
Abstract
Background:
Although the relationship between subclinical hypothyroidism and major depressive disorder (MDD) has been studied in adults in cross-sectional and prospective population-based studies, this has not yet been done in adolescents. However, since thyroid function and MDD risk are subjected to maturational processes and ramifications of illness duration over the life span, these findings may not readily transfer to adolescents.
Methods:
The relationship between subclinical hypothyroidism and MDD was studied in a representative subsample of the nationwide KIGGS (“The German Health Interview and Examination Survey for Children and Adolescents”) survey. A total of 4118 adolescents were examined over a median period of 6 years, and data were analyzed by a logistic regression approach accounting for important covariates related to thyroid function and/or MDD risk. The same approach was chosen to investigate the relationship between quartiles of thyrotropin (TSH) and free thyroxine (fT4) levels and incident MDD in euthyroid participants to broaden the focus on the relationship between thyroid hormone levels and MDD in a dose–response manner.
Results:
During the observation period, 121 cases of MDD were reported. There was no association between subclinical hypothyroidism and MDD when comparing 111 adolescents with subclinical hypothyroidism with 4007 euthyroid adolescents, representative of ∼106,000 and 3,610,000 adolescents from the general pediatric population, respectively. This also applied when studying the relationship between quartiles of TSH and fT4 levels and MDD in euthyroid participants. All results were confirmed by sensitivity analyses accounting for thyroid autoimmunity.
Conclusions:
Consistent with findings in adults, there is no association between subclinical hypothyroidism or quartiles of TSH and fT4 levels in the normal range and MDD in adolescents, despite potential age-related differences regarding thyroid function and MDD risk.
Introduction
Major depressive disorder (MDD) is a debilitating and highly prevalent psychiatric disorder. During adolescence, as many as 20% of teenagers are affected by significant depressive symptoms at some point, 1 and one-third of adolescents suffer from depression attempt suicide. 2 Given these figures, it is important to identify the underlying causes of MDD for early prevention and intervention. In this regard, the contribution of thyroid dysfunction to MDD, especially subclinical hypothyroidism (normal serum free thyroxine [fT4] levels in the presence of elevated serum thyrotropin [TSH] levels—subsequently SCHYPO), remains controversial due to conflicting findings.
However, only recently, Bode et al 3 investigated the relationship between SCHYPO and MDD in ∼172,000 adults based on 17 epidemiological and population-based cohort studies. There was only a slightly increased risk for MDD in adults with SCHYPO that was lost when considering bias by a trim-and-fill analysis. In contrast, two more recent meta-analyses, also including case–control studies assessing more severe cases from clinical settings, found a higher risk of SCHYPO in MDD in 12,315 4 and 103,3755 adults, respectively.
This is in line with results from clinical samples in children and adolescents with MDD. 6,7 Recently, we found a prevalence of SCHYPO of 9.1% in 360 adolescents with MDD, which was significantly higher than in 2329 age- and sex-matched adolescent controls (2.1%). However, the relationship between SCHYPO and MDD has not yet been studied in an epidemiological sample of children and adolescents.
Thus, the aim of the present study was to examine the directional relationship between SCHYPO and the prospective risk for incident MDD in adolescents with thyroid dysfunction from a large and representative nationwide study.
Materials and Methods
Participants
“The German Health Interview and Examination Survey for Children and Adolescents” (KiGGS) is a nationally representative longitudinal study on the health status of children and young people living in Germany. Details on the study design, the sampling strategy, and the study protocol have been described in detail elsewhere. 8
Since the baseline study was conducted between 2003 and 2006, two follow-ups have been completed: KiGGS wave 1 between 2009 and 2012 and KiGGS wave 2 between 2014 and 2017. The baseline study included 17,640 participants (8654 females and 8986 males) aged 0 to 17, among whom 3775 respondents did not take part in any follow-up assessment. 8
The KiGGS baseline study and wave 1 were approved by the ethics committee of the Charité Berlin (No. 101/2000 and No. EA2/058/09, respectively), and wave 2 was reviewed by the ethics committee of the Hannover Medical School (No. 2275-2014). Both studies complied with regulations of the Federal Data Protection Act (BDSG) and the EU General Data Protection Regulation (GDPR). 8 Written informed consent was obtained from parents as well as from children aged 14 years and older.
For the present study, adolescents aged 10 years and older 9 at the time of the KiGGS baseline assessment, who also took part in at least one follow-up examination and were queried on MDD history, were considered for analysis (N = 5271). Participants with incomplete information on MDD history, a history of MDD at baseline, missing information on any covariate of interest and thyroid status, thyroid dysfunction other than SCHYPO, or on medication for thyroid dysfunction or MDD were excluded (Fig. 1).

Study flowchart. fT4, free thyroxine; MDD, major depressive disorder; TSH, thyrotropin.
Questionnaires and interviews
Participants aged 11 years and older and parents of minor participants either completed self-administered, standardized questionnaires (baseline and wave 2) or took part in a telephone interview (wave 1). Among others, the questionnaires/interview addressed health-related behavior, including smoking status, combined oral contraception (COC) use, migration background, and socioeconomic status (SES). The latter was determined by the multidimensional Winkler stratification index, drawing on information from the parents' highest level of educational attainment and the highest professional status as well as the net household income. 10 Smoking status was only queried in participants 11 years and older, and participants younger than that were considered nonsmokers. 11
Parents of minors and young adults (≥18 years) participating in either study completed a computer-assisted personal interview (CAPI) conducted by a specially trained study physician. 12 The CAPI comprised a detailed section on the use of medication within the past seven days. 8,12 The interview also covered the participants' medical history and asked about physician-diagnosed diseases and chronic conditions as well as health care utilization within the past 12 months.
Depression assessment
Beginning with wave 1, the CAPI explicitly addressed the participants' mental health history regarding selected disorders, including MDD, diagnosed by a physician (general practitioner, psychiatrist, neurologist) or psychologist; with wave 2, the age of onset of mental health conditions (in total years) was recorded. The present study examined incident MDD between the KiGGS baseline examination and the first follow-up (wave 1). In participants who only completed the baseline examination and wave 2, the follow-up length regarding incident MDD was determined according to the median follow-up in participants who completed at least the baseline examination and wave 1 for reasons of comparability.
Laboratory studies
At baseline, blood samples for measurement of TSH, fT4, and thyroid peroxidase antibody (TPO-Ab) were obtained by a venous puncture after a median fasting period of two hours. For details, please see the Supplementary Data.
Using RefCurv (Version 0.4.4,
Statistical analysis
Data handling and analyses were performed with SPSS 27.0 (IBM Corp., Armonk, NY) and its Complex Samples® procedures to account for the sample design and design-related effects. For this purpose, all analyses were conducted considering longitudinal weighting factors to account for attrition related to sociodemographic characteristics and the cluster structure of the data. 8
All results were assessed by two-tailed testing. Analyses regarding the relationship between thyroid function and incident MDD were corrected for multiple comparisons controlling the two-tailed false discovery rate at q < 0.05. All other analyses related to sociodemographics or missingness were considered exploratory and not corrected for multiple testing.
Study characteristics
Euthyroid participants (N = 4007) and those with SCHYPO (N = 111) were compared regarding important sociodemographic characteristics and covariates by either adjusted Wald F tests (continuous variables) or (second-order) adjusted χ 2 tests according to Rao and Scott 15 (categorical variables). This also applied when contrasting excluded and included respondents.
The pattern of weighted missing values was analyzed by separate variance t-tests and Little's test.
Logistic regression—thyroid function and MDD
The relationship between SCHYPO (independent variable) and the risk for incident MDD over the follow-up period between the KiGGS baseline study and wave 1 was assessed by two logistic regression models. The first model was unadjusted, whereas the second model also accounted for potential covariates related to either thyroid dysfunction or MDD (age, sex, z-standardized BMI [z-BMI], smoking, COC, migration background, and SES, the latter also as a reliable proxy for adverse life events in childhood and adolescence in Western countries 16 ). The same approach was chosen to investigate the relationship between quartiles of TSH and fT4 levels and incident MDD in euthyroid participants to broaden the focus on the relationship between thyroid hormone levels and MDD in a dose–response manner. 17
The linearity of the relationship between continuous predictors and the logit transform of depression status was evaluated according to the Box-Tidwell approach. Variables of interest were screened for multicollinearity (>0.70).
Sensitivity analysis
Thyroid autoimmunity may not only explain thyroid dysfunction, including SCHYPO, but also constitute a risk factor for MDD on its own by a distinct set of pathophysiological processes related to cerebral inflammation and myelinization 18 –21 as well as by the release of neurotransmitters. 22 Thus, we included TPO-positivity (TPO-Ab levels >100 IU/mL) as an additional covariate in the analyses outlined earlier to provide an unconfounded picture of the relationship between SCHYPO and MDD and to assess the contribution of thyroid autoimmunity to MDD.
Results
Of the 17,640 children and adolescents who took part in the baseline assessment of the KiGGS study, 7380 participants were aged 10 years and qualified for inclusion. Of these, 5271 participants completed at least one follow-up assessment and were screened for a history of MDD. Considering the exclusion of 1153 participants for reasons detailed in Figure 1, 4118 were included for analysis (1896 participants completed all follow-up examinations, 839 completed the baseline study and wave 1, and 1383 completed the baseline study and wave 2).
Participants who were excluded were older (p = 0.005; Supplementary Table S1), had a higher BMI (p = 0.049), had a lower social SES (p = 0.04), and were more often from a migration background (p = 0.03) than the included respondents. Regarding thyroid function, excluded participants evidenced lower z-standardized TSH (p < 0.001) and higher z-standardized fT4 levels (p = 0.04). However, absolute differences were minor and significance was driven by the large sample size. Less than 5% of the 5271 survey participants (3.5% unweighted, 4.1% weighted) did not report information regarding their MDD history, which is generally considered a negligible rate of missing data. 23,24 This also applied to all other continuous and categorical variables, except for TSH and fT4 levels, which were found to be missing in 5.7% (unweighted, 6.5% weighted) of cases. However, further analyses revealed a random pattern of missingness.
Altogether, 111 cases of SCHYPO were identified (Table 1), corresponding to ∼106,000 cases in the German general pediatric population. Three of these cases showed a TSH level above 10 μIU/mL (Fig. 2). No difference was found in the prevalence of SCHYPO depending on the time-of-day that blood was sampled (before vs. after 10 am: 1.9% vs. 2.8%, p = 0.52).

Distribution of TSH and fT4 levels in participants with subclinical hypothyroidism (
Baseline Characteristics—Sociodemographics
Mean, standard deviation (in round brackets), and range (in square brackets) for interval scaled variables, percentages otherwise. The prefix “z” indicates z-standardized variables. Percentages are adjusted for the sampling plan, and standard deviations are based on normalized weights.
Percentages only refer to females in the sample.
Significant uncorrected difference between both samples at p < 0.05.
COC, combined oral contraceptive; fT4, free thyroxine; SES, socioeconomic status; TSH, thyrotropin.
The median follow-up period after baseline regarding a diagnosis of MDD was 6 years (5 years: N = 11, 6 years: N = 3829, 7 years: N = 278; IQR: 0). There was no difference in the proportion of participants with SCHYPO regarding different times to follow-up (5 years: 11.6%, 6 years: 2.6%, 7 years: 4.5%; p = 0.15). Over the entire period, 121 cases of MDD were reported. The median age at MDD diagnosis was 17.84 (SD = 2.51; Table 2 and Fig. 3).

Age at MDD diagnosis for those participants who completed KiGGS wave 2 and reported on the age of MDD onset (Nonweighted = 85,
Follow-up Period and Major Depressive Disorder
Standard deviations are based on normalized weights.
Only regarding participants who completed KiGGS wave 2 and reported on the age of MDD onset.
KiGGS, “The German Health Interview and Examination Survey for Children and Adolescents”; MDD, major depressive disorder.
Thyroid function and incident depression
There was no evidence of a significant relationship between SCHYPO and incident MDD over the entire period in adolescents and young adults, by either the unadjusted (model 1: OR = 0.38 [CI 0.13–1.16], p = 0.09, Table 3) or the adjusted model accounting for important confounders affecting the risk for thyroid dysfunction and/or MDD (model 2: OR = 0.43 [CI 0.14–1.32], p = 0.14). In addition, when studying quartiles of TSH and fT4 levels in the normal range in euthyroid participants, there was no prospective relationship between thyroid hormone levels and incident MDD (Table 3 and Fig. 4).
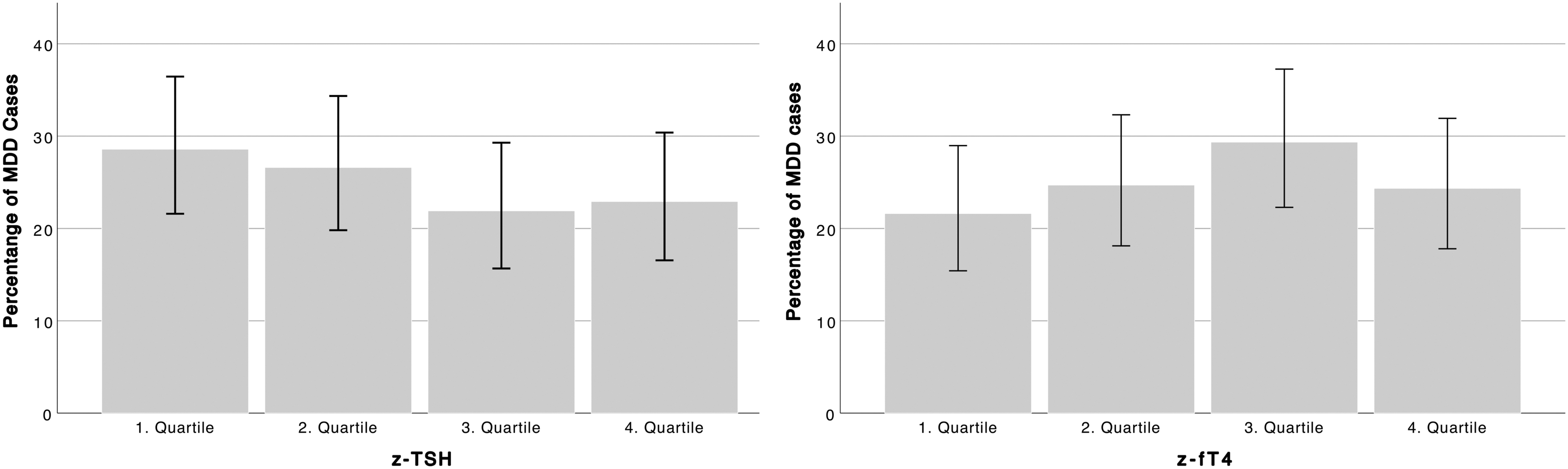
Percentage of MDD cases by quartiles of TSH (
Logistic Regression Results
Relationship between subclinical hypothyroidism (0 = absence, 1 = presence–reference category) as well as quartiles of TSH and fT4 levels and incident MDD. Model 2 is adjusted for age, z-standardized BMI, SES, migration background, smoking, and the use of COCs.
Reference category.
b, unstandardized regression coefficient; CI, confidence interval; OR, odds ratio; SE, standard error.
These findings were confirmed when considering TPO-Ab positivity as an additional confounder of thyroid function and as an independent risk factor for MDD by sensitivity analyses (Supplementary Table S2; details on the demographics of 328 excluded participants with missing information on TPO-Ab levels are provided in Supplementary Table S1).
Discussion
The (directional) relationship between SCHYPO and prospective MDD risk has not yet been studied in adolescents in epidemiological studies. 3,25 However, considering that thyroid function and MDD risk are subjected to maturational processes, especially during puberty, findings from adults may not readily transfer to adolescents. 26,27 Thus, we conducted the first study to prospectively investigate this association in a representative and nationwide sample of 4088 adolescents. There was no relationship between SCHYPO and incident MDD over a median period of six years. This also applied when investigating the association between quartiles of TSH and fT4 levels and MDD in a dose–response manner in euthyroid participants.
These findings were confirmed when considering multiple confounders, including TPO-Ab levels, as an indicator of thyroid autoimmunity.
Although previous studies, also including clinical samples, found an increased prevalence of SCHYPO in MDD in adults and adolescents, 4 –7 no such relationship was reported by meta-analyses of cross-sectional and prospective population-based studies in adults. 3,25 The latter finding is also consistent with small-scale studies assessing the effect of L-thyroxine supplementation on mostly subclinical depressive symptoms in patients with SCHYPO. 28 Regarding the association between thyroid hormone levels in the normal range and MDD, the findings of the present study in adolescents are in line with the largest study to prospectively investigate this relationship in 87,822 euthyroid adults. 17
No such study has been conducted in children and adolescents, but a large cross-sectional study including 7293 euthyroid participants aged 3–18 years found no association between thyroid hormone levels and broadly defined mental health assessed by the strength and difficulties questionnaire, which also applied to participants with SCHYPO (N = 331) in the same study. 29 In addition, a recent two-sample Mendelian randomization study that relied on genetic variants related to normal-range thyroid function as well as subclinical dysfunction and MDD found no evidence of a causal relationship. 30
Thus, the present study's findings in adolescents are consistent with cumulative evidence that neither SCHYPO nor variation in normal-range thyroid hormone levels relates to MDD when studied at the population level. This seems rather plausible for several reasons. First, although there are studies highlighting potential pathophysiological mechanisms regarding the effect of SCHYPO, for example, on the skeletal 31 and cardiovascular systems, 32 to date, no conclusive mechanism has been identified to explain the effect of increased TSH levels in peripheral euthyroidism on mood, even when considering cognitive functioning as a proxy. 33
The “low tissue liothyronine (T3) hypothesis” posits that some but not other tissues, including the brain, may experience local hypothyroidism due to decreased cellular T3 levels. However, findings in humans are fundamentally conflicting. 34 In addition, the most recent genome-wide association study regarding thyroid function, also including hypothyroidism, found that identified variants primarily affect gene expression patterns in thyroid but not in brain tissue. 35
Second, psychological mechanisms suggested to explain impaired mental health in patients with SCHYPO may not hold in population-based studies. Although a diagnosis of a (chronic) condition, including SCHYPO, 34 may itself impair mental health, most patients from epidemiological studies are unaware of their thyroid dysfunction, which seems to apply to children particularly. 29 Third, in children and adolescents, SCHYPO was found to be a transient phenomenon in ∼73% of 3622 children and adolescents over a follow-up period of 5 years, especially if TSH at baseline was below 7.5 μIU/mL. 36
This figure is even higher than in adults, in which normalization of TSH levels was observed in ∼62% of 12,815 outpatients with TSH levels between 5.5 and 10 μIU/mL over a follow-up period of the same length. 37
However, against the earlier outlined considerations, the observation of an increased prevalence of SCHYPO in meta-analyses also including clinical samples from a case–control setting remains to be explained. This even more so applies as the previously mentioned Mendelian randomization study by Kus et al 30 found no causal relationship between SCHYPO and MDD in either direction, that is, MDD did not (directionally) affect SCHYPO in this study as well.
Limitations
Although the present study relied on a nationwide sample representative of ∼3,680,000 adolescents, the absolute number of cases with SCHYPO was limited. Therefore, it was not possible to perform a subgroup analysis of adolescent participants with a TSH level above 7.5 μIU/mL, who are at an increased risk of progression to overt hypothyroidism. 36 However, in a large population-based prospective study including 4384 adults, there was no difference in the relationship between SCHYPO and MDD in those with only mildly (4.5–10 μIU/mL) and severely (>10 μIU/mL) elevated TSH levels. 17
A diagnosis of SCHYPO was established by a single blood draw, even though some authors argue for at least two samples taken on different occasions. 38 Unfortunately, this is a limitation inherent to epidemiological studies. Regarding the diagnosis of SCHYPO and a circadian secretion of TSH peaking in the morning, it is important to note that no difference was found in the prevalence of SCHYPO depending on the time-of-day that blood was sampled.
Although the present study addressed the longitudinal relationship between thyroid (dys-)function and incident MDD, subclinical depressive symptoms were beyond its scope. The earlier mentioned observation that thyroid function, including SCHYPO, did not relate to broadly defined mental health in children and adolescents cross-sectionally 29 suggests that thyroid (dys-)function may not significantly affect subclinical depressive symptoms, but this remains to be determined longitudinally using a depression-specific measure.
Considering that only information on TPO-Ab but not on thyroglobulin antibody (Tg-Ab) levels was available, the present study might not have fully captured the effect of thyroid autoimmunity on thyroid function and the risk for incident MDD. However, Tg-Ab levels are elevated in up to 10% of the general population and are usually not associated with thyroid autoimmunity in the absence of TPO-Ab. 39
Another limitation common to epidemiological studies addressing MDD is that the mental health history was self-reported, and a recall bias cannot be excluded, even though the follow-up period in the present study was notably shorter than in previous studies addressing such a bias. 40,41
Conclusions
In this first study of a large and representative sample of adolescents, there was neither a prospective association between SCHYPO nor quartiles of TSH and fT4 levels in the normal range and MDD. This is consistent with findings in adults, despite conceivable differences between adults and adolescents due to, among others, maturational and puberty-related processes affecting endocrine functioning and mood. This finding is embedded into an emerging theoretical framework, also relying on most recent insights from genetics that SCHYPO and MDD do not seem to be related. Although this seems to hold at the population level, this may not apply to clinical samples. Thus, a longitudinal study, setting in before MDD occurs and in long-term sequel to a first MDD, could help clarify their causal relationship.
Footnotes
Authors' Contributions
R.H. conceptualized the present study, analyzed and interpreted the data, and wrote the article. All authors participated in scientific discussions and revised the article. All authors approved the submitted version.
Data Availability
The datasets for this article are not publicly available as the results reported are based on a secondary analysis of data provided by the Robert Koch Institute (RKI), Germany. Requests to access the datasets should, therefore, be directed to the RKI (kiggsinfo@rki.de).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
R.H. was supported by the UMEA Clinical Scientist Program by the Faculty of Medicine of the University of Duisburg-Essen and the German Research Foundation (DFG). The funders had no role in the study design, data collection and analysis, decision to publish, or article preparation. The Baseline study of the KiGGS cohort was funded by the German Federal Ministry of Health, the Ministry of Education and Research, and the RKI. After establishing the German Health Monitoring System in 2008, further waves of the KiGGS study were funded by the German Federal Ministry of Health and the RKI only. 8
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2