
Abstract
Background:
Thyroid eye disease (TED) involves several pathogenic pathways and a battery of infiltrating mononuclear cells, cytokines, and chemokines in the orbit. Revealing the main molecules, which play a major role in the pathogenesis of TED, will help developing novel treatment strategies.
Methods:
In a multicenter, single-blind, case-control study, 60 tissue samples were collected during orbital decompression (44 TED patients) or non-TED related oculoplastic (16 controls) surgeries. Formalin-fixation and paraffin embedding preserved orbital tissue. Tissue sections were immunostained with 18 antibodies by the micro-polymer labeling technique. Immunostaining slides were scanned by Panoramic Desk and blindly evaluated by a user-independent viewer software.
Results:
Marked lymphocyte infiltration was observed in orbital tissue specimens of patients with clinically active TED (n = 22) and to a much lesser extent in inactive cases (n = 22), while it was absent in controls. Increased vascularity was noted in all samples, with orbital congestion in specimens of clinically active TED. Tissue fibrosis was present in TED samples but not in controls. Immunohistochemistry of orbital tissue clearly differentiated between TED and controls, as well as between active and inactive TED. In contrast to controls and with the exception of cluster of differentiation 20 (CD20), 17 out of 18 antibodies were highly expressed in orbital connective tissue of TED patients. Especially, thyrotropin receptor (TSH-R), insulin-like growth factor 1 receptor (IGF-1R), CD40, cluster of differentiation 40 ligand (CD40L), CD3, CD68, interleukin-17A (IL-17A), IL-23A, IL-1β, IL-4, regulated on activation, normal T cell expressed and secreted (RANTES), macrophage chemoattractant protein 1 (MCP-1), IL-16, and B cell activating factor (BAFF) were overexpressed in clinically active TED (all p < 0.001). Also, the expression of CD40L, IL-17A, IL-23A, IL-6, IL-1β, RANTES, and BAFF was very high (TED/control ratio >3), moderate (ratio >2), and low in active (p < 0.001), inactive TED and controls, respectively. The expression of TSH-R, IGF-1R, CD40, CD40L, CD3, CD68, CD20, IL-17A, IL-23A, RANTES, MCP-1, and BAFF positively and significantly correlated with both serum TSH-R stimulatory antibody concentrations and clinical activity scores while it negatively correlated with TED duration. Orbital irradiation decreased TSH-R (p < 0.001) and IGF-1R expression (p = 0.012); in contrast, neither smoking, age, nor gender did impact immunohistochemical staining.
Conclusions:
Adaptive and cell-mediated immunity, overexpression of TSH-R/IGF-1R and CD40/CD40L are the relevant pathomechanisms in TED. Targeting these key players in the active phase of the disease offers specific and novel treatment approaches.
Introduction
Autoimmune-induced thyroid eye disease (TED) is the most common extra-thyroidal manifestation of Graves' disease (GD). 1,2 The pathological process of TED includes orbital inflammation and edema, adipogenesis leading to expansion of orbital tissue, tissue remodeling, and fibrosis. 3,4 Undrained interstitial fluid released from new blood vessels may also induce local edema in acute TED. 5 The orbital tissue is infiltrated by activated T and B cells, which produce pro-inflammatory cytokines depending on which molecular signals they encounter in the microenvironment.
These cytokines activate orbital fibroblasts (OF) as target effector cells inducing proliferation and differentiation. 6 The OF-mediated interaction with infiltrating immunocytes produces several chemokines and cytokines enhancing overexpression of the thyrotropin receptor (TSH-R) 7 and insulin-like growth factor 1 receptor (IGF-1R), hence entertaining local inflammation. 8
T cell mediated immunity contributes to TED development. 9 Type 1 helper T cells (Th1) predominate in the early stage, with Th2 in the latter inactive phase. 9,10 Th17 cells (CD4+ T cell subset) participate in the adaptive immune response. Interleukin-17 (IL-17) is a cytokine secreted both by Th17 cells as part of the adaptive immune response and by cells of the innate immune response (e.g., neutrophils). 11 –13 IL-17A is increased in the serum of TED subjects. 14
IL-17A and its related cytokines (IL-23A, IL-6, IL-1β) induce the differentiation of pathogenic Th17 cells from naive T cells and the maintenance of effector Th17 cells. 11,12,15 Chemokines, that is, regulated on activation, normal T cell expressed and secreted (RANTES), and the macrophage chemoattractant protein-1 (MCP-1) facilitate lymphocyte trafficking into the orbit. 16,17 In addition, interactions between OF and T cells as well as CD40/cluster of differentiation 40 ligand (CD40L) signaling within the immunological synapse are pivotal to TED pathogenesis. 16
Immunohistochemical analysis of human orbital tissue uncovers the local orbital immunity and correlates microscopic changes with macroscopic clinical manifestations of TED. 18 A recent systematic analysis highlighted numerous methodological limitations of immunohistochemical reports published in the past three decades, including small to very small sample size, 19 subjective user-dependent evaluation, and missing differentiation in clinical stages of TED. 20 Therefore, within a multicenter controlled design, using a well-documented large orbital tissue sample size, we aimed at blindly evaluating the immunohistochemical expression of potentially relevant players in TED pathogenesis with the help of an accurate user-independent software program and without any prior available clinical information.
Materials and Methods
Ophthalmic and endocrine assessment
Clinical activity and severity of all TED patients were defined according to the European Society of Endocrinology endorsed 2021 guidelines of the European Group on Graves' Orbitopathy (EUGOGO) for the management of TED. 1 Clinical and serological evaluation of the autoimmune-induced thyroid dysfunction followed the guidelines of the European Thyroid Association for the management of GD. 21,22
Collection and preparation of orbital tissue
This case-control study followed the declaration of Helsinki, was approved by the local ethical committees and/or IRB, and all patients gave their written consent. Forty-four unselected, consecutive orbital tissue specimens were collected from TED patients undergoing emergent or rehabilitative orbital decompression surgery at the Department of Ophthalmology, JGU Medical Center, Mainz, Germany (Supplementary Fig. S1). In comparison, 16 orbital tissue specimens were collected either at the Department of Ophthalmology, Ninth People's Hospital, Shanghai, China, during blepharoplasty (n = 15), or during surgery for orbital trauma at JGU (n = 1) from subjects devoid of autoimmune orbital and/or thyroid disease and served as controls. Orbital tissues were immediately put into liquid nitrogen after surgical removal and then frozen at −80°C. The rough tissues were thawed at room temperature for 30 minutes before being fixed in formalin overnight and then embedded in paraffin. Two-micrometer-thick tissue sections were cut by a microtome.
Immunohistochemistry
For immunohistochemical staining, we used a micro-polymer labeling technique (Mouse and rabbit-specific HRP/3,3′-diaminobenzidine [DAB] IHC detection Kit, ab236466; Abcam, UK), including hydrogen peroxide block, protein block, mouse specifying reagent (complement), goat anti-rabbit HRP-conjugate, DAB chromogen, and DAB substrate. The primary antibodies (Supplementary Table S1) were as follows: (1) CD3 (1:20; polyclonal; cat. no. PA5-32318), (2) cluster of differentiation 20 (CD20) (1:20; polyclonal; cat. no. PA5-16701), (3) CD40 (1:20; polyclonal; cat. no. PA5-32325), (4) IL-17A (1:50; polyclonal; cat. no. PA5-79470), (5) interferon gamma (IFN-γ) (1:50; polyclonal; cat. no. PA5-95560), (6) MCP-1 (1:100; polyclonal; cat. no. PA5-80413), (7) transforming growth factor beta (TGF-β) (1:30; monoclonal; cat. no. MA523795), (8) CD68 (1:50; monoclonal; cat. no. 14-0689-82), (9) B cell activating factor (BAFF) (1:50; monoclonal; cat. no. 14-9017-82), (10) RANTES (1:50; monoclonal; cat. no. AHC1052), (11) TSH-R (1:100; monoclonal; cat. no. MA528136), and (12) IL-16 (1:200; monoclonal; cat. no. MA529348).
The 12 antibodies cited earlier were purchased from Thermofisher Scientific, USA. (13) IL-1β (1:50; monoclonal; cat. no. 66737-1-Ig), (14) IGF-1R (1:100; monoclonal; cat. no. 66502-1-Ig), (15) CD40L (1:100; monoclonal; cat. no. 66238-1-Ig), (16) IL-4 (1:400; monoclonal; cat. no. 66142-1-Ig), (17) IL-6 (1:500; monoclonal; cat. no. 66146-1-Ig), and (18) IL-23A (1:500; monoclonal; cat. no. 66196-1-Ig) were purchased from Proteintech, Germany. Two-micrometer-thick sections were deparaffinized in 100% xylene two times for 5 minutes each at room temperature, then rehydrated in 100%, 95%, 75% isopropanol two times for 1 minute each, respectively.
Slides were washed in phosphate-buffered saline (pH 7.4). Epitope retrieval was used in retrieval solutions (1% citrate buffer, pH 6.0 in PBS) for 20 minutes under a pressure cooker at 100°C, and it was cooled down at room temperature for 20 minutes. Hydrogen peroxide block and protein block were used to avoid non-specific background staining according to the manufacturer's instructions. Slides were incubated with primary antibodies diluted in antibody diluent (TA-125-ADQ; Thermo Scientific) at room temperature for 1 hour.
Mouse specifying reagent (complement) and goat anti-rabbit HRP-conjugate were used as secondary antibodies, and slides were incubated according to the manufacturer's instructions. Chromogen detection was performed with DAB reagent (30 μL DAB chromogen was added to 1.5 mL of DAB substrate) for 10 minutes. Slides were counterstained in hematoxylin for 3 minutes. For negative control, the primary antibodies were omitted, and antibody diluent was used instead.
Assessment
Immunostaining slides were scanned by Panoramic Desk and evaluated by the user independent Panoramic Viewer software version 1.15.2 DensitoQuant (3DHistotech Ltd., Budapest, Hungary). An application identifies the positive stain, based on an automatic color separation method through which individual positive pixels are counted and classified based on intensity and threshold ranges (brown color indicated positive staining, while blue counterstaining alone indicated negative staining). Quantification (percentage of positivity) was calculated by dividing the ratio of all positive cells to the total number of cells found in each of six independently annotated orbital tissue areas.
The evaluation method was selected for six interesting areas of orbital connective tissue (OCT) and orbital adipose tissue (OAT), respectively, in each slide (Supplementary Fig. S2). Subsequently, the same parameter of the DensitoQuant software was used to evaluate all slides, which were stained by the same antibody and following the software instructions to calculate the percentage of positivity. After defining the percentages of positivity of six areas from OCT and OAT, the mean value of six areas was calculated as protein expression of the corresponding sample.
As long as the same parameter is used, all values are reproducible, independent of the operator, allowing for an automated, quick, and unbiased analysis antibody expression. Immunohistochemical staining was done exclusively before unblinding demographic, serological, and clinical data, diagnosis, duration of TED and GD, activity and severity of TED, specific treatments, for example, steroids and/or orbital irradiation, time interval between medical therapy and orbital surgery, smoking habits, etc.
Statistical analysis
We used the Statistical Package for the Social Sciences software program (version 26). Two groups of TED patients and controls were analyzed by independent sample t tests whether data were normally distributed and with non-parametric tests (Mann Whitney U Test) in case of skewed distributions. For comparing three different groups of clinically active versus inactive TED and control, a one-way ANOVA test was used in case of equivariance while non-parametric tests (Kruskal-Wallis, one-way ANOVA) were used, if skewed distributions were present. Significance levels of p < 0.05 were considered as statistically significant. Graphs were made by Prism (version 9).
Results
Demographic, clinical, and serological data
Demographic, clinical, and serological data are presented in Table 1. Orbital tissue was obtained from 44 consecutive patients with TED of various clinical activity and severity stages. Sixteen euthyroid subjects devoid of autoimmune, thyroidal, and endocrine diseases served as controls. Most TED patients were women. Before orbital surgery, all patients were treated with intravenous methylprednisolone pulses according to the EUGOGO guideline recommendations, and 12 with inactive disease previously received orbital irradiation for diplopia.
Demographic, Clinical, and Serological Data
Data are presented as median and 25th/75th percentiles (Q1/Q3) or N (%). The thyroid-related hormones (Abbott TSH Alinity i Reagent kit; Abbott Ireland, Longford, Ireland) and antibodies (Thyretain® TSI; Quidelortho Corp., San Diego, CA, USA) were measured according to the manufacturer's instructions.
N, number; NA, not available; SRR, specimen to reference ratio; steroid-surgery interval, the interval time between steroid administration and orbital decompression surgery; TED, thyroid eye disease.
Orbital decompression surgery was performed in patients with inactive TED mostly for cosmetic purposes, as a decrease of proptosis subsequent to anti-inflammatory treatment was not satisfactory. Ten patients with active TED had orbital surgery because of acute exacerbation of eye signs and development of compressive optic neuropathy. At orbital surgery, all patients with active TED and 14 with inactive TED were on methimazole therapy and biochemically euthyroid (serum thyrotropin and free T4 within the normal range), while eight patients with inactive TED were off anti-thyroidal medication and in remission. Serum thyroid stimulating immunoglobulins differentiated active from inactive TED (p < 0.001).
Histopathology
Eighteen primary antibodies were evaluated in orbital tissue slices using immunohistochemistry. Compared with control, a significant proliferation of connective tissue was increased in TED orbital tissue samples. Focal lymphocytic infiltration was observed in active specimens and to a much lesser extent in inactive cases and those with a longer disease duration, while it was absent in control tissue. Increased vascularity was noted in all samples, most specifically in active tissue with shorter disease duration and severe phenotype (orbital congestion). Tissue fibrosis was present, mostly in patient samples with severe and active disease, but not in controls.
Immunohistochemical analysis of OCT
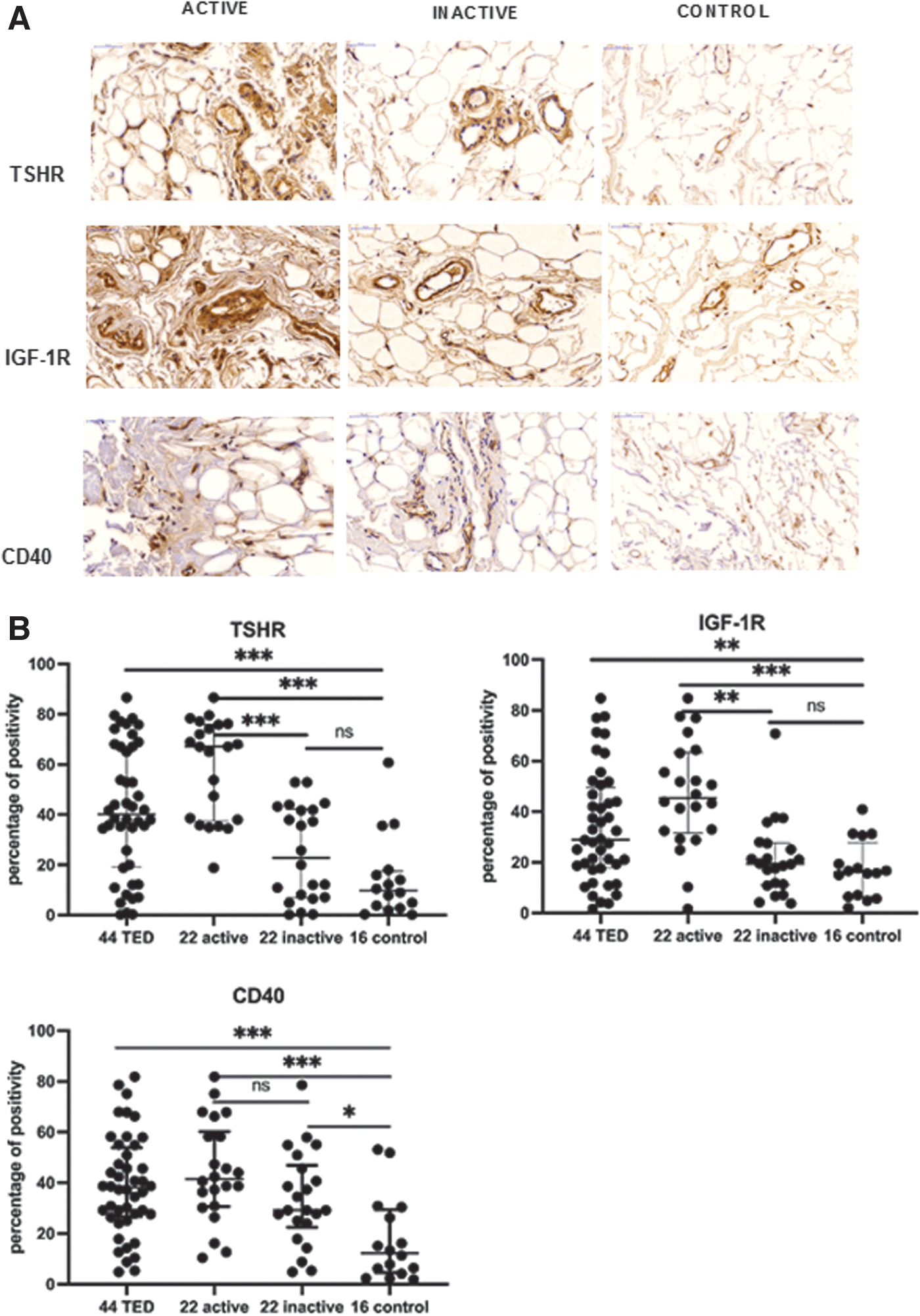
In contrast to controls, 17 out of 18 antibodies, that is, TSH-R (p < 0.001), IGF-1R (p = 0.004), CD40 (expressed on antigen-presenting cells, OF, and B cells, p < 0.001), CD40L (expressed on T cells, p < 0.001), CD3 (T cells, p = 0.001), CD68 (macrophages, p < 0.001), RANTES (p < 0.001), and MCP-1 (p = 0.005), both chemokines, which attract T cells and macrophages into the orbit, IL-23A (p < 0.001) and IL-17A (p < 0.001) as signature cytokines of the adaptive immune response (innate immunity), IL-6 (p < 0.001), IL-1β (p < 0.001), IFN-γ (Th1 cytokine, p = 0.002), IL-4 (Th2 cytokine, p < 0.001), IL-16 (p < 0.001), BAFF (p < 0.001), and TGF-β (p = 0.002) were highly expressed in OCT of TED patients.
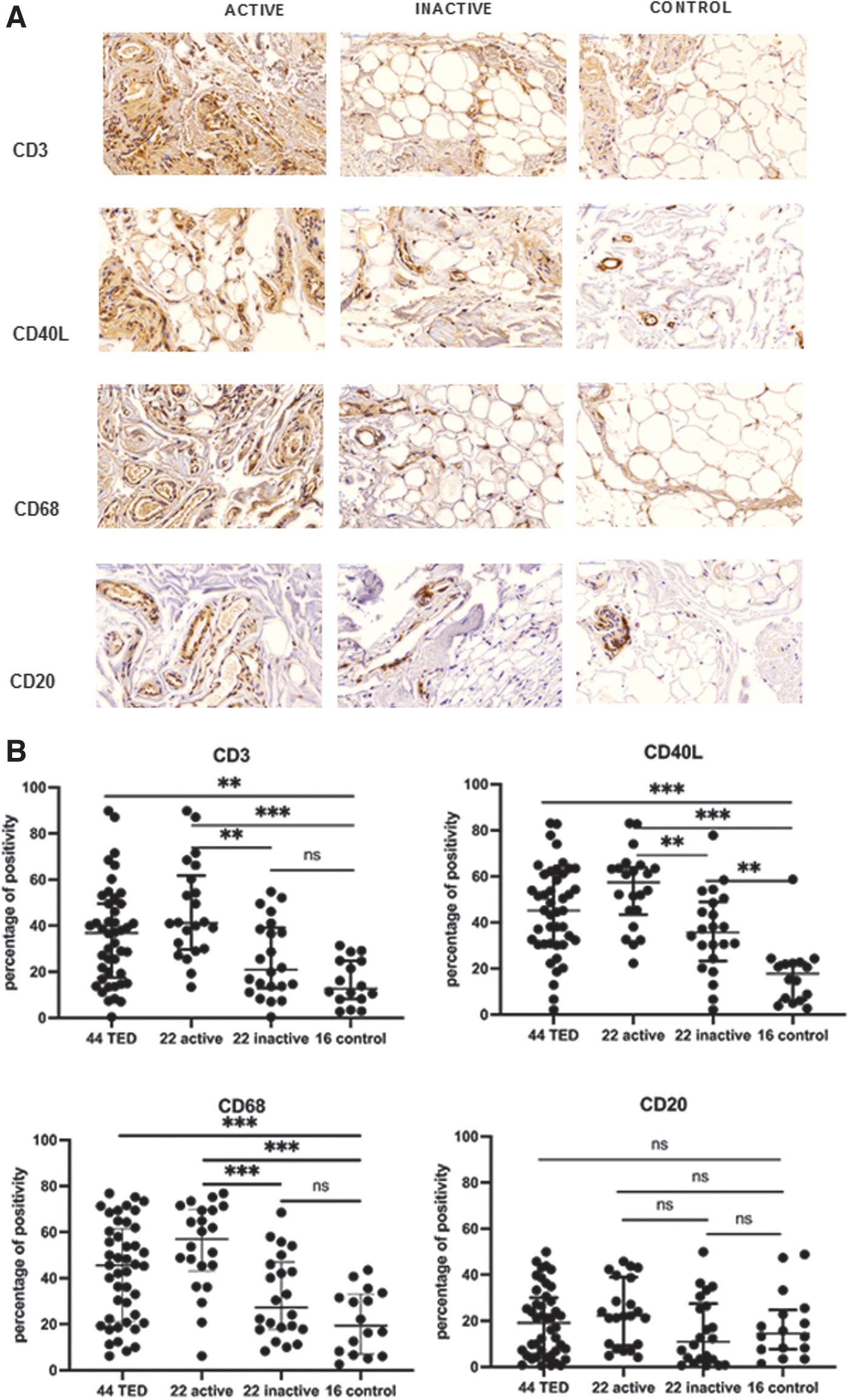
The TSH-R and IGF-1R (Fig. 1) were overexpressed in clinically active (both p < 0.001) and in inactive TED (p < 0.001 and p = 0.001), but not in control tissue. CD40 was overabundant in both active (p < 0.001) and inactive TED, but not in controls. Expression of CD40L, CD3, and CD68 (Fig. 2) was very high (patients vs. control ratio >3, p < 0.001), moderate (ratio >2), and low in active, inactive TED and control tissue, respectively. Mild-to-moderate B cell infiltration (CD20) was not different in active, inactive TED or controls (p > 0.05; Fig. 2).
Panel (
Panel (
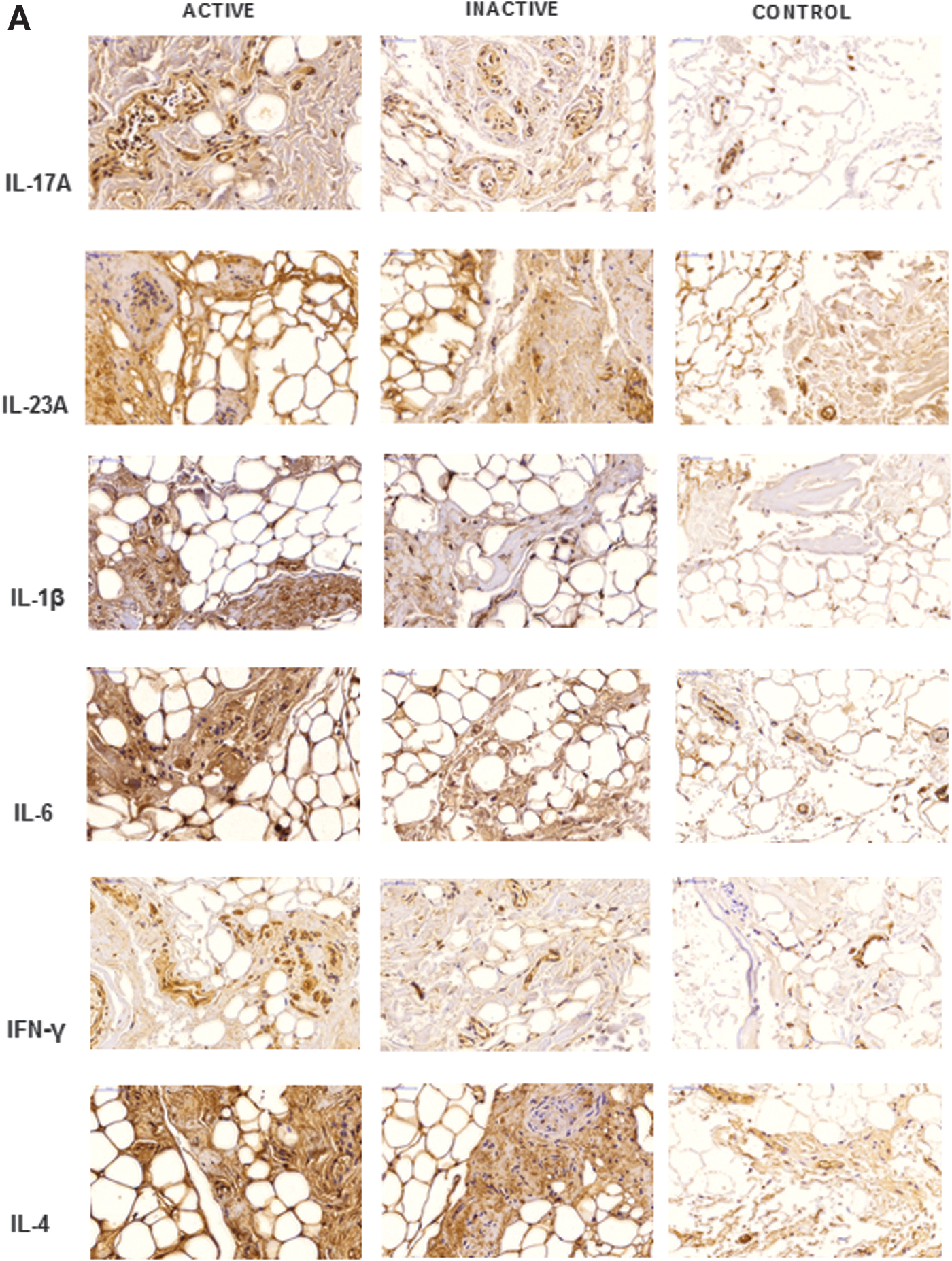
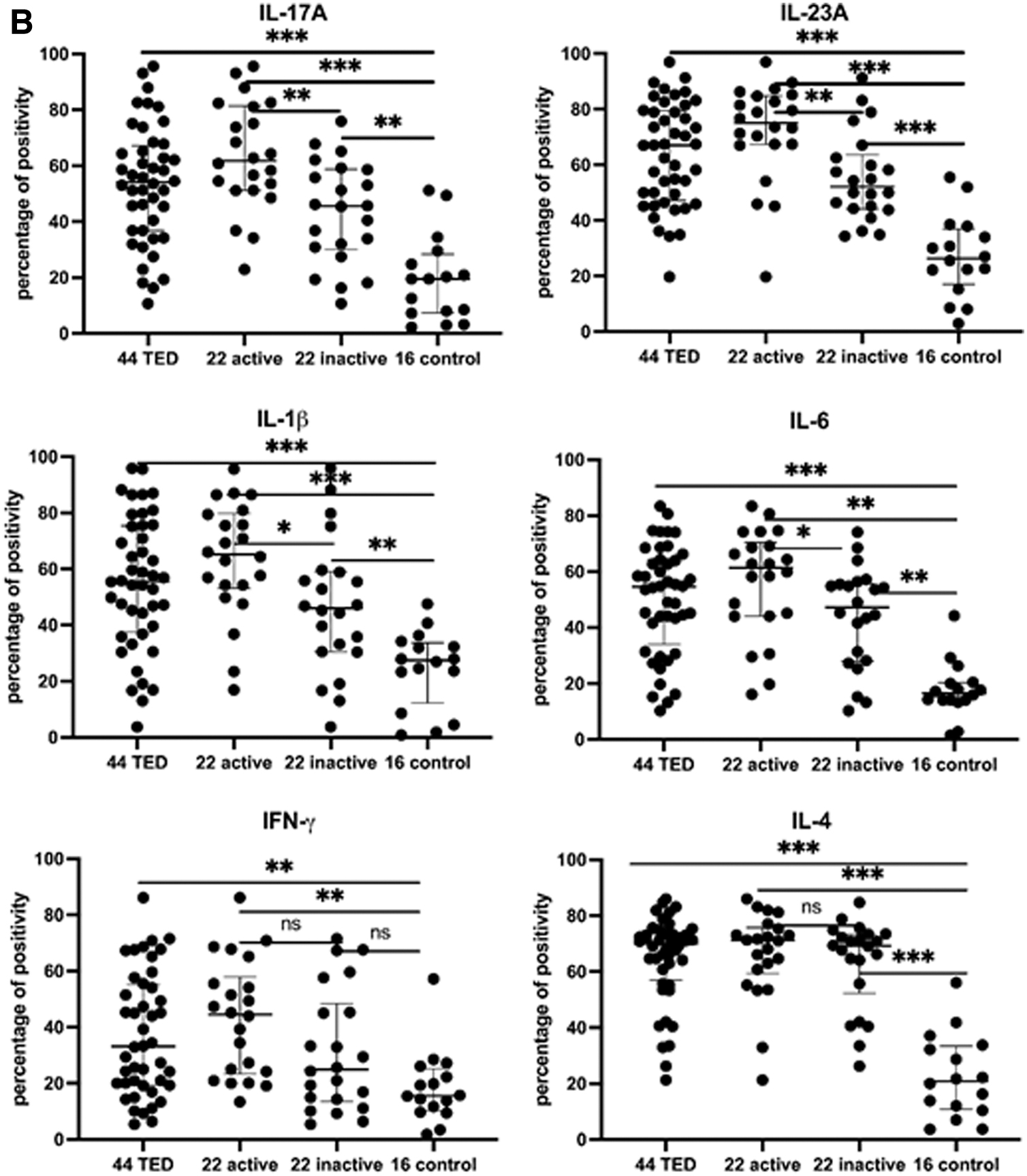
Expression of IL-23A and IL-17A (adaptive immune response; Fig. 3), IL-6, IL-1β, was very high (patients vs. control ratio >3, p < 0.001), moderate (ratio >2), and low in active, inactive TED and control tissue, respectively. IFN-γ (Th1 cytokine) was overexpressed in TED (p = 0.002), especially in active tissue (p = 0.001) while IL-4 (Th2 cytokine) was overabundant in both active (p < 0.001) and inactive TED, but not in controls (Fig. 3).
Panel (
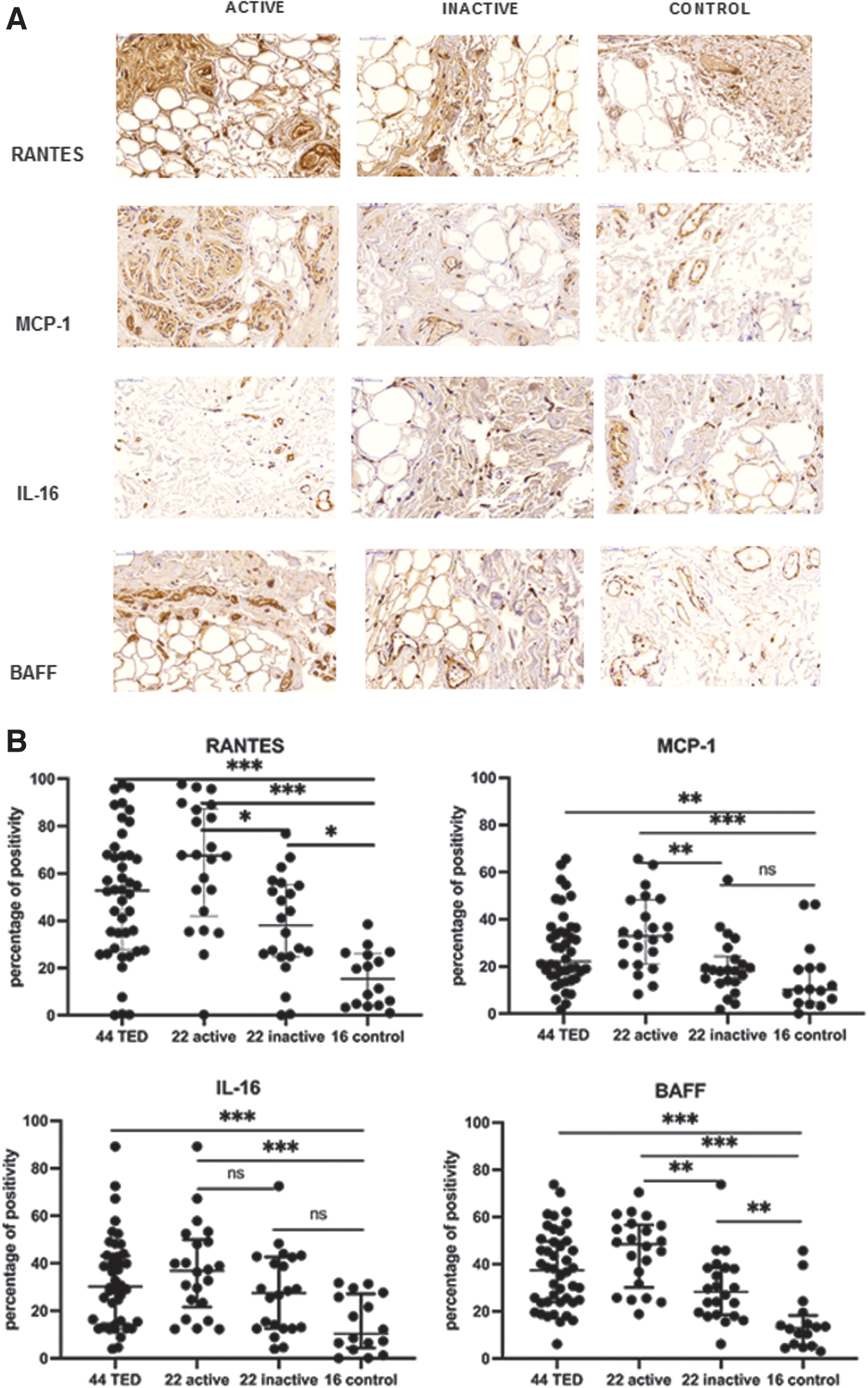
Expression of RANTES, MCP-1, and BAFF (Fig. 4) was very high (patients vs. control ratio >3, p < 0.001), moderate (ratio >2), and low in active, inactive TED and control tissue, respectively. IL-16 (p < 0.001) and TGF-β (p = 0.003) were overabundant in active but not in inactive TED and control. The magnitude of positive staining of the 18 antibodies tested in the OCT of patients with TED in general, inactive, and active disease in particular, as well as controls is shown in Table 2.
Panel (
Immunohistochemical Staining of Orbital Connective Tissue Collected from Patients with Thyroid Eye Disease and Control Subjects
Data are presented as median values and 25th, 75th percentiles (Q1, Q3). Significance values: p1, TED vs. control; p2, active TED vs. control; p3, active vs. inactive TED; p4, inactive TED vs. control. Multiplicity of analyses is explicitly accounted for in the analysis plan, and Table 2 encompasses statistically corrected p-values only. In detail, in the case of equivariance to compare the various groups, we have used a one-way ANOVA test followed by a Bonferroni's post hoc test. If skewed distributions were present, we applied non-parametric tests (Kruskal-Wallis, one-way ANOVA) followed by a Bonferroni's post hoc test.
BAFF, B cell activating factor; CD, cluster of differentiation; IFN-γ, interferon gamma; IGF-1R, insulin-like growth factor 1 receptor; IL, interleukin; MCP-1, monocyte chemoattractant protein 1; RANTES, regulated on activation, normal T cell expressed and secreted; TGF-β, transforming growth factor beta; TSH-R, thyrotropin receptor.
Immunohistochemical analysis of OAT
Compared with connective tissue, OAT showed a variable, rather moderate immunostaining versus controls (Table 3) with overexpression of TSH-R (p = 0.018), IGF-1R (p = 0.011), CD40 (p = 001), CD40L (p = 0.024), CD3 (p < 0.001), IL-23A (p = 0.001), IL-17A (p = 0.001), IL-1β (p < 0.019), IL-6 (p < 0.001), IL-4 (p < 0.001), and BAFF (p < 0.001) in tissues from clinically active TED versus inactive TED and/or control.
Immunohistochemical Staining of Orbital Adipose Tissue Collected from Patients with Thyroid Eye Disease and Controls
The expression of CD3 (T cells) was strong in active TED, moderate in inactive TED, and mild-to-absent in controls. The chemokine RANTES (p = 0.030) was overexpressed in active TED tissue only but not in controls. Neither CD68 (macrophages) nor MCP-1 was significantly increased in TED adipose tissue versus control.
Correlations
The expression of TSH-R, IGF-1R, CD40, CD40L, CD3, CD68, CD20, IL-17A, IL-23A, RANTES, MCP-1, and BAFF positively and significantly correlated with both serum functional TSH-R stimulatory antibody concentrations and clinical disease activity scores while it negatively correlated with TED duration (Supplementary Table S2). Neither gender, age (Supplementary Table S3), nor smoking (Supplementary Table S4) did impact immunohistochemical staining. However, orbital irradiation decreased TSH-R (p < 0.001) and IGF-1R expression (p = 0.012), but not the infiltration of immune mononuclear cells (T and B cells, macrophages) in the orbital tissue.
Discussion
To the best of our knowledge, this is the largest immunohistochemical study of orbital tissue evaluating in a blinded design tissue specimens from patients with TED of variable degrees of clinical activity, severity, and disease duration with the help of a standardized user-independent software program. To minimize subjective evaluation, we have used several approaches (blinded investigation, user independent software, analysis of morphology and staining before any unblinding of diagnosis, demographic and clinical data, activity and severity of the disease, etc.).
Subsequent to completion of immunohistochemical analysis of a large battery of antibodies targeting candidate key players in TED, a correlation analysis with ophthalmic and clinical data was done. We observed that both TSH-R and IGF-1R as well as the CD40 molecule and its ligand CD40L were overexpressed in TED samples when compared with controls. Their immunoreactivity was also significantly more abundant in active versus inactive TED, and this has not been reported in previous immunohistochemical studies.
Also novel is the fact that the expression of the key autoantigens TSH-R and IGF-1R positively and significantly correlated with both serum concentrations of the disease-specific thyroid stimulating immunoglobulins and the clinical activity score of TED. In line with this, disease duration negatively correlated with the expression of both autoantigens. Increased IGF-1R expression has also been reported in non-inflammatory TED. 23 TSH-R is the principal autoantigen in the pathogenesis of TED, and it forms a physical an16d functional complex with the IGF-1R. 24 –28 The stimulation of TSH-R activates two signal transduction pathways, one being IGF-1R independent and the other IGF-1R dependent (i.e., TSH-R/IGF-1R crosstalk pathway with β-arrestin 1 acting as a scaffold).
Both pathways cooperate, resulting in more intense activation of OF. 2,27 The US Food and Drug Administration has approved Teprotumumab, an anti-IGF-1R inhibiting monoclonal antibody, for the treatment of active/severe TED in view of its efficacy demonstrated in clinical trials. 29 –32 As stimulatory TSH-R-Ab is both the specific biomarker and the major pathogenic autoantibody of GD and related TED, 22,33 –37 TSH-R blocking monoclonal antibodies (K1-70) and small molecule TSH-R antagonists also hold great promise for the management of TED. Indeed, K1-70 therapy markedly reduced the stimulatory TSH-R-Ab activity and significantly improved the clinical phenotype in a patient with TED. 38
The observed marked tissue infiltration of T cells, macrophages, and the chemokines (RANTES and MCP-1) in tissues from active TED emphasizes the relevant roles of cell-mediated immunity 39,40 and macrophages 41 as key players in the early inflammatory phase of the disease, and it confirms the findings from our previous report. 18 Indeed, T cells and macrophages were the main infiltrating immunocytes in the inflammatory stage of TED but were reduced in the inactive stage. IFN-γ is the signature cytokine expressed by Th1 cells, whereas IL-4 secretion is a signature of Th2 cells.
In our samples, IFN-γ expression was markedly increased in TED tissue in general, and in active TED in particular when compared with inactive TED. This is consistent with the findings from a recent Italian monocenter study reporting positive correlation between orbital T cell infiltration and CAS. 42 In comparison, in the present work, only very few tissue samples showed B cell infiltration and we did neither observe significant differences between TED and control tissue nor between active and inactive TED. The lack of difference in B cell infiltration but significant difference in BAFF among active TED/inactive TED/controls can be explained by the received steroid medication.
RANTES is a C-C chemokine released by activated OF and it results in T cell migration into the orbit, thus sustaining local inflammation during the active stage. 4,43 OF also secrete MCP-1, a major chemokine that regulates migration and infiltration of monocytes/macrophages. 44 An in vitro study suggested that OF displayed robust induction of MCP-1 on retinoid treatment via an NF-κβ dependent mechanism. 45 Our immunohistochemical analysis demonstrated for the first time overexpression of MCP-1 in TED OCT (especially in active TED).
Interestingly, positive staining of macrophages and MCP-1 highly correlated, which indicates that MCP-1 plays a major role in TED by inducing migration of monocytes/macrophages into the orbit during the early stages of disease.
As anticipated in our previous review 20 and based on the current results, the adaptive immune response (“innate” immunity) with the substantial overexpression of both IL-23 and IL-17 in TED OCT seems to be heavily involved during the active phase of TED. IL-17 is a cytokine secreted both by Th17 cells as part of the adaptive immune response and by cells of the innate immune response, for example, by neutrophils. 11,13 IL-23A, which is produced by dendritic cells and macrophages, plays a major role in autoimmune diseases by keeping the differentiation of Th17 and increasing the production of IL-17A. 46
Further, the pro-inflammatory cytokine IL-6 stimulates the differentiation of naive T cells into Th17 cells, while IL-23A maintains the production of IL-17A by Th17 cells. 11 IL-6, which also promotes TSH-R expression in TED OF, 47 was highly expressed in our active TED samples but not in inactive and control samples. IL-17A stimulates the differentiation of into pre-adipocytes and myofibroblasts, 15 and both IL-17A and IL-23A as well as IL-6 stimulate OF to secrete hydrophilic glycosaminoglycans. 48 IL-17A also promotes RANTES expression in OF via CD40-CD40L combination in TED, 17 hence enhancing monocyte migration into the orbit and maintenance/amplification of immune-induced local inflammation.
The potential limitations of this study are: (1) patients and controls were enrolled from different populations; (2) no comparison was done between pre- and post-medical treatment, as steroid therapy could have modified immunohistochemical pattern to a certain extent; and (3) 12 patients with inactive TED received orbital irradiation and in those patients the expression of the two key antigens (TSH-R and IGF-1R) was significantly decreased.
Surprisingly, radiotherapy did not impact the staining results of the infiltrating immunocytes (T and B cells, macrophages). Further, it is difficult to overcome the earlier two limitations as ethical approval for not specifically treating the patients with active severe TED is unlikely to be granted. (4) Finally, we have not looked at the MHC expression in patient and control samples as this has been previously done and reported numerous times. 18,20
In conclusion, this multicenter, single blind, case-control, immunohistochemical evaluation of OCT and OAT with a user-independent tool demonstrated the relevant role of adaptive immune response, cell-mediated immunity, and overexpression of TSH-R/IGF-1R and CD40/CD40L in the pathophysiology and pathogenesis of TED, especially in the active, inflammatory phase. Targeting these key players will offer more effective and disease-specific treatment strategies.
Footnotes
Authors' Contributions
Y.-P.H.: Investigation, methodology, formal analysis, software, validation, visualization, and writing—original draft. M.E.M.S.: Methodology, investigation, formal analysis, validation, visualization, and writing—review and editing. K.A.P.: Conceptualization, resources, software, and writing—review and editing. H.M.E.: Resources, writing—review and editing. A.C.H.L.: Conceptualization, validation, and writing—review and editing. S.F.: Resources, writing—review and editing. H.Z.: Resources, writing—review and editing. L.F.: Investigation, methodology, and writing—review and editing. J.L.: Data curation, visualization, and writing—review and editing. T.E.: Conceptualization, funding acquisition, methodology, resources, supervision, project administration, validation, visualization, and writing—review and editing. G.J.K.: Conceptualization, funding acquisition, methodology, resources, supervision, project administration, validation, visualization, and writing—original draft, writing—review and editing.
Author Disclosure Statement
All the authors have nothing to disclose.
Funding Information
This work has been partially supported by the Medical Faculty of the JGU Medical Center and the Department of Pharmaceutical and Biomedical Sciences, JGU, Mainz, Germany. No funding was received.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4