
Abstract
Background:
PTEN hamartoma tumor syndrome (PHTS) is associated with a high prevalence and early onset of differentiated thyroid cancer and benign thyroid disease. However, a consensus on the time of initiation and frequency of thyroid cancer surveillance has not yet been reached. Most commonly, guidelines recommend annual thyroid ultrasounds, but vary widely in the time of initiation, ranging from shortly after birth to 18 years of age. Minimal data are available on the development and progression of thyroid disease over time in this population. This study aimed to target this knowledge gap by investigating the time to develop thyroid nodules and thyroid cancer from an initial ultrasound in 76 PHTS patients.
Methods:
The electronic records of 281 prospectively accrued PHTS patients were retrospectively reviewed between 2005 and 2021, and 76 patients were identified as having at least two thyroid ultrasounds. Time-to-event analyses were performed, determining the probability of developing thyroid nodules and thyroid cancer over time.
Results:
We demonstrated that PHTS patients with an initial thyroid ultrasound without nodules (n = 41) had >90% likelihood of remaining free of a clinically actionable nodule at 3 years and an 85% likelihood at 6 years. None of these patients developed thyroid cancer over the entire follow-up period (mean 4.6 years). In patients with a clinically nonactionable nodule, defined as not meeting criteria for fine needle aspiration or thyroidectomy (n = 14), we demonstrated that 80% will not have an actionable nodule at 3 years, and none developed thyroid cancer over the entire follow-up period.
Conclusions:
Our observations suggest stratifying surveillance intervals based on thyroid ultrasound result, and support extending surveillance intervals in PHTS patients without nodules on ultrasound to 3–5 years, and patients with clinically nonactionable nodules to 2–3 years, in contrast to the current recommendation of annual ultrasounds. This change in practice would decrease the burden of frequent ultrasounds, especially in young children and adolescents who are more likely to have a normal or nonactionable ultrasound result.
Introduction
PTEN hamartoma tumor syndrome (PHTS) is a collection of syndromes defined by a pathogenic germline PTEN mutation. PHTS encompasses a wide range of clinical phenotypes, characterized by benign and malignant overgrowths, macrocephaly, and neurodevelopmental disorders. 1 The PTEN gene encodes the tumor suppressor phosphatase and tensin homolog (PTEN), which downregulates the PI3K/AKT/mTOR signaling pathway, and has been implicated in DNA repair and promoting genomic stability. 2,3 As a result, pathogenic PTEN mutations result in uncontrolled cell growth, proliferation, and genomic instability, and have been found in many sporadic and inherited cancers. 4.5 Specifically, pathogenic germline PTEN mutations are associated with a predisposition to breast, thyroid, kidney, skin, endometrial, and colorectal cancers. 6
The thyroid gland is frequently affected in PHTS, developing both benign and malignant disease. 1,6,7 Studies have demonstrated an increased risk of differentiated thyroid cancer (DTC) in PHTS patients, with a lifetime risk as high as 38% compared with 1% in the general population. 6,8,9 Benign thyroid disease is also common with up to 71% of PHTS patients having thyroid nodules, and 27% having autoimmune thyroiditis. 8,10 Thyroid disease is one of the earliest manifesting clinical phenotypes of PHTS, often developing in pediatric patients. 11 –13 DTC has been diagnosed as early as 4 years of age in PHTS, and studies have demonstrated an increased risk of pediatric DTC, ranging from 4% to 12%. 11,14,15 Thyroid nodules have been found in 26–63% of pediatric patients. 14,16,17
Clinicians have adopted thyroid ultrasound surveillance in PHTS patients as an effective and noninvasive way to diagnose and monitor the progression of thyroid disease. However, as PHTS is rare with an estimated prevalence of at least 1 in 200,000 individuals, 1,18 there are limited data demonstrating the development of thyroid disease and cancer in these patients over time, especially from an initial normal thyroid ultrasound. Thus, the current surveillance guidelines are primarily expert opinion based and lack a clear consensus. Recommendations range from initiating ultrasound surveillance at time of diagnosis, age 2–3, age 7, age 10, or age 18, and frequency of ultrasound varies from annual to triennial. 11,16,17,9 –22 Surveillance recommendations are also typically applied to all PHTS patients, regardless of the presence or absence of thyroid disease at initial ultrasound.
This study aimed to investigate the development and progression of thyroid nodules and DTC in PHTS patients, with the goal of providing stronger evidence to refine surveillance recommendations. We sought to address the hypothesis that patients without nodules on initial ultrasound could be safely surveilled less aggressively than patients with thyroid disease. Of particular interest were pediatric, adolescent, and young adult PHTS patients, who are more likely to have ultrasounds without nodules and stand to benefit the most from reduced surveillance.
Methods
This study was approved by the Cleveland Clinic Institutional Review Board (IRB), protocol number IRB 8458. All patients provided written informed consent to participate in this protocol.
Patient selection
Among 6964 subjects prospectively accrued under Cleveland Clinic's IRB 8458 protocol from September 1, 2005 to December 1, 2021, we identified 469 individuals with pathogenic or likely pathogenic germline PTEN mutations. Of these individuals, we selected 181 subjects who had a medical record number (MRN) in the Cleveland Clinic electronic medical record system. We then retrospectively reviewed the electronic charts for thyroid ultrasound reports and excluded subjects who had zero or one thyroid ultrasound. Our final series included 76 subjects with at least two thyroid ultrasounds (Fig. 1).
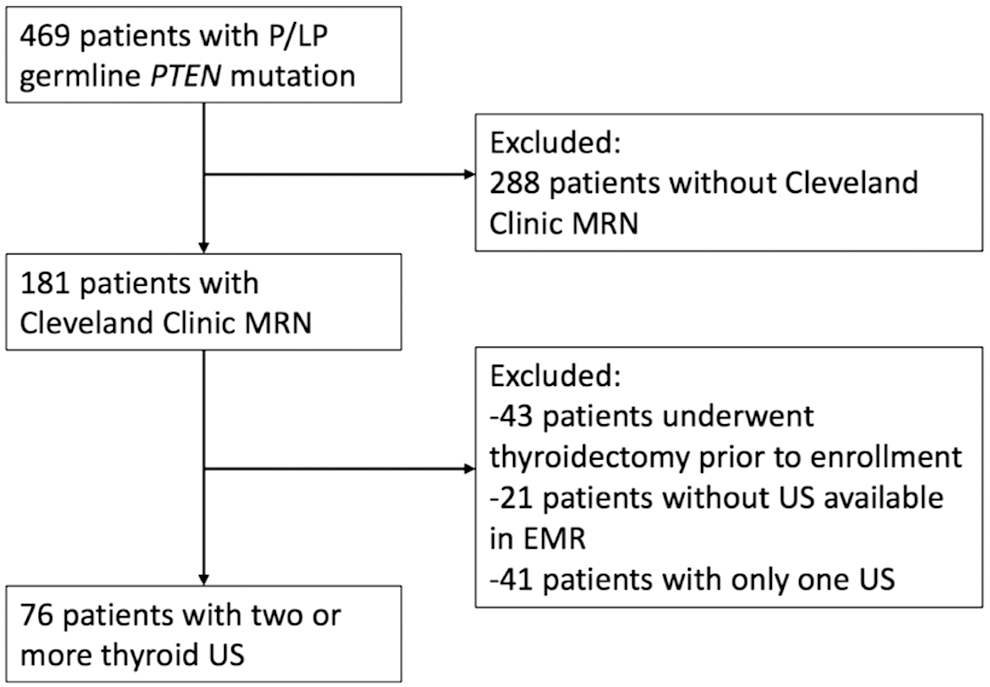
Inclusion and exclusion criteria flow sheet. LP, likely pathogenic; MRN, medical record number; P, pathogenic; PTEN, phosphatase and tensin homolog; US, ultrasound.
PTEN mutation status
Germline PTEN mutation status was determined by clinical genetic testing and verified by polymerase chain reaction or multiplex ligation-dependent probe amplification. The pathogenicity of PTEN variants was classified according to ClinVar database classifications and ClinGen gene-specific criteria for PTEN variant curation. 23,24 For unreported variants, Franklin by Genoox was used along with expert opinion at the Cleveland Clinic. 25
Data collection
Patient electronic records were retrospectively reviewed for thyroid ultrasound reports completed by radiologists, endocrinologists, or endocrine surgeons. The data collection period started at the time of the patient's first ultrasound and ended at the time of total thyroidectomy or censored after the last available ultrasound. The variables collected were ultrasound dates, sonographic findings, fine needle aspirations (FNAs), cytology results, thyroidectomy, and final pathology results.
Subjects were divided into three main groups based on the initial ultrasound findings: (1) no nodules, (2) at least one clinically nonactionable nodule, and (3) at least one clinically actionable nodule. Clinically actionable nodules were defined as nodules meeting criteria for FNA, according to the 2015 American Thyroid Association (ATA) criteria based on sonographic characteristics and sizes of nodules. 26 These criteria were retrospectively applied to all nodules, regardless of the recommendation at the time of ultrasound. Clinically nonactionable nodules were nodules that did not meet these criteria. Reasons for undergoing thyroidectomy included suspicious or indeterminate cytology on FNA, multinodular goiter, obstructive symptoms, and patient preference. Patients who met the criteria for FNA or surgery but did not proceed with intervention were considered to have a clinically actionable nodule. The primary outcomes were the time to develop a clinically actionable nodule, and the time to develop DTC. The secondary outcome was the time to develop a clinically nonactionable nodule.
Statistical analysis
Time-to-event analyses were performed using the survival package in R (version 3.3.-0). 27 The Cox proportional hazards regression model was used to fit our raw data. Event-free probability was calculated and plotted as Kaplan–Meier curves. Descriptive statistics were performed using GraphPad Prism version 9.0 (GraphPad Software, San Diego, CA). Values of p < 0.05 were considered statistically significant.
Results
Patient characteristics
Our final series included 76 PHTS patients with at least two thyroid ultrasound reports (Fig. 1). On initial ultrasound, 41 subjects (53.9%) had no nodules, 14 (18.4%) had at least one clinically nonactionable nodule, and 21 (27.6%) had at least one clinically actionable nodule (Table 1). Average nonactionable nodule size was 0.51 cm (range, 0.2–1.1 cm) and average actionable nodule size was 2.0 cm (1.1–4.1 cm).
Demographics and Patient Characteristics of Final Patient Series
FNA, fine needle aspiration; PTC, papillary thyroid cancer; US, ultrasound.
The median age (in years) at the time of initial ultrasound was 7.7 (range, 0.8–52.1) overall, 6.1 (0.8–34.7) for patients without nodules, 6.7 (2.5–29.65) for patients with clinically nonactionable nodules, and 32.0 (12.1–52.1) for patients with clinically actionable nodules. One-way analysis of variance (ANOVA) was performed to compare the age at initial ultrasound between the three groups. Patients with actionable nodules on initial ultrasound were significantly older (95% confidence interval [CI], 25.9–38.0 years) than patients without nodules (95% CI, 5.7–10.7 years) (p < 0.0001), and patients with nonactionable nodules (95% CI, 5.2–15.2 years) (p < 0.0001). There was no significant difference in age between patients without nodules and patients with nonactionable nodules on initial ultrasound (p = 0.38).
Fisher's exact test was performed to compare the ratio of sexes between the three groups, which revealed no significant difference: no nodules versus nonactionable nodules (p = 0.51), no nodules versus actionable nodules (p = 0.099), and nonactionable nodules versus actionable nodules (p = 0.73). In addition, there was no significant difference in the prevalence of thyroid disease during the entire follow-up between females and males (69.0% vs. 70.2%) (p > 0.99). Fisher's exact test was performed to compare the frequency of mutations in individual PTEN exons in patients with and without thyroid disease, and there was no significant difference found for any exon.
The average interval between ultrasounds was 1.33 years (range, 0.25–5.2). Six patients had ultrasound intervals greater than every 2 years. Of these, three remained nodule free over the entire follow-up period, and three had actionable nodules on initial ultrasound.
Surveillance outcomes
Among subjects without nodules on initial ultrasound (n = 41), 15 (36.6%) developed nonactionable nodules, 6 (14.6%) developed actionable nodules, and none developed DTC. The median age (in years) at the time of initial ultrasound, at the time of developing nonactionable nodules, and at the time of developing actionable nodules was 6.7 (range, 2.5–29.65), 8.2 (3.3–22.2), and 12.5 (5.1–24.7), respectively. Kaplan–Meier curves were used to estimate the event-free probability, with event being development of actionable nodules (Fig. 2) and nonactionable nodules (Fig. 3) from an initial ultrasound without nodules. At 3 years, the model predicted 72.6% (95% CI, 58.7–89.8%) of patients to remain nodule free and 94.3% (95% CI, 86.9–100%) to be without an actionable nodule (Table 2). Mean total follow-up for this group was 4.6 years (range, 0.5–8.4).
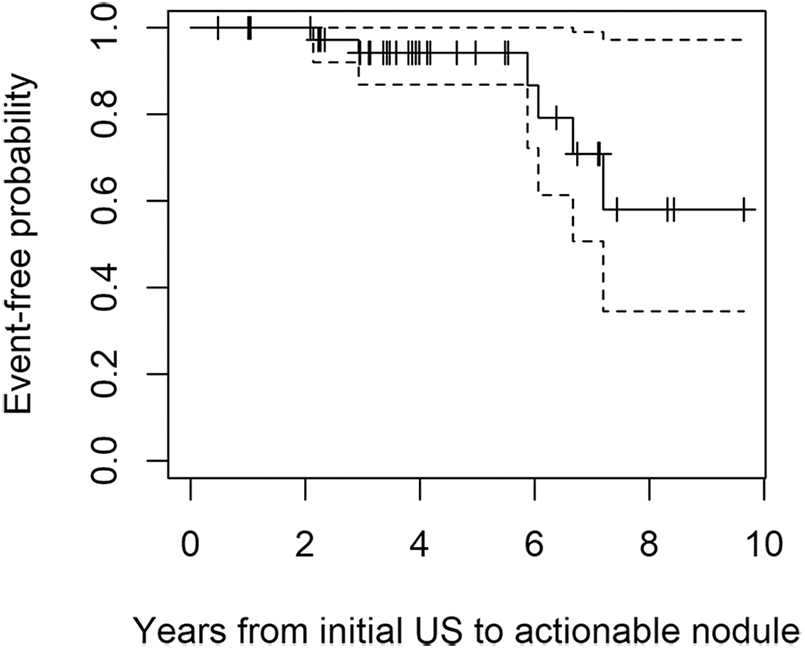
Kaplan–Meier curve, estimating the event-free probability from an initial ultrasound without nodules to developing a clinically actionable nodule. Dashed lines represent 95% CI, and tick marks represent patients lost to follow-up. CI, confidence interval.
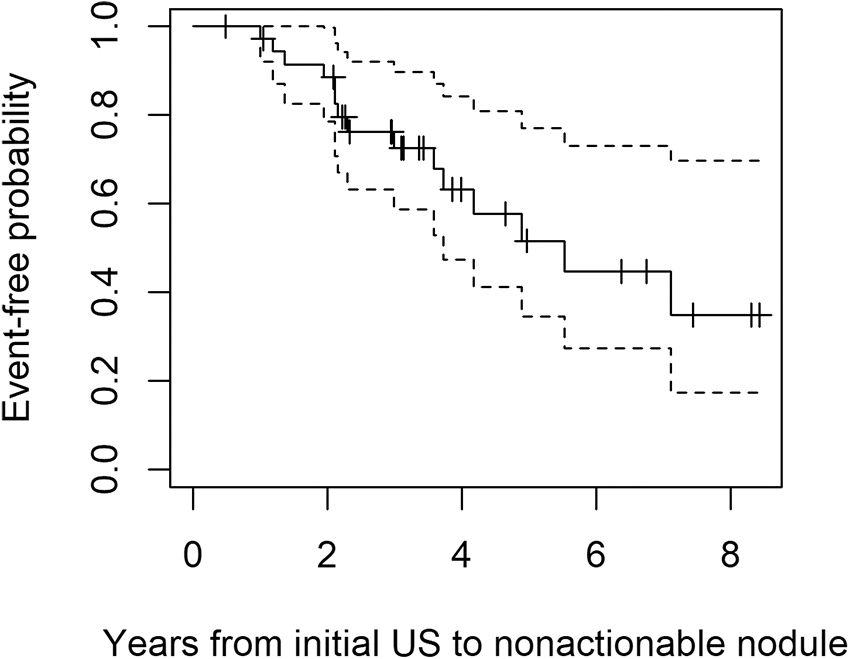
Kaplan–Meier curve, estimating the event-free probability from an initial ultrasound without nodules to developing a clinically nonactionable nodule. Dashed lines represent 95% CI, and tick marks represent patients lost to follow-up.
Event-Free Probability of Developing Thyroid Nodules After an Initial Ultrasound Without Nodules, Using the Kaplan–Meier Curve
CI, confidence interval; US, ultrasound.
Among subjects with nonactionable nodules on initial ultrasound (n = 14), 5 (35.7%) developed actionable nodules and none developed DTC. The median age of initial ultrasound was 6.7 years (range, 2.5–29.65) and the median age of developing actionable nodules was 13.3 years (8.1–31.8). A Kaplan–Meier curve was used to estimate event-free probability, with event being development of an actionable nodule from nonactionable nodules (Fig. 4). At 3 years, this model predicted 79.7% (95% CI, 61.6–100%) of these patients to be without an actionable nodule (Table 3). Mean total follow-up for this group was 4.6 years (range, 0.3–10.1). When subdividing nonactionable nodules into <5 and ≥5 mm in diameter, patients with ≥5 mm nodules were predicted to develop actionable nodules at shorter intervals. At 3 years, 62% (95% CI, 38.0–100%) of these patients remained without an actionable nodule, compared with 89.5% (95% CI, 72.0–100%) of patients with <5 mm nonactionable nodules on initial ultrasound (Table 3).
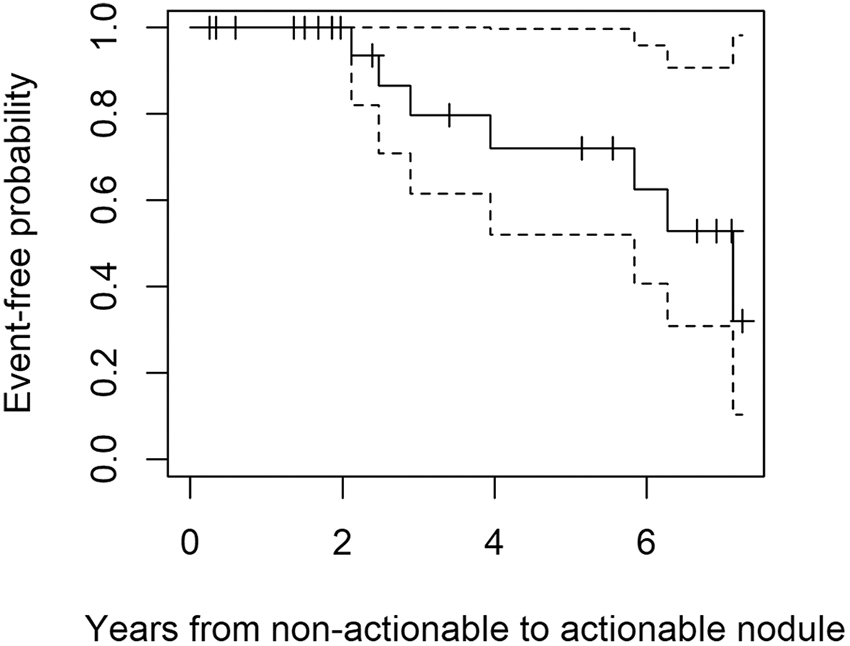
Kaplan–Meier curve, estimating the event-free probability from an initial ultrasound with clinically nonactionable nodules to developing a clinically actionable nodule. Dashed lines represent 95% CI, and tick marks represent patients lost to follow-up.
Event-Free Probability of Developing Clinically Actionable Nodule After an Initial Ultrasound with Clinically Nonactionable Nodules, Using the Kaplan–Meier Curve
CI, confidence interval; US, ultrasound.
The above time-to-event analyses were repeated in pediatric patients (age, <20 years) yielding similar results (Supplementary Table S1).
Cancer prevalence and characteristics
Among subjects with actionable nodules on initial ultrasound (n = 21), 1 (4.8%) developed DTC. On initial ultrasound at age 45, this patient was found to have five distinct nodules, the largest being 1.7 cm. Subsequent FNA cytology was classified as benign according to the Bethesda criteria. 28,29 After 12.4 years of surveillance, a total thyroidectomy was performed because of patient preference, revealing an incidental 0.2-cm papillary thyroid microcarcinoma. As only one patient developed DTC, a time-to-event analysis was not appropriate for predicting development of DTC. Mean total follow-up for this group was 5.5 years (range, 0.7–13.5).
When considering all 181 PHTS patients with a Cleveland Clinic MRN, 18 (9.9%) were diagnosed with DTC (Table 4). Six patients (33.3%) were under the age of 20 at the time of DTC diagnosis, with the youngest being 11.7 years old. Six patients (33.3%) were found to have DTC incidentally after surgery for multinodular goiter. Regional metastases were discovered in two patients (11.1%), and no patients were found to have distant metastases. Of the two patients with regional metastases, both had a single positive lymph node in the central neck, neither of which were observed on preoperative ultrasound. One patient had clinical suspicion of local recurrence, with evidence of a paratracheal mass on ultrasound and an elevated thyroglobulin. However, this patient pursued further diagnosis and treatment at an outside institution, and pathology was not available for confirmation of recurrence. Therefore, for this study, the case was considered to be a recurrence, but it is possible that the mass was from regrowth of residual benign thyroid tissue.
Prevalence and Characteristics of Thyroid Cancer in All PTEN Hamartoma Tumor Syndrome Patients with a Cleveland Clinic Medical Record Number
AJCC, American Joint Committee on Cancer, 8th edition; FTC, follicular thyroid cancer; PTC, papillary thyroid cancer.
Discussion
Despite significant evidence demonstrating the high prevalence and early onset of DTC in PHTS patients and publication of national practice guidelines, a consensus on the age of initiation and frequency of DTC surveillance has not yet been reached. 20 While several studies have characterized the prevalence of thyroid disease in this population, there are minimal data on its development and progression, especially from an initial normal thyroid ultrasound. This study aimed to target this knowledge gap by examining the development and progression of thyroid disease in PHTS patients using surveillance thyroid ultrasounds.
Patients with an initial ultrasound without nodules had a >90% likelihood of remaining free of a clinically actionable nodule at 3 years and an 85% likelihood at 6 years (Table 2). No cases of DTC were diagnosed in this group over the entire follow-up period. These findings strongly support that PHTS patients with a normal thyroid ultrasound can safely undergo surveillance less frequently than the current most common recommendation of annually. 11,16,17,19 –22 While fewer patients are predicted to remain nodule-free over this time frame (77.6% at 3 years, 44.8% at 6 years), earlier discovery of these nonactionable nodules would not impact clinical management as the nodules do not meet criteria for intervention. These results were consistent with the findings of a recent study that demonstrated children with PHTS without nodules >5 mm were unlikely to develop nodules >1 cm within 2 years. 12
Once patients develop a nonactionable nodule, our data shows 80% of these patients will not have a clinically actionable nodule at 3 years, and none developed DTC over the entire follow-up period. However, of patients with nonactionable nodules ≥5 mm, 62% were predicted to not have a clinically actionable nodule at 3 years.
Out of our final series of 76 PHTS patients, only one patient (1.3%) was diagnosed with DTC, which was discovered incidentally on thyroidectomy pathology 12.4 years after initial ultrasound. This observation further supports the safety of a prolonged screening interval. It is crucial to note that this study does not predict the risk of DTC in the overall PHTS population, and can only be applied to the development of disease after initial ultrasound. This is inherent to the fact that many patients develop DTC before PHTS diagnosis, and thus were not captured in this study. When considering all 181 PHTS patients with a Cleveland Clinic MRN, 18 (9.9%) were diagnosed with DTC (Table 4).
When discussing surveillance guidelines, it is paramount to consider both the benefits and risks of the surveillance modality. The primary benefit of DTC surveillance in PHTS patients is earlier diagnosis, and although no study has shown that this translates to improved clinical outcomes in PHTS, this has been demonstrated in sporadic DTC. 30 Of note, studies have demonstrated that DTC in PHTS patients tends to be less invasive and more indolent than sporadic DTC. 11 This is consistent with our larger patient series data, showing low rates of regional and distant metastases, and cancer recurrence (Table 4). While thyroid ultrasound is noninvasive, the procedure can be more burdensome for young children and patients with neurodevelopmental disorders, often seen in PHTS. 1,17 FNA, while safe and associated with minimal complications, can be a painful procedure and lead to significant patient and parental stress and anxiety from both the procedure and awaiting cytology results. 31 Surveillance can also lead to false positive or indeterminate findings resulting in unnecessary surgeries.
After considering the prevalence of DTC in both pediatric and adult PHTS patients and our current surveillance data, we advocate for stratifying surveillance intervals based on initial ultrasound result. In patients with a thyroid ultrasound without nodules, we advocate for repeating ultrasound in 3–5 years. If ultrasound shows a clinically nonactionable nodule, patients can likely be safely followed in 2–3 years; however, this population has a wider range of sonographic findings with varying risk, such as a 0.1 cm simple cyst versus a 0.9 cm hypoechoic nodule. When subdividing nonactionable nodules into < and ≥5 mm, expectantly patients with nodules ≥5 mm were more likely to develop actionable nodules. Therefore, clinical judgment should always be applied, and larger nonactionable nodules should be considered for more frequent surveillance.
Patients with a high suspicion ultrasound pattern should repeat ultrasound in 6–12 months, in accordance with ATA guidelines for following thyroid nodules in the general population. 26 For patients with an actionable nodule, appropriate intervention should be performed. In the case of benign cytology, continued surveillance in 1–2 years is reasonable, in accordance with ATA guidelines. 26 While prior studies have demonstrated a higher risk of thyroid disease in female PHTS patients and patients with mutations in exon 6 or exon 8 of PTEN, our study did not find any statistical difference in gender or location of PTEN mutation when comparing patients with and without thyroid disease. 12,32
Determining when to initiate DTC surveillance in PHTS patients remains challenging. With the youngest documented case of DTC at 4 years old in this population, 11 initiating thyroid ultrasound at the time of PHTS diagnosis may lead to earlier diagnosis of DTC in select cases, as opposed to starting at age 7 or later. However, as DTC is relatively indolent and curable, it is difficult to know if this would translate to improved clinical outcomes. In addition, initiating DTC surveillance at the time of PHTS diagnosis, especially if shortly after birth, has previously carried the burden of annual ultrasounds regardless of ultrasound findings. By expanding the surveillance interval for patients with normal and nonactionable ultrasounds, this burden is reduced. Therefore, we advocate for performing an initial thyroid ultrasound at the time of diagnosis of PHTS if tolerated, and stratifying surveillance intervals based on ultrasound result. This provides the benefit of capturing early cases of DTC, while decreasing the burden of frequent ultrasounds especially in young children.
Given the rarity of PHTS, the greatest strength of our study is that it is a relatively large study investigating the development and progression of thyroid disease in PHTS patients. The study also has the advantage of early and frequent ultrasound results, as the current Cleveland Clinic PTEN Multidisciplinary Clinic and Center of Excellence practice is initiating thyroid ultrasound surveillance at time of PHTS diagnosis with subsequent annual ultrasounds. The primary limitation of the study is that it is a retrospective chart review, although in prospectively accrued participants, with an inherently low sample size when investigating a rare disease like PHTS. In addition, as many patients had thyroidectomies before diagnosis of PHTS or before presentation to our institution, their ultrasounds were not available. Thus, we were not able to comment on the progression of thyroid disease in these patients. Proper review of ultrasound images was also not possible, as ultrasound requires real-time assessment, and captured single views are often inadequate. Therefore, review of ultrasound reports can be associated with interobserver variation.
It is important to note that our patient population is primarily pediatric (76.3%), and our oldest patient with an initial ultrasound without nodules was 29 years old. Thus, our results may not reflect the development of thyroid disease in a middle-aged or elderly population. However, as PHTS shows incomplete penetrance, it is very possible that older patients who have not developed thyroid disease are less likely to express these phenotypes later in life. It should also be emphasized that we set out to address thyroid surveillance in the pediatric, adolescent, and young adult population, where little data and a broad range of clinical practices exist.
Footnotes
Authors' Contributions
G.P.: experimental design, acquisition and analysis of data, interpretation, article drafting, critical review, and editing. T.B.: experimental design, acquisition and analysis of data, article drafting. L.Y.: critical review and revision of article. J.J.: critical review and revision of article. J.S.: critical review and revision of article. C.E.: conceptualization, experimental design, interpretation of analyses, interpretation, critical review and revision of article, resources, overall supervision, project administration. All authors gave approval of the final version of the article.
Acknowledgment
The authors thank Jeff Hammel for his assistance with the statistical analyses presented in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
G.P. and T.B. are Crile Fellows at the Cleveland Clinic. T.B. and L.Y. are Ambrose Monell Cancer Genomic Medicine Fellows at the Cleveland Clinic. C.E. is the Sondra J. and Stephen R. Hardis Endowed Chair in Cancer Genomic Medicine at the Cleveland Clinic. This study is not associated with any external funding or grants.
Supplementary Material
Supplementary Table S1