
Abstract
Background:
Previous studies suggested that mercury may be linked to thyroid cancer due to its bioaccumulation in the thyroid gland, but no studies have evaluated the association between mercury exposure and thyroid cancer risk. We examined the relationship between mercury exposure and thyroid cancer risk, with the potential modification of hematological parameters.
Methods:
We performed a secondary analysis of a prospective cohort study among residents living near industrial complexes in South Korea (recruited from 2003 to 2011). Incident thyroid cancer cases (C73, ICD-10 code) were identified from the National Cancer Registry and Statistics Korea. Urinary mercury concentrations were measured using thermal decomposition amalgamation atomic absorption spectrometry (TDA-AAS). Cox proportional hazards regression models (adjusted for age, sex, educational level, smoking status, and employment) were used to estimate the hazard ratio (HR) and confidence interval [CI] between mercury exposure and the incidence of thyroid cancer.
Results:
We documented 69 cases of thyroid cancer in a total of 5213 participants during follow-up (median 8.7 years). The geometric mean of urinary mercury concentration was 1.8 μg/L for thyroid cancer cases and 1.2 μg/L for noncases (p for difference = 0.001). After adjusting for potential confounders, those in the highest tertile of urinary mercury levels had a twofold higher risk of thyroid cancer (HR = 1.97 [CI 1.03 − 3.80] in the highest tertile vs. the lowest tertile, p for trend = 0.043). This association was stronger for those with lower mean corpuscular volume and mean corpuscular hemoglobin status.
Conclusions:
Urinary mercury concentration was positively associated with the risk of thyroid cancer among residents living near national industrial complexes, and this association was influenced by red blood cell indices status. These results provide some evidence suggesting the adverse effects of environmental metal pollution in the development of thyroid cancer.
Introduction
The global incidence of thyroid cancer has continuously increased in recent decades. 1 In 2018, the Global Cancer Observatory estimated 567,000 new thyroid cancer cases and 41,000 thyroid cancer deaths worldwide. 1 This trend is projected to lead thyroid cancer to the fourth most common cancer by 2030. 2 South Korea is one of the rapidly emerging thyroid cancer epidemic areas 3 with the highest incidence rate worldwide, 4 partially due to improved detection. 5
Substantial variation in the incidence of thyroid cancer has been observed in different parts of the world, which may be related to differences in diagnostic practices, 6 individual risk factors (physical activity, imbalanced iodine intake, and obesity), 6,7 and environmental exposures (radiation, ethnicity, and geographical area). 8,9 Recently, a high incidence of thyroid cancer has been reported in some volcanic and industrial areas. 10,11 Although the reason for the observed high incidence has not been well defined, these regions are contaminated with heavy metals such as cadmium and mercury, suggesting that heavy metals may play a role in the development of thyroid cancer. 12
Mercury is a metal pollutant of global concern and comes from nature (e.g., volcanoes, soils, waters, and mercury-rich geological zones) as well as a wide range of anthropogenic activities (e.g., mining, metal smelting, coal production, and incinerators). 13,14 There are three forms of mercury: elemental mercury (Hg°), inorganic mercury (Hg+ and Hg2+), and organic mercury (methyl, ethyl, and phenyl). 15 In nature, mercury exists in low levels, but it poses health risks to humans due to its persistency, bioaccumulation, and toxicity. 16
Mercury has been reported to accumulate in the thyroid gland of animals 17,18 and humans. 18,19 Recent studies suggest that mercury may trigger genotoxicity, autoimmune reactions, and oxidative damage, which raises the possibility that mercury could have a role in the pathogenesis of thyroid cancers. 19,20 However, there are few epidemiological studies of mercury and thyroid cancers, and most cancer studies have evaluated blood mercury as a relatively short-term indicator. 21 –25
Mercury induces oxidative stress, oxidizes hemoglobin (Hb), impairs the antioxidant defense mechanism, and alters metabolic pathways in human erythrocytes. 26 Recently, mercury-induced changes in erythrocytes were related to diseases such as anemia, hypertension, and cardiovascular diseases. 27,28 Red blood cells (RBCs) also have been proposed as an important model for elucidating the mechanism of heavy metal toxicity. 28 Several prospective studies reported that abnormal hematological conditions might serve as potential surrogate markers for some cancers 29 –32 because changes in these indices could reflect long-term exposure to oxidative stress, which can trigger tumorigenesis. 33
Therefore, it is relevant to investigate the effect modification of hematological parameters as alternative oxidative stress markers in a potential association between mercury and thyroid cancer risk.
We examined the association between urinary mercury concentrations and the risk of thyroid cancer and the effect modification of hematobiochemical alterations among residents living near national industrial complexes in South Korea.
Methods
Data sources and populations
We conducted a secondary analysis of data from the “Monitoring Project for Exposure to Environmental Pollutants and Health Effects Among Residents Living Near Industrial Complexes” survey (hereafter, the “Monitoring Project,” National Institute of Environmental Research [NIER] in South Korea). The Monitoring Project was a prospective multicenter population-based cohort study to investigate the adverse health effects of environmental chemicals, which was conducted in 12 regions located near national industrial complexes in Korea between 2003 and 2011.
Participant demographic and personal information were collected by trained interviewers, and included socioeconomics, lifestyle, indoor and outdoor environment, and medical history. Participants also received medical assessments and provided their blood and urine samples for measurement of the internal levels of environmental chemicals. Study participants were linked to cancer registration records (National Cancer Registry) and death certificates (Statistics Korea) using a personal identification number as described previously. 34,35 Data linkage was conducted by the National Cancer Center in collaboration with the National Institute of Environmental Research.
Our initial cohort included 11,138 participants aged 19 years and older at baseline, with documented information about their cancer diagnosis, and who did not have a history of cancer before baseline. Of these, 6798 participants were randomly selected based on their age, sex, and region for measurement of urinary mercury concentrations.
We excluded the following participants: those who were diagnosed with cancer (except for skin cancer) within 1 year of the baseline survey (n = 47); those who lacked data for urinary creatinine measurement or those with creatinine levels <30 or >300 mg/dL (n = 260); and those who had missing values for covariates such as educational level, smoking status, employment status, and body mass index (BMI) (n = 1278). As a result, we included 5213 participants (1990 men and 3223 women) in the analysis (Fig. 1).

Flowchart of study participants and exclusion criteria.
The study protocol was reviewed and approved by the institutional review board of the National Cancer Center, Goyang, Korea (NCC2021-0297). All participants provided informed consent.
Identification of cancer cases
We defined new cancer cases as primary cancer of thyroid (International Classification of Disease, 10th Revision [ICD-10] code C73) or cancer at all sites (ICD-10, codes C00–C97). New cancer cases in the cohort were determined from annual follow-ups of data from the National Cancer Registry and death certificate information from 2003 to 2016. The Korean Ministry of Health and Welfare established a nationwide hospital-based cancer registry in 1980 that involved >180 hospitals equipped with histopathology laboratories, which represented ∼99% of new cancer cases in Korea. 36 All thyroid cancer cases in the study were detected by biopsy (98.5%) or cytology (1.5%) while the participants were alive.
Mercury concentration in urine
A spot urine sample was collected in polyethylene tubes at each local center, and then frozen and stored at −20°C before analysis. Urinary mercury concentration was measured by conducting thermal decomposition amalgamation atomic absorption spectrometry (TDA-AAS). Quality assurance and control were performed according to the procedures and guidelines of the NIER in South Korea. The range of precision should be within ±25% and the accuracy within 75–125%. The correlation coefficient of the calibration curve was >0.99.
The limit of detection (LOD) for urinary mercury in different regions was as follows: 0.1 μg/L in Pohang; 0.01 μg/L in Cheongju and Daesan; 0.03 − 0.3 μg/L in Ulsan; 0.01 − 0.1 μg/L in Gwangyang, Yeosu, Hadong, and Namhae; 0.01 μg/L in Gangneung; and 0.05 μg/L in Chungju. The final mercury values were adjusted for creatinine concentration.
Hematological parameters
Blood samples were collected after study participants fasted for eight hours. Hematological parameters were analyzed using flow cytometry (Coulter Counter MAXM; Coulter Electronics). The following six RBC parameters were considered as potential modifiers: RBC count (106/μL), Hb (g/dL), hematocrit (Hct, %), mean corpuscular volume (MCV, fL), mean corpuscular hemoglobin (MCH, pg), and mean corpuscular hemoglobin concentration (MCHC, g/dL).
Statistical analyses
Creatinine-adjusted mercury concentrations were natural log transformed because of their skewed distribution and then categorized into three groups according to tertile, with the lowest tertile used as the reference group. We used all measured values of urinary mercury including values below the LOD, where those values ranked in the reference group. 37
Estimates of baseline characteristics are presented as means ± standard deviations (SDs) for continuous variables or frequency with percentages for categorical variables. Differences in baseline characteristics according to tertiles of urinary mercury concentrations were assessed using Tukey's multiple comparison post-test, and p-values for linear trends were obtained by treating the median value in tertiles of mercury as a continuous variable in the general linear model. Urinary mercury concentrations were compared using Student's t-test. The cross-sectional relationships between mercury and RBC parameters were evaluated using Pearson's correlation coefficient.
To estimate the hazard ratio (HR) and confidence interval [CI] between mercury and cancer risk, the random-effects Cox's proportional hazard regression model was used with follow-up period as the timescale. The person-year for participants with recorded cancer cases was calculated between the baseline date and the first diagnosis date of any cancer (except for skin cancer). For participants without recorded cancer cases, the person-year was calculated between the baseline date and the censoring date. If participants did not have a recorded date of cancer incidence or death, they were censored on December 31, 2016.
The proportional hazard assumption using Schoenfeld's residual test was not violated. Potential confounders that were known risk factors for thyroid cancer were selected from a recent review. 6 The directed acyclic graph 38 was used to select the covariates in the final statistical models (Supplementary Fig. S1) as follows: age at baseline, sex, education level (≤12 or >12 years), smoking status (yes or no), BMI (<25 or ≥25 kg/m2), and employment status (yes or no). We included survey year and region by random effect to adjust for potential heterogeneity from the six national industrial complexes.
To test the significance of linear trends across categories of urinary mercury, p-values for trends were computed by fitting the exposure tertile as an ordinal categorical variable, and then treating this as a continuous variable in the Cox's proportional hazards model. We tested for potential effect modification by hematological parameters by conducting stratified analyses and evaluating interaction terms.
All statistical analyses were performed using SAS software (Version 9.4; SAS Institute, Inc., Cary, NC, USA). The statistical significance level was set at 0.05 in two-sided tests.
Results
Study population characteristics and urinary mercury concentrations
A total of 5213 participants were included in this study. We documented 310 cases of all cancers and 69 cases of thyroid cancer during follow-up (median 8.7 years). Baseline characteristics of the study population according to tertiles of urinary mercury concentrations are given in Table 1. Participants with higher exposure to mercury tended to be older, more likely to be female, less educated, less likely to be smokers, and more likely unemployed. The hematological indices of RBC, Hb, Hct, and MCHC were significantly lower in participants with the highest tertile of mercury exposure than those with the lowest tertile. By contrast, MCV was higher in those with the highest tertile of mercury exposure than in those with the lowest tertile.
Baseline Characteristics of the Study Participants According to Tertiles of Urinary Mercury Concentrations
Values are expressed as means ± SDs or frequency (%).
p Values for differences were computed by the GLM using Tukey's multiple comparison post-test.
p for linear trends were obtained by treating participants the median value in their tertiles of mercury as a continuous variable using the GLM.
BMI, body mass index; GLM, general linear model; Hb, hemoglobin; Hct, hematocrit; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; RBC, red blood cell; SD, standard deviation.
Table 2 gives the distribution of urinary mercury concentrations in the study population. Participants with thyroid cancer cases had significantly higher geometric mean of urinary mercury concentration than noncases. Higher urinary mercury concentrations were observed in women and nonsmokers in all cancer cases. By contrast, urinary mercury concentrations did not significantly differ according to the participant characteristics in thyroid cancer cases (Table 3).
Distribution of Mercury Concentration
p Values for difference between cases and noncases were tested by Student's t-test.
GM, geometric means; GSD, geometric standard deviation.
Mercury Concentrations in Urine by the Characteristics of Study Population
p Values for difference according to the subgroups were tested by Student's t-test.
Correlation between urinary mercury concentrations and RBC parameters
The distributions and correlations of urinary mercury concentrations and RBC parameters are presented in Figure 2. The RBC count, Hb level, and Hct level were strongly correlated (r = 0.67–0.97, p < 0.001). The mercury concentration was negatively correlated with Hb, Hct, and MCHC levels in both thyroid cancer cases and noncases. The mercury concentration was positively correlated with RBC (r = 0.15, p > 0.05) and negatively correlated with MCV levels (r = −0.23, p > 0.05) in thyroid cancer cases, whereas it was negatively correlated with RBC (r = −0.08, p < 0.001) and positively correlated with MCV (r = 0.04, p < 0.01) in nonthyroid cancer cases.
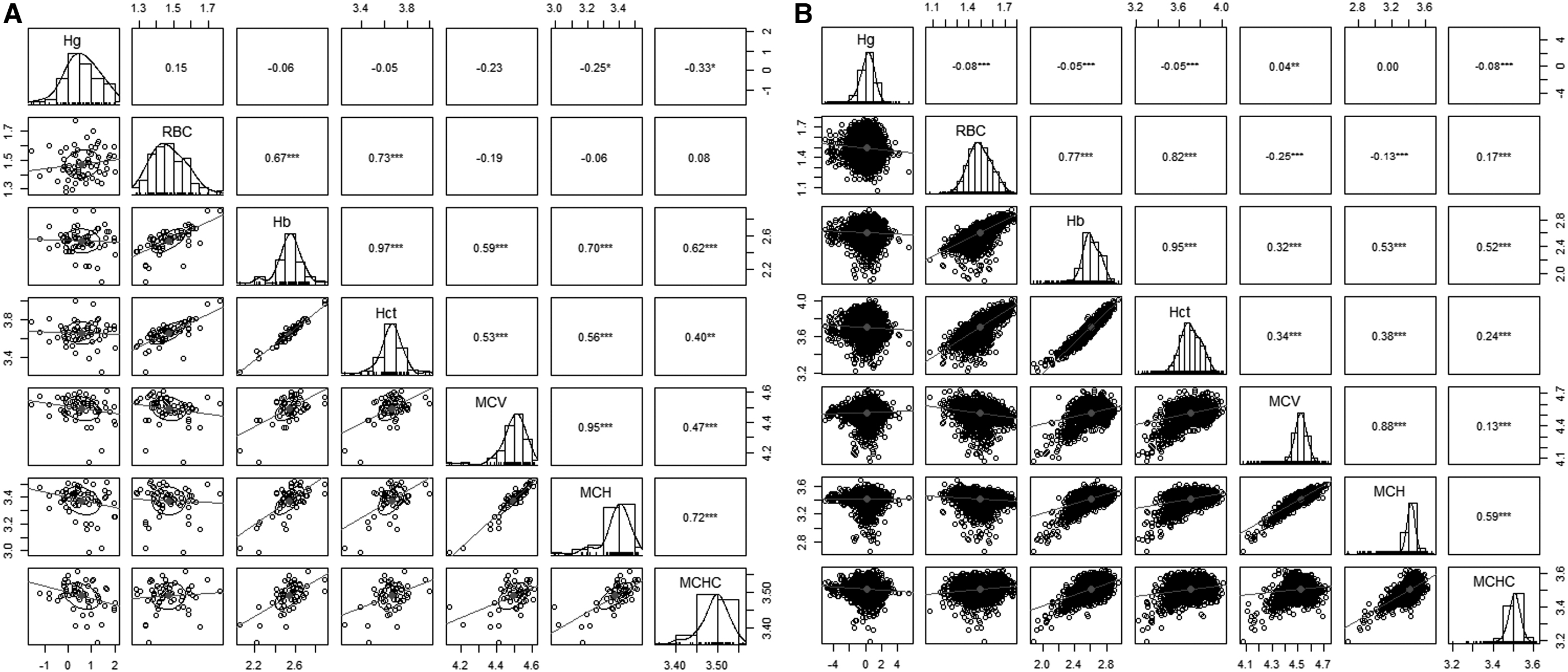
Correlation matrix of urinary mercury and hematological parameters in thyroid cancer cases (
Urinary mercury concentration and cancer risk
The associations of urinary mercury with risks of all cancer and thyroid cancer are presented in Table 4. In the age- and sex-adjusted model, urinary mercury concentration was positively associated with the risk of thyroid cancer (HR = 2.11 [CI 1.11–4.03] in T3 vs. T1, p for trend = 0.023). This positive association was still significant even after adjusting for potential confounders (HR = 1.97 [CI 1.03–3.80] in T3 vs. T1, p for trend = 0.043). However, we did not find a significant association between urinary mercury concentration and all cancers.
The Hazard Ratio and Confidence Intervals for All Cancer and Thyroid Cancer According to Tertiles of Urinary Mercury Concentration
p for linear trends were obtained by treating participants the median value in their tertiles of mercury as a continuous variable in the Cox's proportional hazards model.
Model 1 was adjusted for age (years) and sex (men/women).
Model 2 was adjusted for age (years), sex (men/women), education level (≤12/>12 years), smoking status (yes or no), employment (yes or no), BMI (<25/≥25 kg/m2), survey year (random effect), and region (random effect).
CI, confidence interval; HR, hazard ratios.
Effect modification of thyroid cancer by hematological parameters
We tested whether hematological parameters affected the association between urinary mercury concentration and thyroid cancer by conducting stratified analyses using the median value of each RBC parameter and evaluating interaction terms (Table 5). Although all p-values for interactions were higher than the level of significance (p > 0.05, data not shown), we observed that urinary mercury was more strongly associated with increased risk of thyroid cancer in groups with lower MCV and MCH levels (adjusted model 2: HR = 2.78 [CI 1.16–6.63] in T3 vs. T1, p for trend = 0.017 for MCV ≤ median; HR = 2.60 [CI 1.11–6.12] in T3 vs. T1, p for trend = 0.019 for MCH ≤ median).
The Hazard Ratio and Confidence Intervals for All Cancer and Thyroid Cancer According to Tertiles of Urinary Mercury Concentration by Hematological Parameters
Statistical models given were adjusted for age (years), sex (men/women), education level (≤12/>12 years), smoking status (yes or no), employment (yes or no), BMI (<25/≥25 kg/m2), survey year (random effect), and region (random effect).
Stratified by median value of each hematological parameter.
p for linear trends was obtained by treating participants the median value in their tertiles of mercury as a continuous variable in the Cox's proportional hazards model.
Discussion
We found that urinary mercury concentration was positively associated with the risk of thyroid cancer among residents living near national industrial complexes in Korea. This association was stronger for those who had lower values of two RBC indices: MCV and MCH. However, there was no significant association between urinary mercury concentration and all cancer risk in this study.
Mercury undergoes biological transformation and interconversion to circulate between the environment and human beings. Therefore, all humans have the potential for short-term and long-term exposure to mercury compounds with regional differences. 39 In this study, the geometric mean of urinary mercury concentration (adjusted for creatinine) was 1.3 μg/g creatinine (median 1.4 μg/g creatinine). This value was higher than the urinary mercury concentration in the general population of Western countries such as Canada (median 0.22 μg/g creatinine), 14 Germany (median 0.4 μg/L), 39 and the United States (median 0.30 μg/g creatinine), 40 but similar to those in the western Pacific region (median 1.4 μg/L) 39 with relatively high consumption of seafoods and grains, the major sources of mercury. 41
In general, the urinary mercury concentration in people without known exposure to mercury is <5 μg/L. 42 The German Human Biomonitoring (HBM) Commission recommends toxicologically based guidance values for urinary mercury concentration of 7 μg/L (5 μg/g creatinine, HBM I) and 25 μg/L (20 μg/g creatinine, HBM II). 43 This study population comprised the residents living near national industrial complexes who coexist with environmental pollutants in their daily lives, although the levels were within normal range. Their urinary mercury levels could have reflected the atmospheric mercury concentrations from industrial emissions.
Mercury toxicity has been evaluated in experimental and epidemiological studies, which primarily focus on the nervous system and kidney where mercury accumulation occurs. 20 However, several studies reported that mercury also accumulated in the thyroid gland of animals 17,18 and humans. 18,19 Two autopsy studies of mine workers reported that inorganic mercury concentrations were higher in thyroid than in kidneys. 44,45 A recent autopsy study observed mercury in human thyroid cells, and the proportion of thyroid cells containing mercury increased with age. 20
A study of residents near volcanic areas reported that many trace elements, including Hg, were more concentrated in the thyroid tissue than in muscle and fat tissue. 18 Therefore, mercury could have toxic and carcinogenic effects in the thyroid gland because the high affinity of mercury in specific organs can impair the organ system function, such as the effects of mercury in kidney. 46
To our knowledge, this study was the first investigation of the association between environmentally exposed low-level mercury and thyroid cancer. Several ecological studies postulated that mercury was associated with thyroid cancer due to the high incidence rate of thyroid cancer in metal-polluted areas such as volcanic and industrial sites. Hawaii is the most active volcanic region in the United States, and it has the highest rate of thyroid cancer in the nation. 47 Other volcanic areas such as Vanuatu, 48 New Caledonia, 49 and Catania province in Italy 50 also have high incidence of thyroid cancer.
Residents near Mt. Etna (Catania province, Italy) have higher urinary concentrations of cadmium, mercury, and manganese than residents in nonvolcanic areas, with mercury levels 2.6 times higher. 10 Residents near industrial plant sites in Italy had significantly higher risk of thyroid cancer than reference rates of the Italian macro area between 2006 and 2013. 11 Those studies did not identify specific factors that increase the thyroid cancer incidence due to the limited ecological study design, but they suspected mercury as an endocrine-disrupting factor involved in the pathogenesis of thyroid cancer. 11,12
The role of mercury in the development of thyroid cancer has not been established, but experimental studies suggest that mercury may be a carcinogen. Volcanic environmental levels of mercury promoted the proliferation of thyroid stem/precursor cells in vitro, but not mature thyroid cells; this proliferation occurred through activation of the ERK1/2 pathway, which is a central regulator of cell proliferation that controls cell growth and cell cycle progression. 51 Those authors suggest that low concentrations of mercury can damage immature thyroid cells but not mature cells, and the damaged progenitor cell produces progeny cells that are susceptible to transformation, eventually resulting in thyroid tumorigenesis.
Another proposed carcinogenic pathway considers that mercury may inhibit gap junction intercellular communication and proinflammatory cytokine release. This potentially isolates cells from tissue-specific homeostasis and promotes cell proliferation. 20 Mercury also is involved in the detoxification system. Mercury compounds have high affinity for sulfhydryl groups, and this can inactivate selenocysteine antioxidant enzymes such as glutathione peroxidase and thioredoxin reductase. 52 This can disrupt the homeostasis of reactive oxygen species and increase cellular oxidative stress, 20 resulting in thyroid tumorigenesis by stimulating MAP kinase and PI3K/Akt pathway genes such as BRAF, PIK3CA, PTEN, and RAS. 53,54
We found that the association between mercury and thyroid cancer was influenced by hematological status. Blood is a known target of mercury, and mercury preferentially accumulates in RBCs because of its high affinity for sulfhydryl groups on Hb and glutathione. 52 Mercury accumulation in RBCs induces oxidative stress, oxidizes Hb, impairs the antioxidant defense mechanism, and alters metabolic pathways in human erythrocytes. 26 RBCs have a powerful antioxidant defense system and contribute to removing oxidative products.
However, if damaged RBCs arrive at inflamed tissues, their role changes from reactive oxygen species (ROS) scavenger to ROS generator, thereby promoting an oxidative microenvironment favoring tumorigenesis. 33 Our findings that urinary mercury concentration was negatively correlated with Hb and Hct are consistent with previous studies of mercury-exposed artisanal and small-scale gold miners 55,56 and individuals with dental amalgams. 57 In addition, we observed that the correlation between mercury concentration and RBC count was positive in thyroid cancer cases and negative in noncases.
Similarly, our stratified analyses showed that the positive association between mercury and thyroid cancer was stronger in groups with higher RBCs and lower MCV and MCH. Based on the results of our study, we believe that mercury-induced morphological and oxidative changes in RBCs may be a surrogate marker for the development of thyroid cancer. Further epidemiological and experimental studies are needed to determine the role of RBCs in the mechanism of mercury-induced disease.
This study had several strengths: it used a prospective, multicenter, and population-based cohort design with complete follow-up data through linkage with national cancer registries. We assessed long-term exposure to mercury by measuring urinary mercury concentration, which is a direct and validated biomarker. 13 Thus, urinary mercury concentration is a suitable biomarker for monitoring mercury exposure in residents living near national industrial complexes. However, our study also had some limitations that require caution when interpreting our results. First, we measured urinary mercury at a single time point, and could not estimate potential temporal fluctuations in urinary mercury concentration.
Second, we cannot rule out that some carcinogens such as cadmium and arsenic may have affected the association between mercury exposure and thyroid cancer risk. However, our data indicate that urinary mercury was poorly correlated with urinary cadmium and arsenic (ρ = 0.28 and 0.12, respectively), although the sample size decreased due to the lack of available data for cadmium and arsenic concentrations. We also conducted a stratified analysis of the median cadmium and arsenic levels; although the results displayed positive trends, they did not achieve sufficient statistical power due to fewer thyroid cancer cases (data not shown).
Third, we did not consider possible confounders such as dietary factors and family history of thyroid cancer. However, this study was meaningful because it verified the adverse health effects of industrial complexes using high statistical power in large-scale environmental epidemiology monitoring studies. Fourth, we cannot obtain information on clinical features such as tumor stage, size, histotype, or treatment for thyroid cancer and medical conditions of thyroid. To better understand the pathomechanism by which mercury acts on thyroid cancer, future studies are needed to consider qualitative and quantitative changes during the development of thyroid cancer.
Finally, the small sample size of incident thyroid cancer cases was unable to define clinical hematological status. Future studies are needed to extend the clinically relevant evidence, particularly for anemia.
Conclusions
There is insufficient data to definitively assess the carcinogenicity of mercury, especially in long-term studies and those assessing environmentally low levels of mercury. 58 Our findings support the results of previous studies that suggested the association between mercury and thyroid cancer risk and provide further evidence for the role of environmental metals in the development of thyroid cancer.
Footnotes
Authors' Contributions
S.K. contributed to conceptualization, methodology, formal analysis, data curation, and writing—original draft. S.-H.S. was involved in project administration. C.-W.L. was in charge of project administration and writing—review and editing. J.-T.K., E.Y.P., J.-K.O, and H.-J.K. carried out writing—review and editing. E.P. took care of data curation and validation. B.K. was in charge of conceptualization, writing—original draft, writing—review and editing, supervision, and funding acquisition.
Acknowledgments
The authors thank all investigators who conducted this study and all participants in the research project (NIER-2016-01-038) supported by the National Institute of Environmental Research of the Republic of Korea.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a National Cancer Center grant funded by the Korea Government, Republic of Korea (NCC-2110240-1).
Supplementary Material
Supplementary Figure S1