
Abstract
Background:
Hypothyroidism is a risk factor for dyslipidemia. We explored whether dyslipidemia is a risk factor for hypothyroidism.
Methods:
We performed a retrospective analysis of data from a longitudinal cohort study of South Korean adults who underwent medical examination and ≥4 biochemical assessments of thyroid function. The primary outcome was hypothyroidism (thyrotropin [TSH] >4.2 mU/L), and the secondary outcome was severe subclinical hypothyroidism (SCH; TSH ≥10.0 mU/L and normal free thyroxine [fT4] level) or overt hypothyroidism (OH; total triiodothyronine <80 ng/dL and/or fT4 < 0.93 ng/dL and high TSH values). The association of baseline dyslipidemia status with subsequent hypothyroidism was evaluated using Kaplan–Meier curves with the log-rank test and Cox proportional hazards regression models (for the entire population and respective genders). Subgroup analyses according to age (<40 and ≥40 years) and body–mass index (BMI; <23, 23–25, and ≥25 kg/m2) were performed according to gender.
Results:
We included 1665 participants. During a median follow-up period of 61.0 months, 24.3% (404/1665) individuals developed hypothyroidism. Among these, 36 participants (2.1%) had severe SCH or OH. Excluding patients with a first abnormal TSH level at last follow-up, 44.5% (126/283) of the patients with hypothyroidism had spontaneous TSH normalization. In respective multivariate analyses, dyslipidemia at baseline was independently associated with development of hypothyroidism in women (adjusted hazard ratio [HR] = 2.05 [1.31–3.19], p = 0.002), but not in men (adjusted HR = 1.00 [0.77–1.30], p = 0.991). In women, the presence of dyslipidemia at baseline was associated with development of severe SCH or OH (adjusted HR = 5.33 [1.41–20.12], p = 0.014). In women, respective associations according to age and BMI were as follows: age <40 years, adjusted HR = 2.90 (1.34–6.26, p = 0.007); age ≥40 years, adjusted HR = 1.85 (1.08–3.14, p = 0.023); BMI <23 kg/m2, adjusted HR = 1.68 (0.82–3.43, p = 0.151); BMI = 23–25 kg/m2, adjusted HR = 2.17 (0.93–5.07, p = 0.071); and BMI ≥25 kg/m2, adjusted HR = 2.82 (1.16–6.86, p = 0.022).
Conclusions:
In Korean adults, dyslipidemia was associated with development of hypothyroidism in women. Our findings require confirmation.
Introduction
The prevalence of dyslipidemia in South Korea is as high as 40%. 1 Dyslipidemia is the second highest and third highest risk factor for adverse cardiovascular outcomes in Korean women and men, respectively. 2 Hypothyroidism is also relatively common and may be associated with adverse cardiovascular outcomes. 3 –5 Therefore, levothyroxine replacement is recommended, especially for treating overt hypothyroidism (OH) and severe subclinical hypothyroidism (SCH). 6,7
In recent decades, cross-sectional studies have suggested an association between hypothyroidism and dyslipidemia. 8 –10 Furthermore, longitudinal studies have shown that hypothyroidism is a risk factor for dyslipidemia. 11,12 However, previous studies have focused on dyslipidemia as an outcome of hypothyroidism rather than as a risk factor for hypothyroidism.
Previous studies demonstrated that dyslipidemia promotes autoimmune activation and leads to autoimmune diseases such as systemic lupus erythematosus (SLE) and IgG nephritis. 13 –15 Considering that autoimmunity is the most common cause of hypothyroidism in iodine-sufficient areas, 16 it is hypothesized that dyslipidemia may be a risk factor for hypothyroidism. Until now, the role of hypothyroidism in dyslipidemia management is confined to it being a secondary cause of dyslipidemia.
Our aim was to determine whether dyslipidemia is a risk factor for development of hypothyroidism in South Korean adults. We further explored the potential effects of gender, age, and body–mass index (BMI) groups on this potential relationship.
Materials and Methods
Study design and study population
This was a retrospective analysis of longitudinal cohort data. A cohort of South Korean patients who completed an annual or biennial examination between 2007 and 2014 at the Gyeongsang National University Hospital (GNUH) Health Care Center in South Korea was assessed for eligibility (N = 2372).
The inclusion criteria were as follows: (1) age ≥18 years and (2) underwent medical examination and ≥4 serial thyroid hormone assessments. After excluding participants who unmet inclusion criteria (2 participants aged <18 years and 124 participants with <4 assessments of thyroid function), 2246 participants were included.
After further excluding participants with abnormal initial results of the thyroid function test (N = 294), missing anthropometric or laboratory data (N = 272), and a history of thyroid disease or recent medication affecting thyroid function (N = 15), 1665 participants were included in the final analysis (Fig. 1).
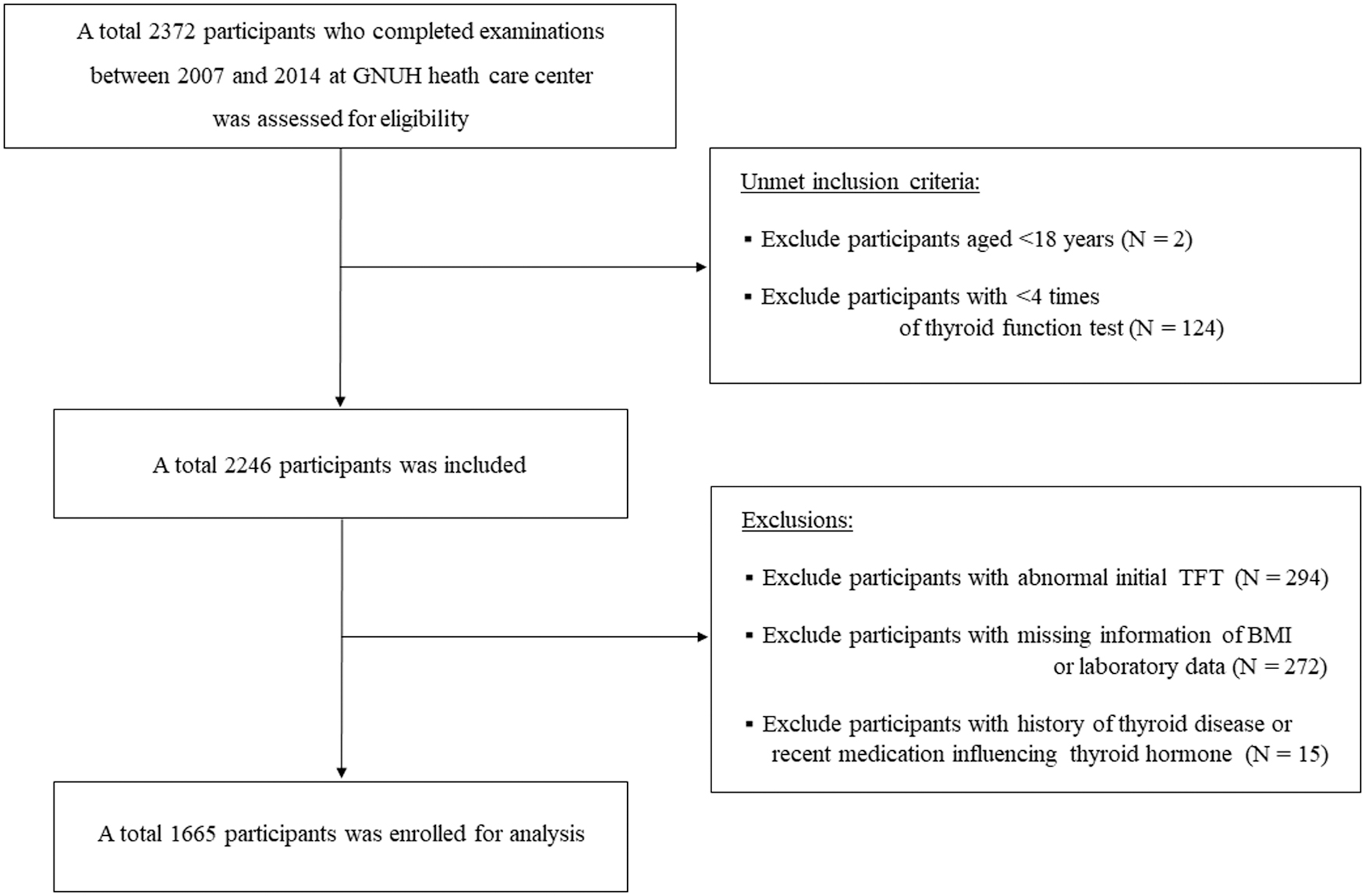
Flow chart of study participants.
This study was approved by the Institutional Review Board of GNUH (No. 2022-02-003) and the requirement for informed consent was waived by the review board.
Measurements
Demographic, anthropometric, and laboratory data were collected. Height and body weight were measured by trained nurses, and BMI was calculated as the body weight (kg) divided by height squared (m2). The following laboratory data were collected after overnight fasting: levels of low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), TG, aspartate aminotransferase (AST), alanine transaminase (ALT), creatinine, and HbA1c and the thyroid function.
A lipid profile, including LDL-C, HDL-C, and TG levels, was obtained using a homogeneous enzymatic colorimetric test (Roche Diagnostics Ltd., Mannheim, Germany; reference ranges of 0–130 mg/dL for LDL-C, 35–75 mg/dL for HDL-C, and 0–200 mg/dL for TG).
Thyrotropin (TSH), free thyroxine (fT4), and total triiodothyronine (TT3) levels were measured using an electrochemiluminescence immunoassay (Roche Diagnostics Ltd.; reference ranges of 0.27–4.2 mU/L for TSH, 0.93–1.70 ng/dL for fT4, and 80–200 ng/dL for TT3; intra-assay coefficient variation [CV] ranges of 1.1–2.3% for TSH, 1.7–2.3% for fT4, and 4.3–7.8% for TT3; and interassay CV ranges of 1.4–2.9% for TSH, 1.4–2.5% for fT4, and 4.6–12.3% for TT3).
The participants who recorded mild TSH elevation repeated the thyroid function test within 2 weeks and the lower TSH level was recorded.
Study outcomes and definitions
The primary outcome was development of hypothyroidism, which was defined as a serum TSH level greater than the normal upper limit (4.2 mU/L). When the TSH level was normalized by a repeated test within 2 weeks, we assumed it was not hypothyroidism. OH and severe SCH are widely accepted indications for levothyroxine replacement. 7
Therefore, development of OH (hypothyroidism with TT3 < 80 ng/dL and/or fT4 < 0.93 ng/dL and abnormally high TSH values) or severe SCH (hypothyroidism with TSH ≥10.0 mU/L and normal fT4 level) 5 was used as the secondary outcome in the sensitivity analysis.
Participants with any of the following features were defined as having dyslipidemia: (1) TG ≥200 mg/dL, (2) LDL-C ≥ 160 mg/dL, and (3) HDL-C ≤ 40 mg/dL. 1 In addition to the initial dyslipidemia status, age, gender, BMI, initial TSH, and initial diabetes status were included as adjustment variables. AST, ALT, and creatinine levels were also adjusted because the liver function impacts thyroid hormone metabolism 18 and the prevalence of hypothyroidism increases consistently with an increasing creatinine level. 19,20
To evaluate the different effects of dyslipidemia on hypothyroidism risk by age, subgroup analyses of age at baseline (<40 and ≥40 years) were performed. 21 BMI was classified into three subgroups [<23 (normal), 23–25 (overweight), and ≥25 kg/m2 (obese)] using criteria specific to the Asian population. 6
Statistical analyses
All continuous variables are presented as medians and interquartile ranges (IQRs), and all categorical variables are presented as numbers and percentages. The Mann–Whitney U test was used to compare continuous variables, and the chi-square test was used to compare categorical variables. To assess whether the baseline dyslipidemia status was associated with the risk of subsequent hypothyroidism in each subgroup, Kaplan–Meier curves with the log-rank test and Cox proportional hazards regression models were generated.
Hazard ratios (HRs) with 95% confidence intervals are reported. A correlation analysis was used to conduct a post hoc secondary analysis of change in the TSH level and BMI. The statistical analyses were performed using IBM SPSS Statistics for Windows (version 22.0; Armonk, NY, USA). Two-sided p-values of <0.05 were considered statistically significant.
Results
Baseline characteristics
Baseline characteristics of the 1655 participants are presented in Table 1. In the study population, 35.0% (583/1680) were women, and median age at baseline was 43.0 years (IQR = 37.0–50.0 years). The median BMI was 23.7 kg/m2 (21.8–25.7 kg/m2). The median initial AST, ALT, and creatinine levels were 21.0 IU/L (17.0–26.0 IU/L), 21.0 IU/L (15.0–30.0 IU/L), and 0.81 mg/dL (0.67–0.93 mg/dL), respectively.
Baseline Characteristics of Participants According to Dyslipidemia Status
Statistically significant p-values (p-values <0.05) are indicated in bold.
Mann–Whitney U test.
Chi-square test.
AST, aspartate aminotransferase; ALT, alanine transaminase; BMI, body–mass index; fT4, free thyroxine; IQR, interquartile range; TSH, thyrotropin; TT3, total triiodothyronine.
The median serum TSH, fT4, and TT3 levels were 1.69 mU/L (IQR = 1.19–2.34 mU/L), 1.31 ng/dL (1.20–1.43 ng/dL), and 109.0 ng/dL (98.13–119.90 ng/dL), respectively. Among the participants, 29.6% (493/1665) had dyslipidemia and 9.1% (152/1665) had diabetes at baseline. The participants with dyslipidemia were older with slightly higher BMI and AST, ALT, and HbA1c levels than those without dyslipidemia.
There was no significant difference in the serum TSH, fT4, TT3, and creatinine levels between the two groups.
Development of hypothyroidism and survival analysis for all participants
During the follow-up period of a median of 61.0 months (IQR = 51.0–71.0 months), 24.3% (404/1665) of participants developed hypothyroidism, with the median time to onset of 36.0 months (23.0–49.0 months). Except for participants who recorded first hypothyroidism at last follow-up, a considerable proportion (126/283, 44.5%) showed spontaneous normalization of TSH levels during follow-up.
Among the participants who developed hypothyroidism, 29 (1.7%) and 7 (0.4%) had severe SCH and OH, respectively. Kaplan–Meier curves showed that dyslipidemia was significantly associated with the risk of developing hypothyroidism (log-rank p = 0.026) (Fig. 2A). Similar associations were observed for severe SCH or OH (log-rank p = 0.016; Fig. 2D).

Kaplan–Meier graphs for hypothyroidism in all (
However, in the multivariable analysis, statistical significance was absent for hypothyroidism (adjusted HR = 1.20 [0.95–1.50]; p = 0.116) (Table 2), whereas the significance for severe SCH or OH (adjusted HR = 2.22 [1.07–4.61]; p = 0.031) was sustained (Table 3).
Multivariate Cox Proportional Hazards Models for Hypothyroidism Risk
Statistically significant p-values (p-values <0.05) are indicated in bold.
Model: adjusted for age, gender, BMI (kg/m2), AST level (IU/L), ALT level (IU/L), creatinine level (mg/dL), diabetes status, initial TSH level (mU/L), and dyslipidemia status.
Model: adjusted for age, BMI (kg/m2), AST level (IU/L), ALT level (IU/L), creatinine level (mg/dL), diabetes status, initial TSH level (mU/L), and dyslipidemia status.
CI, 95% confidence interval; HR, hazard ratio; TSH, thyrotropin.
Multivariate Cox Proportional Hazards Models for the Risk of Severe Subclinical Hypothyroidism or Overt Hypothyroidism
Statistically significant p-values (p-values <0.05) are indicated in bold.
Model: adjusted for age, gender, BMI (kg/m2), AST level (IU/L), ALT level (IU/L), creatinine level (mg/dL), diabetes status, initial TSH level (mU/L), and dyslipidemia status.
Model: adjusted for age, BMI (kg/m2), AST level (IU/L), ALT level (IU/L), creatinine level (mg/dL), diabetes status, initial TSH level (mU/L), and dyslipidemia status.
A high LDL-C level (adjusted HR = 1.53 [1.11–2.10]; p = 0.008) rather than a low HDL-C level (adjusted HR = 1.06 [0.79–1.41]; p = 0.691) or high TG level (adjusted HR = 0.93 [0.68–1.27]; p = 0.672) was more strongly associated with incident hypothyroidism in the multivariable analysis, including TG ≥200 mg/dL, LDL-C ≥ 160 mg/dL, and HDL-C ≤ 40 mg/dL, instead of dyslipidemia (Supplementary Table S1).
Gender-specific analyses
We performed the same survival analysis for men and women. Kaplan–Meier curves for hypothyroidism risk in men (log-rank p = 0.723) (Fig. 2B) and women (log-rank p = 0.001) (Fig. 2C) were generated according to the initial dyslipidemia status. In the multivariate analysis, having dyslipidemia at baseline was the risk factor most strongly associated with development of hypothyroidism (adjusted HR = 2.05 [1.31–3.19]; p = 0.002) in women. However, this association was insignificant in men (adjusted HR = 1.00 [0.77–1.30]; p = 0.991) (Table 2).
The association of dyslipidemia with the risk of severe SCH or OH was significant in women (log-rank p = 0.001; Fig. 2F), but insignificant in men (log-rank p = 0.349; Fig. 2E). The multivariate analysis showed that dyslipidemia at baseline was also an independent risk factor for severe SCH or OH in women (adjusted HR = 5.33 [1.41–20.12]; p = 0.014), but not in men (adjusted HR = 1.66 [0.72–3.85]; p = 0.231) (Table 3).
In summary, gender-specific survival analyses demonstrated that dyslipidemia was independently associated with hypothyroidism risk only in women.
Subgroup analyses according to age in men and women
Subgroup analyses were performed in men and women. When the women were classified into two subgroups according to age (<40 and ≥40 years), the effect of dyslipidemia on hypothyroidism risk was as follows: age <40 years, adjusted HR = 2.90 (1.34–6.26, p = 0.007); and age ≥40 years, adjusted HR = 1.85 (1.08–3.14, p = 0.023) (Fig. 3A and Supplementary Table S2).
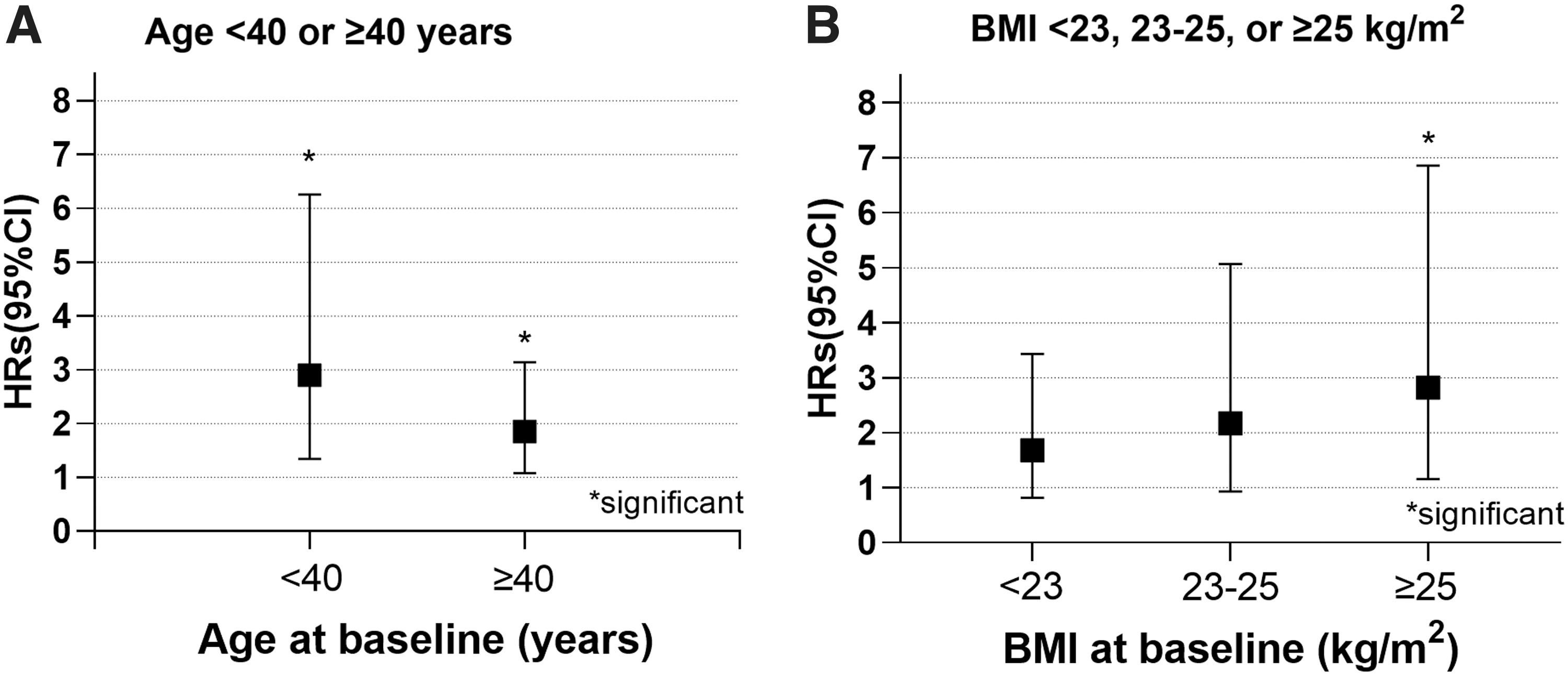
Comparison of the adjusted HRs of hypothyroidism according to subgroups of women participants aged <40 (N = 234) or ≥40 years (N = 349) (
Subgroup analysis according to BMI in men and women
After dividing the women into three BMI subgroups (<23, 23–25, and ≥25 kg/m2), the adjusted HRs of the effect of dyslipidemia at baseline on hypothyroidism risk were 1.68 (0.82–3.43; p = 0.151), 2.17 (0.93–5.07; p = 0.071), and 2.82 (1.16–6.86; p = 0.022), respectively. The effect of dyslipidemia on hypothyroidism risk successively increased as BMI increased and was significant only in obese subgroups (Fig. 3B and Supplementary Table S3).
In a post hoc secondary analysis of women participants with dyslipidemia (N = 84), the change in TSH level from baseline was significantly linearly associated with baseline BMI (r = 0.218, p = 0.048) rather than BMI change (r = −0.106, p = 0.336).
Discussion
In this retrospective analysis of longitudinal cohort data, we found that dyslipidemia was a risk factor for developing hypothyroidism in women. The association of dyslipidemia with incident hypothyroidism in women was most prominent in young participants aged <40 years and in obese participants (BMI of ≥25 kg/m2).
Previous studies 11,12,22 have shown that the thyroid hormone plays a role in lipid metabolism and dyslipidemia is an outcome of hypothyroidism. However, this is the first longitudinal study to demonstrate that dyslipidemia is also a risk factor for hypothyroidism. The fact that the sensitivity analysis, including severe SCH or OH, was concordant with the main analysis supports the validity of our findings. The possible mechanism is autoimmunity, which is the most common cause of hypothyroidism in iodine-sufficient areas. 16
Notably, dyslipidemia leads to development of other autoimmune diseases, such as SLE and IgG nephritis, by autoimmune activation 13,15 through follicular helper T cells with interleukin 27 and IgG autoantibodies. 14 Furthermore, several studies 23,24 have reported that lipid-reducing agents relieve the severity of autoimmunity. Similarly, hydroxychloroquine, an immune modulator widely used in SLE, is associated with reduction in LDL-C levels in patients with SLE. 17 Taken together, autoimmunity and dyslipidemia are closely related.
A study from Greece 25 previously demonstrated a higher incidence of dyslipidemia (25% vs. 6%) in patients with positive thyroid autoantibodies than in normal individuals, supporting our hypothesis. Among the components of dyslipidemia, a high LDL-C level was the main component that was related to developing hypothyroidism in our study. In previous studies for other autoimmune diseases, the most frequent abnormal lipid component was a high LDL-C level, 26 and statins, which mainly lower the LDL-C level, may lead to improvement of disease. 27
In the gender-specific analysis, only women participants demonstrated a significant temporal association between dyslipidemia and hypothyroidism. In the current study, women with dyslipidemia had almost twice the crude incidence rate (35.7% vs. 19.0%) of hypothyroidism than those without dyslipidemia. In contrast, men demonstrated similar crude incidence rates for hypothyroidism (25.9% vs. 25.7%) regardless of the presence or absence of dyslipidemia. This gender disparity can be explained by the effects of estrogen on the thyroid hormone and lipid metabolism.
A previous experimental study 28 that showed estrogen-mediated LDL elevation, and reviewed the postmenopausal effect on thyroid function, 29 supports the explanation. When we performed a subgroup analysis for women participants older than the average age of menopause (49.9 years) in Korean women, 30 the association between baseline dyslipidemia and hypothyroidism occurrence disappeared (adjusted HR = 1.84 [0.83–4.04]; p = 0.129) (Supplementary Table S4).
However, these observations require validation in a larger population as this subgroup analysis had a small number of participants (N = 156). When considering potential gender-specific effects, an in vitro study on SLE demonstrated that estrogen receptor-α deficiency attenuated the autoimmune response in lupus-prone mice, 31 which suggests that estrogen plays a key role in autoimmune activation. 32,33
Considering that autoimmunity is a possible important link between dyslipidemia and hypothyroidism, the role of estrogen in autoimmunity is a potential explanation for gender disparity in the current study.
In the subgroup analysis of this study, the impact of dyslipidemia as a risk factor for hypothyroidism was more considerable (almost 1.5 times higher) for young women aged <40 years than for those aged ≥40 years. Previous studies reported that the effect of TSH on TT3 production was blunted with reduced deiodinase activity in patients older than 40 years. 21,34 This age disparity also has been reported for other metabolic diseases, 35 suggesting that the relationship between thyroid hormone function and dyslipidemia may also vary by age.
A BMI disparity was also evident. In obese women (BMI ≥25 kg/m2) with dyslipidemia, a strong association between dyslipidemia and hypothyroidism risk (adjusted HR = 2.82) was observed. However, this association successively decreased as BMI decreased. A previous study reported reduced fT3 receptors of fat cells in obese individuals, 36 indicating that thyroid hormone function may have a BMI disparity for some diseases.
Additionally, an in vitro study in rats demonstrated that a high-fat diet led to fat accumulation in thyroid tissue, causing hypothyroidism. 37 Overactive fat tissue promotes inflammation and produces an additive effect on disrupting the immune system. 38,39 It is important to determine whether BMI modification is effective in lowering the TSH level in women with dyslipidemia in future larger studies.
The current study has several strengths. First, to our knowledge, this is the first study demonstrating that dyslipidemia is also a risk factor for hypothyroidism. Second, the longitudinal design with a relatively long-term follow-up and sensitivity analysis supports the robustness of our study.
Third, the results provided important and new clinical insights for two common diseases. The current study implies that not only an initial investigation of hypothyroidism but also constant attention to incident hypothyroidism is needed during treatment of dyslipidemia. Notably, the association between dyslipidemia and hypothyroidism was sustained even after excluding mild SCH as a component of the outcome.
In contrast to mild SCH, severe SCH or OH is a clinically important indication for levothyroxine replacement to reduce the risk of cardiovascular mortality. 7 Considering that the purpose of treating dyslipidemia is to reduce the risk of cardiovascular outcomes, correction of incident severe SCH or OH can provide additional benefits to that provided by statins. In contrast to dyslipidemia, for patients with type 1 diabetes, regular thyroid hormone monitoring (1–2 times per year) is recommended in guidelines, 40 and recent data demonstrate that thyroid disease has an incidence rate of ∼1032 per 100,000 persons per year. 41
In the current study, similarly, the calculated incidence rate of severe SCH or OH was 1214.3 per 100,000 persons per year for women with dyslipidemia. Even though we could not recommend an unconditional regular thyroid function test, considering the low incidence of severe SCH or OH, clinicians should pay attention to incident hypothyroidism in women with dyslipidemia.
The current study has some limitations. First, thyroid autoantibody data were not investigated. Therefore, we should keep in mind that dyslipidemia could not predict hypothyroidism independent of autoimmunity in this study. A future study with TPO Ab data is warranted to determine whether the temporal association between dyslipidemia and hypothyroidism is dependent on autoimmunity.
Second, this was a retrospective study involving participants of one specific ethnicity from a specific region (an iodine-sufficient area); the median urine iodine concentration level in Gyeongsangnam-do, where the GNUH Health Care Center is located, is higher (307.2 μg/L) than in the general Korean population (293.9 μg/L). 42 In addition, even though we used the manufacturer's reference range in the current study, Koreans have a higher reference range of TSH (0.62–6.68 mU/L) according to the Korea National Health and Nutrition Examination Survey data. 43 Hence, an external validation of our findings in other study populations is needed.
Third, although the participants who recorded hypothyroidism repeated the thyroid function test within 2 weeks and a lower TSH level was recorded, there is a possibility that mild SCH cases were only transient. Spontaneous normalization of the TSH level in patients with mild SCH is a well-known phenomenon. 44,45 In the current study, of the participants who presented with mild hypothyroidism at any point before the last follow-up, a considerable proportion (126/283, 44.5%) showed spontaneous normalization of TSH levels during follow-up.
Fourth, in this study population, unfortunately, the use of statin treatment during follow-up was not investigated. Whether using statins is associated with lowering the risk of hypothyroidism in dyslipidemia patients would be an interesting topic for future studies.
Last, we could not adjust the socioeconomic or smoking status in this study because of the limitation of crude data.
Conclusions
We found that dyslipidemia was associated with incident hypothyroidism in South Korean women. Our findings should be confirmed in other large prospective studies.
Footnotes
Acknowledgments
The authors acknowledge the support from the National Research Foundation of Korea and Development Fund Foundation, Gyeongsang National University.
Authors' Contributions
H.I.K. was involved in conceptualization (lead); formal analysis (supporting); writing—original draft (lead); investigation (supporting); and writing—review and editing (equal). T.H.K. was involved in conceptualization (supporting); formal analysis (lead); investigation (lead); and writing—review and editing (equal). H.K. and S.W.K. were involved in writing—review and editing (equal). J.R.H. was involved in conceptualization (supporting); data curation (lead); supervision (supporting); and writing—review and editing (equal). J.H.C. was involved in conceptualization (supporting); supervision (lead); and writing—review and editing (equal).
Author Disclosure Statement
The authors do not have any conflicts of interest to disclose.
Funding Information
This study was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science, ICT and Future Planning (NRF-2015R1A5A2008833) and by the Development Fund Foundation, Gyeongsang National University (May 2015).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4