
Abstract
Background:
Infection with SARS-CoV-2 has initially been known as a respiratory disease but in the course of the pandemic the understanding has emerged that severity is owing to fatal inflammatory responses apart from lung injury. In this context, endocrine disorders such as thyroiditis as well as pituitary dysfunction in addition to nonthyroidal illness syndrome have been described. Furthermore, angiotensin-converting enzyme 2 (ACE2), the SARS-CoV-2 cell receptor, has been detected in most endocrine tissues, including the thyroid gland.
Objective:
To evaluate histopathologic changes and compare thyroidal ACE2 protein expression in thyroid tissue from patients who died from severe COVID-19 with thyroid tissue from patients without SARS-CoV-2 infection in a retrospective case series. Furthermore, to assess and compare alterations in thyroid function tests (TFTs) between patients with or without SARS-CoV-2 infection as well as association of TFTs with the severity of the disease in a prospective cohort study.
Methods:
Thyroid tissue of deceased COVID-19 patients (n = 23) was analyzed for histopathology and ACE2 expression by immunohistochemical staining. A total of 153 patients with confirmed SARS-CoV-2 were evaluated regarding TFTs and divided into a severe (intubation, intensive care treatment) and an intermediate group.
Results:
Thyroidal ACE2 expression was detected in 87% of the deceased COVID-19 patients. Normal thyroid tissue from patients without SARS-CoV-2 infection showed no ACE2 protein expression. Half of the severely ill COVID-19 patients had low free triiodothyronine (fT3) levels. Combination of low fT3 and thyrotropin (TSH) was associated significantly with deadly disease.
Conclusion:
The high percentage of positive ACE2 immunostaining in deceased patients compared with normal thyroid tissue of patients without SARS-CoV-2 infection suggests involvement of the thyroid in COVID-19, although further research will have to show the pathogenic role of thyroidal ACE2 in COVID-19. Abnormal fT3 and a TSH of ≤0.5 mU/L were associated with a fatal outcome in our severely ill SARS-CoV-2 patient cohort. Therefore, assessment of TFTs is crucial in the treatment of severely ill COVID-19 patients.
Trial Registration:
COVID-19 Registry of the LMU University Hospital Munich (CORKUM), WHO trial ID DRKS00021225.
Introduction
Preliminary data of COVID-19 patients point to alterations in thyroid function tests (TFTs) with a low or suppressed serum thyrotropin (TSH), with and without elevations in free thyroxine (fT4) concentrations. 1 Data from the last SARS epidemic in 2002 have already suggested significant effects on the thyroid gland. Wei et al examined tissue samples from five SARS autopsies and reported severely damaged follicular epithelium with distortion, dilatation, and collapse of the follicular structure, suggesting destructive thyroiditis. 2 In another study, significantly decreased levels of triiodothyronine (T3) and thyroxine (T4) were reported in SARS patients; during the acute phase 94% and 46% of 48 patients showed decreased serum T3 and T4, respectively, compared with 90% and 38% during the convalescent phase. 3 In addition, TSH levels were significantly decreased. These changes in thyroid hormone could be indicative of nonthyroidal illness syndrome (NTI).
However, they could also be caused by severe hypothalamus–pituitary dysfunction based on SARS-induced hypophysitis. Among SARS survivors, Leow et al found hypothyroidism in 4 of 61 patients, including central hypothyroidism in 3 cases. 4 The possible pathogenesis is a SARS-induced hypophysitis or direct affection of the hypothalamus causing central hypothyroidism and hypocortisolism. 4 The presence of edema and neuronal degeneration as well as the detection of viral genome sequences in the hypothalamus and the cortex support the potential effect on the hypothalamus. 5 However, data by Wei et al indicate, that, besides dysfunction of the hypothalamic–pituitary–thyroid axis, SARS-induced injury to the thyroid gland may play a central role as cause of hypothyroidism. 2 It has not been resolved, how SARS induces organ injury to the thyroid gland. The suspected mechanism is host immune overreaction, as seen in subacute thyroiditis de Quervain.
In the current SARS-CoV-2 pandemic, there is increasing evidence for thyroid manifestations, as indicated by various published cases of thyroiditis. 6 –10 Autopsies of suspected SARS patients showed SARS genomic sequence–positive lymphocytes and monocytes in the vessels of the thyroid gland. 5 Furthermore, gene expression of angiotensin-converting enzyme 2 (ACE2), the SARS-CoV-2 cell receptor, has been detected in most endocrine tissues, including the thyroid gland. 11 The ACE2 gene maps on chromosome Xp22.2 leading to x-inactivation in females to balance gene expression between sexes. Nevertheless, some genes may escape the gene inactivation, which may lead to sex-based differences in ACE2 expression. 12
Taken together, available data suggest that COVID-19 can be associated with severe thyroid dysfunction other than NTI owing to thyroiditis or secondary owing to hypothalamic–pituitary dysfunction.
The study addressed two primary questions:
In a retrospective case series, we aimed to investigate thyroidal histopathology and ACE2 protein expression in patients who died from severe course of COVID-19 and compare it with thyroid tissue derived from non-COVID-19 thyroid patients as well as normal thyroid tissue at a tertiary care center in Germany. In a prospective cohort study, we analyzed patient characteristics, prevalence of alterations in TFTs, and outcome in relation to the presence or absence of COVID-19.
Methods—Patients
Setting
Retrospective case series
Patients who died from severe course of COVID-19 at the Ludwig-Maximilians-University (LMU) Hospital Munich, Germany were included in this retrospective case series. Two patients were also part of the COVID-19 Registry of the LMU Hospital. In this part, we report on thyroid findings at autopsy in patients with severe COVID-19 and analyzed thyroid ACE2 protein expression. Thyroid tissue derived from otherwise healthy patients (n = 111) with Graves' disease, thyroid follicular nodular disease, or papillary thyroid cancer (PTC) as well as normal thyroid tissue from 23 patients with PTC was used as a control.
Prospective cohort study
Patients with confirmed COVID-19 were included in this prospective cohort study. This study was conducted as part of the COVID-19 Registry of the LMU Hospital Munich, Germany (CORKUM, WHO trial ID DRKS00021225). Of 177 patients, 153 were diagnosed with SARS-CoV-2 using reverse transcriptase–polymerase chain reaction (RT-PCR) of nasopharyngeal swab specimens in the accredited diagnostic laboratories at the Pettenkofer-Institute, Munich, as previously described. 13 The control group consisted of patients who presented to the emergency department and were initially suspected to have COVID-19 but had a negative RT-PCR. Patients gave written informed consent for participation and analysis of their data. The study was approved by the local ethics committee (no: 20-245) and complies with the Declaration of Helsinki.
Data acquisition: retrospective case series
The selection of patients is given in Figure 1.
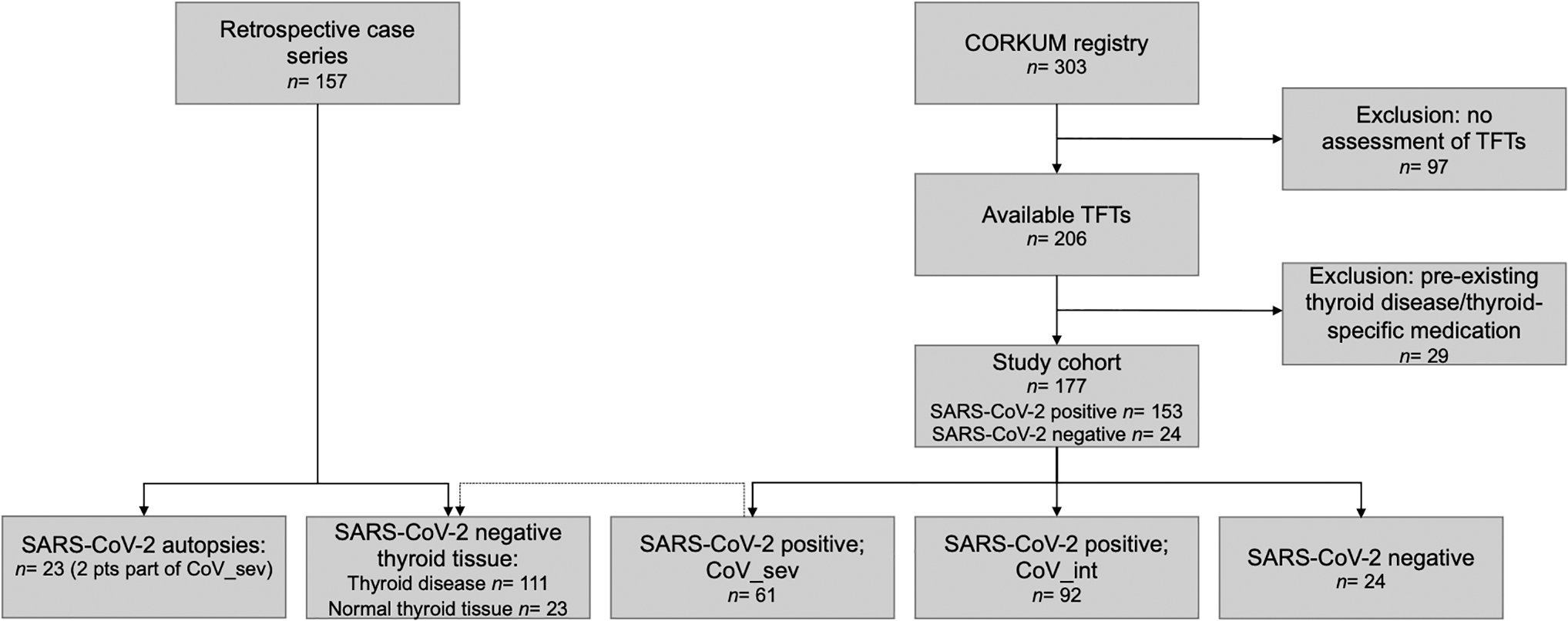
Selection of patients. SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TFTs, thyroid function tests.
Histomorphology
In postmortem specimens, thyroid tissue was obtained and formalin-fixed after autopsy. Owing to minimization of the time between death and autopsy, no relevant autolytic changes were detected. The immunohistochemical staining was performed on formalin-fixed, paraffin-embedded tissue without autolytic changes. Hematoxylin and eosin staining was performed to investigate the histopathological changes of thyroid tissue derived from patients who died from severe course of COVID-19 (n = 23). Histomorphology was evaluated according to histopathological observations of the thyroid in SARS published by Wei et al: destruction of the follicular epithelium and exfoliation of epithelial cells into the follicle, changes in follicle size (microfollicle configuration, dilated, distorted, and/or collapsed follicles), capillary congestion in the connective tissue, and interfollicular fibrosis. 2
Immunohistochemistry
In addition, we analyzed ACE2 protein expression by immunostaining in thyroid tissue derived from patients who died from severe course of COVID-19 (n = 23) compared with thyroid tissue derived from otherwise healthy patients (n = 111) with Graves' disease, de Quervain's thyroiditis, thyroid follicular nodular disease, or PTC. Normal thyroid tissue from 23 patients with PTC was used as a control. Detailed methods including ACE2 immunohistochemistry are described in the Supplementary Methods.
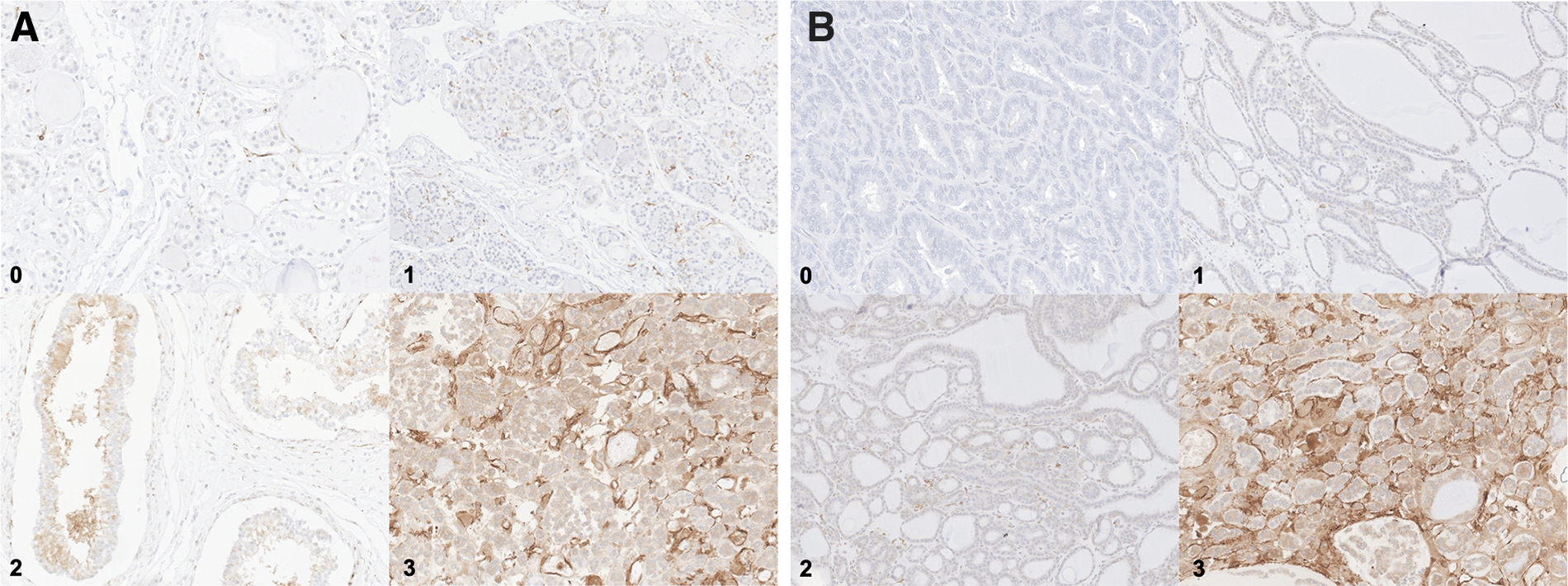
The number of ACE2-positive cells was quantified by a reproducible tissue score: 0 = negative, 1 = low expression, 2 = moderate expression, 3 = strong expression. The tissue score was evaluated by two researchers (V.F.K., T.K.), independently. In case of discrepancies in the scoring results of the investigators, consent was built after individual re-evaluation of each sample at the multiheaded microscope. All researchers were blinded to the clinical data. Staining examples for the used reproducible tissue score from postmortem thyroid material as well as from in vivo cases (PTC) are given in Figure 2A and B.
(
Data acquisition: prospective cohort study
The selection of patients is given in Figure 1. In the time period of February 28, 2020 until July 28, 2020, 303 subjects were included in the CORKUM registry. Ninety-seven subjects without assessment of TFTs were excluded. A total of 177 subjects were included in our study (n = 153 with COVID-19 and n = 24 non-COVID-19 as a control group). Twenty-nine patients with a preexisting thyroid disease or thyroid-specific medication (levothyroxine, carbimazole) were excluded. COVID-19 patients were divided into two groups: CoV_sev (n = 61), severe cases requiring intubation and intensive care treatment, and CoV_int (n = 92), intermediate cases, which were hospitalized and either required no oxygen or received noninvasive supplemental oxygen.
Our primary predictor of interest was the presence of TFT alterations. Clinical data were recorded by trained personnel in the designated COVID-19 database. TFTs were performed at the time of admission and during hospitalization according to the physician's discretion. Euthyroidism was defined as TSH, free triiodothyronine (fT3), and fT4 within the reference range of 0.27–4.2 mU/L, 2–4.4 pg/mL, and 0.9–1.7 ng/dL, respectively, subclinical hypothyroidism by elevated TSH with normal fT4/fT3, hypothyroidism by elevated TSH with decreased fT4/fT3, subclinical hyperthyroidism by reduced TSH with normal fT4/fT3, and hyperthyroidism by reduced TSH and elevated fT4/fT3. Central hypothyroidism and NTI reveal values of TFTs that largely overlap, 14 therefore these entities were combined and defined as low fT3 and normal or moderately decreased fT4 with low/normal TSH.
Statistical analysis
We performed complete case analyses with casewise deletion of observations with missing data. Since the study was planned as an exploratory study, no formal sample size calculation was performed.
Statistical analyses were performed with SPSS version 25 (IBM, Chicago, IL). GraphPad Prism 9.0 (GraphPad Software, San Diego, CA) and Microsoft Office Excel Version 16.55 were used for graphical presentation and additional analyses. For categorical variables, we calculated relative and absolute frequencies; for numeric variables, we calculated medians and interquartile ranges (IQR). For direct comparisons between two groups, unpaired, nonparametric Mann–Whitney U-test was used for numerical variables, and chi-squared tests for the categorical variables. The Kruskal–Wallis test was used for comparison of numerical variables among more than two groups. Values of p < 0.05 were considered statistically significant.
Results
Histomorphology: retrospective case series
Table 1 provides baseline clinical characteristics of patients who died from COVID-19 with available thyroid tissue. Tissue samples obtained from autopsies were available in all cases and revealed thyroid follicular nodular disease (14/23; 61%), C cell hyperplasia (1/23; 4%), and chronic lymphocytic thyroiditis (1/23; 4%). Features suggestive for thyroiditis were detected in 20 of 23 (87%) cases.
Patient Characteristics of the Retrospective Case Series with Angiotensin-Converting Enzyme 2 Protein Expression and SARS-CoV-2 Infection
COPD, chronic obstructive pulmonary disease; fT3, free triiodothyronine; fT4, free thyroxine; ICU, intensive care unit; IQR, interquartile range; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TFTs, thyroid function tests; TSH, thyrotropin.
Thyroidal ACE2 protein expression: retrospective case series
In patients without SARS-CoV-2 infection, thyroid surgery was performed because of Graves' disease, thyroid follicular nodular disease, or PTC. Median ACE2 protein expression in non-COVID-19 patients is given in Table 2. Table 3 compares the thyroidal ACE2 protein expression in patients with and without COVID-19. Figure 3 provides high ACE2 protein expression from a patient with severe COVID-19. ACE2 protein expression was detected in almost all tissue samples from COVID-19 patients (20/23, 87%, exact 95% confidence interval [CI] 66%–97%), and in 82/112 (73%, CI 64%–81%) of tissue samples from non-COVID-19 thyroid patients (p = 0.16). Evaluation of normal thyroid tissue from 23 non-COVID-19 patients with PTC showed no ACE2 protein expression. Endothelial cells within the thyroid gland were negative for ACE2 in these cases.
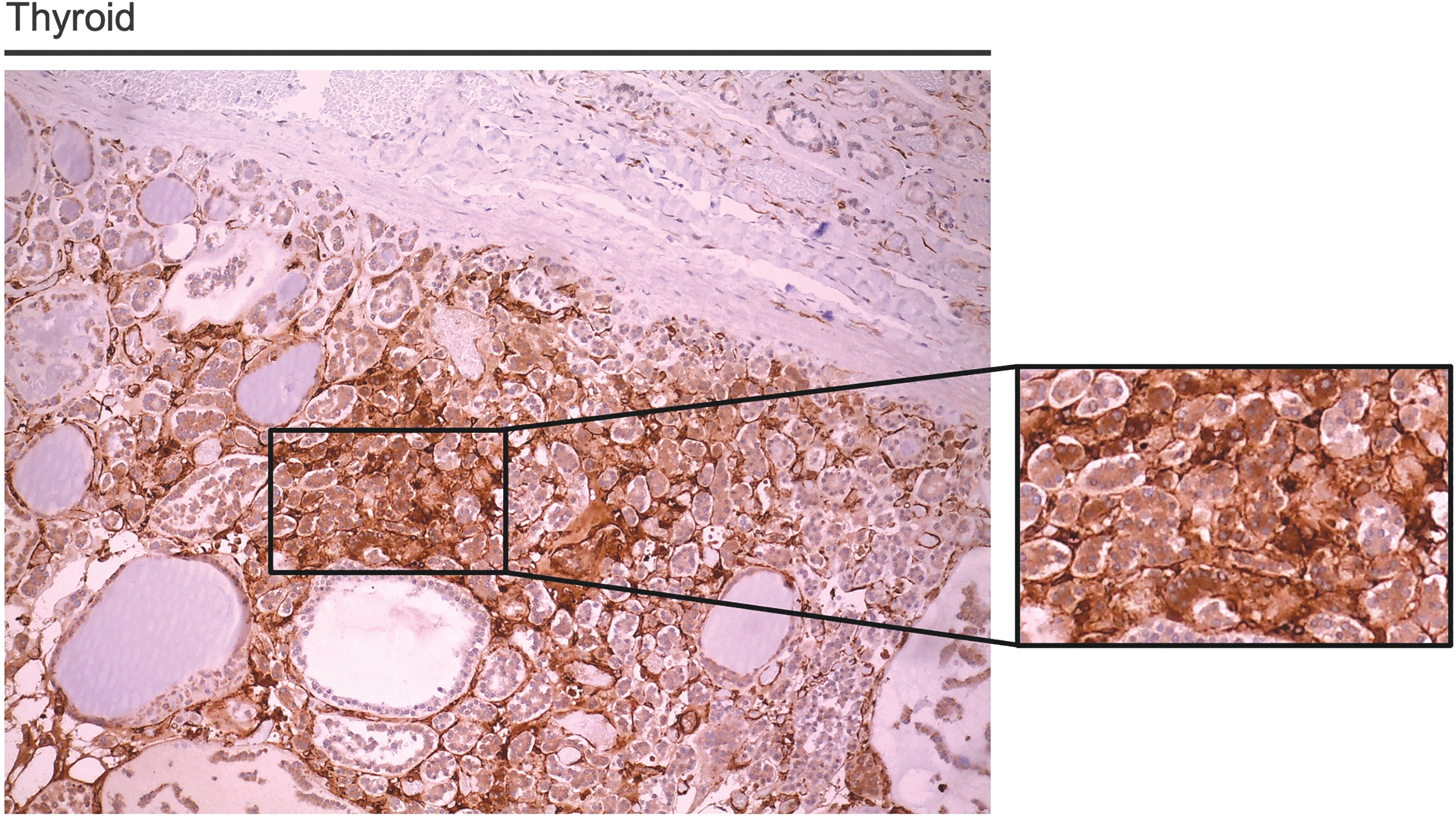
High ACE2 protein expression in thyroid tissue from a patient with severe COVID-19. ACE2-specific immunoreactivity was detected in thyroid follicular cells. The image is shown at 20 × magnification, the high-power insert is shown at 40 × magnification. ACE2, angiotensin-converting enzyme 2.
Angiotensin-Converting Enzyme 2 Expression of Non-SARS-CoV-2–Infected Patients (N = 133)
ACE, angiotensin-converting enzyme; IQR, interquartile range; NA, not applicable.
Angiotensin-Converting Enzyme 2 Expression of the Retrospective Case Series
Without normal thyroid tissue.
Considering patients with positive ACE2 protein expression, the median score for ACE2 expression was 2 (IQR 1–3) in the non-COVID-19 group and 1 (IQR 1–1) in the COVID-19 group (p = 0.003). We did not detect sex-based differences in the COVID-19 group (p = 0.18) and the non-COVID-19 group (p = 0.57). Data on ACE2 in the non-COVID-19 and the COVID-19 group are given in Figure 4. ACE2 protein expression was significantly higher in PTC and Graves' disease compared with tissue from SARS-CoV-2 patients (p < 0.001, p = 0.009). Owing to limited patient number, one patient with de Quervain's thyroiditis was excluded.
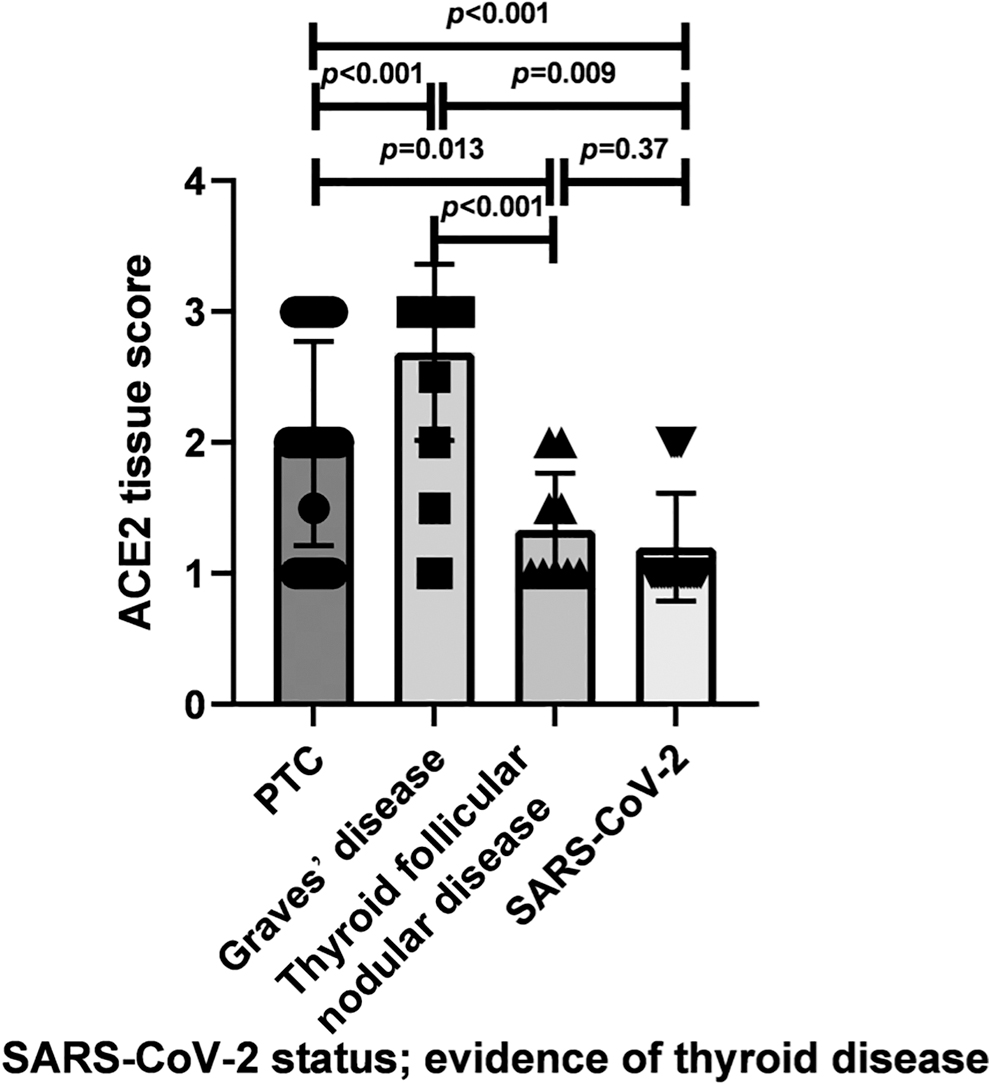
Comparison of ACE2 protein expression in PTC, Graves' disease, thyroid follicular nodular disease, and SARS-CoV-2. ACE2 protein expression assessed by a reproducible tissue score was significantly higher in PTC and Graves' disease compared with SARS-CoV-2 thyroid tissue. No significant differences could be observed between thyroid follicular nodular disease and SARS-CoV-2 thyroid tissue. PTC, papillary thyroid cancer.
Clinical characteristics: prospective cohort study
A total of 153 patients with laboratory-confirmed COVID-19 and 24 non-COVID-19 patients were included. Table 4 provides baseline clinical characteristics of COVID-19 patients and the control group. Five (21%) patients in the control group, 0 patients in the CoV_int group, and 25 (41%) patients in the CoV_sev group received steroid treatment.
Patient Characteristics of the Prospective Cohort Study
CoV_int, group of intermediate severity; CoV_sev, group of severe cases requiring intubation and intensive care treatment.
Laboratory characteristics: prospective cohort study
Laboratory characteristics of the study population are given in Table 5. Median serum TSH was lowest in the CoV_sev group (1.1 mU/L; IQR, 0.5–1.7; range, <0.01–6), compared with 1.4 mU/L (IQR, 0.9–2.1; range, 0.1–11.2) in the CoV_int group, and 1.4 mU/L (IQR, 1–2.4; range, 0.3–10.5) in the control group (p = 0.041). The CoV_sev group had significantly lower fT3 and fT4 than the CoV_int and control group (p < 0.001, p = 0.011). Laboratory characteristics of SARS-CoV-2 nondeaths versus SARS-CoV-2 deaths and CoV_sev nondeaths versus CoV_sev deaths are compared in Supplementary Tables S1 and S2, respectively. Supplementary Table S3 provides defined laboratory abnormalities of SARS-CoV-2–infected patients.
Laboratory Characteristics of the Prospective Cohort Study
One (1%) patient in the CoV_int group had biochemical features of manifest hyperthyroidism, 1 (1%) had biochemical features of subclinical hyperthyroidism, 1 (1%) of subclinical hypothyroidism, 2 (2%) of manifest hypothyroidism, and 5 (5%) of NTI. In the CoV_sev group, 1 (2%) patient had biochemical features of manifest hyperthyroidism, 2 (3%) of subclinical hyperthyroidism, no patient of subclinical hypothyroidism, 2 (3%) of manifest hypothyroidism, and 35 (57%) of NTI. Half the patients (30, 49%) in the CoV_sev group presented with low fT3 levels <2.0 pg/mL, from whom 8 (27%) had a mildly suppressed TSH between 0.1 and 0.5 mU/L and 3 (10%) had a suppressed TSH <0.1 mU/L. Patients in the CoV_sev group had NTI significantly more often compared with the CoV_int group (35/61 vs. 6/92, p < 0.001). In the CoV_sev group, an abnormal fT3 level <2.0 pg/mL and a TSH of <0.01–0.5 mU/L was significantly associated with death compared with patients with a low fT3 level and a TSH within the reference interval (death 6/11 vs. 2/19, p = 0.009).
Discussion
Several studies highlight a potential mechanism of SARS-CoV-2 infection on hypothalamic–pituitary–thyroid axis. Possible mechanisms are direct virus infection or direct effects via immune cells and indirect effects through abnormal systemic inflammatory-immune responses. 15 COVID-19–related thyroid disorders reported in the current literature are thyrotoxicosis owing to subacute thyroiditis, 6,10 atypical thyroiditis, 1 Graves' disease, 16 hypothyroidism because of central hypothyroidism, 17 primary hypothyroidism 1,18 as well as NTI. 1,17 Since the beginning of the pandemic, data on the relationship of COVID-19 and the thyroid gland have been rapidly increasing. In our prospective study, we compared TFTs in COVID-19 patients requiring intubation and intensive care treatment (CoV_sev) with a group of intermediate severity (CoV_int) and a control group.
To provide further evidence on whether the thyroid gland might be a direct target organ of SARS-CoV-2, we compared ACE2 protein expression in thyroid tissue derived from patients who died from severe course with thyroid tissue from non-COVID-19 patients. ACE2 combined with the transmembrane protease serine 2 (TMPRSS2) is the key molecular complex for the SARS-CoV-2 virus to enter and infect host cells, 19,20 and it has been reported earlier that ACE2 and TMPRSS2 expression is high in thyroid tissue. 11,21
Histomorphology analysis of thyroid tissue from patients who had died from severe SARS-CoV-2 infection in our study showed changes, consistent with data reported by Wei et al. 2 Nevertheless, thyroid follicular nodular disease, present in 61% of the autopsies, and postmortem autolysis could also cause part of these alterations.
Yet it has not been resolved as to how SARS-CoV-2 induces organ injury to the thyroid gland and if it is a direct target organ. It is known that the SARS-CoV-2 infection depends on the presence of the host cell receptor. 19 To our knowledge, this is the first comprehensive study on ACE2 protein expression by immunostaining in COVID-19–related thyroid tissue. ACE2 protein expression was detected in almost all COVID-19 samples, and to a lesser extent in non-COVID-19 thyroidal tissue samples from patients with thyroid disease. Nevertheless, the median tissue score for ACE2 expression was significantly higher in the non-COVID-19 group than in the COVID-19 group. The direct comparison between in vivo and postmortem thyroid tissue has limitations owing to delayed fixation of postmortem tissue and possible effects of postmortem changes (such as tissue hypoxia or necrosis) on the regulation of various gene products in the thyroid gland.
Supporting our results, a very recent analysis by Poma et al detected SARS-CoV-2 genome and antigens in 9 of 25 thyroid specimens of subjects dying from COVID-19, showing that the thyroid gland can be directly infected by the SARS-CoV-2. 22 Tanda et al furthermore recently detected SARS-CoV-2 by RT-PCR in a seronegative patient with thyroid sarcoma. 23 Li et al analyzed ACE2 gene expression in tissues derived from genotype-tissue expression biobank. 11 Among the 31 human tissues studied, the thyroid gland showed one of the highest ACE2 expression levels. Nevertheless, these findings were generated by in silico prediction analysis and the mRNA expression pattern of ACE2 does not necessarily correlate with its protein expression pattern, which is presented in our analysis. Data from Rotondi et al demonstrated that the ACE2 mRNA is expressed in thyroid follicular cells in thyroid surgical specimens and in primary cultures of thyroid cells. 24 However, these findings also do not confirm that ACE2 protein is present in thyroid cells. Noteworthy, in our cohort normal thyroid tissue did not reveal ACE2 expression.
In addition, non-COVID-19 PTC patients revealed a significantly increased ACE2 protein expression compared with thyroid follicular nodular disease. To explore the role of ACE and ACE2 in thyroid carcinogenesis, Narayan et al analyzed 61 thyroid tissues. 25 ACE2 was significantly increased in PTC in comparison with thyroid follicular nodular disease, follicular adenoma, undifferentiated thyroid cancer, and in follicular thyroid cancer as compared with thyroid follicular nodular disease. 25 Although the exact functional or biological role of ACE and ACE2 in thyroid cancer remains unclear, currently available data deserve further investigation. 25
Limitations of the retrospective case series include the lack of comparison with postmortem tissue from patients with thyroid disease, the relatively small size of the study with a small number of cases and differences in clinical characteristics between cases and controls.
Laboratory characteristics of the study cohort showed a significant difference between median TSH, fT4, and fT3 levels, with the lowest levels in the most severely ill patients (CoV_sev). Furthermore, abnormal TFTs, defined as values above/below the reference range, were more frequent in the CoV_sev group with the major difference between abnormal fT3 levels. This finding is also evident comparing patients who died from COVID-19 with patients still alive as well as comparing CoV_sev patients who died in the intensive care unit (ICU) with patients discharged alive. Our data suggest that a substantial proportion of COVID-19 patients, requiring ICU treatment, present with abnormal TFTs. These hormonal changes are most likely the result of NTI. A decrease in TSH could also be induced or reinforced by corticosteroid therapy, which was performed in 41% of severely ill patients (CoV_sev). Furthermore, secondary hypothyroidism because of hypothalamic–pituitary dysfunction cannot be excluded in our cohort.
Recent data have already shown that a high proportion of COVID-19 patients showed alterations in TFTs. 1,17,18 Muller et al described thyrotoxicosis and low serum TSH concentrations as a consequence of a combination of subacute thyroiditis induced by SARS-CoV-2 and NTI. 1 Lania et al interpreted the remarkable number of hospitalized patients with suppressed TSH as very likely an expression of thyrotoxicosis rather than NTI, particularly because none had low fT3 levels. 18 This is one major difference to our cohort, where we found a median fT3 level below the reference range particularly in the CoV_sev group, while median TSH remained within the reference range.
Furthermore, only 1% of COVID-19 patients showed biochemical features of manifest hyperthyroidism and 2% showed biochemical features of subclinical hyperthyroidism. A Chinese cohort with 50 COVID-19 patients showed significantly lower TSH levels in the severe group compared with non-COVID-19 pneumonia patients. 17 The authors suspected a unique effect of COVID-19 on TSH-secreting cells by a direct viral effect on the pituitary cells or an indirect effect wherein systemic changes (e.g., proinflammatory cytokines) led to hormonal changes in the pituitary–endocrine axis feedback loops. 17
In addition to these findings, we detected that abnormal fT3 and TSH <0.01–0.5 mU/L was more likely associated with fatal outcome in CoV_sev patients. Furthermore, we detected significantly more often biochemical features of NTI in COVID-19 patients compared with the control group as well as in patients of the CoV_sev group compared with the CoV_int group. This could simply demonstrate NTI being associated with the severity of the disease. However, one could also hypothesize that low TSH and fT3 may be related to central “pituitary” dysregulation possibly corresponding to a central nervous system affection and therefore prognostic for lethal outcome. Owing to lack of systematic screening of further hormones of pituitary axis, precise differentiation of central hypothyroidism versus NTI is not possible.
Our prospective cohort study is limited by small sample size of the control group and heterogeneity between the different subgroups.
Conclusion
The results of this study emphasize that a high proportion of COVID-19 patients have TFT alterations, mostly indicative of NTI. We argue for a routine assessment of TFTs at least in COVID-19 patients requiring ICU treatment. Differentiation between NTI and pituitary dysfunction is difficult in the ICU setting, but has to be considered in the individual patient requiring complete pituitary function test and thyroid supplementation.
In addition, we present the first comparative analysis of ACE2 protein expression in thyroid tissue from SARS-CoV-2 patients as well as non-COVID-19 thyroid patients, demonstrating that ACE2 protein is widely expressed in SARS-CoV-2 patients and to a lesser extent in thyroid pathologies from non-COVID patients with the highest expression levels in PTC, while normal thyroid tissue showed no ACE2 protein expression. More research is needed to evaluate the role of ACE2 protein expression in thyroid disease, and particularly in thyroid cancer.
Footnotes
Acknowledgements
The authors thank all CORKUM investigators and staff. The authors also thank the patients and their families for their participation in the CORKUM registry.
Authors' Contributions
V.F.K.: Data acquisition, analysis and interpretation, drafted the article, and designed the tables/figures. T.K.: histopathological analysis and immunohistochemical staining, critical revision and final approval of the article. S.E.H.: data acquisition, critical revision, and final approval of the article. C.S.: data acquisition, critical revision, and final approval of the article. J.C.H.: CORKUM registry platform and data, critical revision and final approval of the article. M.M.: virologic analyses, CORKUM registry platform and data, critical revision, and final approval of the article. S.M.M.: data acquisition, critical revision, and final approval of the manuscript. E.H.: methodological and statistical advice, critical revision, and final approval of the article. R.L.: critical revision and final approval of the article. C.S.: supervising physician, involved in planning, and supervised the work, critical revision, and final approval of the article. All authors discussed the results and commented on the article.
Author Disclosure Statement
V.F.K. has received honoraria for lectures and travel expenses from Novartis and Sanofi.
Funding Information
This work was supported by the “Förderprogramm für Forschung und Lehre (FöFoLe), Reg.-Nr. 1031” of the medical faculty of the LMU Munich.
Supplementary Material
Supplementary Methods
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3