
Abstract
Background:
The safety of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines is widely appreciated. However, there is limited knowledge regarding the potential impact of SARS-CoV-2 vaccines on the thyroid.
Methods:
We performed two prospective clinical trials between April and June, 2021, enrolling recipients of the inactivated SARS-CoV-2 vaccine (BBIBP-CorV and CoronaVac). Thyroid function, antithyroid antibody levels, and SARS-CoV-2 neutralizing antibody levels were detected for each participant before receiving the first vaccine dose and 28 days after receiving the second vaccine dose.
Results:
A total of 657 recipients participated in the study. The overall median thyroid function and levels of antithyroid antibodies before and after SARS-CoV-2 vaccination were within the normal range. Among the 564 participants with normal thyroid function at baseline, 36 (6.38% [confidence interval; CI 4.51–8.73]) developed thyroid dysfunction. Of the 545 recipients with negative antithyroid antibodies at baseline, none developed abnormal antibodies after vaccination. Notably, 75.27% (70/93 [CI 65.24–83.63]) of the 93 recipients with thyroid dysfunction returned to normal function after vaccination. The levels of antithyroid peroxidase antibody (96.20% [CI 89.30–99.21]) and antithyroglobulin antibody (TgAb; 88.31% [CI 78.97–94.51]) remained positive after vaccination in most patients with abnormal values at baseline. However, the TgAb levels in more than half of the patients (48/77) decreased. All of 11 abnormal thyrotropin receptor antibody levels at baseline decreased postvaccination.
Conclusions:
Vaccination with an inactivated SARS-CoV-2 vaccine had no significant adverse impact on thyroid function or antithyroid antibodies within the first 28 days after the second dose.
Clinical Trial Registration:
ChiCTR2100045109 and ChiCTR2100042222.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused the ongoing coronavirus disease 2019 (COVID-19) global pandemic. Currently, >500 million people worldwide suffer from SARS-CoV-2 because of the highly contagious nature of the virus. 1 Vaccination has become one of the most important public health strategies against COVID-19.
Vaccines against COVID-19 have been urgently developed and their safety has been widely accepted. Common vaccination side effects include mild fever, fatigue, headache, muscle pain, diarrhea, and pain at the injection site.2–4 Currently, there is limited knowledge regarding the impact of SARS-CoV-2 vaccines on the thyroid. A few studies have reported thyroid diseases after SARS-CoV-2 vaccination, such as thyroiditis, 5 –10 hyperthyroidism, 11 –13 and central hypothyroidism. 14
However, there is limited knowledge regarding thyroid function and autoimmune antibody levels before and after SARS-CoV-2 vaccination. Because of the widespread use of vaccines, examining the potential influence of vaccines on thyroid function and autoimmunity is essential, particularly in those with thyroid disorders. In addition, it is important to examine whether thyroid function and autoimmune antibody levels affect vaccine efficacy.
Utilizing data from our randomized controlled trial and prospective cohort study, we aimed to evaluate thyroid function and antithyroid antibodies before and after vaccination with an inactivated SARS-CoV-2 vaccine, and their effect on the levels of SARS-CoV-2 neutralizing antibodies (NAbs).
Materials and Methods
Design and participants
We performed a randomized controlled trial between April 15 and April 28, 2021, and a prospective cohort study between May 8 and June 30, 2021, in the First Affiliated Hospital of Sun Yat-sen University. This study is a secondary analysis of clinical trial data from the mentioned two studies. The randomized controlled trial aimed at investigating the potential impact of SARS-CoV-2 vaccine delivery timing on immune response, and there was no significant difference in the baseline characteristics, thyroid function, and antithyroid antibodies between morning and afternoon groups in the randomized controlled trial. Therefore, the randomization grouping was not relevant to the secondary analysis of the data. The eligibility and exclusion criteria for the two studies were similar. Adults aged 18–59 years were enrolled in the study.
Exclusion criteria were as follows: (1) allergy history to any component of a vaccine or a history of severe allergic reaction to a vaccine; (2) fever, acute disease, severe chronic disease, or acute phase of any chronic disease; (3) pregnancy, breastfeeding, or planned pregnancy within three months (for women); (4) a history or family history of convulsions, epilepsy, encephalopathy, or mental disorder; or a history of progressive neurological injury or Guillain–Barré syndrome; (5) autoimmune disease, or congenital or acquired immunodeficiency such as HIV infection, lymphoma, or leukemia; (6) severe respiratory disease, severe cardiovascular disease, hepatic or renal disease, or malignant tumor; (7) use of immunosuppressant agents or immunopotentiators; (8) history of SARS-CoV-2 infection; and (9) an unsuitable condition for vaccination per clinician evaluation. The eligibility and exclusion criteria referred to the clinical trials of BBIBP-CorV and CoronaVac.2,3
Both the randomized controlled trial and prospective cohort study were approved by the ethics committee of the First Affiliated Hospital of Sun Yat-sen University (Approval Nos.: 2021008 and 2021254), and registered in the Chinese Clinical Trial Registry. Written informed consent was obtained from all participants for the measurement of thyroid-related blood tests as part of the original research ethics approval.
Data and sample collection
All participants received a 0.5 mL dose of inactivated SARS-CoV-2 vaccine (BBIBP-CorV, Sinopharm, Beijing; or CoronaVac, Sinovac Life Sciences, Beijing) on days 0 and 28 by intramuscular injection into the deltoid muscle. The adjuvant in both vaccines was aluminum hydroxide. An ∼5 mL sample of venous blood was collected from each participant before the first dose and 28 days after the second dose. Before the first vaccination, we used questionnaires to collect the following information: age, sex, marital status, height, weight, daily exercise, and smoking and alcohol consumption.
Measurement of thyroid function and antithyroid antibody levels
Levels of serum-free triiodothyronine (fT3), free thyroxine (fT4), total triiodothyronine (TT3), total thyroxine (TT4), thyrotropin (TSH), antithyroglobulin antibody (TgAb), and antithyroid peroxidase antibody (TPOAb) were determined by chemiluminescent immunoassays (CLIA) using the Beckman Coulter DXI 800 (Beckman Coulter, Brea, CA, USA). Levels of TSH receptor antibody (TRAb) were assessed by electrochemiluminescence immunoassays using a Cobas 6000 analyzer (Roche Diagnostics, Mannheim, Germany).
The intra-assay coefficients of variations (CVs) for serum assays of fT3, fT4, TT3, TT4, TSH, TgAb, TPOAb, and TRAb were 2.6–6.6%, 1.82–4.4%, 3.22–5.22%, 3.16–5.08%, 1.5–3.5%, 3.6–5.7%, 5.1–7.1%, and 0.8–7.5%, respectively. The interassay CVs for serum assays of fT3, fT4, TSH, TgAb, TPOAb, and TRAb were 1.3–8.0%, 3.34–8.08%, 0.2–1.6%, 0–5.2%, 2.2–4.4%, and 1.3–9.1%, respectively. Reference ranges were defined as follows: fT3 3.81–6.91 pmol/L; fT4 7.50–21.10 pmol/L; TT3 0.88–2.44 nmol/L; TT4 78.38–157.40 nmol/L; TSH 0.56–5.91 μIU/mL; TgAb ≤3.99 IU/mL; TPOAb ≤9.00 IU/mL; and TRAb 0.00–1.75 IU/L.
SARS-CoV-2 NAbs measurement
Levels of serum SARS-CoV-2 NAbs were determined by CLIA using the iFlash 2019-nCoV NAb kit (YHLO Biotech Co., Shenzhen, China). In brief, SARS-CoV-2 NAbs are detected by a competitive one-step immunoassay. For this assay, SARS-CoV-2 NAbs are designed to compete with acridinium ester-labeled angiotensin-converting enzyme 2 for binding to the receptor-binding domain of SARS-CoV-2. Luminescence intensities are measured using an iFlash3000 automated CLIA analyzer, and then the levels of SARS-CoV-2 NAbs are calculated according to the manufacturer's instructions (YHLO Biotech Co.). SARS-CoV-2 NAb levels expressed in arbitrary units (AU/mL) are considered positive above 10 AU/mL.
Definitions of clinical diagnoses
According to the guidelines of American Thyroid Association 15,16 and the reference ranges of thyroid function tests in our hospital, the following diagnostic criteria for thyroid dysfunction were used. Overt hyperthyroidism: TSH <0.56 μIU/mL, fT3 > 6.91 pmol/L, or fT4 > 21.10 pmol/L. Subclinical hyperthyroidism: TSH <0.56 μIU/mL, fT4 7.50–21.10 pmol/L, fT3 3.81–6.91 pmol/L. Overt hypothyroidism: TSH >5.91 μIU/mL, fT4 < 7.50 pmol/L. Subclinical hypothyroidism: TSH >5.91 μIU/mL, fT4 7.50–21.10 pmol/L.
“Normal” of thyroid function or antithyroid antibodies was defined as abnormal measured values prevaccination returned to normal within respective reference ranges postvaccination. “Improved” of thyroid function or antithyroid antibodies was defined as abnormal measured values prevaccination did not return to normal postvaccination, but had a smaller difference from respective reference ranges. “Aggravated” of thyroid function or antithyroid antibodies was defined as a larger difference in measured values from respective reference ranges.
Statistical analysis
Quantitative data are presented as means and standard deviation (SD), or median and interquartile range as appropriate; qualitative data are presented as numbers and percentages. The confidence intervals (CIs) of the proportion were calculated using the Clopper–Pearson method. To evaluate whether there was a difference before and after the SARS-CoV-2 vaccination, a paired t-test or paired Wilcoxon test for quantitative variables and McNemar's test for qualitative variables were applied. Spearman correlation was applied to evaluate the association between thyroid function and antithyroid antibody and SARS-CoV-2 NAb levels. Statistical analysis was performed using Stata/MP 14.0. A p-value <0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 503 and 238 participants were initially enrolled in the randomized controlled trial and prospective cohort, respectively. Eighty-four participants were excluded because of insufficient blood samples for the detection of thyroid function and antithyroid antibodies, and the remaining 657 participants formed the basis of the analysis (Fig. 1). The mean age was 32.8 (SD, 9.2) years, and 72.5% (476/657) were female, the other characteristics are summarized in Table 1.
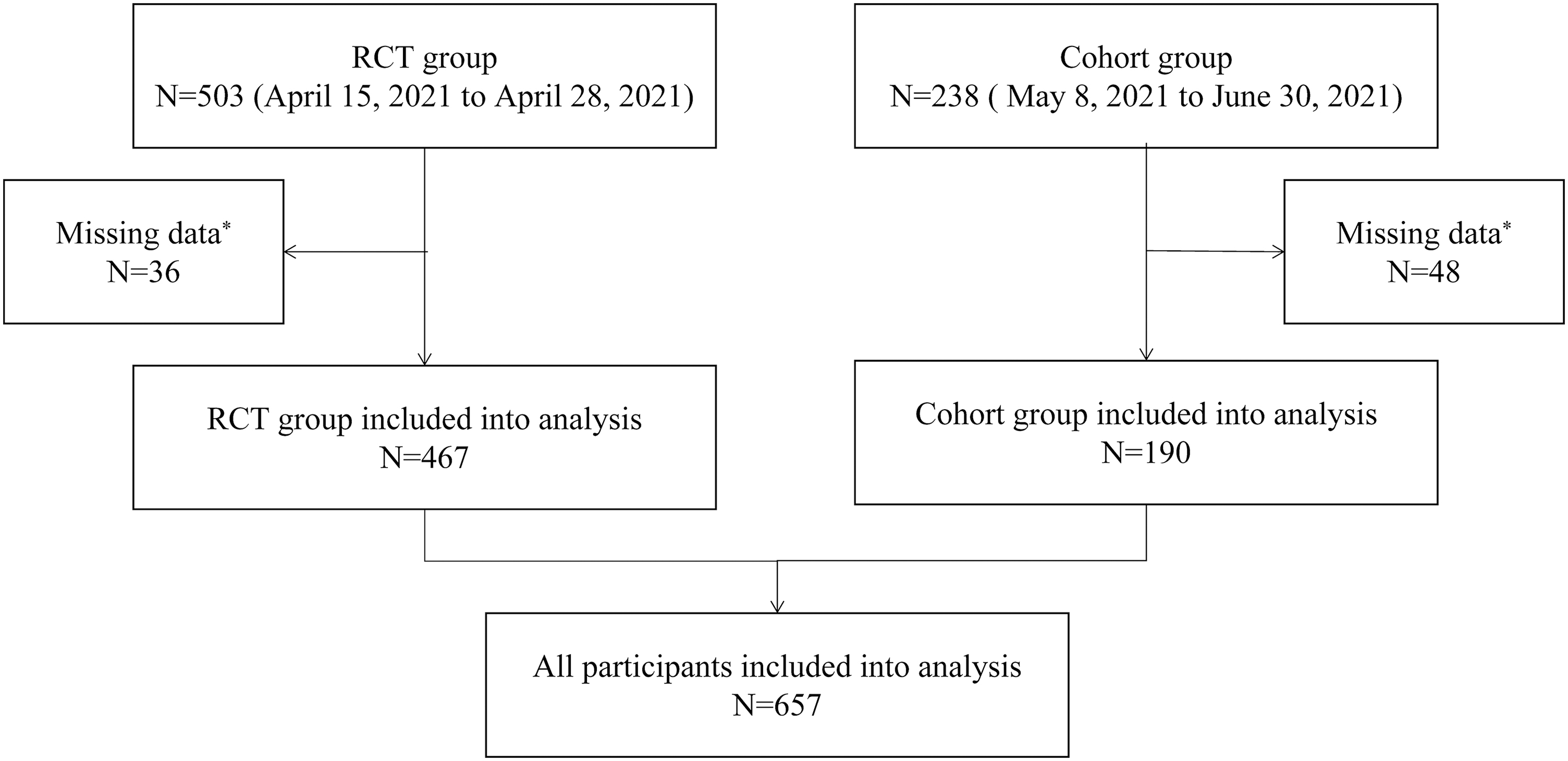
Patient flowchart. *Insufficient blood sample for the measurement of thyroid function and antithyroid antibodies.
Demographic Characteristics of Participants
BMI, body mass index; SD, standard deviation.
Thyroid function and autoimmunity before and after SARS-CoV-2 vaccination
In general, the overall median thyroid function and antithyroid antibody levels before (baseline) and after SARS-CoV-2 vaccination were within the normal range (Supplementary Table S1). The percentages of overt and subclinical hyperthyroidism postvaccination were 0.30% (2/657 [CI 0.04–1.10]) and 2.74% (18/657 [CI 1.63–4.30]), respectively, while those of overt and subclinical hypothyroidism were 0 and 1.06% (7/657 [CI 0.43–2.18]), respectively.
Among those participants with normal thyroid function at baseline, 6.38% (36/564 [CI 4.51–8.73]) developed thyroid dysfunction postvaccination; the indicators of the highest abnormal rate were TSH (3.02% [CI 1.83–4.67]), followed by TT4 (2.88% [CI 1.71–4.51]) and fT3 (1.30% [CI 0.56–2.54]) (Table 2). A total of 545 recipients tested negative for all three antithyroid antibodies at baseline, and none of these recipients developed abnormal antibodies postvaccination.
The Change of Thyroid Function and Antithyroid Antibodies Pre- and Post-Severe Acute Respiratory Syndrome Coronavirus 2 Vaccination
Normal total thyroid function means each indicator of thyroid function was within normal range; abnormal total thyroid function means any indicator of thyroid function was out of normal range; normal total antithyroid antibodies mean each indicator of antithyroid antibodies was within normal range; abnormal total antithyroid antibodies mean any indicator of antithyroid antibodies was out of normal range.
CI, confidence interval; TSH, thyrotropin; fT3, free triiodothyronine; fT4, free thyroxine; TgAb, antithyroglobulin antibody; TPOAb, antithyroid peroxidase antibody; TRAb, thyrotropin receptor antibody; TT3, total triiodothyronine; TT4, total thyroxine.
Among those with negative TPOAb, TRAb, or TgAb at baseline, almost all of them (>99%) maintained a normal level within the corresponding reference ranges, while the TPOAb or TRAb level of three participants was slightly elevated. Of the 93 recipients with abnormal baseline thyroid function, 75.27% (70/93 [CI 65.24–83.63]) returned to normal after vaccination; the indicators of the highest normal rate in decreasing order were fT4, TT3, and fT3. For recipients with thyroid function inversed to normal, most of the recipients' indicators had relatively significant improvement (Supplementary Fig. S1).
Most recipients with abnormal TPOAb and TgAb values at baseline continued to test positive, at a rate of 96.20% ([CI 89.30–99.21], 76/79) and 88.31% ([CI 78.97–94.51], 68/77), respectively, after vaccination. However, the TgAb levels in more than half of these recipients (48/77) decreased (Supplementary Table S2). Abnormal levels of TRAb in 11 recipients at baseline decreased postvaccination, whereas those in 7 cases (63.64%; [CI 30.79–89.07]) changed to negative. Table 3 gives the relationship between the alterations in thyroid function and those in autoimmune status.
Participants in Different Thyroid Function and Antithyroid Antibody Levels Pre- and Post-Severe Acute Respiratory Syndrome Coronavirus 2 Vaccination
TF, thyroid function; Abs, antithyroid antibodies; norm, normal; abn, abnormal; neg, negative; pos, positive.
Correlation between thyroid function, autoimmunity, and SARS-CoV-2 NAbs
The positive rate of SARS-CoV-2 NAb postvaccination was 97.3% (639/657). Spearman correlation analysis revealed no correlation between most of the indicators of thyroid function and autoantibody levels pre- and postvaccination, and SARS-CoV-2 NAb levels 28 days after the second dose. However, prevaccination levels of TT3, TT4, and TgAb and the postvaccination level of TT4 showed weak correlations with SARS-CoV-2 NAb titers, with correlation coefficients of 0.09, 0.09, 0.08, and 0.10, respectively (Figs. 2 and 3).
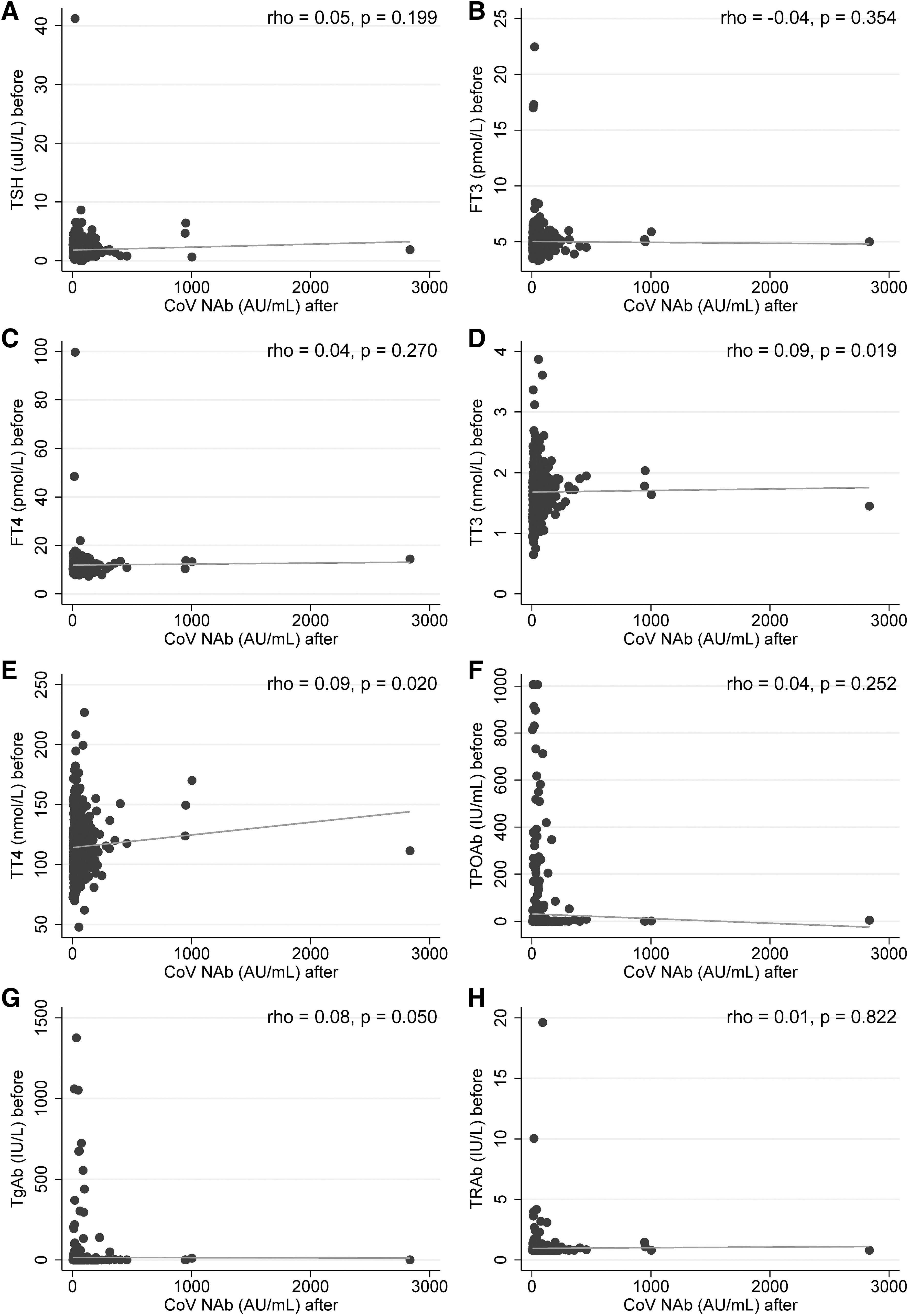
The correlation between the level of thyroid function and antithyroid antibodies prevaccination and CoV NAb. TSH (
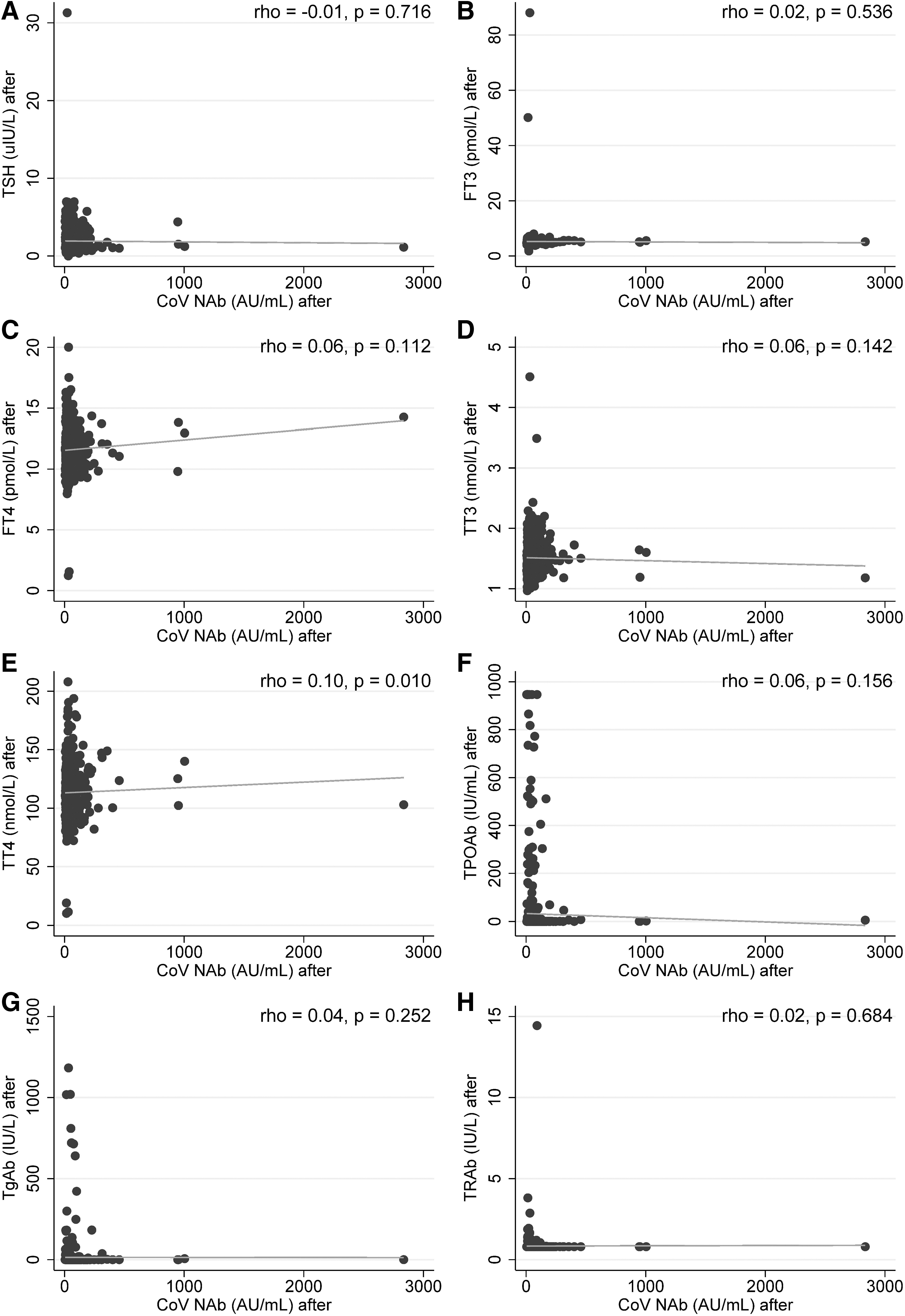
The correlation between the level of thyroid function and antithyroid antibodies postvaccination and CoV Nab. TSH (
Discussion
To the best of our knowledge, this is the largest report of thyroid function and antithyroid antibody levels in postinactivated SARS-CoV-2 vaccinated recipients, and their correlation with SARS-CoV-2 NAb levels was explored. In brief, vaccination against SARS-CoV-2 did not have a significant adverse impact on recipients with normal thyroid function and antithyroid antibodies within the first 28 days after the second dose. For those with abnormal thyroid function and autoimmunity at baseline, only a few became aggravated, whereas most recipients showed an improvement trend postvaccination.
Although SARS-CoV-2 vaccines have been used worldwide, knowledge about their impact on the thyroid remains limited. Currently, there are several cases of inflammatory or autoimmune responses in the thyroid after SARS-CoV-2 vaccination, such as Graves' disease 11 –13 and thyroiditis. 5,6,8 –10 The incidental phenomena of disturbance of thyroid function and autoimmunity may be associated with vaccine adjuvants, which is referred to as autoimmune/inflammatory syndrome induced by adjuvants. 17
In some genetically susceptible individuals, adjuvants may cause autoimmune responses, including autoimmune thyroid diseases, through aberrant activation of immune cascade signaling pathways. 18,19 Molecular mimicry may be another factor in autoimmunity. The genetic similarity of the SARS-CoV-2 spike glycoprotein in vaccines and mammalian proteomes 20 may cause immune cross-reactions to induce autoimmune thyroiditis. 21,22
Few studies have investigated the impact of SARS-CoV-2 vaccination on thyroid function and antibodies; however, conclusions of these studies were controversial due to the limited sample size. 23,24 In our study, we found that, after vaccination, 6.38% of recipients with normal baseline thyroid function developed thyroid dysfunction; 0.35% and 0.15% of recipients switched from normal thyroid autoimmune statuses of TPOAb and of TRAb to abnormal thyroid autoimmune statuses, respectively.
The American Thyroid Association and the European Society of Endocrinology have provided information on the safety of SARS-CoV-2 vaccination for patients with stable thyroid diseases. 25,26 Our findings support these recommendations.
Some studies have shown that the antibody response to SARS-CoV-2 vaccine may be influenced by age, sex, and chronic conditions such as hypertension and diabetes mellitus. 27 –30 Tretyn et al also reported that thyroid diseases could affect the concentration of anti-SARS-CoV-2 IgG antibodies. 29 Our study found no statistical difference between SARS-CoV-2 NAb titers and most of the thyroid function and antithyroid antibody indicators pre- and postvaccination. The correlation coefficients of the indicators with statistical significance were ≤0.1. Thus, our data suggest very weak correlation between thyroid function and antithyroid antibody levels pre- and postvaccination and SARS-CoV-2 NAbs.
There are some limitations in this study. First, we included only inactivated SARS-CoV-2 vaccines in this study and our findings may not be generalizable to other SARS-CoV-2 vaccines. In mainland China, the mRNA SARS-CoV-2 vaccine was not approved for use at the time of this study; thus, data on it could not be acquired. It is important to study whether other types of SARS-CoV-2 vaccines impact thyroid function and/or autoimmunity. Another limitation is that we only monitored thyroid function and antithyroid antibody levels for a short period after the second vaccine dose and did not collect long-term data.
In conclusion, in this study, inactivated SARS-CoV-2 vaccination had no severe impact on thyroid function or antithyroid antibodies within the first 28 days after the second dose. The potential impact of different types of SARS-CoV-2 vaccines on thyroid function and autoimmunity at different time points postvaccination requires further study.
Footnotes
Authors' Contributions
H.X. and M.L. supervised the study. L.L., X.C., B.L., and D.L. contributed equally to the study. H.X., M.L., L.L., and Y. Liu conceived and designed the study. D.L., Y. Liu, R.M., and F.L. recruited participants and collected blood samples. L.L., Y. Liu, and R.M. performed the experiments and collected data. B.L. performed statistical analysis. L.L., X.C., B.L., and D.L. drafted the report. H.X., M.L., Y. Li, S.P., R.L, and Y. Liu made critical revision on the article. All authors contributed to the interpretation of data. All authors approved the final version before submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by The Talent Program of the First Affiliated Hospital, Sun Yat-sen University (Grant No. Y70311).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2