
Abstract
Background:
The incidence of papillary thyroid cancer is increasing worldwide due to more frequent pathological detection of papillary thyroid microcarcinomas (PTMC), which are cancers measuring 1 cm or less in diameter. In rare cases, the course of PTMC can be aggressive, with an increased risk of recurrence/persistent disease. The aim of this study of Polish patients diagnosed with PTMC was to assess the impact of concomitant B-type Raf kinas-activating mutation in codon 600 of exon 15 (BRAFV600E ) and telomerase reverse transcriptase (TERT) hotspot mutations on clinicopathological features, response to treatment, potential recurrence, and the final outcome.
Methods:
A retrospective analysis of the 430 PTMC cases diagnosed during 2001–2020 at a single center was performed. All PTMC cases were assessed histopathologically, and analyses of BRAFV600E and TERT promoter were performed based on DNA isolated from tumor blocks.
Results:
There were 29/430 (6.7% [confidence interval: 4.6–9.5]) patients in whom the TERTC228T and/or TERTC250T mutations coexisted with the BRAFV600E mutation. A statistical comparison between PTMC cases with concomitant BRAFV600E and TERT hotspot mutations and those without any of those mutations revealed no significant differences between the two groups with respect to risk stratification, response to primary treatment, clinical course, or final disease status.
Conclusion:
Regardless of the molecular background of PTMC, the overall response to therapy is excellent, and long-term disease-free survival rates can be achieved by most patients.
Introduction
Differentiated thyroid cancer (DTC) represents about 90% of all types of thyroid cancer, with the papillary histotype being the most common. 1 The incidence of papillary thyroid cancer (PTC) is increasing worldwide. 2,3 Simultaneously, mortality due to thyroid cancer has declined over the past few years. However, in some countries such as the United States, the age-adjusted death rates are increasing slightly. 4 The overall decline in mortality is due to overdiagnosis and more frequent pathological detection of papillary thyroid microcarcinomas (PTMC), which are cancers measuring 1 cm or less in diameter. 5,6 In this context, the definition of PTMC does not refer to histopathological findings (i.e., angioinvasion, extrathyroidal extension [ETE], and a microscopically margin-negative resection) or the status of local or distant metastases at the time of diagnosis. Therefore, the risk of PTMC recurrence, or its persistence, can vary when assessed using the ATA (American Thyroid Association) Risk Stratification System for Thyroid Cancer.
In the latest 8th Edition of the American Joint Committee on Cancer (AJCC) staging system for thyroid cancer the presence of minimal ETE does not affect the staging classification. 7 Thus, minimal ETE does not influence the risk of thyroid cancer-related death. The latest AJCC classification system can better distinguish disease-specific survival rates in relation to cancer stage, and they emphasize the high survival rates for those with small PTC and localized disease. 7 Despite this, however, the presence of minimal ETE increases the risk of recurrence or relapse of thyroid cancer according to the ATA, regardless of tumor size and stage. That said, in most cases of localized PTMC, the prognosis is excellent, with 5-year treatment-free survival rates of up to 96%. 8
In addition, in recent decades, there has been a decline in PTC recurrence rates, which is attributable to the growing number of so-called low-risk PTC. 9 These observations have been acknowledged by Japanese studies, which suggest that active surveillance is the optimal way forward when managing low-risk PTMC in the adult population. Active surveillance of a selected group of low-risk PTMC has no negative effect on survival rates, and can prevent potential complications from surgery, including permanent hypoparathyroidism or vocal cord paralysis. 10 However, there are rare cases of aggressive PTMC with local or distant metastases at the time of diagnosis; these cases require complex treatment.
All of the aforementioned has led to the search for potential prognostic factors for PTMC; these factors should better distinguish patients with low-risk disease, who may benefit from less aggressive treatment and less rigid follow-up. Genetic alterations may be such a marker that will allow better patient stratification and management. An example may be the presence of a concomitant B-type Raf kinas (BRAF)-activating mutation in codon 600 of exon 15 (V600E), and telomerase reverse transcriptase (TERT) hotspot mutations (C228T and C250T), in PTC.
Coexistence of BRAFV600E and TERT mutations is more common in highly aggressive PTC, which carries a high risk of recurrence or relapse. 11,12 In addition, in cases of recurrent PTC, the simultaneous presence of BRAFV600E and TERT mutations is associated with loss of radioactive iodine avidity, which can lead to poor outcomes. 13 Overall, the concomitant presence of BRAFV600E and TERT mutations in PTC is related to a more advanced stage at the time of diagnosis, a worse response to treatment, a higher risk of recurrence and a shorter disease-free survival time.
The most recent European Society for Medical Oncology guidelines assert that coexistence of BRAFV600E and TERT mutations predicts a high risk of persistent or recurrent PTC, regardless of tumor size and lymph node status. 14 To the best of our knowledge, only one article to date has analyzed the effect of concomitant BRAFV600E and TERT hotspot mutations on clinical management of PTMC with respect to treatment. 15
Therefore, the aim of this study was of Polish patients diagnosed with PTMC to retrospectively assess the impact of concomitant BRAFV600E and TERT hotspot mutations on clinicopathological features, response to treatment, potential recurrence, and the final outcome.
Materials and Methods
All of the study procedures were approved by the institutional review board at the Holycross Chamber of Physicians in Kielce, Poland (approval number 109/2018-VII). All patients provided written informed consent. All patients were provided with information about the nature and objectives of the study, as well as the methods. All PTMCs were assessed histopathologically in accordance with the 8th edition of the AJCC staging system for thyroid cancer. 7
All patients included in the study underwent surgery (lobectomy, total thyroidectomy, or total thyroidectomy with central, or central and lateral, compartment lymphadenectomy) as the primary treatment. The extent of the surgery and surgical procedures have been described previously. 16
The evaluation of response to therapy was made 1 year after initial treatment. Patients who were qualified for radioiodine (131I) ablation after surgery were assessed using ATA criteria, which were first proposed by Tuttle et al 17,18 Patients not qualified for radioiodine (131I) treatment were evaluated using the criteria proposed by Momesso and Tuttle. 19 All practices regarding monitoring disease course after operation till evaluation of response to therapy and further follow-up likewise evaluation of treatment have been described previously. 20,21 Treatment response was classified as excellent, indeterminate, biochemically incomplete, or structurally incomplete.
The target value of thyrotropin (TSH) for patients who were evaluated with excellent response to treatment was 0.5-2.0 mU/L. Patients with indeterminate or biochemically incomplete response to treatment had target value of TSH between 0.1 and 0.5 mU/L. Those with structurally incomplete response to treatment had full TSH suppression <0.1 mU/L. Recurrence was defined as detection of biochemical or structural disease after a period (at least 12 months after initial therapy) of no evidence of disease (NED). The clinical status of the patients at the end of the observation period was assessed based on medical records.
During the past 20 years, the approach to radioiodine (131I) treatment in patients with DTC has changed significantly. Previously, all patients with DTC in Poland were treated with radioiodine (131I) after thyroid resection, regardless of the initial risk stratification. In accordance with changes made by a group of Polish experts, patients with low-risk PTMC no longer receive ablation therapy. 22,23
One patient, whose treatment at the Holycross Cancer Centre (HCC) was interrupted (1/430; 0.2%), was assessed as not cured (according to clinical data from the last follow-up visit). Overall, 10/468 (2.3%) patients died. There were no cases of thyroid cancer-related death. Five-years overall survival was 99.5% (Kaplan–Meier estimate). Data from all included patients were censored at September 30, 2021.
Paraffin-embedded tumor blocks specimens after thyroid operation were used for DNA isolation and molecular analyses of BRAFV600E and TERT. No molecular analyses of fine-needle aspiration samples obtained before surgery were performed. Detailed data regarding detection of BRAFV600E and TERT mutations are described in our previous report. 24
Statistical analyses
Categorical data were summarized as numbers and percentages. The χ2 or Fisher's exact test was applied to compare proportions as appropriate. The prevalence rate of BRAF/TERT genetic alterations was presented by point as well as interval estimate (confidence interval [CI]). Particular data were presented as the median and interquartile range, and assessed using the Mann–Whitney U test. The association between selected categorical variables was performed by calculating the odds ratio (OR) and CIs. A two-tailed p-value <0.05 was considered statistically significant. All statistical analyses were performed using R (version 4.0.3; The R Foundation for Statistical Computing, Vienna, Austria).
Results
Study group characteristics
In total, there were 1633 cases of PTMC controlled and treated in our clinic between 2001 and 2020. From this group, consecutive patients who gave their consent during control visits were enrolled to the study. The initial group comprised 505 PTMC cases diagnosed during 2001–2020 at a single tertiary oncology referral center (The HCC in Kielce). In 17 cases, there was degradation of genetic samples. In addition, 56 patients were ruled out due to Sanger sequencing limitation in small PTMC tumors below 3 mm in diameter; therefore, 430 patients were enrolled in the study (Fig. 1).
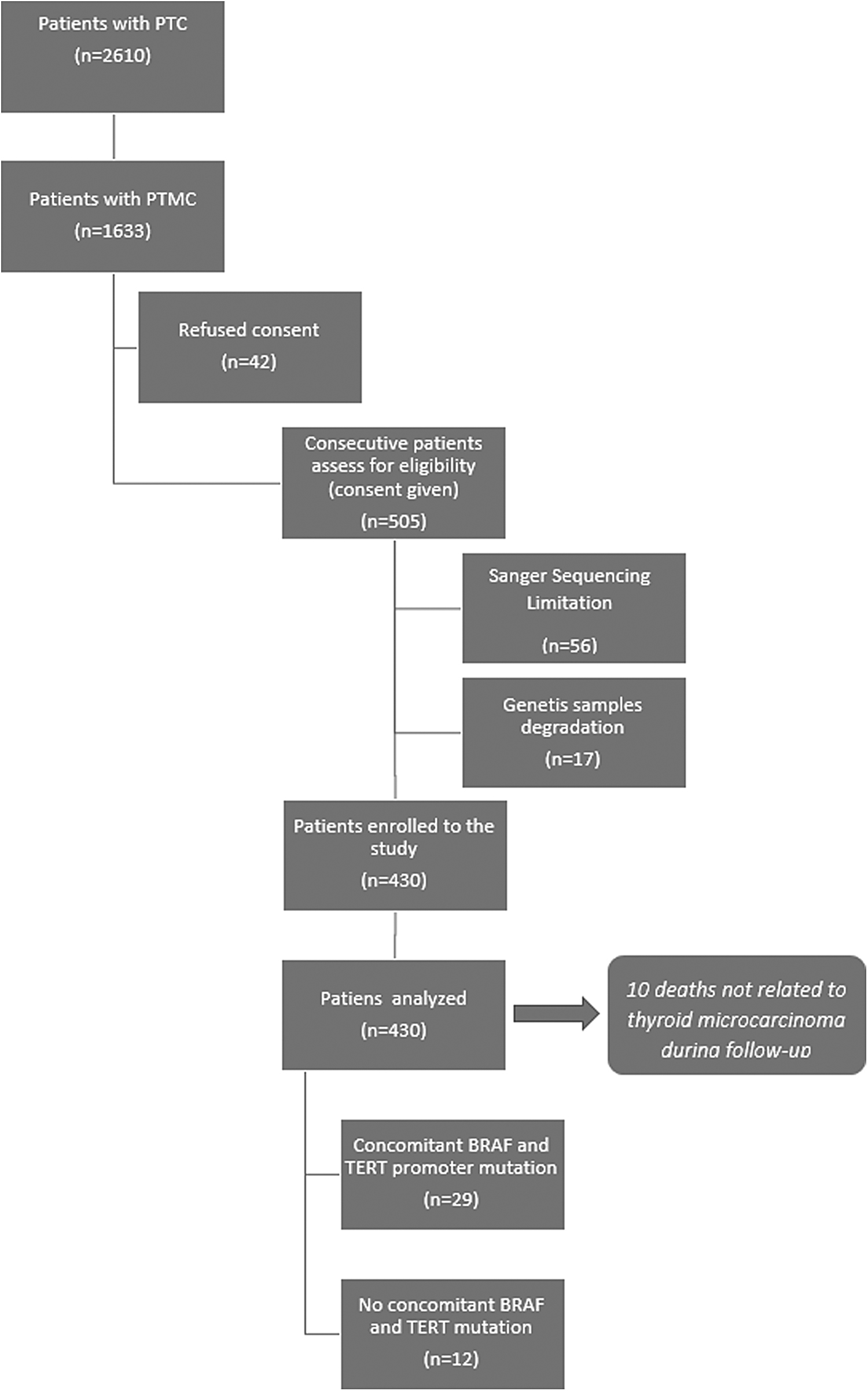
Numbers of individuals at each stage of study.
Three hundred seven of these patients were previously analyzed in our other study. 24 Patient characteristics are presented in Table 1.
Characteristics of Patients with Papillary Thyroid Microcarcinoma at the Time of Diagnosis: American Joint Committee on Cancer 8th Edition
ATA, American Thyroid Association; Q1, first quartile; Q3, third quartile; SD, standard deviation.
There were 280 (65.1%) cases of PTMC diagnosed preoperatively. One hundred fifty (34.9%) patients in whom PTMC was diagnosed after surgery were qualified for the operation due to thyroid goiter. In total, 39 (9.1%) lobectomies, 82 (19.1%) total thyroidectomies without central compartment lymphadenectomy, 293 (68.1%) total thyroidectomies with central compartment lymphadenectomy, and 16 (3.7%) total thyroidectomies with lateral compartment lymphadenectomy were performed. The range of operation depended on the known presence of PTMC, PTMC location, occurrence of thyroid nodules in the second lobe, fine-needle biopsy verified metastases to lymph nodes, and the presence of enlarged lymph nodes during operation.
In all cases, there were no cancers other than PTMC. Three (0.7%) patients were assessed as high risk for recurrent/persistent disease; all of them had large lymph node metastases (>3 cm in diameter). None of these patients had coexisting BRAFV600E and TERTC228T and/or TERTC250T mutations.
The genetic background of PTMC
The BRAFV600E mutation was present in 298 (69.3% [CI 64.7–73.6]) cases. In total, there were 41 TERT hotspot mutations: 28 (6.5%) cases with TERTC228T mutations and 13 (3.0%) with TERTC250T mutations. There were two cases (0.4%) with concomitant TERTC228T and TERTC250T mutations, and both had a coexisting BRAFV600E mutation. There were 29 (6.7% [CI 4.6–9.5]) patients in whom the TERTC228T and/or TERTC250T mutations coexisted with the BRAFV600E mutation. Ten (2.3%) cases had isolated TERTC228T mutations or TERTC250T mutations without BRAFV600E mutations. The data are presented in Table 2. TERT mutations other than hotspot C228T and/or C250T mutations were observed in 14 (3.3%) patients (Supplementary Table S1).
Characteristics of Genetic Alterations in Patients with Papillary Thyroid Microcarcinoma
BRAFV600E , B-type Raf kinas-activating mutation in codon 600 of exon 15; CI, confidence interval; TERT, telomerase reverse transcriptase.
All patients were divided into four subgroups according to the type of mutation: (A) BRAFV600E -negative and TERT C228T- and/or C250T-negative; (B) BRAFV600E -negative, but TERT C228T- and/or C250T-positive; (C) BRAFV600E -positive, but TERT C228T- and/or C250T-negative; and (D) BRAFV600E -positive and TERT C228T and/or C250T-positive. The characteristics of, and associations between TERT hotspot mutations and the BRAFV600E mutation, and their coexistence, is presented in Supplementary Table S2. Subgroup (A) and subgroup (D) were analyzed further.
Clinicopathological features and presence of mutations
Statistical comparisons between PTMC cases with concomitant TERT hotspot mutations and a BRAFV600E mutation, and those without any of these mutations, revealed no significant differences between the two with respect to sex, age at diagnosis, tumor diameter, histological variant, multifocality, vascular invasion, ETE, or pathologically confirmed lymph node metastases (Table 3).
Characteristics and Association Between Patients with Papillary Thyroid Microcarcinomas and Concomitant BRAFV600E Mutation and TERT Hotspot Mutations and Those Without Any of Those Mutations
PTC, papillary thyroid cancer.
Response to initial therapy and presence of mutations
Responses to initial treatment by all patients are presented in Table 4. One case (0.2%) showed an initial incomplete structural response due to regional lymph node metastases; after reoperation, the patient achieved an excellent response during final follow-up.
Characteristics of Patients with Papillary Thyroid Microcarcinoma During Treatment and Follow-Up
To facilitate an appropriate evaluation and comparison, patients from subgroup (A) and subgroup (B) were further divided into those who underwent surgery only, and those who underwent surgery with additional 131I treatment. There were no statistically significant differences in response to initial treatment between patients with a concomitant BRAFV600E mutation and TERT hotspot mutations and those without any of these mutations (Table 5).
Comparison Between Response to Initial Treatment in Papillary Thyroid Microcarcinomas Cases with Concomitant TERT and BRAFV600 E Mutations and Those Without Any of Those Mutations Which Underwent Operation With or Without Radioiodine (131I) Therapy
Recurrence and presence of mutations
Recurrence was observed in eight patients (1.9%). Five of these patients were assessed as intermediate-risk PTMC and three as low-risk PTMC. None of these patients had coexisting BRAFV600E and TERTC228T and/or TERTC250T mutations. Mean time to recurrence was 5.6 years. There were three cases (0.7%) of PTMC recurrence in the second lobe after initial lobectomy, two cases (0.5%) of lymph node recurrence on the side of the primary thyroid cancer, one case (0.2%) of PTMC recurrence in the thyroid bed on the side of primary thyroid cancer, and two cases (0.5%) of biochemical recurrence due to increasing thyroglobulin (Tg) serum concentration; in one of these cases, the level increased from an undetectable basal concentration to 4.6 ng/mL, and in the second case, the level increased from an undetectable stimulated Tg serum concentration to a stimulated Tg concentration of 2.8 ng/mL (after administration of recombinant TSH).
Both cases had negative images on ultrasonography and a diagnostic whole body scan. In the first case, the patient died from comorbid disease before further treatment. In the second case, a second radioiodine therapy was performed (the patient achieved NED).
Finally, after further treatment comprising reoperation (two patients with recurrence in the second lobe, two with lymph node recurrence and one with recurrence in thyroid bed), and/or radioiodine therapy (all patients after reoperation and one patient with biochemical recurrence), six of the eight patients with recurrence (1.4%) were evaluated as having an excellent response to therapy, whereas one (0.2%) patient failed to reported to our department, and one (0.2%) patient died from comorbid disease before further treatment, as stated earlier. Overall, the status of the recurrence was not affected by the presence of concomitant BRAFV600E and TERTC228T and/or TERTC250T mutations (Table 5).
Final clinical status and presence of mutations
Final responses to treatment in all patients are presented in Table 4.
The presence of BRAFV600E and TERT hotspot mutations (as compared with the absence of BRAF V600E and TERT hotspot mutations) was not associated with a final clinical outcome other than excellent (p = 0.6246, univariable OR: 0.59 [CI, 0.07–4.97]). The relation of PTMC course, depending on cancer diagnosis known before or after operation is presented in Supplementary Table S3. The analysis of patients with clinical nodal metastases is presented in Supplementary Table S4.
Discussion
The role of BRAFV600E and TERT hotspot mutations in PTMC is still unclear. However, the influence of these mutations on advanced PTC is well established, and both are more common in tumors with unfavorable clinicopathological features. TERT mutations are present mostly in older patients with advanced TNM stage, lymph node metastasis, ETE, or persistent and recurrent disease. 25 The most common TERT mutations in thyroid cancer are so-called hotspot mutations: mainly TERTC228T and TERTC250T ; the former is predominant regardless of the ethnic group. 26,27
However, data suggest that the overall rate of TERT hotspot mutations in PTMC can vary between different countries. An Italian multicenter study by de Biase et al found TERT hotspot mutations in about 4.7% of PTMC cases. 28 Markedly fewer TERT hotspot mutations in PTMC were reported in Korean and Japan studies, in which the prevalence of these mutations was 1.0% or even lower. 29,30 In this study, we found that TERT hotspot mutations were more common (9.1%). However, this can be attributed (partially) to the overall higher mean age of the patients enrolled in our study (52.4 and 48.9 years for TERT-positive and TERT-negative patients, respectively, compared with 50.2 and 47.8 years, respectively, in the Italian study). 28
In addition, the median age for TERT-positive patients in our study was 53 years. In our study, 10/430 (2.3%) cases had isolated TERTC228T or/and TERTC250T mutation without BRAFV600E mutation. Even higher proportion of isolated TERT promoter mutations were published by Parvathareddy et al, which show that about 3.3% of PTMC cases had only TERTC228T or TERTC250T mutation without BRAFV600E mutation. 31 Eventually, the ratio between TERTC228T and TERTC250T mutations can vary significantly depending on study and population even in PTC, which together with little data regarding the overall presence of those mutation in PTMC, makes it hard to compare our results with other studies. 32
In addition, the rate of TERT hotspot mutations in Polish patients with PTC, regardless of tumor size, is usually greater than that reported in larger studies (13.5% vs. 12.0%, respectively). 24,25,33
These data show that acquisition of a TERT promoter mutation is mainly a late genetic event that takes place during PTC development; thus, these mutations are very uncommon in small DTC (such as PTMC) or benign thyroid tumors. 28,32,34 By contrast, early genetic events during thyroid cancer initiation and progression involve activation of a BRAF mutation, particularly at codon 600, which results in a BRAFV600E mutation due to a thymine-to-adenine transversion in exon 15. 35,36 This mutation represents more than 90% of all BRAF mutations and is present widely in PTC. 34 The high prevalence of the BRAFV600E mutation in PTC, coupled with the usually mild course, mean that the role of the BRAFV600E mutation as a prognostic marker in its own right is still uncertain. 37,38
Overall, the BRAFV600E mutation is present in about 60.6% of PTC cases and in 47.48% of PTMC cases. 39,40 Data suggest that PTC with a positive BRAFV600E status is associated with multifocality, ETE, lymph node metastases, and more aggressive clinical features (even for PTMC). 37,41 However, other data show that the relationship between the presence of the BRAFV600E mutation and the status of central lymph nodes, without considering other clinicopathological features, is not clear. 42 Furthermore, observations from long-term follow-up of PTMC cases at our center show that the presence of BRAFV600E in tumors without diagnosed lymph node metastases is not associated with aggressive or recurrent disease. The prevalence of the BRAFV600E mutation in this group was 69%, which indicates that the presence of this mutation in low-risk PTMC has a doubtful impact on an unfavorable disease course. 39
Coexisting BRAFV600E and TERT mutations act cooperatively in PTC to increase the risk of recurrence; tumors that are positive for both mutations have recurrence rates of about 68.6%, compared with 8.7% for tumors with neither the BRAFV600E nor the TERTC228T mutation. 33 This observation, and the relationship between these two genes, can be explained by their synergistic role at the molecular level. Somatic mutations in the TERT promoter lead to reactivation of telomerase, which inhibits aging and apoptosis of neoplastic cells by protecting the chromosome ends from shortening. 43,44
In addition, both TERT hotspot mutations create 11 base pair (bp) sequence “CCCGGAAGGGG,” which greatly mimics binding motif of E-twenty six (ETS) transcription factor family and leads to increased TERT gene transcription. This process is further augmented by, related to BRAFV600E mutation presence, activation of mitogen-activated protein kinase pathway, which upregulates ETS transcription factors. 44 –47 This proposed genetic pathway has not been confirmed, but increased TERT expression can be observed in thyroid cancer with coexisting BRAF and TERT mutations. 44
Despite the large number of studies acknowledging the potent role of coexisting BRAF and TERT mutations in poor thyroid cancer outcomes, there are few that have examined the potential role of these mutations in PTMC. This may be due to the fact that only a small number of PTMCs harbor TERT hotspot mutations compared with the commonly observed BRAFV600E mutation. 29
de Biase et al reported that concomitant BRAFV600E and TERT hotspot mutations are present in about 3.43% (13/379) of patients with PTMC, and that they correlate positively with tumor size (pT) and advanced lymph node metastases (pN), and inversely with multifocality. However, coexistence of those mutations did not affect the clinical outcome when compared with the rest of patients with PTMC. 28 A recent study by Lee et al shows that coexisting BRAFV600E and TERT hotspot mutations in PTMC are related neither to an unfavorable clinicopathological features nor to lymph node metastasis. 15
However, the study included only newly diagnosed patients with a relatively short-term follow-up; also, they were not assessed in terms of initial therapy response. In addition, data show that even in low-risk PTMC with neither structural nor functional evidence of disease at the initial post-treatment examination, recurrence can be observed (although very rarely) even after a few years. 9 In our study, we observed PTMC recurrence at 10.25 years post-NED in a patient without concomitant BRAFV600E and TERT hotspot mutations.
In this study, we show that the presence of concomitant BRAFV600E and TERT hotspot mutations is not related to unfavorable clinicopathological features, a worse response to initial therapy or a worse clinical outcome when compared with patients without these mutations.
Nonetheless, the small number of patients with concomitant BRAFV600E and TERT hotspot mutations from a single referential center, although with relatively long-term follow-up, is the main limitation of this study. In addition, the retrospective nature of our research has potential for that is convenience sampling.
Conclusion
The BRAFV600E mutation is common in PTMC, whereas TERT mutations are rare; thus, coexistence of these mutations, especially in small tumors, in an exceptional genetic event. However, regardless of the PTMC molecular background, the overall response to therapy is excellent, and long-term disease-free survival can be achieved by most patients, even those with concomitant TERT hotspot and BRAFV600E mutations. All this makes an active surveillance in low-risk PTMC a valid option, especially in older patients and those with comorbidities. However, the small number of patients with PTMC harboring concomitant BRAFV600E and TERT hotspot mutations means that further studies are needed to confirm our findings.
Footnotes
Authors' Contributions
Conceptualization, data curation, and supervision by A.K. (Artur Kuchareczko), S.G., and A.K. (Aldona Kowalska); methodology and formal analysis by A.K. (Artur Kuchareczko), J.K., A.K. (Artur Kowalik), K.H.-N., A.P., M.C., and A.K. (Aldona Kowalska); validation by A.K. (Artur Kowalik), K.H.-N., and M.C.; software by A.K. (Artur Kuchareczko) and M.C.; investigation by J.K., A.K. (Artur Kowalik), K.H.-N., and A.P.; writing—original draft preparation and project administration by A.K. (Artur Kuchareczko) and A.K. (Aldona Kowalska); writing—review and editing and resources by A.K. (Artur Kuchareczko), J.K., A.K. (Artur Kowalik), K.H.-N., A.W., I.P., T.T., M.S., D.G.-P., K.G.-J., E.M., I.P., A.S., A.P., M.C., T.Ł, S.G., and A.K. (Aldona Kowalska); funding acquisition by S.G. and A.K. (Aldona Kowalska). All authors have read and agreed to the published version of the article.
Author Disclosure Statement
All the authors have nothing to disclose.
Funding Information
The project was financed under the program the Minister of Education and Science called “Regional Initiative of Excellence” in the years 2019–2022, project no. 024/RID/2018/19, amount of financing 11 999 000,00 PLN. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article; or in the decision to publish the results.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4