
Abstract
Background:
Given the paucity of epidemiological studies on thyroid storm, we aimed to estimate the incidence rate and case fatality of thyroid storm in Germany based on a large claims database.
Methods:
Using the German Pharmacoepidemiological Research Database (GePaRD) we identified patients with at least one inpatient discharge diagnosis of thyroid storm (International Statistical Classification of Diseases and Related Health Problems, 10th revision, German modification; ICD-10-GM E05.5) between 2007 and 2017 and calculated age-standardized and age-specific incidence rates in males and females (no age restriction). We defined deaths occurring within 30 days of the diagnosis as thyroid storm-associated and determined case fatality by sex and age group. Point estimates were reported with confidence intervals [CIs].
Results:
We identified 1690 patients with an incident diagnosis of thyroid storm. Of these, 72% were females (n = 1212). The mean age was 60 years (standard deviation: 18.6 years). The age-standardized incidence rate per 100,000 persons per year was 1.4 [CI 1.2–1.7] in females and 0.7 [CI 0.5–0.9] in males. In females ≤60 and >60 years of age, the incidence rate was 0.9 [CI 0.9–1.0] (males: 0.4 [CI 0.3–0.4]) and 2.7 [CI 2.5–2.9] (males: 1.7 [CI 1.5–1.9]), respectively. The case fatality of thyroid storm was 1.4% [CI 0.6–2.8] in females ≤60 years and 10.9% [CI 8.6–13.7] in females >60 years. In males, the case fatality was 1.0% [CI 0.2–4.0] in those aged ≤60 years and 16.7% [CI 12.6–21.7] in those >60 years.
Conclusions:
Incidence rates of thyroid storm were markedly higher in females than in males and were three times higher in persons >60 years compared with younger age groups. The case fatality was below 2% in persons aged ≤60 years and markedly higher in older persons (males: 17 times and females: 8 times).
Background
Thyroid storm is a rare and life-threatening condition characterized by an acute exacerbation of thyrotoxicosis (elevated free triiodothyronine or free thyroxine and suppressed thyrotropin) with severe clinical symptoms. It often results in multiorgan failure involving one or more organ systems such as the central nervous, cardiac, hepatic, pulmonary, respiratory, digestive, and gastrointestinal excretory systems. The diagnosis is based on clinical signs using scoring classifications suggested by Burch and Wartofsky 1 or by the Japan Thyroid Association. 2 Surgeries, infections, trauma, amiodarone use, and acute iodine exposures (by radiocontrast agents) have been identified as the most common potential triggers of thyroid storm in a hospital setting. 3,4 The underlying conditions causing thyroid storm include Graves' disease, toxic multinodular goiter, and solitary toxic adenoma. 5,6
Globally, only three studies have reported on the epidemiology of thyroid storm using population-based databases. The incidence rate of thyroid storm has been estimated to range from 0.20 to 0.76 per 100,000 persons per year. 2,7,8 Females have been reported to be more susceptible to this condition (female-to-male ratio: 3:1), as were individuals >40 years of age. 8 Four studies have provided estimates for the case fatality of thyroid storm. These estimates, which were mostly based on small sample sizes, varied between 8% (2 out of 25 patients), 9 10% (134 out of 1324 patients), 10 11% (38 out of 356 patients), 2 and 25% (7 out of 28 patients). 11
In Germany, the current knowledge on the incidence and case fatality of thyroid storm is limited to the results of a questionnaire-based retrospective multicenter study conducted in 1992. 12 However, interpretation of this study is difficult as neither the underlying method is clearly described nor it is clear whether the study population was representative for Germany. Apart from this, only case studies published between 1970 and 1989 are available from Germany. 13 –15 Given the general lack of descriptive epidemiological studies on thyroid storm, we aimed to estimate the incidence rate and case fatality of thyroid storm using data from a large German claims database.
Materials and Methods
Data source
We used the German Pharmacoepidemiological Research Database (GePaRD), which contains claims data from four statutory health insurance providers in Germany. 16 This database includes ∼25 million persons who have been insured with one of the four health insurance providers since 2004 or later. 17 GePaRD covers ∼20% of the general German population and it includes persons from all the geographical regions of Germany. Diagnoses in GePaRD are coded according to the International Statistical Classification of Diseases and Related Health Problems, 10th revision, German Modification (ICD-10 GM). For this study, we used data from the years 2007 to 2017.
The use of GePaRD data for this study was approved by all four health insurance providers as well as the German Federal Office for Social Security and the Senator for Health, Women and Consumer Protection in Bremen as their responsible authorities. Informed consent for studies based on claims data is required by law unless obtaining consent appears unacceptable and would bias results, which was the case in this study. According to the Ethics Committee of the University of Bremen, studies based on GePaRD are exempt from institutional board review. The study was performed according to the institutional guidelines of the Leibniz Institute for Prevention Research and Epidemiology—BIPS. All data were analyzed anonymously and the authors did not have access to identifying information.
Around 90% of the general population in Germany is covered by statutory health insurances. 18 The main characteristics of the German health insurance system are uniform access to all levels of care and free choice of providers. It has been shown that the data in GePaRD are representative of the German population regarding drug prescriptions, hospital admissions, and hospital diagnoses. 19,20
Study population and study design
To identify cases with incident thyroid storm, we considered all patients (irrespective of age) with at least one inpatient diagnosis code (main or secondary hospital discharge diagnosis) of thyroid storm (ICD-10 GM E05.5) within the study period (2007–2017). The admission date of the hospital stay for which “thyroid storm” has been coded as discharge diagnosis was assigned as the index date (i.e., date of first diagnosis). We excluded patients with missing information on sex or gender diverse, age, and those who do not live in Germany. Furthermore, we excluded patients who were not continuously insured for at least one year before the index date. We used this exclusion criterion because shorter preobservation periods would not allow to assess whether patients were newly diagnosed or still under treatment for a former diagnosis of thyroid storm.
Patients were followed until end of the study period (i.e., December 31, 2017), end of the insurance period, or death, whichever occurred first. We also determined whether patients had more than one inpatient diagnosis of thyroid storm during the study period. Patients dying within 30 days following an inpatient diagnosis of thyroid storm were defined as cases of death associated with thyroid storm. In sensitivity analyses, the maximum permissible time period from the date of diagnosis to the date of death was varied (15 days, 45 days).
To determine the incidence rate of thyroid storm for each calendar year between 2007 and 2017, a denominator was required as well. For the denominator, we included all individuals represented in GePaRD in the respective calendar year, excluding those with missing information on sex or gender diverse, age, and those who do not live in Germany as well as those with continuous insurance of less than one year before the first day they were insured in the respective calendar year.
Data analysis
We stratified the patients with thyroid storm by sex and described them regarding age at index date, type of admission, and the number of inpatient diagnoses of thyroid storm during the study period. Type of admission is an information recorded by hospitals that distinguishes between admission for “usual care” versus admission for “emergency care” versus “others.” Analogously, we described the cases of death associated with thyroid storm.
In addition, we assessed relevant comorbidities coded in the year before the incident diagnosis of thyroid storm for all patients with thyroid storm and additionally for the subgroup of patients dying within 30 days after the diagnosis. The comorbidities were defined based on algorithms that combine information from diagnoses codes, procedures, and drug dispensations. 21 We also examined concurrent diagnoses, that is, discharge diagnoses of the hospital stay coded in addition to thyroid storm.
We calculated incidence rates stratified by sex and age group for each calendar year between 2007 and 2017, using the number of incident cases with thyroid storm of the respective calendar year as the numerator and the number of persons in GePaRD (see the Study Population and Study Design section) as the denominator. To calculate the overall incidence rates for the whole study period (2007–2017), we summed up the numerators and the denominators of each calendar year. We determined both crude and age-standardized incidence rates per 100,000 persons per year with corresponding confidence intervals [CIs] based on exact Poisson confidence limits. Age-standardized incidence rates were calculated using the age distribution of the German population in 2017 as standard. 22
We also calculated the case fatality of thyroid storm for each calendar year by considering the number of thyroid storm-associated deaths in the respective calendar year as the numerator and the total number of patients with a thyroid storm diagnosis (only incident diagnosis) identified in the same calendar year as the denominator. The corresponding CIs were calculated based on the Wilson score method. 23
We performed all analyses using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA). 24
Results
Patient characteristics
We identified 1690 patients with an incident diagnosis of thyroid storm during the study period. Two patients were excluded due to missing information on sex or gender diverse, five patients because they did not live in Germany, and 83 patients were excluded because they were not continuously insured for at least one year before the index date (Supplementary Fig. S1). As shown in Table 1, the mean age was 60 years (standard deviation [SD]: 18.6 years) and 77% (1310/1690) of patients were ≥46 years of age. The female-to-male ratio in the age groups <18, 18–30, 31–45, 46–60, 61–70, 71–80, and >80 years was 2.8, 4.2, 3.7, 2.5, 2.1, 1.9, and 2.9, respectively. In about 38% (635/1690) of patients, the type of admission to the hospital was coded as “usual care.”
Characteristics of Patients with an Incident Diagnosis of Thyroid Storm During the Study Period 2007–2017
IQR, interquartile range; SD, standard deviation.
In 6.7% (114/1690) of patients, there was more than one inpatient diagnosis of thyroid storm during the study period. The characteristics of these patients were similar to those of the overall group of thyroid storm patients (see Supplementary Table S1). The median time between the first and second inpatient diagnosis of thyroid storm was 25 days, with an interquartile range from 8 to 57.
As shown in Table 2, there were 125 cases of death associated with thyroid storm. The mean age at death was 77 years (SD: 11.7 years) and 92% of the deceased patients were >60 years. In a sensitivity analysis using a maximum permissible time period of 14 days (instead of 30 days) between the date of diagnosis and the date of death, the number of cases decreased to 87. The number of cases increased to 166 when a time period of 45 days was used (see Tables 6 –8).
Characteristics of Cases of Death a Associated with Thyroid Storm
Death within 30 days of a diagnosis of thyroid storm was considered to be associated with thyroid storm.
As shown in Table 3, 66% (1123/1690) of all thyroid storm patients and 87% (109/125) of those who died had any of the selected comorbidities. A total of 48% (805/1690) of all patients had any medical treatment for cardiovascular disease. Other common comorbidities were medically treated diabetes (12% of all patients [201/1690]) and obesity (14% of all patients [228/1690]). Graves' disease was coded in 4% (67/1690) of all patients. Most comorbidities were more common in the subgroup who died compared with all patients. For example, prevalence in those who died was more than twice as high compared with all patients for several cardiovascular comorbidities such as acute myocardial infarction (5% [6/125] vs. 2% [38/1690]), dementia (13% [16/125] vs. 5% [83/1690]), and chronic obstructive pulmonary disease (15% [19/125] vs. 7% [119/1690]).
Comorbidities Recorded One Year Before Diagnosis of Thyroid Storm in All Patients with Incident Thyroid Storm and in Those with Thyroid Storm-Associated Death
The number of patients (% of group total) is shown for each category.
Death within 30 days of a diagnosis of thyroid storm was considered to be associated with thyroid storm.
With regard to hospital discharge diagnoses coded in addition to the thyroid storm diagnosis, 41% (688/1690) of all patients and 65% (81/125) of those who died had a code for atrial fibrillation and flutter. Heart failure was coded in 27% (456/1690) of all patients and in 57% (72/125) of those who died. Most other conditions were also coded more often in those who died (Table 4). For the results presented in Tables 3 and 4, a stratification by sex is provided in Supplementary Tables S2 and S3 and a restriction to patients older than 60 years is provided in Supplementary Tables S4 and S5.
Hospital Discharge Diagnoses Coded in Addition to Thyroid Storm Diagnosis
The no. of patients (% of group total) is shown for each category.
Death within 30 days of a diagnosis of thyroid storm was considered to be associated with thyroid storm.
Incidence rates of thyroid storm
The overall age-standardized incidence rate of thyroid storm was 1.1 [CI 0.9–1.3] per 100,000 persons per year. In females and males, the age-standardized incidence rate was 1.4 [CI 1.2–1.7] and 0.7 [CI 0.5–0.9] per 100,000 persons per year, respectively. Stratification of the age-standardized incidence rates by calendar year showed little variation over time from 2010 to 2017, with overlapping CIs across the calendar years (Fig. 1). Age-standardized and crude incidence rates were almost identical (see Supplementary Fig. S2). As shown in Table 5, the incidence rate (per 100,000 persons per year) increased with age. It was lowest in patients aged <18 years (females: 0.1 [CI 0.1–0.2], males: 0.04 [CI 0.01–0.1]) and highest in those aged >80 years (females: 4.0 [CI 3.4–4.7), males: 2.6 [CI 1.9–3.4]).
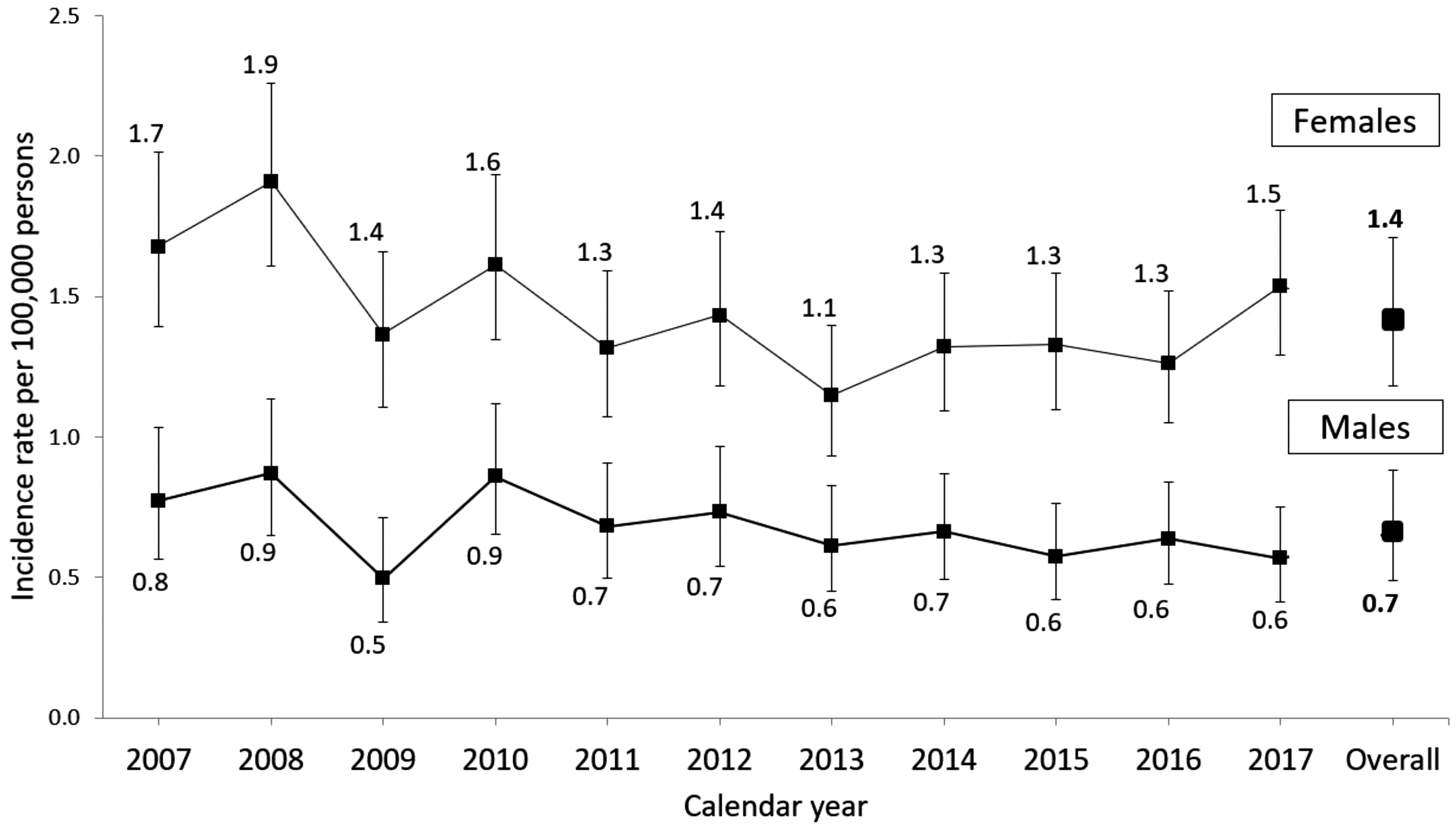
Annual age-standardized incidence rates of thyroid storm stratified by sex.
Incidence Rates (per 100,000 Persons per Year) of Thyroid Storm, Overall and Stratified by Age Group and Sex
Case fatality of thyroid storm
As shown in Table 6, case fatality of thyroid storm varied by sex (lower in females than in males) and was higher in older than in younger age groups. The overall case fatality was 6.3% [CI 5.0–7.8] in females and 10.3% [CI 7.8–13.3] in males. In females, it ranged between 1.7% and 24.3% across age groups; in males, it ranged between 0.9% and 31.0%. Both males and females >80 years of age showed the highest case fatality.
Case Fatality of Thyroid Storm, Overall and Stratified by Age Group and Sex: Maximum Permissible Time Period of 30 Days (Base Case Analysis)
A similar pattern by age and sex was observed in sensitivity analyses using different time periods for the definition of thyroid storm-associated deaths (15 days and 45 days; see Tables 7 and 8). The overall case fatality increased was 7.8% [CI 6.5–9.5] in females and 14.9% [CI 11.9–18.3] in males when the maximum permissible time period was extended from 30 to 45 days. Figure 2 shows case fatality in men and women stratified by calendar year between 2007 and 2017, with largely overlapping CIs across years.
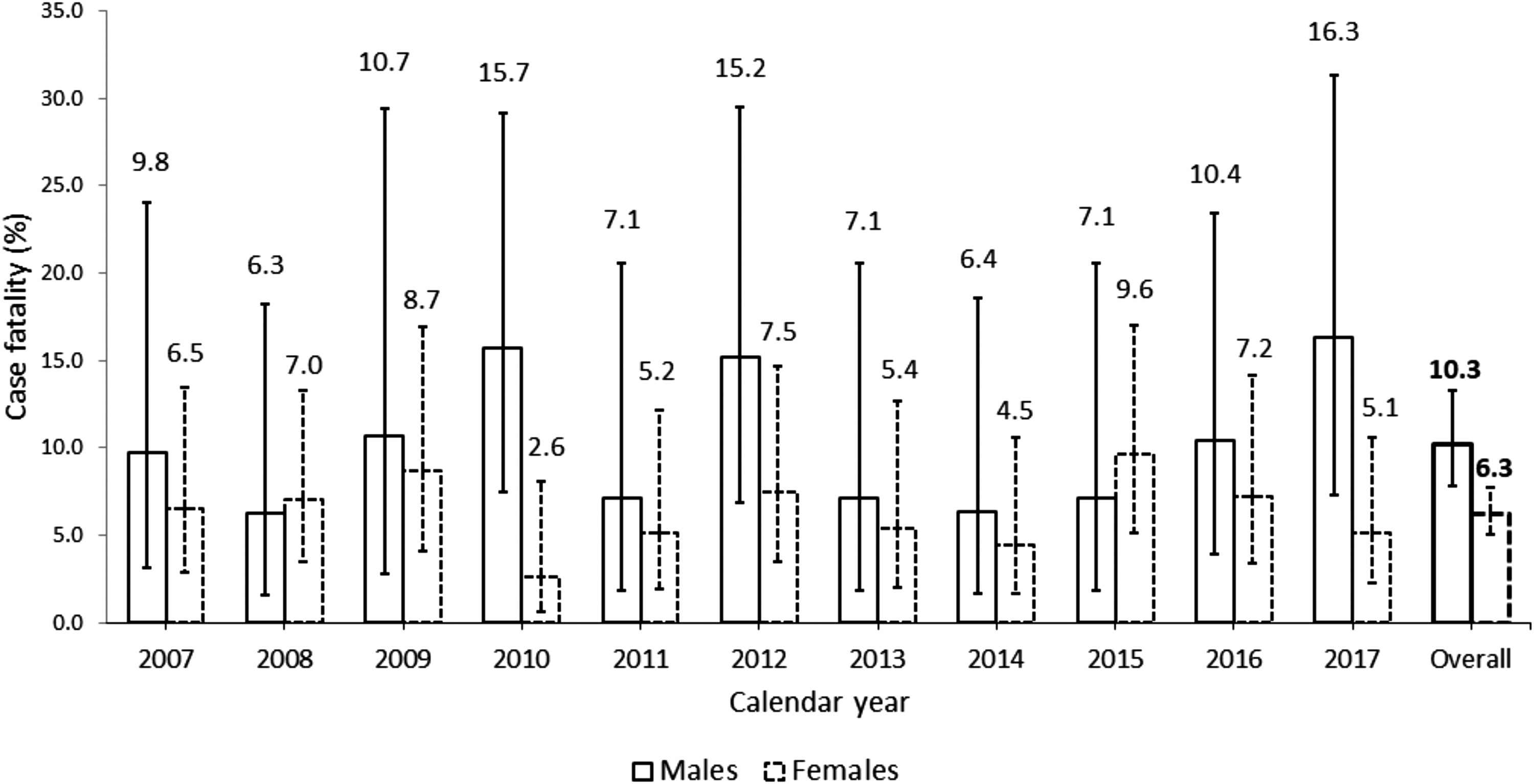
Annual case fatality of thyroid storm stratified by sex.
Case Fatality of Thyroid Storm, Overall and Stratified by Age Group and Sex: Maximum Permissible Time Period of 15 Days (Sensitivity Analysis)
Case Fatality of Thyroid Storm, Overall and Stratified by Age Group and Sex: Maximum Permissible Time Period of 45 Days (Sensitivity Analysis)
Discussion
To the best of our knowledge, this is the first study reporting population-based data on incidence and case fatality of thyroid storm in Germany. Our findings suggest that every year there was about one case of thyroid storm per 100,000 persons in Germany during the study period (2007–2017). However, incidence strongly varies with age and sex. In our study, the age-standardized incidence rate of thyroid storm was two times higher in females than in males (1.4 vs. 0.7 per 100,000 persons per year) and it was three times higher in persons >60 years compared with younger individuals. For example, in females >60 years of age, the incidence rate was 3 per 100,000 persons per year. Also, case fatality of thyroid storm strongly varied with age and sex. While it was below 2% in persons aged ≤60 years, it was 17% in males and 11% in females >60 years of age.
Our finding that the age-standardized incidence rate of thyroid storm in females was twice as high as in males is consistent with other population-based studies conducted in Japan, Taiwan, and the United States. 2,7,8 In these studies, about two-thirds to three-quarters of all cases with thyroid storm occurred in females. This is consistent with the fact that also certain risk factors of thyroid storm are more common in females. For example, for Graves' disease, a female-to-male ratio of 5:1 has been reported. 25 The overall incidence rate observed in our study (1 per 100,000 persons per year) was higher than in the abovementioned studies. For Japan, an incidence rate of 0.2 cases per 100,000 persons per year was reported based on data from 2004 to 2008. 2 In the study from Taiwan using data from 2005 to 2014, an incidence rate of 0.6 cases per 100,000 persons per year was estimated. 7
In the study from the United States, the incidence rate varied from 0.6 to 0.8 per 100,000 persons per year over the 10-year study period (2004–2013). 8 A higher incidence of thyroid storm in Germany may be plausible given that Germany used to be a region with mild-to-moderate iodine deficiency. Accordingly, Germany used to have a high prevalence of thyroid disorders that increase the risk of thyroid storm. 26 Even though the iodine fortification program implemented in 1993 has substantially improved the iodine status in Germany, 27 it may still differ from the status in countries such as Japan or Taiwan. 28 However, caution is needed for the interpretation of between-country differences since they could also result from different data sources and coding practices.
In our study, case fatality of thyroid storm strongly varied with age. A study from Japan investigating factors associated with death from thyroid storm also reported a seven times higher risk of death among patients with thyroid storm aged 60–79 and a 12 times higher risk among those aged ≥80 years compared with patients >20 years of age. 10 A higher risk of death was reported for patients developing cardiovascular complications 29 and also for those with cardiovascular comorbidities. 7,10 We observed that concomitant cardiovascular events and cardiovascular comorbidities as well as other comorbidities were markedly more common in patients >60 years than in all patients, which may explain the higher case fatality. The study from Japan also reported a higher risk of death among male compared with female patients even though this difference was not statistically significant. 10
In our study, we observed a higher case fatality in older males than in older females. Given that other studies did not report the absolute values of case fatality stratified by age and sex, a direct comparison with our findings is not possible. Furthermore, the absolute value depends on the definition of case fatality. In our base case analysis, we defined patients dying within 30 days following an inpatient diagnosis of thyroid storm as cases of death associated with thyroid storm. Our sensitivity analyses illustrated that case fatality gradually increased when the permissible time period between the date of diagnosis and the date of death was extended. In agreement with this, a study from Taiwan also found an increase in case fatality when this time period was increased from 14 to 90 days. 7
Considering the severe complications and potential fatality of thyroid storm, the extent to which and how it is preventable is a key question. Regarding underlying conditions, most patients with thyroid storm present either a subclinical hyperthyroidism or irregular use of antithyroid drugs with previously diagnosed hyperthyroidism. 2,30,31 With respect to subclinical hyperthyroidism, patient screening for thyroid disorders before major medical procedures, particularly in those >60 years of age, could play a significant role in preventing thyroid storm. This would be particularly relevant in regions with former or current iodine deficiency. For patients with previously diagnosed hyperthyroidism stopping treatment with antithyroid drugs, the European Thyroid Association recommends regular follow-up including medical examination and thyroid function tests. 32 This would be beneficial in controlling the blood thyroid level and lower the risk of developing thyroid storm in these patients. 32
In 38% of patients with thyroid storm in our study, the type of admission was coded as “inpatient, usual care.” If coding is correct, this would imply that these patients likely developed thyroid storm after their admission to the hospital. Thyroid storm in these patients may have been potentially preventable if a screening for thyroid disorders had occurred in the hospital before exposure to a triggering factor.
Our study has several strengths and limitations. The large claims database allowed us to estimate the population-based incidence and case fatality of this rare condition without nonresponder or recall bias. The almost identical age-standardized and crude incidence rates in our study (see Supplementary Fig. S1) suggests a lack of relevant differences between the age distribution in GePaRD and the German population as a whole. Our study also allowed us to investigate incidence and case fatality of thyroid storm stratified by age and sex, which was insufficiently addressed in previous studies. Furthermore, our database also contains information on other diseases, and so, we could describe comorbidities and concomitant diagnoses in patients with thyroid storm.
There are also limitations to be considered in the interpretation of our results. Our study used health insurance claims data, that is, data collected for reimbursement rather than for research purposes. The quality of such data may not be optimal. This applies especially to diagnoses coded in the outpatient setting as medical records and laboratory parameters for confirmation of thyroid storm diagnoses based on diagnostic criteria (i.e., Burch and Wartofsky Score 1 or score from the Japan Thyroid Association 2 ) are not available in GePaRD. In our study, however, we only considered hospital discharge diagnoses, which are considered to have a very high validity due to strict coding guidelines and regular audits. To describe comorbidities, we used algorithms combining different types of information to maximize the validity of definitions.
We could not describe the treatment during thyroid storm because GePaRD does not contain information on medications dispensed in the hospital (except for certain very expensive drugs that are not relevant for the treatment of thyroid storm). While our study focused on describing population-based incidence and case fatality of thyroid storm in Germany, it will also be interesting to investigate risk factors of thyroid storm in future analyses using a study design that is appropriate for this research question. Also, exploring factors that may explain the observed differences in case fatality between males and females in future studies would be of value.
In conclusion, our study found incidence rates of thyroid storm to be markedly higher in females than in males and three times higher in persons >60 years compared with younger age groups. Case fatality was below 2% in persons aged ≤60 years and markedly higher in older persons (males: 17 times and females: 8 times).
Footnotes
Acknowledgments
The authors would like to thank all the statutory health insurance providers who provided data for this study, namely AOK Bremen/Bremerhaven, DAK-Gesundheit, Die Techniker (TK), and hkk Krankenkasse. The authors would also like to thank Sarina Schwarz for double programming the study results and Anja Gabbert, Alina Ludewig, Inga Schaffer, and Jost Viebrock for statistical programming of the data sets.
Authors' Contributions
A.T.: conception and design of the research; formal analysis; and writing—original draft. K.P.: conception and design of the research; and writing—review and editing. T.I.: writing—review and editing. H.V.: writing—review and editing. U.H.: conception and design of the research; review and editing; and supervision. All authors have read and approved the article.
Author Disclosure Statement
A.T., K.P., and U.H. are working at an independent, nonprofit research institute, the Leibniz Institute for Prevention Research and Epidemiology—BIPS. Unrelated to this study, BIPS occasionally conducts studies financed by the pharmaceutical industry. Almost exclusively, these are postauthorization safety studies (PASS) requested by the health authorities. The design and conduct of these studies as well as the interpretation and publication are not influenced by the pharmaceutical industry. The study presented was not funded by the pharmaceutical industry and was performed in line with the ENCePP Code of Conduct. T.I. and H.V. have no conflict of interest to disclose.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5