
Abstract
Objective:
The use of antithyroid drugs (ATDs) carries potential risk for teratogenic effects. For women with well-controlled hyperthyroidism on a low dose of ATDs, drug withdrawal upon pregnancy is recommended by international medical guidelines. Therefore, it is necessary to determine the characteristics of patients suitable for ATD withdrawal, subsequent changes in thyroid function after ATD discontinuation, and its impact on pregnancy and offspring outcomes.
Methods:
This prospective study recruited 63 pregnant women with well-controlled Graves' hyperthyroidism who had stopped ATDs during early pregnancy. Patients were followed up until the end of pregnancy and data on pregnancy outcomes were collected.
Results:
Overall, 20 patients (31.7%) had rebound of hyperthyroidism. Patients with either subnormal thyrotropin (TSH) levels (TSH <0.35 mIU/L, odds ratio [OR] = 5.12, confidence interval [CI = 1.29–20.34], p = 0.03) or positive thyrotropin receptor antibody (TRAb) (TRAb >1.75 IU/L, OR = 3.79, [CI = 1.17–12.30], p = 0.02) at the time of ATDs withdrawal presented a higher risk of rebound than those with either normal TSH levels or negative TRAb. Patients with both subnormal TSH and positive TRAb at the time of ATD withdrawal were more likely to experience rebound (83.3%, 5/6) than those with both normal TSH and negative TRAb (13%, 3/23, OR = 33.33, [CI = 2.83–392.60], p = 0.003). The prevalence of adverse pregnancy outcomes was significantly higher in patients who experienced rebound compared with those who did not (55.0% vs. 9.3%, OR = 11.92, [CI = 3.08–46.18], p = 0.0002).
Conclusions:
Subnormal TSH levels and TRAb positivity at the time of ATD withdrawal in early pregnancy may be associated with rebound of Graves' hyperthyroidism. Rebound of hyperthyroidism during pregnancy may increase the risk of adverse pregnancy outcomes. Larger prospective studies are needed to confirm these findings.
Introduction
Graves' disease (GD) is the most common cause of hyperthyroidism among women of childbearing age (1). Uncontrolled thyrotoxicosis may increase pregnancy complications, such as pregnancy-induced hypertension, pre-eclampsia, placental abruption, miscarriage, and premature birth (2,3). Therefore, thyroid function should be well controlled in patients with hyperthyroidism who are planning to become pregnant (4,5). Antithyroid drugs (ATDs), such as methimazole (MMI) and propylthiouracil (PTU), are the treatment of choice for many patients with hyperthyroidism as they have the advantage of being easily orally administered (6). However, a disadvantage of ATDs is a high rate of relapse after withdrawal (50–60%) (7,8). Furthermore, both MMI and PTU can cross the placental barrier, which may increase the risk of birth defects, especially during the 6th to 10th week of gestation (9,10).
Given the potential teratogenic effects of ATDs, careful consideration should be made before their use during pregnancy. Both the American Thyroid Association (ATA) and the European Thyroid Association (ETA) recommend that patients taking ATDs should try to become pregnant only after their hyperthyroidism is well controlled (11,12). Appropriately selected patients may withdraw from ATD treatment as soon as pregnancy is diagnosed.
However, there is no direct evidence to indicate which patients meet the criteria for ATD withdrawal. Discontinuation of ATDs may be considered for GD patients with a low risk of rebound. The factors thought to be associated with a low risk of rebound in GD patients include a low thyrotropin receptor antibody (TRAb) level, having received ATDs for at least 6 months before becoming pregnant, and achieving an euthyroid state on a low dose of MMI (≤5–10 mg/day) or PTU (ATA: ≤100–200 mg/day, ETA: ≤50–100 mg/day) (11,12). However, the evidence for these criteria is derived from nonpregnant patients and may not be directly generalizable to pregnant women.
Therefore, in this prospective study, we recruited 63 women with well-controlled hyperthyroidism during early pregnancy. Participants were followed after ATD withdrawal and the changes in thyroid function were examined. We identified risk factors for hyperthyroidism rebound during pregnancy and determined its subsequent impact on pregnancy and fetal outcomes.
Materials and Methods
Subjects
Sixty-six patients with Graves' hyperthyroidism treated with ATDs (PTU or MMI) and completion of the sixth week of pregnancy were recruited by three senior endocrinologists at the outpatient service of Department of Endocrinology and Metabolism, First Affiliated Hospital of China Medical University (Shenyang, Liaoning Province, P.R. China). All participants were from Liaoning Province in Northeast China. Three participants were lost to follow-up. Hence, 63 patients were followed up every 1–3 months until their end of pregnancy between September 2014 and March 2017 (Fig. 1).
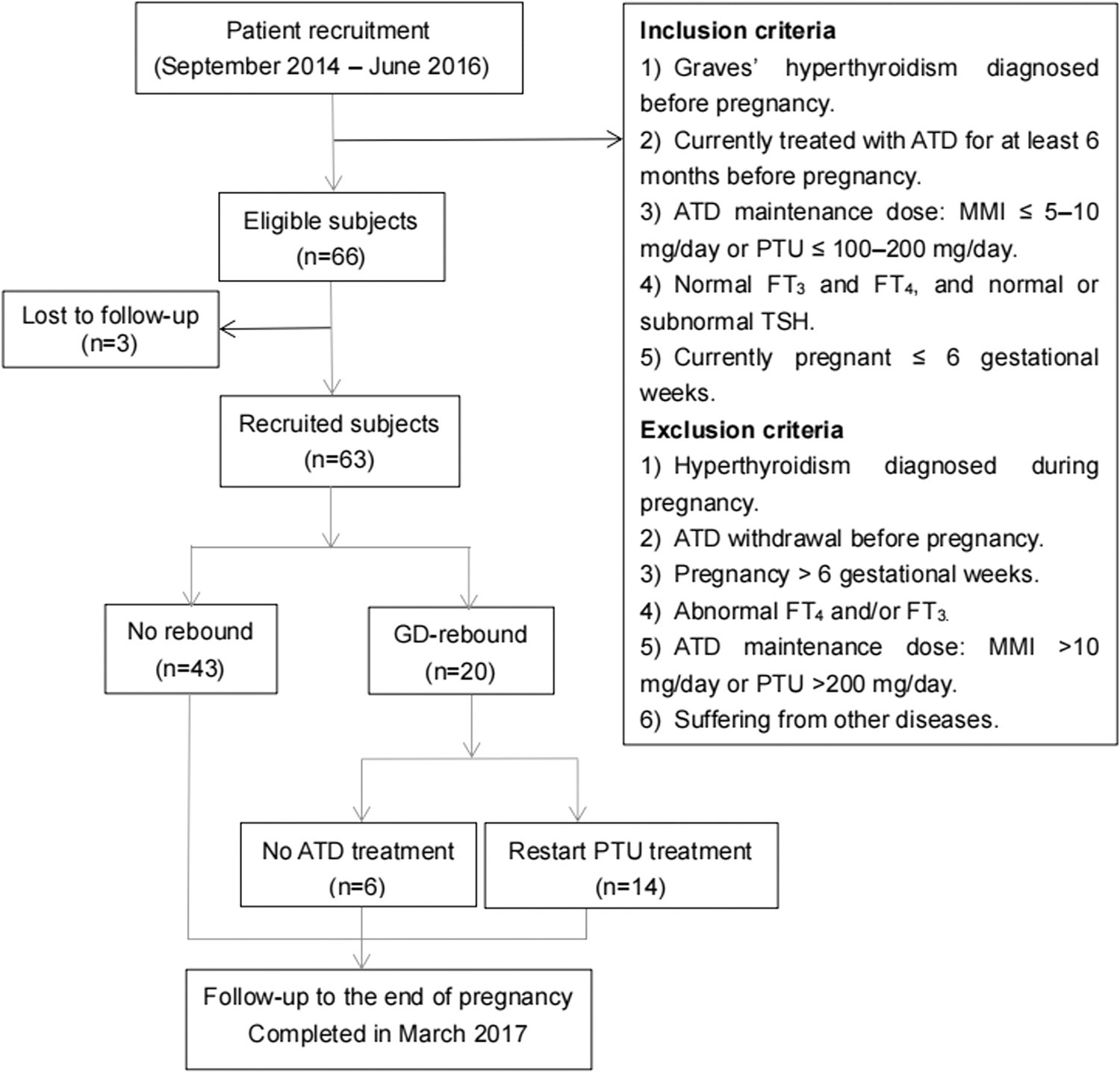
Flowchart of the subject recruitment and selection process. ATD, antithyroid drug; fT3, free triiodothyronine; fT4: free thyroxine; MMI, methimazole; PTU, propylthiouracil; TSH, thyrotropin.
Baseline data collection
Baseline data were collected using a standard questionnaire, which included current age, date of GD diagnosis, current ATD dose, ATD course (duration of ATD treatment before pregnancy), ATD withdrawal date, smoking status, disease history, current medication, miscarriage history, and family history.
Fasting blood samples were collected to evaluate thyroid function and thyroid autoantibodies at the time of ATD withdrawal.
Follow-up investigation and outcome assessment
We re-examined for thyroid function and thyroid autoantibodies two to four weeks after ATD withdrawal in the first trimester. Patients (n = 43) who remained euthyroid during the entire pregnancy were reassessed for thyroid function and autoantibodies every 2–3 months in the second and third trimesters. If a patient had GD rebound (n = 20), the physicians would discuss with the patient whether to restart ATDs according to the clinical practice guidelines (i.e., to maintain maternal serum-free thyroxine [fT4] around the upper normal limit with PTU in the first trimester or PTU/MMI in the second and third trimesters). After weighing the pros and cons of ATD treatment, 14 patients chose to restart PTU and 6 patients chose surveillance. Thyroid function and autoantibodies were tested once every two weeks until thyroid function returned to normal and were tested monthly thereafter during the follow-up.
All patients were followed up until the end of pregnancy. Pregnancy and offspring outcomes were collected from outpatient clinical follow-up records and inpatient delivery and birth records, including date of delivery, delivery mode, maternal perinatal outcomes and neonatal outcomes.
Ethics
Informed consent was obtained from each patient after full explanation of the purpose and nature of the study. The study was approved by the Medical Ethics Committee of China Medical University ([2012]2011-32-4) and was congruent with the Declaration of Helsinki.
Serum assays
The concentrations of serum thyrotropin (TSH), free triiodothyronine (fT3), fT4, thyroid peroxidase antibody (TPOAb), and thyroglobulin antibody (TgAb) were measured in all blood samples using the ARCHITECT i2000SR (Abbott Diagnostics, Abbott Park, IL). TSH receptor antibody (TRAb or thyrotropin binding inhibiting immunoglobulins) was analyzed using an electrochemiluminescence immunoassay on a Cobas 601 analyzer (Roche Diagnostics, Switzerland). The intra- and interassay coefficients of variation for these serum parameters were <8.0%.
Since thyroid function during pregnancy does not change significantly until the seventh week of gestation (13), reference ranges provided by the assay manufacturer for general population were used at the time of ATD withdrawal (TSH 0.35–4.94 mIU/L, fT3 2.63–5.70 pmol/L, fT4 9.01–19.05 pmol/L, TPOAb ≤5.61 IU/mL, TgAb ≤4.11 IU/mL, and TRAb ≤1.75 IU/L). Subnormal TSH was defined as <0.35 mIU/L. Pregnancy-specific reference ranges of TSH, fT3 and fT4 were used during the subsequent follow-up. These reference ranges were established in pregnant Chinese women (Supplementary Table S1) (14).
Well-controlled hyperthyroidism during pregnancy was defined as normal fT3 and fT4, with normal or subnormal TSH. Rebound of Graves' hyperthyroidism was defined as subnormal TSH with elevated fT4 and/or fT3. Positive TRAb, TPOAb, and TgAb were defined as the antibody concentrations greater than 1.75 IU/L, 5.61 IU/mL, and 4.11 IU/mL.
Statistical analysis
Quantitative data were expressed as the means (±standard deviation). Data for TSH, TPOAb, and TgAb are expressed as median and 2.5th–97.5th percentiles. The data were tested for normality using the Kolmogorov–Smirnov test. Student's t-test and analysis of variance were used for the analysis of quantitative data. The chi-squared test and Fisher's exact test were used for the analysis of categorical data presented as counts and percentages.
Univariate analysis of age, course of ATD (the duration of ATD treatment before pregnancy), miscarriage history, family history of autoimmune thyroid diseases, dose of ATDs at the time of drug withdrawal, and serum levels of TSH, fT4, fT3, TgAb, TPOAb, and TRAb at the time of ATD withdrawal were performed. A p-value of <0.05 was considered statistically significant. All data were analyzed using the SPSS statistical software package v17.0 (Chicago, IL).
Results
General information
Sixty-three patients with well-controlled Graves' hyperthyroidism who withdrew from ATD treatment within six weeks of pregnancy were included in this study. The average age of the patients was 27.76 ± 3.74 years. Twenty-eight patients were multigravida, of whom 22 patients had a history of miscarriage. Seventeen patients had a family history of autoimmune thyroid diseases (Table 1). The thyroid function and autoantibodies levels of pregnant women are listed in Table 2. Twenty patients experienced hyperthyroidism rebound during pregnancy (31.7%), and of these, 10 patients experienced rebound between 6 and 10 weeks of pregnancy, 5 patients between 11 and 12 weeks, and 5 patients between 13 and 20 weeks. Among these 20 patients, 6 opted for observation without ATD, while 14 (22.2% of the total) restarted PTU treatment at the time of rebound (Fig. 2).

Follow-up outcomes of the patients and offsprings. ATD, antithyroid drug; GD, Graves' disease; GDM, gestational diabetes mellitus; GW, gestational weeks.
General Characteristics of Pregnant Women in the Rebound Group and Nonrebound Group
ATD course: the duration of ATD treatment before pregnancy.
AITD, autoimmune thyroid diseases; ATD, antithyroid drug.
Thyroid Function and Autoantibody Levels of Pregnant Women in the Rebound Group and Nonrebound Group
Subnormal TSH: TSH <0.35 mIU/L.
Baseline: Thyroid function and autoantibodies at the time of ATD withdrawal.
Rebound group vs. nonrebound group a p < 0.01, b p < 0.05.
Data for TSH, TPOAb, and TgAb were expressed as median and 2.5th–97.5th percentiles, since they failed the normality test.
Data of some patients were missing: c n = 18, d n = 19,e n = 19, f n = 42, g n = 40, h n = 41, i n = 41.
fT3, free triiodothyronine; fT4, free thyroxine; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TRAb, thyrotropin receptor antibodies; TSH, thyrotropin.
Rebound-related factors of Graves' hyperthyroidism in pregnancy
Univariate analysis showed that patients with subnormal TSH levels had a higher risk of rebound than those with normal TSH levels (p = 0.029, odds ratio [OR] = 5.12, confidence interval [CI = 1.29–20.34]). In addition, patients with positive TRAb had a higher risk of rebound after ATD withdrawal than those with negative TRAb (p = 0.022, OR = 3.79, [CI = 1.17–12.30]).
In the combined analysis, the patients were stratified according to TRAb positivity and TSH levels. The rebound rate of patients with positive TRAb and subnormal TSH serum levels was significantly higher than that of patients with negative TRAb and normal TSH (83.3% vs. 13.0%, OR = 33.33, [CI = 2.83–392.60], p = 0.003). Most of the patients (87%, 20/23) who were euthyroid with negative TRAb did not experience rebound, and 64.3% (18/28) of euthyroid patients with positive TRAb also did not experience rebound (Supplementary Table S2).
Adverse outcomes of pregnancy and offspring
In the subgroup of 20 patients who experienced hyperthyroidism rebound, 11 patients developed adverse pregnancy outcomes (miscarriage, premature birth, induced labor, gestational hypertension, and gestational diabetes). In the subgroup of 43 patients who did not experience rebound, 4 patients developed adverse pregnancy outcomes (miscarriage, premature birth, and gestational hypertension) (Fig. 2). The risk of adverse pregnancy outcomes in the rebound group was significantly higher than that in the nonrebound group (55.0% vs. 9.3%, OR = 11.92, [CI = 3.08–46.18], p = 0.0002).
In this study, the prevalence rate of neonatal abnormalities was 20.0% (4/20) in the subgroup of patients experiencing hyperthyroidism rebound and 4.7% (2/43) in the subgroup of patients who did not experience rebound (Fig. 2). There were no differences in adverse offspring outcomes between the two groups (p = 0.08).
Discussion
Uncontrolled hyperthyroidism during pregnancy adversely affects both the mother and the infant (3,15). It is recommended that thyroid function be controlled in women of childbearing age before pregnancy; however, the implementation is not always feasible. Considering the potential teratogenic effects of ATDs, the ATA clinical practice guideline suggests that “women with a stable euthyroid state on 5–10 mg MMI per day achieved within a few months, and a falling TRAb level, are likely candidates to withdraw from ATD therapy in early pregnancy” (11). However, there has been little evidence in the pregnant population to directly support this suggestion, which was surmised based on data from nonpregnant patients.
In this prospective study, 63 pregnant women with Graves' hyperthyroidism discontinued their ATD treatment during early pregnancy according to recommendations by the ATA and ETA. We observed changes in thyroid function of these patients. The results showed that two-thirds of the patients could maintain stable euthyroid status, and the cumulative rebound rate of hyperthyroidism was 31.7%. Half of the patients experienced hyperthyroidism rebound >4 weeks after ATD withdrawal (i.e., after 10 weeks gestational age), which seemed to have circumvented the most sensitive period of teratogenesis between 6 and 10 weeks of pregnancy (9).
We identified subnormal TSH and TRAb positivity as risk factors associated with rebound of hyperthyroidism after ATD withdrawal in early pregnancy. In our study, hyperthyroidism rebound occurred in 83.3% of patients with both subnormal TSH and positive TRAb, whereas occurred only in 13.0% of patients with normal TSH and negative TRAb. The TSH level after ATD withdrawal is also a predictor of GD relapse in nonpregnant patients (16 –18). A prospective study of 128 patients with recurrent GD who restarted ATDs showed that patients with low-normal TSH at the time of ATD withdrawal had a significantly lower remission rate than the patients with relatively high TSH levels (18).
In nonpregnant GD patients, TRAb should be tested before deciding whether ATDs can be stopped. The third-generation TRAb test is a good predictor of hyperthyroidism recurrence after a course of ATDs (19 –21). Carella et al. reported that TRAb positivity was associated with risk of the relapse of hyperthyroidism within 8 weeks of ATD withdrawal, and the positive predictive value was 97% (21). However, little is known about whether TRAb positivity is also predictive in pregnant GD patients. This study suggested that TRAb positivity at the time of ATD withdrawal may be a prognostic factor for increased risk of Graves' hyperthyroidism rebound during pregnancy.
Finally, we found that GD rebound was associated with increased risk of adverse pregnancy outcomes. Yet it is known that poor control of hyperthyroidism during pregnancy is associated with multiple pregnancy complications, such as miscarriage, premature delivery, and gestational diabetes mellitus (GDM), among other issues (3,22). In contrast, in this study, the overall risk of neonatal abnormalities in the rebound group was not different from that in the nonrebound group. However, larger prospective studies are required to conclude whether ATD withdrawal affects fetal outcome.
The main limitation of our study is the small sample size from a single center. Hence, a larger prospective study is needed to overcome the potential selection bias and to verify the conclusions of this study. Second, our conclusions are drawn from a Chinese cohort. We anticipate further studies on ATD withdrawal in early pregnancy in patients with hyperthyroidism being performed in different ethnic groups.
Conclusion
Our study found that 20 of 23 (87%) of pregnant women who were euthyroid and had negative TRAb at the time of ATD withdrawal, and 18 of 28 (64%) of pregnant women who were euthyroid and had positive TRAb at the time of ATD withdrawal, did not develop rebound of Graves' hyperthyroidism, supporting the current ATA clinical practice recommendation. The risk of rebound was observed to be increased in women with subnormal TSH and/or positive TRAb who had stopped ATDs in early pregnancy. The risk of perinatal complications was significantly increased in the GD rebound patients. Clinicians should discuss the pros and cons of ATD withdrawal early in pregnancy, especially with pregnant women with subnormal TSH and/or positive TRAb.
Footnotes
Authors' Contributions
All the authors contributed to the study design or concept, the analysis and interpretation of the data. All the authors critically reviewed and edited the article. All the authors approved the final version and were responsible for the decision to submit the article.
Acknowledgments
The authors are grateful to all of the patients, as well as the physicians who referred the patients and verified the diagnosis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the National Natural Science Foundation of China (81970682, 81570709, and 81700697), the National Key Research and Development Program of China (2017YFC0907403), the Health and Medicine Research Foundation in Shenyang City (17-230-9-02), and the Central Government-Guided Local Special Funds for Scientific and Technological Development (2019416021).
Supplementary Material
Supplementary Table S1
Supplementary Table S2