
Abstract
Introduction:
Long-term cardiovascular (CV) risk is a concern for differentiated thyroid cancer (DTC) survivors.
Methods:
We performed a systematic review and meta-analysis evaluating the risks of CV mortality and morbidity in DTC survivors compared with the general population. Respective meta-analyses were conducted for data that were adjusted for relevant confounders and crude data. We searched five electronic databases from inception to October 2021, supplemented with a hand search. Two reviewers independently screened citations, reviewed full text articles, extracted data, and critically appraised the studies, with discrepancies resolved by a third reviewer. The primary outcome was CV mortality. Secondary outcomes included atrial fibrillation, ischemic heart disease, stroke, and heart failure. We estimated the relative risk (RR) and confidence intervals [CI] of outcomes using random-effects models (adjusted for age and gender), compared with the general population.
Results:
We reviewed 3409 unique citations, 65 full text articles, and included 7 studies. CV mortality risk was significantly increased in DTC survivors in one study adjusted for confounders—adjusted RR (aRR) 3.35 ([CI 1.66–6.67]; 524 DTC, 1572 controls). The risk of CV morbidity in DTC survivors, adjusted for risk factors, was estimated as follows: atrial fibrillation—aRR 1.66 [CI 1.22–2.27] (3 studies, 4428 DTC, I 2 = 75%), ischemic heart disease—aRR 0.97 [CI 0.84–1.13] (2 studies, 3910 DTC, I 2 = 0%), stroke—aRR 1.14 [CI 0.84–1.55] (2 studies, 3910 DTC, I 2 = 69%), and heart failure—aRR 0.98 [CI 0.60–1.59] (2 studies, 3910 DTC, I 2 = 79%). In meta-analyses of unadjusted data, the risks of CV mortality were not significantly increased but the CV morbidity risks were similar to adjusted data.
Conclusions:
There is limited evidence suggesting that DTC survivors may be at an increased risk of CV death and atrial fibrillation (after adjustment for confounders). We did not observe a significantly increased risk of ischemic heart disease, stroke, or heart failure. Most analyses were subject to significant heterogeneity and further research, with careful attention to CV risk factors, is needed to clarify CV risk in DTC survivors.
Registration:
PROSPERO CRD42021244743
Introduction
Thyroid cancer is the most common endocrine malignancy, representing 3% of global incidence of all cancers, with 586,000 incident cases worldwide in 2020 alone (1). However, thyroid cancer-specific mortality risk is low (1,2), making long-term risk of mortality and morbidity from other causes an important consideration. Differentiated thyroid cancer (DTC) is the most common type of thyroid cancer (3). DTC treatments include thyroidectomy, thyroid hormone for replacement or thyrotropin (TSH) suppression, and radioactive iodine (3). Exogenous thyroid hormone excess in DTC survivors may potentially contribute to adverse cardiac events (4 –8). TSH suppression and metabolic risk factors, which are associated with DTC development, may increase the risk of cardiovascular (CV) events in this population.
CV risk factors, such as metabolic syndrome (9 –13), are associated with the risk of developing thyroid cancer. A large prospective cohort study suggested that women with diabetes (but not men) had a significantly increased risk of thyroid cancer (14). Thyroid cancer survivors may also be at increased CV risk, as a large population-based study suggested that thyroid cancer survivors had a 2-fold increased risk of hypertension and a 1.7-fold increased risk of dysglycemia, compared with controls (15). Adverse metabolic risk factors that may predispose to thyroid cancer may, thus, contribute to an increased risk of CV morbidity and mortality in DTC survivors. A better understanding of CV outcomes in DTC survivors is needed, with attention to CV risk factors.
We performed a systematic review and meta-analysis to estimate the CV mortality risk in adult DTC survivors, compared with age- and gender-matched controls. Secondary outcome analyses included risk estimates of atrial fibrillation, stroke, ischemic heart disease, and heart failure. Our prioritized focus was on studies that adjusted for established CV risk factors; however, crude, unadjusted data were also examined.
Methods
We conducted a systematic review and meta-analysis and reported our study procedure and findings according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement (16). The protocol for this systematic review and meta-analysis was registered in PROSPERO (CRD42021236180).
Eligibility criteria
The population, intervention, comparator, and outcome components of our research question were as follows: (i) Population: DTC survivors aged ≥18 years (diagnosis confirmed by histologic confirmation, regardless of age at diagnosis), (ii) intervention: DTC treated by thyroid surgery (total or partial thyroidectomy), (iii) comparison group(s): age- and gender-matched controls from the general population without thyroid cancer, (iv) follow-up period after thyroidectomy of at least 1 year (for the DTC group), (v) outcomes(s) and measures: CV mortality (primary outcome) or CV morbidity (secondary outcomes).
Secondary CV morbidity included any of the following outcomes: (i) atrial fibrillation, (ii) ischemic heart disease, (iii) stroke, and (iv) heart failure (excluding perioperative events within 1 month of any thyroid cancer surgery). We examined observational studies (cohort and cross-sectional studies, excluding case reports), which included a general population control group comparison.
The primary outcome was CV mortality, defined as a CV event that directly resulted in death (per original authors' definition). Examples of qualifying CV events for CV death included: myocardial infarction, stroke, or aortic aneurysm. Our secondary study outcomes of new onset of non-fatal CV events included: atrial fibrillation, ischemic heart disease (including myocardial infarction, angina), stroke, or heart failure.
Our first priority was to examine data adjusted for CV risk factors, such as hypertension, diabetes, hypercholesterolemia, increased body mass index (BMI), smoking, or any combination of these. However, we also reviewed and analyzed crude data (unadjusted for these CV risk factors), due to a paucity of available adjusted data.
We excluded papers that did not meet our inclusion criteria, studies that were case reports, studies that focused on pediatric cohorts, studies on thyroid cancer patients other than DTC, duplicate or overlapping study population reports (i.e., excluding the smaller or earlier overlapping study), and papers not reported in English.
Search strategy
An electronic search of five databases (Medline, Medline-in-Process, Medline Epub Ahead of Print, Embase (OvidSP), and Cochrane Library (Wiley)) from 1946 to October 22, 2021, was performed by an experienced information specialist (EU, details in Supplementary Table S1). The electronic search was supplemented by a hand search of relevant cross-references and papers from files of a senior author (A.M.S.). Content experts (A.M.S., S.E., and L.L.L.) were consulted for any potentially relevant additional studies.
Data collection and appraisal
Two reviewers (J.K.Q. and R.A.) independently screened citations. Studies deemed potentially suitable for inclusion by either reviewer were retrieved for full text review and were independently reviewed by the two reviewers. Citations were tracked, and reviewers' data were collected electronically (Covidence, Australia). Data extraction and collection was independently completed using piloted forms by two abstractors (J.K.Q., R.A.).
Risk-of-bias assessment of all eligible studies was completed by two independent reviewers (J.K.Q. and R.A.) using the CLARITY tool (17). Authors of the original studies were contacted via email for clarification regarding study data and if any critical, missing data needed to be obtained. If consensus could not be achieved between the two reviewers on inclusion of studies, data extraction, or quality assessment, disagreement was resolved by another investigator (A.M.S.).
Statistical analysis/data synthesis
Descriptive data were summarized in percentages for categorical data and mean or median ± standard deviation (SD) or interquartile range (IQR) for continuous data. Random effects meta-analyses estimating the relative risk (risk ratio, RR, with confidence intervals [CI]), of age- and gender-adjusted CV mortality compared with the general population were performed for data adjusted for CV risk factors and unadjusted crude data, respectively.
Studies on CV mortality that did not account for competing risks of death from a non-CV cause were included; however, we performed a subgroup analysis where we pooled studies that provided a Fine and Gray (18) estimate of CV mortality. We assumed that other summary measures including hazard ratio, standardized mortality ratio (SMR), odds ratio, and standardized incidence ratio approximated relative risk in studies with a low event rate (<10% cumulative mortality incidence within the follow-up period) (19). The generic inverse variance method was used in pooling the relative risk estimates with a risk ratio of >1 representing increased risk (20).
The χ2 statistic (Q statistic) (21) and I 2 statistic (22) were used to determine the degree of heterogeneity across all the studies. In interpreting the I 2 statistic, we considered <25% as low, 25–50% as low-moderate, 51–75% as moderate, and >75% as large variation across studies (23). Sensitivity analyses were performed to explore the effect of study quality and follow-up duration on risk estimates and to explore sources of heterogeneity. For studies that reported the risk of CV mortality and incidence of non-fatal CV diseases stratified by histopathological subtype, without an overall risk estimate, we included the risk estimate for each of the subtypes separately in the meta-analysis.
We planned to assess for publication bias visually using a funnel plot, if there were at least 10 studies for the outcome examined. Review Manager (RevMan) Version 5.4.1 (24) was used for all meta-analyses. All statistical tests were two-sided, with p-value <0.05 considered statistically significant.
Results
We identified 3409 unique citations. A total of 65 full text articles were reviewed, of which 58 were excluded as they met one or more exclusion criteria (Fig. 1). We included seven observational studies (25 –31). The characteristics of the included studies are described in Table 1. Supplementary Table S2 summarizes the risk factors that were accounted for in the adjusted analyses, according to outcome. A list of excluded studies and reasons for exclusion are provided in Supplementary Table S3.

Study flow diagram. *For CV death (four studies total, one adjusted for CV risk factors); atrial fibrillation (five studies total, three adjusted for CV risk factors); cardiac ischemia (three studies total, one adjusted for CV risk factors), stroke (three studies total, two adjusted for CV risk factors), heart failure (three studies total, two adjusted for CV risk factors). CV, cardiovascular.
Description of Included Studies and Overall Risk-of-Bias Assessment, Assessed Using the CLARITY Tool
All eligible patients seen in clinic in 2009–2010 were included.
Authors reported that patients underwent TSH suppression for a mean of 11 years.
Authors included patients diagnosed with thyroid cancer at age 15 and above.
Overall cohort.
These two studies were part of a larger study called PREVEND “Prevention of REnal and Vascular ENd-stage Disease (PREVEND)” but examined different outcomes.
Patients were classified according to the risk of recurrence of DTC: low (Tx-T2, Nx-N0, Mx-M0), intermediate (any T3 or N1 tumor), or high (any T4 or M1 tumor).
Examined primary outcome of CV mortality.
Examined secondary outcome of atrial fibrillation.
CV, cardiovascular; DTC, differentiated thyroid cancer; IQR, interquartile range; RAI, radioactive iodine; SD, standard deviation; SEER, Surveillance, Epidemiology, and End Results; THIN, The Health Improvement Network database; TSH, thyrotropin.
Risk of CV mortality
Only one study, by Klein Hesselink et al. examined the risk of CV mortality after adjustment for CV risk factors (25). This was a retrospective cohort study, which compared the risk of CV mortality in 524 DTC patients from two Dutch centers with 1572 age- and gender- matched controls from a population-based epidemiologic study. The mean age of the subjects was 49 years (SD 14 years). The median follow-up period was 8.5 years (IQR 4.1–15.9 years) for DTC patients and 10.5 years (IQR 9.9–10.9 years) for controls. The geometric mean TSH in the DTC group was 0.11 [CI 0.09–0.12].
Klein Hesselink et al. reported that 22 out of 100 deaths among 524 DTC patients (4.2%) were attributed to CV disease whereas 24 out of 85 controls (1.5% of overall control population) died from CV causes (25). The DTC patients were reported to have an increased risk of CV mortality (adjusted RR [aRR] 3.35 [CI 1.66–6.74]), adjusted for the presence of pre-existing CV disease or CV risk factors (age, gender, BMI, diabetes, smoking, hypertension, hypercholesterolemia). The authors reported that in the DTC group, a lower TSH value was associated with a higher risk of CV mortality among these DTC patients (aRR 3.08 [CI 1.32–7.21], for each 10-fold decrease in geometric mean TSH).
Four large cohort studies (25 –27,31), including 167,726 DTC survivors, examined CV mortality risk without adjustment for CV risk factors. Subgroup data were examined from one study (26). The mean age at DTC diagnosis ranged from 44 to 55 years among these studies. The mean follow-up duration ranged from 8 to 18 years. Two of these studies adjusted for competing risks of death from non-CV causes (26,27). Pajamäki et al. (27) reported on TSH levels in 469 out of 901 patients. In this cohort, 215 (46%) patients had a geometric mean TSH of <0.1 mIU/L, 163 (35%) had TSH 0.1–0.5 mIU/L, and 89 (19%) had TSH >0.5 mIU/L (27).
Du et al. (26) reported on data from 159,401 DTC patients (147,864 papillary, 11,537 follicular) who were diagnosed with DTC between 1975 and 2015, and who were included in the Surveillance, Epidemiology, and End Results (SEER) database (from the United States), The mean follow-up period was 8.4 years. Of the 14,321 deaths that occurred in the papillary thyroid cancer group, 3422 occurred due to CV causes (2.3% of the overall papillary group). Compared with the age- and gender-matched general population, the SMR was 0.57 [CI 0.55–0.59] in patients with papillary thyroid cancer. Of the 2576 deaths that occurred in the follicular thyroid cancer group, 658 cases (5.7% of overall follicular group) were attributed to CV disease (SMR 1.14 [CI 1.06–1.23]). Pajamäki et al. (27) followed 901 Finnish DTC patients over a median of 18.8 years (IQR 14.4–23.5 years). In total, 81 CV deaths occurred in the DTC group (8.9%) compared with 533 out of 4485 (11.9%) in controls (27). Zoltek et al. (31) compared CV mortality in 6900 Swedish DTC patients with the general population. Over a mean follow-up period of 9.6 years, 550 out of 6900 (8%) of DTC patients experienced CV death and the SMR was 1.02 [CI 0.94–1.10].
In a meta-analysis of crude data (unadjusted for CV risk factors), the RR of CV death in the DTC group was 0.96 ([CI 0.65–1.42], N = 4 studies, 167,726 DTC patients, median follow-up 8.4–18.8 years, I 2 = 99%, Fig. 2). Adjusting for competing risks of death from non-CV causes and stratifying by follow-up duration and study quality revealed similar risk estimates and did not explain the heterogeneity among studies (Fig. 2). The number of eligible studies for inclusion was too small (<10) to generate a meaningful funnel plot to formally examine for publication bias.
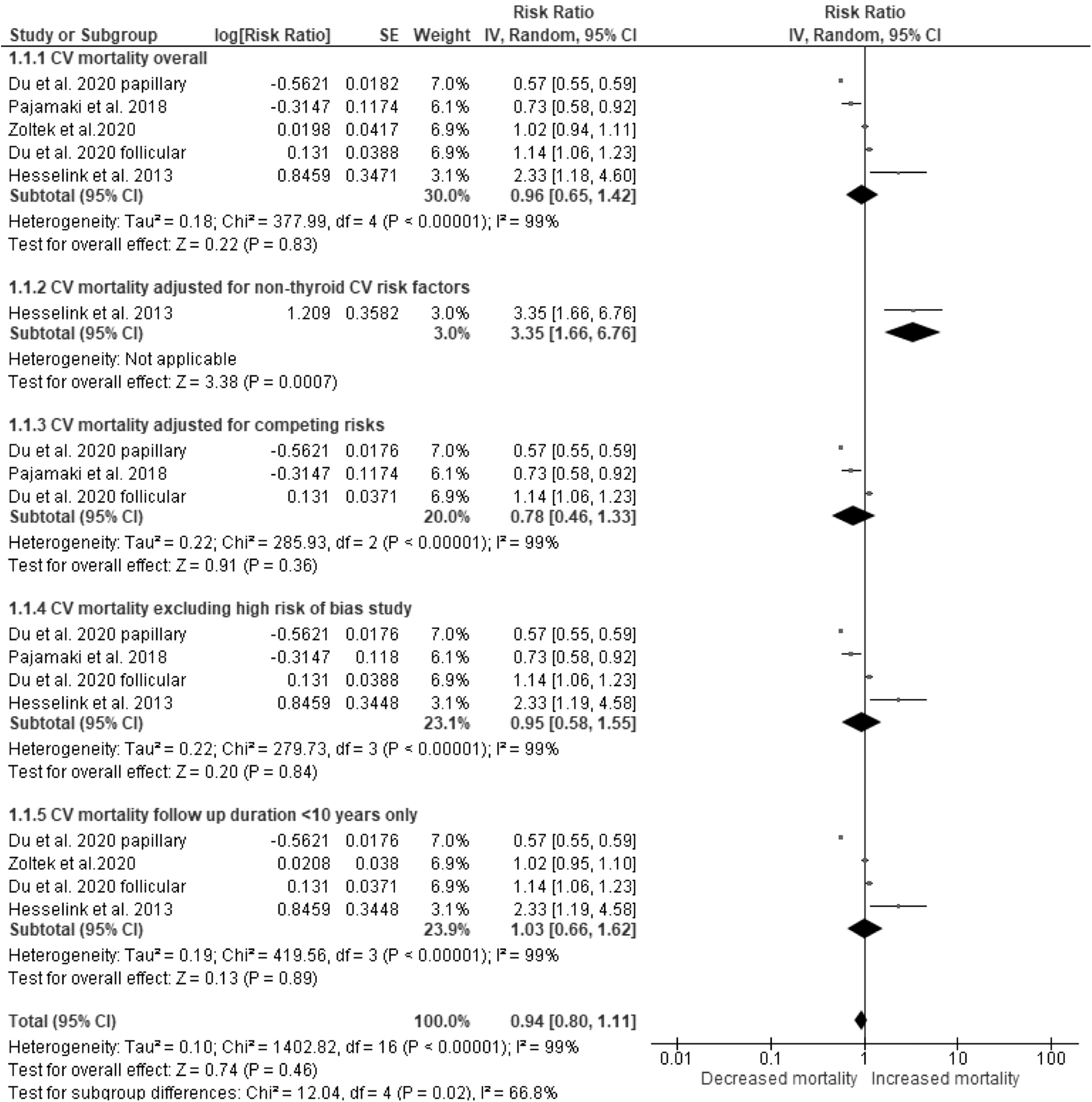
Age- and gender-adjusted long-term CV mortality comparing DTC survivors with controls. Forest plot showing a random-effects meta-analysis of age- and gender-adjusted, long-term risk of CV mortality (1.1.1). 1.1.2. Shows the risk estimate for the one study that accounted for non-thyroid CV risk factors. 1.1.3. Shows the random-effects meta-analysis adjusting for competing risks of death from non-CV causes. 1.1.4. Shows a sensitivity analysis where a study with a high overall risk of bias was excluded. 1.1.5. Shows another sensitivity analysis where studies with <10 years of follow-up were included. The diamond at the bottom of the figure represents the pooled relative risk (risk ratio). DTC, differentiated thyroid cancer.
Risk of CV morbidity
Atrial fibrillation
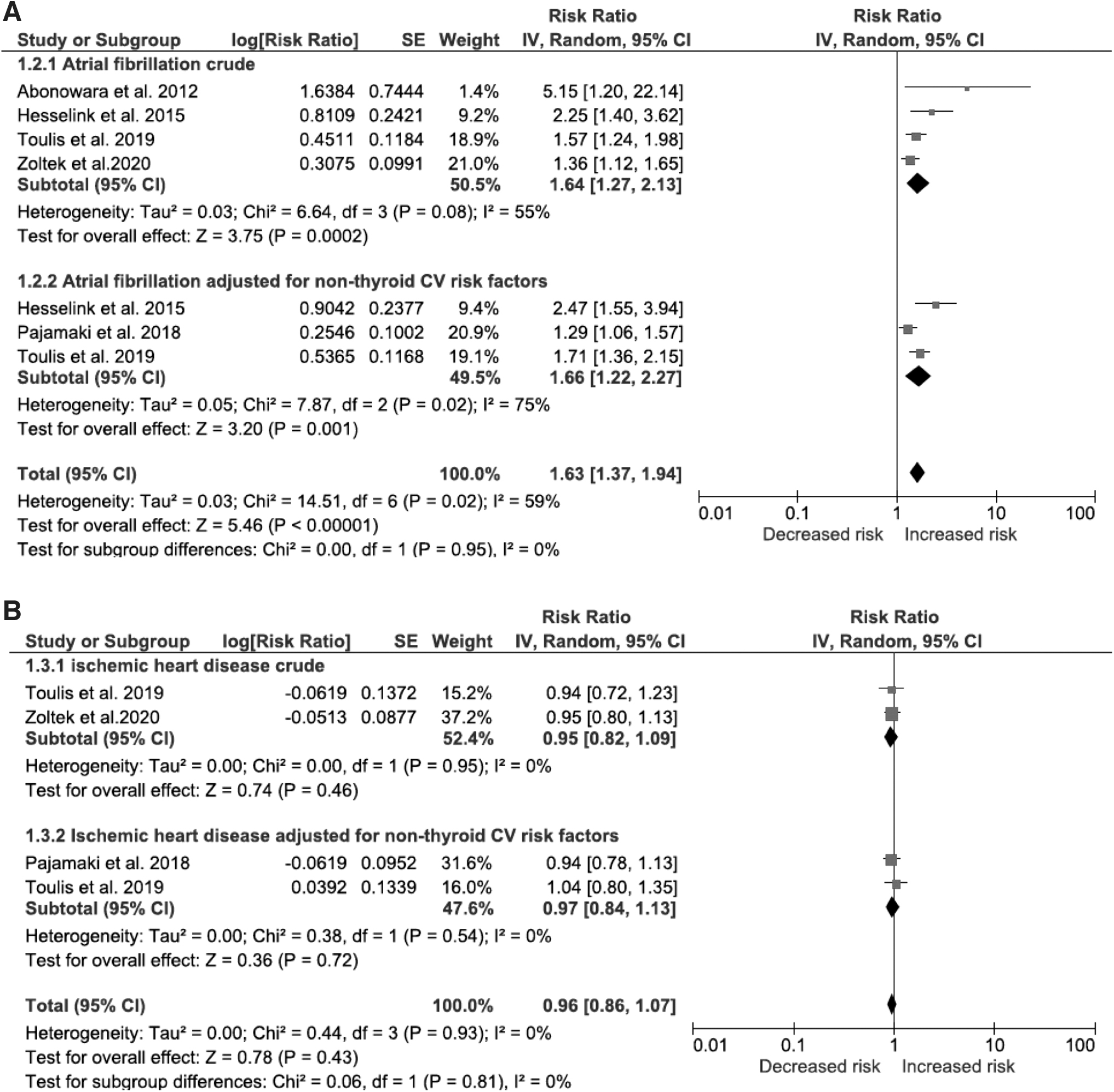
Three studies including a total of 4428 DTC patients compared the risk of atrial fibrillation risk in DTC patients compared with the general population, after adjusting for CV risk factors (risk factors shown in Supplementary Table S2) (27,29–30). The median follow-up periods in these studies ranged from 5.0 to 18.8 years (27,29–30). The respective study characteristics are shown in Table 1. In total, 257 out of 4428 (5.8%) of DTC and 789 out of 17,351 (4.5%) of controls developed atrial fibrillation. After adjustment for CV risk factors, the aRR for atrial fibrillation was 1.66 ([CI 1.22–2.27], I 2 of 75%, N = 3 studies, 4428 DTC cases Fig. 3a).
(
A total of 4 studies, including 10,563 DTC cases, with a median follow-up period of 5.0–11.0 years, examined the risk of atrial fibrillation, without adjustment for CV risk factors (28 –31). In the meta-analysis of unadjusted crude data, the RR was 1.64 ([CI 1.27–2.13], I 2 = 55%, 4 studies, 10,563 DTC patients, Fig. 3a).
Ischemic heart disease
Two studies including 3910 DTC patients, with a median follow-up period of 5.0–18.8 years, examined the risk of ischemic heart disease comparing DTC patients with non-DTC controls, after adjusting for non-thyroid CV risk factors (27,30). Supplementary Table S2 shows the risk factors that were adjusted for in the analyses. The pooled aRR for ischemic heart disease was 0.95 ([CI 0.82–1.09], I 2 of 0%, 2 studies, 3910 DTC patients, Fig. 3b).
Two studies, including a total of 9909 DTC cases, with a median follow-up period of 5.0–9.7 years, reported on the risk of ischemic heart disease (without adjustment for CV risk factors) (30,31). In pooling crude, unadjusted data, the ischemic heart disease risk in DTC survivors compared with controls was estimated as RR 0.97 ([CI 0.84–1.13], and I 2 of 0% Fig. 3b).
Cerebrovascular disease
Two studies including 3910 DTC patients, with a median follow-up period of 5.0 to 18.8 years, examined stroke risk in DTC survivors as compared with the general population, after adjusting for non-thyroid CV risk factors (risk factors shown in Supplementary Table S2) (27,30). After adjustment for CV risk factors, the aRR for cerebrovascular disease was 1.14 for DTC survivors compared with controls ([CI 0.84–1.55], I 2 = 69%, N = 2 studies, 3910 DTC cases, Supplementary Fig. S1).
In pooling crude data, unadjusted for CV risk factors, the stroke risk in DTC cases was estimated as RR 1.03 ([CI 0.81–1.31], and I 2 = 65%, N = 2 studies, 9909 DTC cases, mean follow-up 5.0–9.7 years, Supplementary Fig. S1), as compared with controls (30,31).
Heart failure
Two studies including 3910 DTC patients, with median follow-up periods of 5.0–18.8 years, examined the risk of heart failure risk in DTC survivors as compared with the general population, after adjusting for non-thyroid CV risk factors (risk factors shown in Supplementary Table S2) (27,30). After adjustment for CV risk factors, the risk of heart failure in DTC survivors was estimated as aRR 0.98 ([CI 0.60–1.59], and I 2 = 79%, N = 2 studies, 3910 DTC cases), as compared with controls (Supplementary Fig. S2).
The unadjusted, crude estimate for heart failure risk in DTC was estimated as RR 0.99 ([CI 0.88–1.10], I 2 = 0%, N = 2 studies, 9909 DTC cases, mean follow-up 5.0–9.7 years, Supplementary Fig. S2).
Risk-of-bias assessment and evaluation of the quality of evidence
The overall risk of bias for most of the included studies was found to be moderate, as assessed by the CLARITY tool (Table 1). The results of the individual domains of assessment are shown in Supplementary Table S4.
Discussion
Earlier studies have suggested that the risk of CV mortality and morbidity in DTC survivors may be increased compared with the general population. However, the risk of CV mortality and morbidity after accounting for CV risk factors has been unclear, and it was the subject of this systematic review.
Klein Hesselink et al. reported an increased risk of CV mortality in DTC survivors compared with the general population, after adjustment for CV risk factors (25). However, in pooling crude data that were not adjusted for CV risk factors, we observed no significant difference in the risk of CV death between DTC survivors and controls. The differences between adjusted and non-adjusted analyses also underscore the importance of statistical adjustment for relevant confounders, which may provide a less biased estimate for the true association between an exposure and an outcome (32). This concept is particularly important in the case of DTC survivors, where CV risk factors may also be associated with the risk of the malignancy.
It is of clinical interest to explore the potential relationship between TSH suppression with levothyroxine and CV outcomes of DTC survivors. However, under-reporting of details of TSH suppression in CV outcome studies limits the ability to analyze this outcome in this meta-analysis. In our review, only two of the four eligible studies examining the unadjusted primary outcome reported any TSH values (25,27).
Klein Hesselink et al. (25) showed that with adjustment for age, sex, non-thyroid CV risk factors, DTC risk classification, histology, cumulative radioiodine dose, and neck radiotherapy, TSH suppression was associated with a higher CV mortality with an hazard ratio (HR) of 3.08 [CI 1.32–7.21], but not all-cause mortality (HR 1.43 [CI 0.97–2.12]). Pajamäki et al. (27) showed in subgroup analysis that the patients with a geometric mean TSH level under 0.1 mU/L had an increased risk of CV disease (HR 1.27 [CI 1.03–1.58]), as compared with controls.
We observed an increased risk of atrial fibrillation in DTC survivors compared with the general population in meta-analyses adjusted and not adjusted for CV risk factors. However, in adjusted and non-adjusted analyses, the risk of ischemic heart disease, stroke, and heart failure, risks were not significantly different between DTC survivors and controls.
Given the well-established knowledge of the association between atrial fibrillation and hyperthyroidism, it is important for clinicians to carefully consider the need for TSH suppression in the treatment of DTC survivors. The 2015 American Thyroid Association guidelines recommend TSH suppression in those at intermediate or high risk for recurrence and in those with indeterminate, biochemically, or structurally incomplete response to treatment (3). Therefore, patients who have low-risk disease or have achieved an excellent response to treatment are unlikely to benefit and may be potentially harmed by TSH suppression. It is important to reflect on our findings in light of other recently published systematic reviews and meta-analyses examining CV risk in thyroid cancer patients in general (not specifically restricted to DTC), without adjustment for CV risk factors (33,34). With respect to atrial fibrillation, both Lee et al. (33) and Kostopoulos et al. (34) estimated a 1.5-fold increased risk of atrial fibrillation in pooled analyses, including 18 and 6 studies, respectively, but neither meta-analyses accounted for CV risk factors. We observed a relatively similar 1.7-fold increased risk of atrial fibrillation based on three studies that did adjust for CV risk factors.
With respect to ischemic heart disease and cerebrovascular disease, our finding of no significant increase in the risk in DTC survivors after adjustment for CV risk factors contrasted with that of a recently published meta-analysis by Lee et al. (33) (coronary artery disease RR = 1.10 [CI 1.00–1.21], cerebrovascular accidents RR = 1.15 [CI 1.09–1.20]). We believe that the positive association between DTC and ischemic heart disease and cerebrovascular disease observed in the meta-analysis by Lee et al. (33) may be primarily attributed to two studies (35,36), which were not entirely DTC cohorts and were thus excluded from our meta-analysis.
One of these studies (35) used data from the Korean National Health Insurance database, which may be subject to some differences in the cancer registry validation procedure (37), and which is known to be enriched in low-risk papillary carcinomas detected as part of a national mass-screening program. Heterogeneity in the study population, variability in data quality, and TSH levels may have also contributed to the differences in results. For example, Suh et al. (35) showed that the risk of ischemic heart disease and ischemic stroke may be mediated by thyroxine dose. Those who received 145–160 or >170 mcg/day of levothyroxine had a higher risk of ischemic heart disease with an HR of 1.19 [CI 1.07–1.31] and 1.47 [CI 1.34–1.6], respectively. Similarly, those who were exposed to a higher dose of levothyroxine had a higher risk of ischemic stroke with an HR of 1.22 [CI 1.1–1.36] for the 145–169 mcg/day group and HR of 1.56 [CI 1.42–1.72] for the >170 mcg/day group. TSH was not available in the study by Izkhakov et al. (36).
The strengths of the current study are that we conducted a comprehensive, systematic literature search, and we applied stringent inclusion criteria to ensure that risk estimates were pooled from only DTC survivors. Two reviewers independently screened and evaluated relevant studies, and the quality of studies was appraised using an established quality appraisal tool. We also focused on CV mortality, which is of primary clinical importance but has not been specifically examined in other systematic reviews. We also pooled data statistically adjusted for CV risk factors, which has not been performed in previously published meta-analyses.
However, our study is also subject to several limitations. First, there was a limited number of studies that adjusted for CV risk factors for all outcomes, but particularly for the primary outcome of CV mortality. The meta-analyses of crude data are subject to bias from potential confounders from the original studies. Second, the overall risk of bias for most studies was moderate for most studies. We also relied on the authors' determination of CV death and other outcomes, as well as the identification of relevant CV risk factors, which may be subject to ascertainment bias and reporting. Third, residual confounding effects in terms of DTC treatments cannot be ruled out since details on thyroid hormone and radioactive iodine treatments were not available in many studies. Some of our meta-analyses were also subject to significant heterogeneity (i.e., atrial fibrillation [adjusted and crude data], stroke [adjusted and crude data], and congestive heart failure [adjusted data]). Finally, publication bias could not be meaningfully assessed due to the paucity of included studies.
In conclusion, we observed very limited evidence suggesting an increased risk of CV mortality and of atrial fibrillation in DTC survivors, after adjustment for CV risk factors. However, many of our meta-analyses were subject to significant heterogeneity. In the future, high-quality, prospective studies, with attention to stratification for CV risk factors and DTC treatments (e.g., TSH suppressive therapy) are needed to accurately define the risk of CV mortality and morbidity in DTC survivors.
Footnotes
Acknowledgments
The authors would like to thank Dr. Andrew Advani for critically reviewing the first draft of the manuscript. They also gratefully acknowledge the assistance of Drs. Saro Armenian, Ali Imran, and Kyeong Jin Kim in clarifying key patient characteristics in their respective publications.
Authors' Contributions
J.K.Q. designed the study, reviewed citations, critically appraised all studies, extracted data, performed the meta-analyses, and drafted the manuscript. R.A. reviewed citations, critically appraised all studies, and extracted study data; E.U. conducted the literature search; S.E. was a content expert and was consulted for additional potentially relevant studies, critically reviewed, and edited the manuscript. L.L.L. was consulted for additional potentially relevant studies. She also helped design the study, critically reviewed, and edited the manuscript. A.M.S. helped design the study, reviewed citations, critically appraised all studies, extracted data, reviewed, and edited the manuscript.
Author Disclosure Statement
J.K.Q., R.A., E.U., S.E., and L.L.L. have no conflicts of interest to declare. A.M.S. has no financial conflict of interest to declare; however, she is the current editor-in-Chief of Thyroid and she was blinded to the entire peer review process of this manuscript.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4