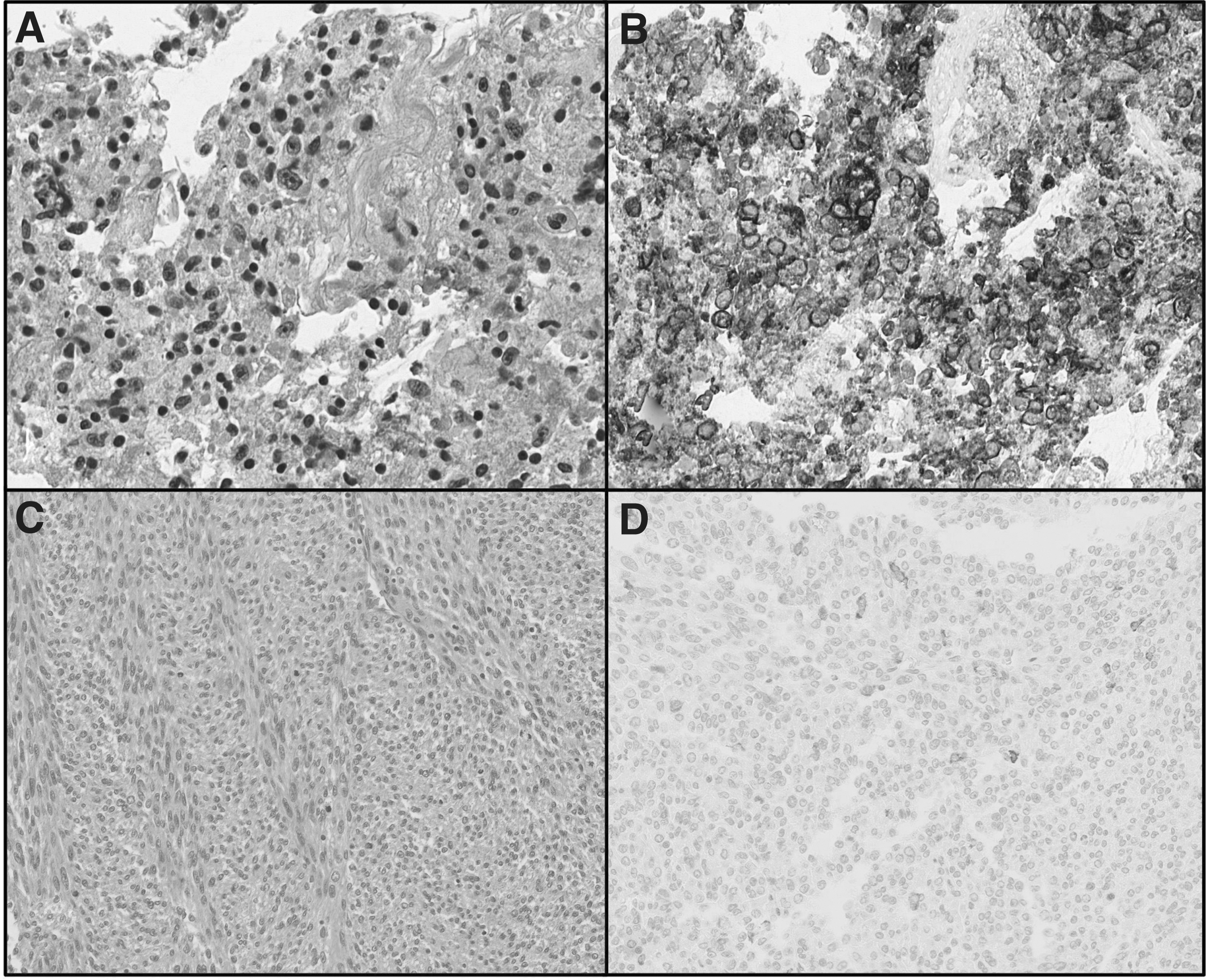
Ten patients (77%) had tumor tissue available for PD-L1 testing (Fig. 2) and all had PD-L1 CPS ≥1. Six of these 10 patients had a PD-L1 CPS of 90% or more. All patients had tumor tissue hotspot mutation testing done and seven (54%) had a BRAF V600E mutation. Five patients underwent tumor mutation burden testing, but none were with TMB-H.
(
Prior treatments
Ten patients (77%) had at least one prior therapy before receiving an immune checkpoint inhibitor and many received a combination of different treatment modalities (Table 2). The median number of prior lines of treatment was 2 (range 0–5). Five patients had up-front resection of their primary tumors as first-line therapy. This was followed by chemotherapy alone (#6 and 8), dabrafenib and trametinib (#2), concurrent chemoradiation (#13), or concurrent dabrafenib and trametinib plus radiation (#10).
Two patients had up-front dabrafenib and trametinib followed by pembrolizumab either in the second-line (#5) or in the third-line setting after progression on concurrent chemoradiation (#12). Two patients had up-front chemotherapy alone followed by pembrolizumab in the second-line (#3) or third-line setting following progression on dabrafenib and trametinib (#4).
One patient had up-front concurrent chemoradiation, followed by chemotherapy alone, and received pembrolizumab monotherapy at progression (#11). Three patients were systemic therapy-naïve (#1, 7, and 9). Of the seven patients with BRAFV600E -positive disease, six had prior progression with dabrafenib and trametinib (#2, 4, 5, 8, 10, and 12). The seventh patient is on concurrent dabrafenib plus trametinib and pembrolizumab as first-line systemic therapy (#7).
Response
There were two patients with PR (#1 and 3) based on RECIST, v1.1 (Table 3 and Fig. 3). A third patient (#9), with stage IVB ATC, no longer had a palpable neck mass following two cycles of pembrolizumab therapy. This patient experienced severe immune checkpoint-mediated thyroiditis and expired before the first radiographic assessment on pembrolizumab could be performed. The ORR was 15% (2/13 [CI 0.0–0.4]) in addition to this unconfirmed clinical response.
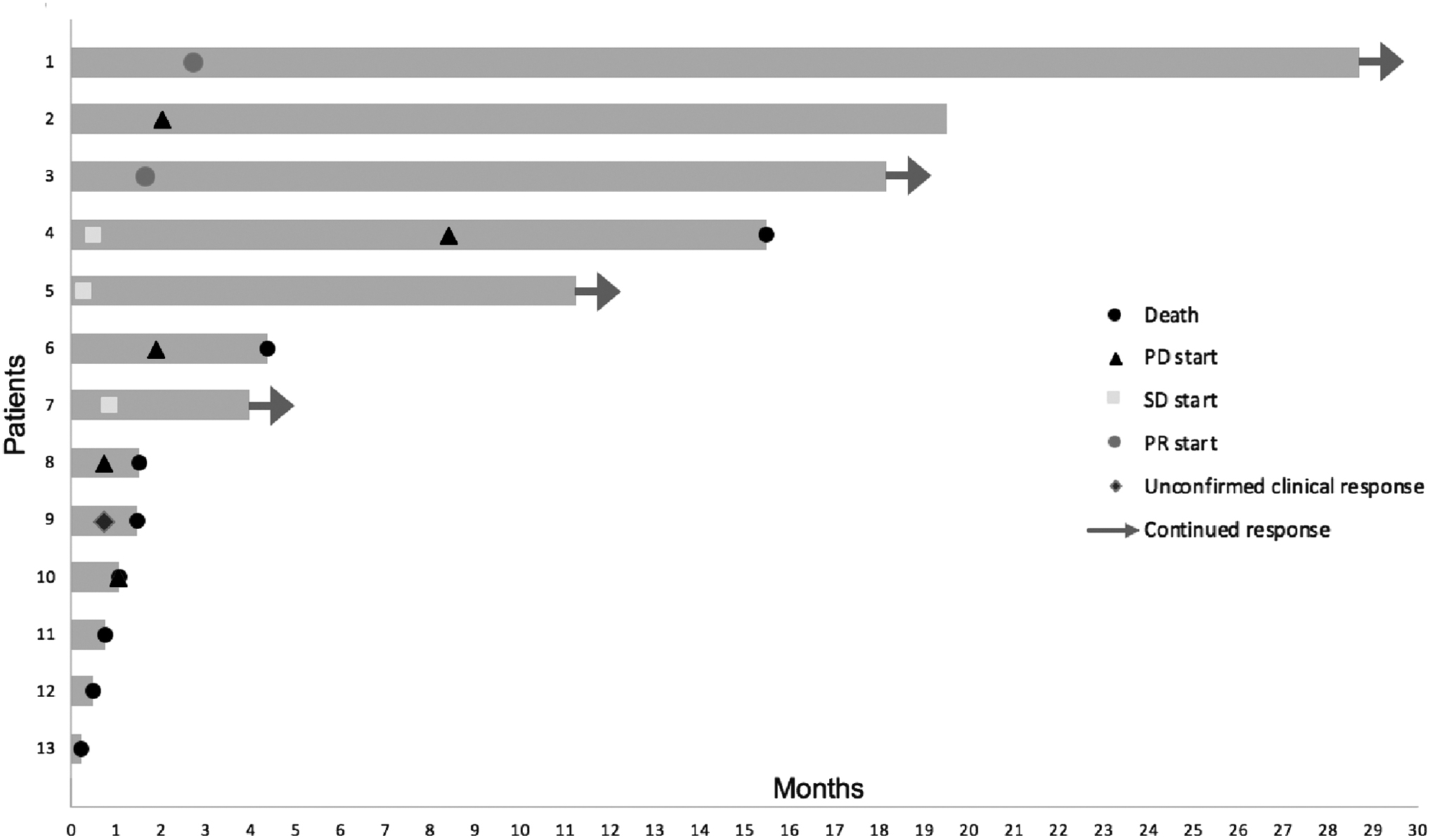
Swimmer plot of responses to immunotherapy. PD, progressive disease; PR, partial response; SD, stable disease.
Survival and Response Rates
Unconfirmed due to death.
CI, confidence interval; IQR, interquartile range; OS, overall survival; PFS, progression-free survival; RECIST, response evaluation criteria in solid tumors.
Responses were relatively durable considering the aggressive nature of this disease. One patient (#1) with a PR continues to be progression free at 29 months. This patient had stage IVA disease and did not have prior surgery or radiation (Fig. 4).
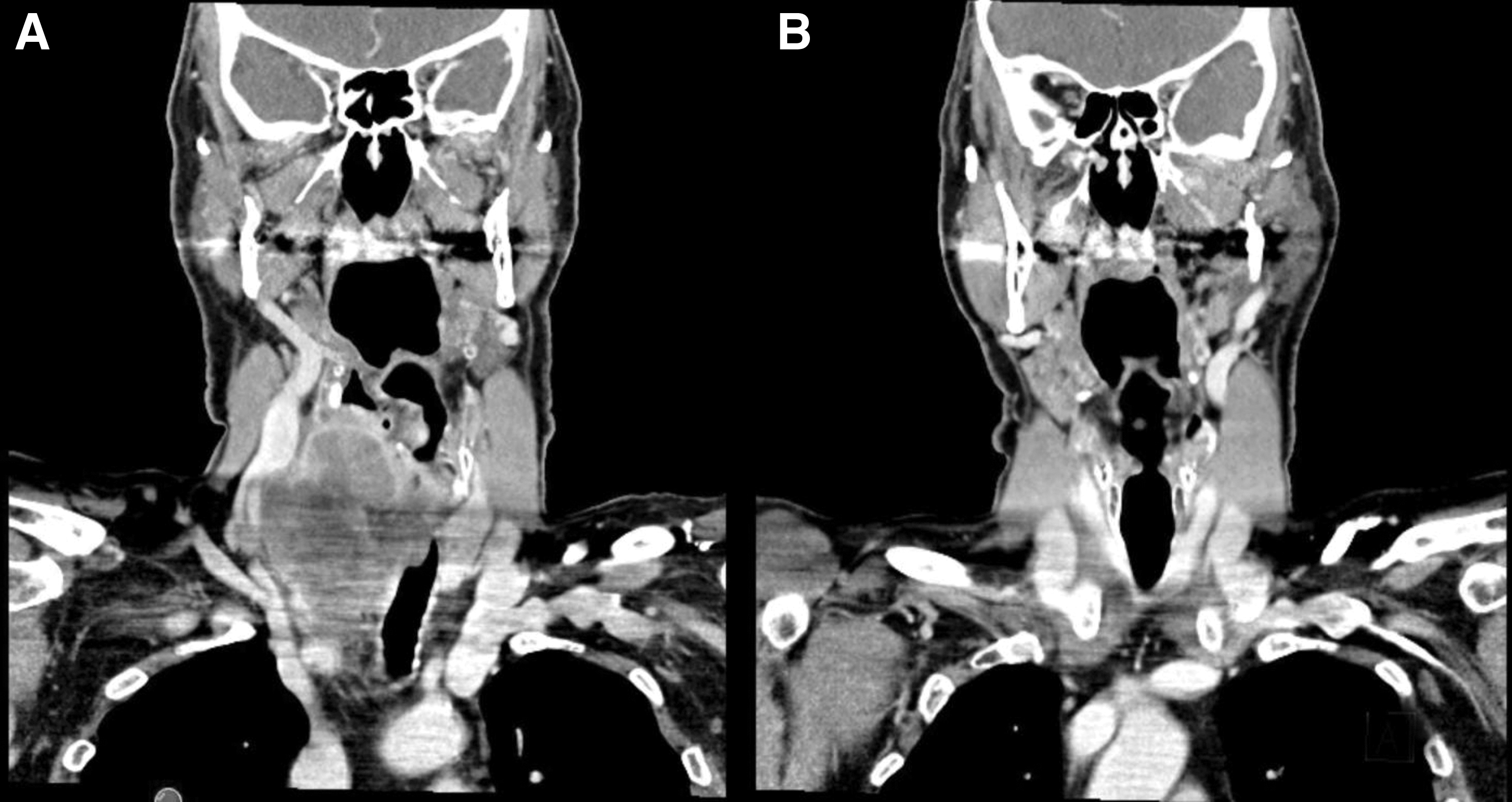
Patient #1. (
The second patient with a PR (#3) had stage IVC disease with metastases to lungs, axillary lymph nodes, and subcutaneous tissue. He began pembrolizumab after having progressed in the neck following nine weekly doses of chemotherapy with carboplatin and paclitaxel. Eleven months after initiation of treatment with pembrolizumab, the patient developed oligoprogressive disease in a discrete axillary lymph node, which was treated with local radiotherapy. This patient remains on pembrolizumab 18 months since beginning treatment.
The CBR was 38% (5/13 [CI 0.1–0.7]). Two patients (#4 and 7) had stable disease for 4 months (ongoing) and 8.5 months (ended). A third patient (#5) with stable disease experienced oligoprogression six months after initiation of treatment, which was also treated with local radiotherapy. This patient remains on pembrolizumab 12 months after initiation of treatment. Among the two patients with a PR, OS is 30 months and 22 months from date of diagnosis (both ongoing).
Among patients with a clinical benefit, after a median follow-up of 13.5 months, median OS had not been reached. Responses were ongoing in 4/5 subjects, with OS ranging between 4+ and 29+ months. The one-year survival rate was 38% (5/13 [CI 0.1–0.7]).
Reflecting the aggressive nature of ATC, four patients (#10, 11, 12, and 13) expired or entered comfort care within three weeks of their first dose and did not receive another dose of treatment. One patient (#2) developed recurrent fevers/chills from dabrafenib and trametinib, and therapy was switched to pembrolizumab. This patient had immediate progressive disease noted on the first set of scans following nine weeks of therapy, and pembrolizumab was discontinued.
Concurrent chemo-radiation followed by chemotherapy was initiated and the patient remains alive with stable disease at 20 months after being treated with pembrolizumab. The unusually prolonged period of disease stability raises the possibility that the progressive disease noted may have been related to rebound increased MAPK signaling from TKI withdrawal, a phenomenon that has been described in malignant melanomas, as opposed to a lack of efficacy of immune checkpoint blockade (16).
Overall, the median duration of immunotherapy was 1.9 months (range: 1 week–29 months [ongoing]). The median OS was 3.9 months (Table 3 and Fig. 5A) and median PFS was 1.9 months (Table 3 and Fig. 5B). Limited sample sizes precluded formal statistical analysis of differences in OS by BRAF status or PD-L1 score (Fig. 5C). Among patients with PD-L1 score >50% (n = 8/10), the median OS was 15.5 months. The median OS from diagnosis was 15.6 months and remained unchanged regardless of BRAF status.
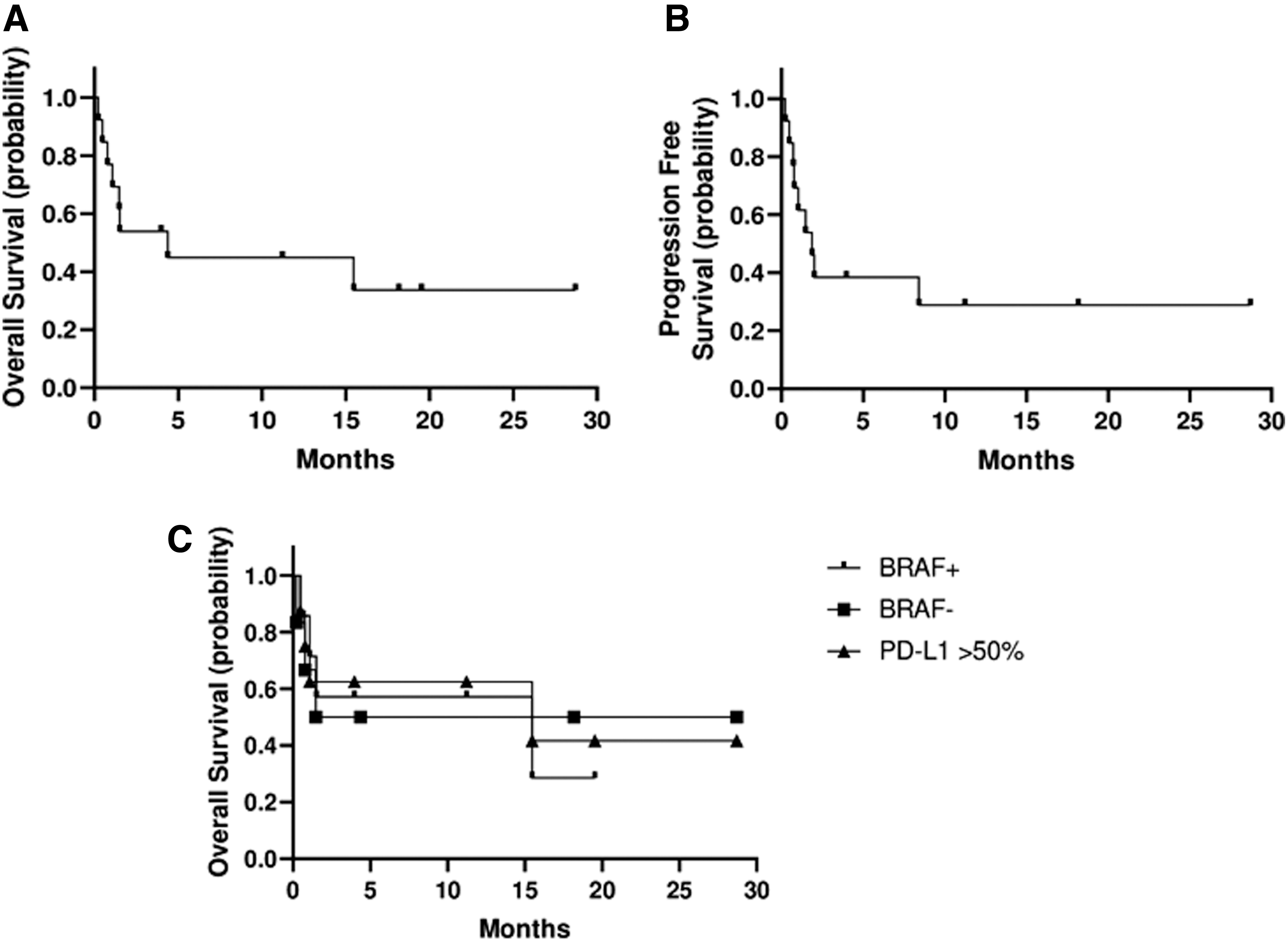
Survival. (
Safety
With regard to safety, there were few reports of adverse events related to immunotherapy (Table 4). Six patients (46%) experienced immune-related adverse events. Grade 3 and above adverse events were noted in two patients (15%).
Immune-Related Adverse Events
One patient (#9) developed grade 5 immune checkpoint-related thyroiditis. This was a 91-year-old female patient with a past medical history of atrial fibrillation and chronic heart failure. She was diagnosed with stage IVB ATC and was started on pembrolizumab. After just two cycles of treatment, she experienced a dramatic shrinkage in her neck mass clinically, but developed tachycardia and shortness of breath and was found to have atrial fibrillation with rapid ventricular response.
Thyrotropin was found to be suppressed to 0.06 and free thyroxine was elevated to 2.65 (upper limit of the normal range = 1.7). Despite treatment with steroids and beta-adrenergic blockade, her respiratory status continued to worsen, and ultimately the patient chose to enter hospice and expired shortly afterward before restaging scans could be performed.
Another patient (#6) developed grade 3 hyperglycemia possibly related to immune checkpoint inhibition.
Two patients (#1 and 3) developed grade 1 dermatologic toxicities: pruritus and lichen planus, which resolved with topical treatments. One patient (#4) experienced grade 2 joint pain, myalgias, and neuropathy, which were responsive to steroids, while another patient (#5) developed diplopia and Bell's palsy. While Bell's palsy was likely not treatment related, causation could not be completely ruled out. At the cutoff date, there were eight deaths in the cohort, all (but one) related to progressive disease.
Discussion
Since 2017, there has been increasing recognition of the clinical efficacy of immune checkpoint blockade in treatment of ATC. Reflecting the aggressive nature of the disease, the majority of patients received two or fewer months of treatment and discontinued therapy due to disease progression and rapid clinical deterioration. However, one patient who received only two doses of pembrolizumab achieved a clinical response; two other patients had PR and continued on therapy for 18+ and 29+ months at the time of preparation of the manuscript.
Among patients who achieved a response, the PD-L1 status was unknown for the patient who achieved the radiologically unconfirmed response, while the remaining two patients with PR were PD-L1 positive with a CPS of 40% and 95%, respectively. Similarly, patients with stable disease had tumors with high CPSs of 95% and 100%.
The ORR of 15% and disease control rate of 38% with duration of response of 18 and 29 months in patients with PR are clinically meaningful for this disease given its exceptional resistance to chemotherapy and radiotherapy after progression on prior treatment. This result is corroborated by phase II data of spartalizumab, which reported an objective response rate of 19% and disease control rate of 31%.
There is emerging evidence that resistance to single-agent checkpoint blockade may be mediated through vascular endothelial growth factor (VEGF) signaling. Iyer et al. reported 12 patients with ATC who were treated with combination therapy of pembrolizumab with VEGF TKIs. A PR rate of 42% (5/12) and stable disease rate of 33% (4/12) were encountered (17).
Further evidence of the efficacy of this approach is available from an interim analysis performed in the European phase II study (Anaplastic Thyroid Carcinoma Lenvatinib Pembrolizumab) of the combination of lenvatinib and pembrolizumab. Among 26 evaluable patients, the ORR was 39% (10/26 PR). PFS was 8.3 months and OS was 10 months. Among 16 patients with a two-year follow-up, the ORR was 69% (11/16 PR) and stable disease rate was 31% (5/16). The CBR was 100% (18).
The strength of this study is that detailed information about patterns of response, toxicity, and efficacy of immune checkpoint inhibition is available from a cohort of ATC patients who had extensive prior treatments, including surgery, chemotherapy, and radiation alone or in concurrent manner, as well as BRAF-directed treatments. These results may therefore be broadly applicable to the typical patient population encountered in practice.
The major limitations are the limited sample size, single center, and retrospective nature, which preclude more rigorous subset analysis of PD-L1 and BRAF mutation status as predictors of response. A lack of universal molecular characterization due to limited availability of tissue from scant cytological specimens is also a limitation. In addition, it is unclear if immunotherapy is most effective in the up-front setting versus in the later lines of therapy. These are questions that warrant further investigation.
However, our results are broadly in agreement with published data on spartalizumab and add to the evidence of efficacy of immune checkpoint blockade in ATC. There are currently a number of ongoing clinical trials testing pembrolizumab (NCT02688608), nivolumab plus ipilimumab (NCT03246958), and atezolizumab (NCT03181100) as well as the combination of anti-PD-1/PD-L1 with targeted therapies in ATC, the results of which are awaited.
In conclusion, patients with ATC experience significant morbidity and mortality due to the aggressive nature of the malignancy in addition to the lack of response to conventional therapy options after disease progression. Immune checkpoint blockade may be an effective, well-tolerated treatment option for a subset of patients with ATC.
A one-year survival of close to 40% was encountered. Biomarkers of clinical benefit will need to be rigorously evaluated to identify the mechanistic underpinnings of response and resistance to immune checkpoint blockade in ATC patients.
Footnotes
Authors' Contributions
A.H. participated in the design, collection and assembly of data, data analysis and interpretation, and manuscript writing.
B.A. and H.A. participated in the conception and design, provision of study patients, collection of data, data analysis and interpretation, and manuscript writing.
M.H.S. and B.K. participated in data analysis and interpretation and manuscript writing.
A.L.L. interpreted the PD-L1 IHC stains and provided representative images.
M.X. participated in data analysis and interpretation.
V.S. participated in collection and assembly of data, data analysis and interpretation, and manuscript writing.
Author Disclosure Statement
A.H., B.A., H.A., M.X., A.L.L., and V.S. have no conflicts of interest to disclose. M.S. declares research funding from Merck and Eli Lilly and Co. B.K. declares grant funding (to the institution) from Eli Lilly and Co., Eisai, Merck, Xencor, and Bristol Myers Squibb.
Funding Information
No funding was received for this article.