
Abstract
Background:
Fasting during Ramadan may be challenging for patients on levothyroxine (LT4), as the drug has a narrow therapeutic index and is administered on an empty stomach. The majority of Muslims who fast in Ramadan have two meals per day, iftar immediately after sunset and suhoor just before dawn. This study aimed at evaluating the impact of LT4 timing during Ramadan on thyrotropin (TSH) levels in patients who underwent total thyroidectomy to determine the best timing for intake and identify the predictors of TSH level changes.
Methods:
We conducted a parallel, double-blind, randomized controlled trial on Saudi patients diagnosed with hypothyroidism who underwent total thyroidectomy. Patients were required to have stable thyroid function for 6 months before the study period and fast ≥20 days of Ramadan. Participants were randomized to one of three times for LT4 administration: Group A, 30 minutes pre-iftar (n = 48); Group B, 3 hours post-iftar (n = 47); or Group C, 1 hour pre-suhoor (n = 47). The number of participants in the final analysis (excluding patients who dropped out) was as follows: Group A, (n = 31); Group B, (n = 34); and Group C, (n = 22). The changes in TSH and free thyroxine (fT4) levels two weeks before and after Ramadan were compared. Factors associated with a change in TSH levels were examined through multivariable analysis.
Results:
The TSH levels significantly increased in Group B (1.7 ± 1.8 mU/L vs. 3.1 ± 3.9 mU/L, p = 0.003) and Group C (2 ± 1.7 mU/L vs. 5.5 ± 10 mU/L, p = 0.011), but not Group A (1.8 ± 1.6 mU/L vs. 3.3 ± 4.2 mU/L, p = 0.158). The change in fT4 levels was comparable among the groups: Group A, 16.5 ± 2.7 mcg/dL vs. 15.9 ± 3.2 mcg/dL, p = 0.144; Group B, 15.8 ± 3.8 mcg/dL vs. 16.3 ± 3.6 mcg/dL, p = 0.620; and Group C, 17.5 ± 2.8 mcg/dL vs. 17.3 ± 3.9 mcg/dL, p = 0.770. In multivariable linear regression analysis, the following variables were significantly independently associated with TSH level change: age, weight gain, and the number of nonadherence days to LT4, where β = −0.2, p = 0.026; β = + 0.2, p = 0.026; and β = + 0.5, p < 0.0001, respectively.
Conclusions:
Fasting patients who took LT4 pre-iftar did not experience significant changes in TSH, whereas those who took LT4 post-iftar or pre-suhoor did. The TSH changes during Ramadan may be associated with age (inverse association), weight gain, and the number of non-adherence to LT4 days.
Trial Registration:
SCTR Application no. 21122002.
Introduction
Hypothyroidism is one of the most common endocrine diseases worldwide and it is treated with levothyroxine (LT4). LT4 is recommended to be taken in the morning, on an empty stomach, one hour before breakfast, and separated at least four hours from other drugs that interfere with LT4 absorption (1). Several studies have reported a high rate of non-adherence to LT4 among patients with hypothyroidism (2,3).
During the month of Ramadan, Muslims refrain from eating and drinking from sunrise to sunset, with major changes in physical activity, sleeping times, and dietary patterns. Most Muslims in Ramadan consume two main meals per day, one immediately after sunset (iftar), and one just before dawn (suhoor). Consequently, LT4 intake during Ramadan can be a challenge for most Muslims. To ensure LT4 intake on an empty stomach during Ramadan, patients should fast at least an additional 30 minutes after sunset. Recently, interest in research on diabetes management during Ramadan has increased (4 –6); however, data on thyroid disorders and LT4 replacement during Ramadan remain sparse (7,8).
Numerous discussions on the best timing for taking LT4 have taken place. Some studies have revealed that no difference exists between LT4 intake at bedtime and its intake in the morning (9,10), while other studies favor bedtime (11) or morning intake (12). Thus, the optimal LT4 timing during Ramadan remains undetermined, and, to date, very few studies have evaluated the optimal time to take LT4 during Ramadan, particularly among patients who have undergone total thyroidectomy (13).
This double-blind, randomized controlled trial aimed at evaluating the impact of LT4 timing on thyrotropin (TSH) during Ramadan in patients who underwent total thyroidectomy for benign goiter or differentiated thyroid cancer to determine the best time for LT4 intake during Ramadan. In addition, we examined the factors associated with changes in TSH levels during Ramadan.
Materials and Methods
Study design
We conducted a parallel, double-blind, randomized controlled trial of patients diagnosed with hypothyroidism who had undergone total thyroidectomy. Participants were randomized to one of three time-points for LT4 administration during Ramadan. The study was conducted from February to May 2021 at a tertiary care center in Riyadh, Saudi Arabia. Written informed consent was obtained from all participants before enrollment. The study was approved by the Institutional Review Board of King Saud University and registered at the Saudi Food and Drug Authority (SFDA) Clinical Trials Department (SCTR No.: 21122002).
Participants
Patients aged 18 years or older diagnosed with hypothyroidism, with stable thyroid function (TSH levels of 0.59–4.37 mU/L, per the local adult reference range) (14) were eligible for the study. Further, those willing to fast during the month of Ramadan (April 13 to May 12, 2021) with a history of total thyroidectomy, taking LT4, without any change in LT4 dose in the six months before the study period, were enrolled.
Patients who were planning pregnancy, had a chronic illness impacting fasting or LT4 absorption, or had high-risk thyroid cancer that required TSH suppression below the normal reference range were not eligible for enrollment in the study.
Randomization
Eligible participants were randomized by computerized block randomization into three groups according to the time of LT4 intake: Group A, pre-iftar: LT4 intake is at the time of the iftar meal and delay feeding for at least 30 minutes; Group B, post-iftar: LT4 intake is at least 3 hours after the iftar meal and abstain from feeding at least 30 minutes after; and Group C, pre-suhoor: LT4 intake is at least 1 hour before the predawn meal (suhoor) and abstain from feeding for at least 2 hours before the meal. Our pharmacy staff prepared containers with strips containing LT4 and a placebo.
The patients were advised to take a pill at each time-point and were blinded to the assigned timing. All patients were given all three tablets: a pre-iftar tablet, post-iftar tablet, and pre-suhoor tablet. Depending on the random group, one of the tablets contained the active ingredient and the other two tablets were placebo. The participants were randomized to a container number indicating group assignment. The container identification was kept concealed by the pharmacist, who was not participating in the study. Participants were instructed to maintain their usual Ramadan diet and exercise patterns.
Follow-up and outcomes
The TSH levels, free thyroxine (fT4) levels, weight, and body mass index (BMI) values were measured during the two weeks before and the two weeks after Ramadan, where all patients were tested at least six weeks and, at most, eight weeks apart. Baseline characteristics and thyroid-related records, including age, sex, nationality, underlying conditions that necessitated LT4 initiation, diagnosis after thyroidectomy, duration of LT4 intake, weekly dose of LT4, dose of LT4 per kg, comorbidities, and medications affecting LT4 absorption, were collected.
During the follow-up period, patients were interviewed by telephone and were asked about the number of days fasted out of the 30-day period, number of days any of the pills were not taken, and their opinion on the convenience of LT4 timing. Participants were informed of their allocation to each group only after the analysis was completed and the study had ended. The participants' outcome of perceived convenience of the timing of LT4 intake was evaluated using binary responses (Yes/No) for the question: “Taking medication every day at a specific time is a real inconvenience for some people. Do you feel hassled about sticking to LT4 timing?” Patients who failed to undergo biochemical testing for TSH and T4, fasted for <20 days, or missed >5 days of LT4 intake during Ramadan were excluded.
The primary study outcome was the difference in serum TSH levels before and after Ramadan. Secondary outcomes included fT4 levels, weight change, and participant self-reported convenience.
Thyroid function test
Serum concentrations of TSH and fT4 were measured using the electrochemiluminescence immunoassay (ECLIA) method (Cobas; Roche Diagnostics, Mannheim, Germany), and the reference ranges were 0.27–4.2 mU/mL and 12–22 pmol/L, respectively.
Statistical analysis and power calculation
Categorical variables were summarized using frequency and percentage distributions, and descriptive analyses were performed as appropriate. Continuous variables were summarized by calculating measures of central tendency (mean) and dispersion. To assess the normality of their distribution, the three scale scores were examined using the Kolmogorov–Smirnov normality test, and their kurtosis and skewness were also examined.
The Pearson correlation test was employed to assess the direction, magnitude, and statistical significance of the (univariate) relationships among the continuous variables. Continuous variables were compared using Mann–Whitney and Kruskal–Wallis tests. For within-subject analysis, the Wilcoxon signed-rank test was used to assess any significant changes. A multivariable linear regression analysis was used to assess the association of the independent variables (age, number of days of missing LT4, and weight change) with the dependent variable (TSH change from before to after Ramadan). For all of these tests, an alpha of 0.05 was set as the cut-off point of statistical significance. Analyses were performed using IBM SPSS version 26 (IBM Corp., Armonk, NY).
Out of the 202 subjects who attended the Specialized Thyroid Clinic, 142 were eligible for recruitment into the study, and 87 completed the study as 55 participants dropped out. A post hoc power analysis was performed using GPower software. The premises used in this calculation were the ANOVA test results for the T4 comparison among the three groups. The results indicated that the total sample of participants who completed the study was sufficient to support the minimal acceptable sample power with α = 0.05 and β = 0.8.
Results
Patient characteristics
A total of 202 participants were screened for eligibility (Fig. 1). The main reason for the declining study participation was the inconvenience of travel/transport to the hospital for laboratory tests. The number of participants randomized was 142. Participants were randomized to one of three times for LT4 administration: Group A, 30 minutes pre-iftar (n = 48); Group B, 3 hours post-iftar (n = 47); or Group C, 1 hour pre-suhoor (n = 47). A total of 33 participants were excluded after randomization for the following reasons: 14 because the TSH values were above the upper limit of the reference range during the pre-Ramadan period, 8 for fasting for <20 days of Ramadan, and 11 for noncompliance with the pills for >10 days.
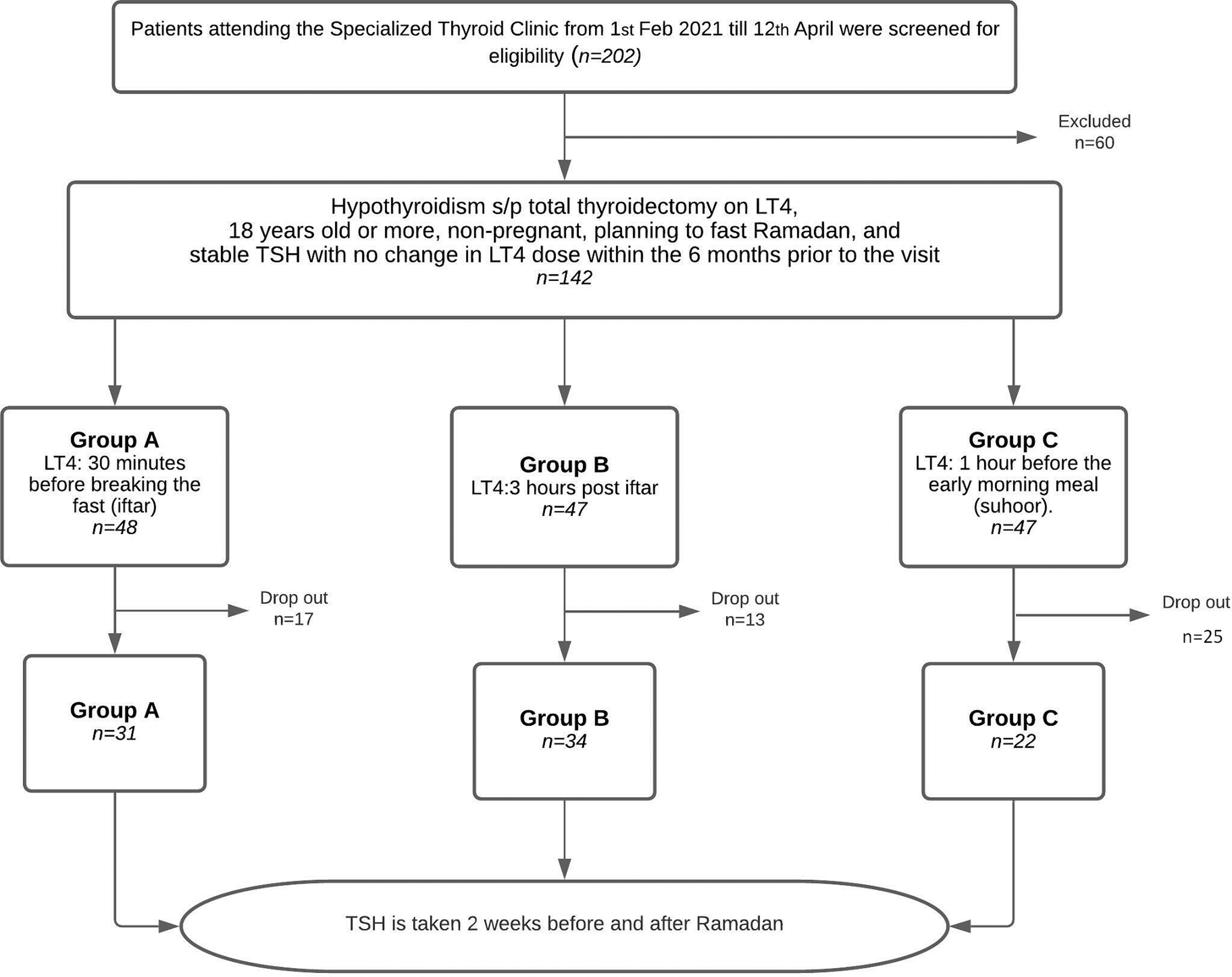
Consort participant flow diagram. A total of 202 patients attending the Specialized Thyroid Clinic were screened for eligibility, and 142 met the inclusion criteria. These were randomly assigned to Group A (pre-iftar), B (post-iftar), or C (pre-suhoor) (48, 47, and 47 patients, respectively). Of these, 17, 13, and 25 patients dropped out of the study from Group A, B, and C, respectively, and 31, 34, and 22 (a total of 87) patients in the respective groups completed the study. LT4, levothyroxine; TSH, thyrotropin.
In addition, 22 patients withdrew due to personal reasons that hindered their ability to present to the hospital for laboratory investigations. A total of 87 randomized participants completed the study: 31 in Group A (pre-iftar), 34 in Group B (post-iftar), and 22 in Group C (pre-suhoor), excluding individuals who dropped out of the study after randomization.
Most of the participants were Saudi nationals (96.5%) and women (84%), with a mean age of 45 years, BMI of 29.70 kg/m2, and LT4 intake for 7.28 years. The clinical indication for the initiation of LT4 was hypothyroidism after total thyroidectomy for cancerous or benign lesions in 81.6% of the participants, and ∼18.4% were started on LT4 due to underlying Hashimoto's thyroiditis before they underwent total thyroidectomy for cancerous or benign lesions and continued taking the drug after surgery. The mean dose of LT4 was 785.3 ± 231.8 mcg per week (1.5 ± 0.5 mcg/kg/day).
Overall, the average number of days fasted by the participants was 27.2 ± 3.2 days, with an average of 2.7 ± 3.2 days of missing the LT4 dose. Moreover, the mean TSH and fT4 values at baseline were 1.7 ± 1.7 mIU/L and 16.5 ± 3.2 pmol/L, respectively. The study groups were comparable at baseline, as no significant differences were observed between the three groups in terms of demographic characteristics (Table 1).
Baseline Characteristics of the Study Participants (n = 87)
Data are shown as mean (SD) and the number of participants (%) as appropriate.
Levothyroxine timing during Ramadan: Group A: pre-iftar, levothyroxine intake is at the time of the sunset meal with the meal delayed for at least 30 minutes; Group B: post-iftar, levothyroxine intake is at least 3 hours after the sunset meal with any oral intake is delayed for at least half an hour after levothyroxine; Group C: pre-suhoor, levothyroxine intake is at least 1 hour before the predawn meal while avoiding oral intake for at least 2 hours before levothyroxine intake.
Differences in the timing of levothyroxine intake were examined using the Kruskal–Wallis test for continuous variables and the chi-square test for categorical variables.
BMI, body mass index; fT4, free thyroxine; HTN, hypertension; PPI, proton pump inhibitor; SD, standard deviation; T2D, type 2 diabetes; TSH, thyrotropin.
Primary and secondary outcomes: changes in TSH, fT4, and anthropometrics
In the entire study population, a significant increase in TSH levels was observed between pre- and post-Ramadan levels (1.8 ± 1.7 mU/L vs. 3.8 ± 6.1 mU/L, p = 0.001). This significant change was driven mainly by the significant increase in the TSH level in Group B (pre 1.7 ± 1.8 mU/L vs. post 3.1 ± 3.9 mU/L, p = 0.003) and Group C (pre 2 ± 1.7 mU/L vs. post 5.5 ± 10 mU/L, p = 0.011); however, the difference in TSH levels in group A did not achieve statistical significance (1.8 ± 1.6 mU/L vs. 3.3 ± 4.2 mU/L, p = 0.158).
The change in fT4 levels was comparable among the three groups: Group A, 16.5 ± 2.7 mcg/dL vs. 15.9 ± 3.2 mcg/dL, p = 0.144; Group B, 15.8 ± 3.8 mcg/dL vs. 16.3 ± 3.6 mcg/dL, p = 0.620; and Group C 17.5 ± 2.8 mcg/dL vs. 17.3 ± 3.9 mcg/dL, p = 0.770. No significant difference was observed in weight or BMI between the participants pre- and post-Ramadan in any of the groups (Table 2).
Group Comparisons in Their Pre- and Post-Ramadan Thyrotropin and Free Thyroxine Levels, Weight, and Body Mass Index
Bold p-values are significant.
Data are shown as the mean (SD). Groups according to levothyroxine timing during Ramadan: Group A: pre-iftar, levothyroxine intake is at the time of the sunset meal with the meal delayed for at least 30 minutes; Group B: post-iftar, levothyroxine intake is at least 3 hours after the sunset meal with any oral intake delayed for at least half an hour after levothyroxine; Group C: pre-suhoor, levothyroxine intake is at least 1 hour before the predawn meal while avoiding oral intake for at least 2 hours before levothyroxine intake.
p-Value comparing pre- with post-Ramadan variables.
Coefficient of variation for fT4 and TSH
The coefficient of variation was calculated to compare the magnitude of variation of fT4 pre- and post- Ramadan. The variability of the fT4 levels remained the same pre- and post-Ramadan, which may indicate independence from the time of the fT4 levels. However, the extent of variation in the TSH levels increased by 0.6 between pre- and post-Ramadan measurements.
Factors associated with TSH change from before to after Ramadan
In a univariate analysis, the number of days on which the LT4 dose was missed was the most strongly associated with TSH level change, as each day of missing LT4 was associated with an increase in TSH change by 0.5 (β = + 0.5, t = 5.8, p < 0.001). Age was significantly inversely associated with TSH level (β = −0.2, t = −2.26, p = 0.026), indicating that each 1-year increase in the participant's age was associated with a 0.2 decrease in the change from pre- to post-Ramadan TSH levels.
In contrast, the change in weight was significantly positively associated with a change in TSH levels (β = +0.2, t = 2.2, p = 0.026). Each 1 kg increase in the participants' weight resulted in a 0.2 increase in the difference between the pre- and post-Ramadan TSH levels. In a multivariable linear regression analysis, participants' age, weight, and medication adherence were significantly associated [F = 17.7, (df) = 3, p < 0.0001] with the difference in TSH levels from before to after Ramadan. Collectively, these factors were associated with the magnitude of TSH level change, as reflected by an adjusted determination coefficient R 2 of 37% (p < 0.0001) (Table 3). A figure of the Multivariable linear regression analysis examining factors associated with thyrotropin level changes before and after Ramadan is found in Supplementary Figure S1.
Univariate Analyses and Multivariate Linear Regression Analysis Examining Factors Associated with Thyrotropin Level Changes Before and After Ramadan
R 2 refers to the coefficient of determination: to test the overall magnitude of the effect size of the independent variables on the dependent variable.
β Refers to the Standardized Regression Coefficients: to examine the magnitude of the effect size of the independent variables on the dependent variable.
t Refers to the Student's t-test: to examine the significant difference between β and 0.
p-Value = level of significance. p-Value is considered statistically significant at 0.05.
F-multivariate analysis test.
df, degree of freedom.
Convenience of LT4 timing
The majority of overall participants (n = 76, 87.4%), as well as most participants in each group (Group A [n = 29, 93.5%], Group B [n = 30, 88.2%], Group C [n = 17, 77.3%]), reported that their experience with the LT4 timing was convenient. Comparing the three groups, the proportions of participants who reported convenience in each group were close, with no statistically significant difference, despite some variations according to the chi-squared test (χ2 = 3.1, df = 2, p = 0.223).
Discussion
In our study on patients who underwent thyroidectomy and were fasting during Ramadan, pre-iftar LT4 administration was not associated with any significant changes in TSH levels, whereas significant changes in TSH levels were observed with LT4 administration post-iftar or pre-suhoor. Previous studies have shown contradictory results regarding the optimal timing of LT4 administration. Some authors have reported that the best time for LT4 intake is at bedtime (9,15).
Other authors have reported that taking LT4 in the morning is better for maintaining a stable TSH level (12); yet researchers from another study observed no significant change in TSH level, regardless of the timing (16). The THYRAM study examined the optimal timing of LT4 intake, and the authors did not observe any significant differences among the three timings of LT4 intake (pre-iftar, post-iftar, and pre-suhoor); however, the lack of randomization may have contributed to some bias (13).
Moreover, a significant increase in TSH levels among participants regardless of the timing of LT4 intake or the interval between LT4 intake and the meal during Ramadan was observed in a smaller study (17). Dabbous et al conducted a prospective study and reported a significant increase in TSH in both timings of LT4 intake, pre-iftar and pre-suhoor, with no difference in the effect between the two timings (18).
Several studies have been conducted on the optimal LT4 timing in patients with primary hypothyroidism during Ramadan (7,8). Nevertheless, our study is the first to evaluate patients who have undergone total thyroidectomy for benign or cancerous lesions. Thyroidectomy is the primary therapeutic modality for differentiated thyroid cancer with individualized TSH targets according to the therapeutic response and risk of recurrence (19). Thus, studying the best time for LT4 intake during the month of Ramadan is vital, particularly among people who have undergone thyroidectomy who were not previously investigated.
Moreover, our finding of a strong association between nonadherence to LT4 intake and the change in TSH levels demonstrates the importance of choosing the most convenient time for LT4 intake, especially for patients who are fasting during the month of Ramadan. In addition, weight gain during Ramadan was associated with a significant increase in the change in TSH levels, irrespective of the timing of LT4 intake. Thus, whether increasing the dose of LT4 during Ramadan would be effective in stabilizing TSH levels should be investigated (20,21).
The prolonged fasting hours that are usually followed by heavy meals after breaking the fast during Ramadan may cause alterations in gastric motility, circadian rhythm, and deiodinase activity, resulting in subsequent changes in LT4 absorption and metabolism (7). We did not advise the patients to restrict their calorie intake or follow a specific diet, nor did we monitor their diet with a dietary diary; however, the three allocated times for LT4 intake support the premise that the medication would be taken on an empty stomach.
Studies have shown that fasting affects hormonal physiology, such as causing a decrease in triiodothyronine levels, whereas TSH levels remain unchanged (22). However, increasing the LT4 dosage during prolonged periods of fasting may not be suitable for all age groups, as reflected by our finding that increasing age negatively impacted the change in TSH levels; that is, the older the person, the more TSH levels decreased after Ramadan. Ultimately, age, weight, and adherence were found to be significantly independently associated with TSH change from before to after Ramadan.
Fasting for prolonged hours is challenging for patients, as they should wait for half an hour before breaking their fast when they are on LT4, especially in countries with prolonged fasting hours. In addition, patients find it difficult to wake up half an hour before suhoor to take LT4, so they may either miss the dose or take it with food. An important consideration in managing chronic conditions, along with the therapeutic targets, is making the therapeutic regimen easy and convenient for patients.
In our study, we investigated patients' opinions regarding the convenience of their LT4 timing during Ramadan. Interestingly, most patients in our study found it convenient to take LT4 regardless of the timing: pre-iftar, post-iftar, or pre-suhoor.
Our study is the first double-blind, randomized controlled trial investigating the change in TSH levels during prolonged fasting throughout Ramadan, specifically focusing on patients who underwent thyroidectomy and were on LT4 replacement therapy. The implicit assumption with this design is that randomization and blinding would control for any possible bias.
The order of the tablet containing the active ingredient in a three-times-per-day dosing scheme may make the participants of all the groups self-assess their adherence as being “good” based on the fact that they were adherent to their first dose; however, they may have all been less adherent to the second and third doses. This may result in an apparent advantage to taking the tablet pre-iftar and could partially explain the results. For example, Paes et al. reported more adherence to the first tablet of a three-times-per-day dosing scheme in patients with diabetes compared with the second and third tablets (23).
Our study had several limitations. First, this was a single-center study that included patients who underwent thyroidectomy, which may not represent the general population of patients taking LT4 for primary hypothyroidism or radioactive iodine treatment-induced hypothyroidism. Second, the small sample size and the high participant dropout rates (in all three treatment arms) may affect the internal validity of the results and could have resulted in random variation rather than true biological changes in TSH.
However, a post hoc power calculation suggested sufficient powering of the study. Third, TSH was measured only at two time-points, two weeks before and two weeks after Ramadan. These TSH changes could be related to random changes in TSH and fT4, diurnal rhythm, or the day-to-day changes in the lab, rather than a real change due to the timing of LT4 intake. If we could have measured TSH and fT4 every one to two weeks during the trial period, the results of TSH and fT4 changes would have been more compelling in showing a consistent trend.
However, it would not have been convenient for the patients to visit the hospital that often while fasting the month of Ramadan. This is particularly important, as the inability to revisit the hospital for laboratory investigations during the two designated time-points was the main reason for participants dropping out of the study. Also, the history of compliance with LT4 timing was self-reported by participants, which may have affected reliability.
Clear clinical practice guideline recommendations should be developed to inform optimal counseling on LT4 treatment and follow-up, for patients on thyroid hormone replacement (including those with prior thyroidectomy) who plan to fast during Ramadan.
Conclusion
Our study results suggest that LT4 administration pre-iftar, but not post-iftar or pre-suhoor, may be more likely to maintain stable TSH levels during Ramadan fasting in patients who have undergone thyroidectomy. Changes in TSH levels during Ramadan may be associated with patients' age, weight gain, and the number of days of nonadherence to LT4. Nevertheless, our findings require confirmation in other populations.
Footnotes
Authors' Contributions
A.A.J.: Conceptualization, Methodology, Investigation, Resources, Writing-Review and Editing, Supervision, Visualization, and Project Administration. K.M.A.-Q.: Data Curation, Writing-Original Draft, and Writing-Review and Editing. I.A.A.: Data Curation and Writing-Original Draft. A.M.A.: Data Curation and Writing-Original Draft. N.S.A.: Data Curation and Writing-Original Draft. R.M.B.: Writing-Review and Editing. E.Y.A.: Methodology, Data Curation, Writing-Original Draft, Writing-Review and Editing, and Supervision. All authors have read and agreed to the published version of the article.
Acknowledgments
The authors are grateful to the patients who participated in this study. They would like to thank Editage for English language editing.
Data Availability
The data used to support the findings of this study are included within the article.
Author Disclosure Statement
No competing financial interests exist. The research meets the ethics guidelines, including adherence to the legal requirements of the country where the study was performed.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1