
Abstract
Background:
Radioactive iodine lobar ablation (RAILA) of the contralateral thyroid lobe has been suggested as an alternative to completion thyroidectomy in patients of differentiated thyroid cancer (DTC) who underwent initial hemithyroidectomy. However, data on long-term outcomes are scarce. In this study, we intended to describe the long-term outcomes of RAILA versus completion thyroidectomy in a cohort of low-risk DTC patients.
Methods:
Data of patients with low-risk DTC who underwent initial hemithyroidectomy, and were subsequently treated with either completion thyroidectomy or RAILA between 1996 and 2015, were collected and analyzed. The treatment outcomes included ablation rate, recurrence rate, recurrence-free survival (RFS), and adverse events, and were validated by propensity score matching analysis.
Results:
Of the 1243 patients (median age: 34 years, range: 5–78) with low-risk DTC, 514 patients underwent upfront RAILA while 729 patients underwent completion thyroidectomy followed by remnant ablation. The ablation rate following the first radioactive iodine (131I) cycle was 75.3% [95% confidence interval (CI) 71.3–78.9] in the RAILA group versus 84.1% [CI 81.2–86.6] in the completion thyroidectomy group (p < 0.001). Over median follow-up of 11.4 years (interquartile range: 8.3–15.8), the recurrence rates between the two groups were not significantly different (1.6% [CI 0.7–3.2] vs. 1.0% [CI 0.4–2.1], respectively, p = 0.343). The product limit estimate of RFS at 10 years was 98.6% [CI 97.6–99.6%] in the RAILA group versus 99.1% [CI 98.3–99.9%] in the completion thyroidectomy group (p = 0.391). The outcomes in 497 matched pairs generated through propensity score analysis were similar. None of the patients in the RAILA group experienced permanent hypocalcemia or recurrent laryngeal nerve palsy, while the corresponding rates in the completion thyroidectomy group were 10/729 (1.4%) (p = 0.006) and 5/729 (0.7%) (p = 0.080), respectively. Radiation thyroiditis was seen in 25/514 (4.9%) patients in the RAILA group versus 3/729 (0.4%) in the completion thyroidectomy group (p < 0.001).
Conclusions:
Upfront RAILA is seen to be a noninvasive, safe, and effective alternative to surgical completion thyroidectomy in low-risk DTC patients in the absence of macroscopic malignancy in the remaining thyroid lobe.
Introduction
Thyroid cancer currently ranks as the ninth most commonly occurring cancer worldwide. 1 Differentiated thyroid cancers (DTCs) comprise the majority of all thyroid cancers, of which, papillary thyroid cancer (PTC) is most common. 2 Current American Thyroid Association (ATA) guidelines recommend hemithyroidectomy for many patients with low-risk DTC, a somewhat controversial recommendation. However, during the time of our study, total or near-total thyroidectomy, with or without subsequent remnant ablation by radioactive iodine (131I), was the accepted treatment of choice for most DTCs. 3–4 However, in patients with preoperative indeterminate cytological diagnosis, or small, unifocal, intrathyroidal carcinomas, hemithyroidectomy is usually preferred. 4
Ablation of the contralateral lobe with 131I has been suggested as an alternative to completion thyroidectomy in few studies. 5 –11 Being a noninvasive procedure, radioactive iodine lobar ablation (RAILA) can avoid the risks associated with a second surgery, particularly, permanent hypocalcemia, and recurrent laryngeal nerve (RLN) palsy. 12 The modality is also of potential utility for patients with comorbidities, and hence, at increased risk on resurgery. Nevertheless, despite encouraging results, large-scale acceptance of this procedure remains elusive in the absence of long-term outcomes. Furthermore, there is an uncertainty concerning the recurrence rates following RAILA in lieu of completion thyroidectomy. In this retrospective study, we, therefore, intended to describe the long-term outcomes of RAILA versus completion thyroidectomy in a cohort of low-risk DTC patients undergoing initial hemithyroidectomy. We also used propensity score matching to create matched pairs for analysis to overcome the biases associated with a retrospective study.
Materials and Methods
Patient population
This was a retrospective analysis of a prospectively maintained registry at the Thyroid Clinic, All India Institute of Medical Sciences, New Delhi, India. Data of consecutive patients of thyroid cancer treated at our center between 1996 and 2015 were collected. Of these, only patients with low-risk, histopathologically proven DTC, who underwent initial hemithyroidectomy, were considered for inclusion. Low-risk disease was defined as per the 2015 ATA guidelines. 4 These patients subsequently underwent either completion thyroidectomy followed by remnant ablation (completion thyroidectomy group), or upfront RAILA (RAILA group). Only those patients who had minimum follow-up of 5 years were included. The decision for treatment following initial hemithyroidectomy, that is, either completion thyroidectomy or RAILA, was based on physician and patient preference. Patients were sufficiently explained in their vernacular about both modalities, including the risks for adverse outcomes following second surgery, as well as the unproven nature of long-term outcomes after upfront RAILA. Informed consent was obtained from the patients before either procedure. The study was approved by the Institute Ethics Committee (IEC-459/06.05.2022).
Interventions
The interventions in either group of patients have been described previously. 6,8,9 In the RAILA group, patients initially underwent radioiodine uptake (RAIU) study, followed by pertechnetate thyroid scan to assess the remaining functional thyroid tissue. Accordingly, an empirical therapeutic activity of 131I (0.93–3.7 GBq) was orally administered.
In the completion thyroidectomy group, whole-body diagnostic 131I scan (DxWBS) was performed with 74 MBq 131I after 4–6 weeks of surgery when thyrotropin (TSH) level of ≥30 mIU/L was reached. DxWBS was acquired 24–48 hours after 131I administration on General Electric or Siemens systems with bed speed of 10 cm/minute. Patients were subsequently treated with 0.55–3.7 GBq of oral 131I for remnant ablation.
In both groups, whole-body post-therapy scans were performed after 48–72 hours, to look for any occult metastasis. The patients were then started on suppressive dose of levothyroxine (2 mcg/kg) daily. Subsequent cycles of 131I were administered at 6-month intervals depending on the extent of remnant tissue noted on the follow-up DxWBS after levothyroxine withdrawal. All the patients in both the groups achieved serum TSH level of ≥30 mIU/L upon levothyroxine withdrawal. None of the patients underwent exogenous TSH stimulation using recombinant human TSH.
Follow-up and treatment outcomes
Patients were followed up at 6 months with levothyroxine withdrawal for DxWBS, stimulated thyroglobulin, and anti-thyroglobulin values. The criteria for ablation have been described previously. 6,8,9 In brief, major criterion: negative DxWBS along with minor criteria: 24-hour RAIU ≤0.2%, stimulated thyroglobulin <10 ng/mL and negative anti-thyroglobulin. The patients were retreated with 131I if DxWBS was positive with 24-hour RAIU >0.2% or stimulated thyroglobulin >10 ng/mL or positive anti-thyroglobulin. After successful ablation, patients were followed up annually with physical examination, and thyroglobulin values (or anti-thyroglobulin values, if positive earlier). Structural imaging with ultrasonography, computed tomography (CT), or18-fluorodeoxyglucose positron emission tomography/CT, was carried out in cases of suspected recurrence (suspicious findings on palpation, and/or rising thyroglobulin or anti-thyroglobulin values). Fine-needle aspiration cytology was done wherever feasible.
The short-term outcomes assessed in the present series included ablation rate and initial adverse events (AEs). The long-term outcomes included recurrence rate, recurrence-free survival (RFS), overall survival (OS), and delayed AEs. Of these, the recurrence rate was designated as the primary endpoint, whereas the rest were secondary endpoints. Ablation rate was defined as the proportion of patients achieving successful ablation as per the abovementioned criteria. Recurrence rate was defined as the proportion of patients with documented structural recurrence at any time following successful ablation. RFS was estimated from the date of completion thyroidectomy or RAILA until documented structural recurrence. OS was estimated from the date of completion thyroidectomy or RAILA until death due to any cause. AEs were evaluated using the Common Terminology Criteria for AEs, version-5.0 (CTCAE-v5.0).
Statistical analysis
Based on the primary endpoint, the sample size of 1243 patients provided 85% power at two-sided alpha-level of 5% while assuming recurrence rates of 3.5% and 1.0% in the RAILA and completion thyroidectomy groups, respectively, and an allocation ratio of ∼1:1.5. Statistical analysis was performed using IBM SPSS-Statistics for Windows, version-20.0, and MedCalc® Statistical Software version-14.8.1. To account for the effect of covariates, namely, age, sex, and histopathological variant on the outcomes in the two groups, matching covariate analysis was done using the propensity score method. Exact matching was done for sex and histopathological variant, while for age, the maximum allowable difference was two units. Propensity score was calculated using logistic regression (treatment group as the dependent variable and the other abovementioned covariates as independent variables). Matched pairs were then generated based on the propensity score using the nearest-neighbor method, with allocation ratio of 1:1.
Categorical variables were expressed as number and percentages. Chi-square and Fisher's exact tests were used for testing significance of difference in these variables across the groups. Continuous variables were expressed as median and interquartile range (IQR, 1st quartile to 3rd quartile). Mann–Whitney U test was used for testing significance of difference in these variables between two groups. Survival analysis was done using Kaplan–Meier curve method and Cox proportional hazards model. The median duration of follow-up was estimated using reverse Kaplan–Meier curve method. Log-rank test was used to compare survival times between the groups. A two-tailed p-value <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics
A total of 1243 patients with low-risk DTC who underwent initial hemithyroidectomy were included. Of these, 729 patients underwent completion thyroidectomy followed by remnant ablation, whereas 514 patients underwent upfront RAILA (Fig. 1). The demographic and clinical characteristics of the patients were observed to be comparable between the two groups (Table 1). The median age of the patients was 34 years (range: 5–78 years), and a female preponderance (n = 983/1243, 79%) was noted. One thousand one hundred fifty-three per 1243 (93%) patients had an initial presentation of solitary thyroid nodule, whereas a postoperative histopathological diagnosis of PTC was noted in 1085/1243 (87%) patients. Patients in the RAILA group, had significantly higher baseline 24-hour RAIU values compared with those in the completion thyroidectomy group (median 13.5%, IQR: 9.5–17.4 vs. 2.7%, IQR: 1.1–7.0, p < 0.001). One hundred eighteen per 729 (16.2%) completion thyroidectomy procedures yielded positive for malignancy in the residual lobe, all of which were microcarcinomas (≤1 cm). The indications for contralateral lobe ablation are specified in Table 2.
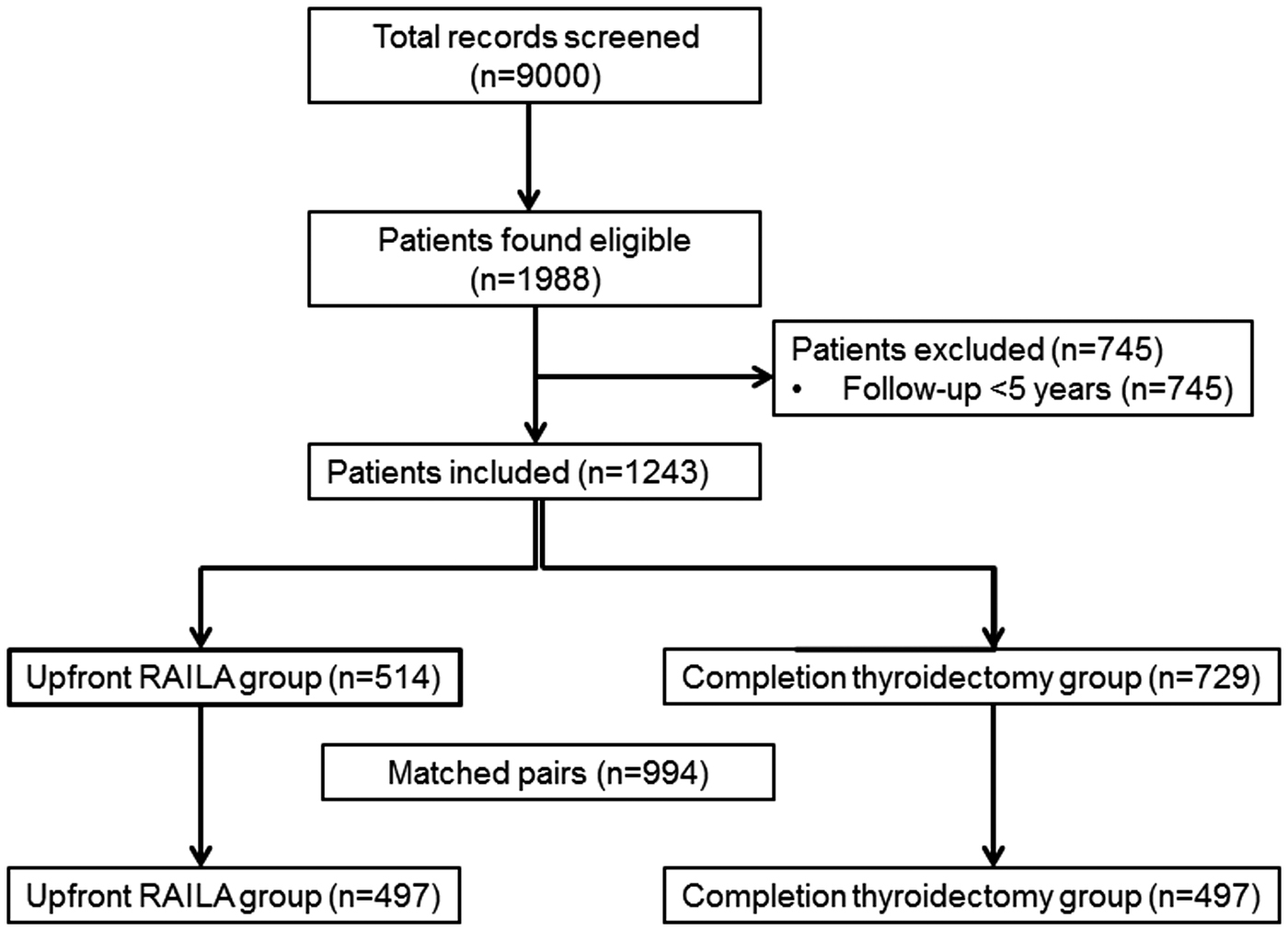
Flowchart showing the patient selection process. RAILA, radioactive iodine lobar ablation.
Baseline Characteristics of Patients in the Two Groups
Tumor–node–metastasis staging done as per the eighth edition of the American Joint Committee on Cancer.
I, radioactive iodine; FTC, follicular thyroid cancer; IQR, interquartile range; MNG, multinodular goiter; PTC, papillary thyroid cancer; RAILA, radioactive iodine lobar ablation; RAIU, RAI uptake; STN, solitary thyroid nodule.
Indication for Second Intervention Following Initial Hemithyroidectomy
Some patients had more than one feature supportive for contralateral lobe ablation.
T3, triiodothyronine.
Treatment characteristics
The median activity of the first cycle of 131I administered to the patients was 1.48 GBq in the RAILA group versus 1.11 GBq for remnant ablation in the completion thyroidectomy group (p = 0.858). Overall, 387/514 (75.3%) patients in the RAILA group required a single cycle of 131I, whereas 114/514 (22.2%) patients required two cycles, and 13/514 (2.5%) patients required ≥3 cycles for successful lobar ablation. Likewise in the completion thyroidectomy group, 613/729 (84.1%) patients required a single cycle, whereas 114/729 (15.6%) patients required two cycles, and two patients required three cycles of 131I for remnant ablation. The cumulative activities of 131I administered in the two groups were not significantly different (p = 0.082) (Table 1).
Response outcomes
The ablation rate following the first cycle of 131I was 75.3% [95% confidence interval (CI) 71.3–78.9] in the upfront RAILA group compared with 84.1% [CI 81.2–86.6] in the completion thyroidectomy group (p < 0.001). Also after two cycles of 131I, a slightly higher ablation rate was noted in the completion thyroidectomy group compared with the upfront RAILA group (99.7% [CI 98.9–99.9] vs. 97.5% [CI 95.6–98.6], p < 0.001).
The patients were followed up for a median duration of 137 months (IQR = 100–190 months). The median follow-up in the upfront RAILA and completion thyroidectomy groups was 144 months (IQR = 107–190 months), and 129 months (IQR = 94–189 months), respectively. In the course of this follow-up, 8/514 (1.6%) patients in the RAILA group developed structural recurrence, which was not significantly different from the recurrence rate noted in the completion thyroidectomy group (1.6% [CI 0.7–3.2] vs. 1.0% [CI 0.4–2.1], respectively, p = 0.343). Most of the recurrences were localized to the cervical lymph nodes (Table 3).
Treatment Outcomes in the Two Groups
CI, confidence interval; NR, not reached; RFS, recurrence-free survival.
The 10-year RFS rate was 98.6% [CI 97.6–99.6] in the upfront RAILA group versus 99.1% [CI 98.3–99.9] in the completion thyroidectomy group (hazard ratio, 1.56 [CI 0.56–4.37], p = 0.391) (Fig. 2). One death was observed in the completion thyroidectomy group owing to progressive pulmonary metastatic disease, and the median OS was not reached in either group (p = 0.397).
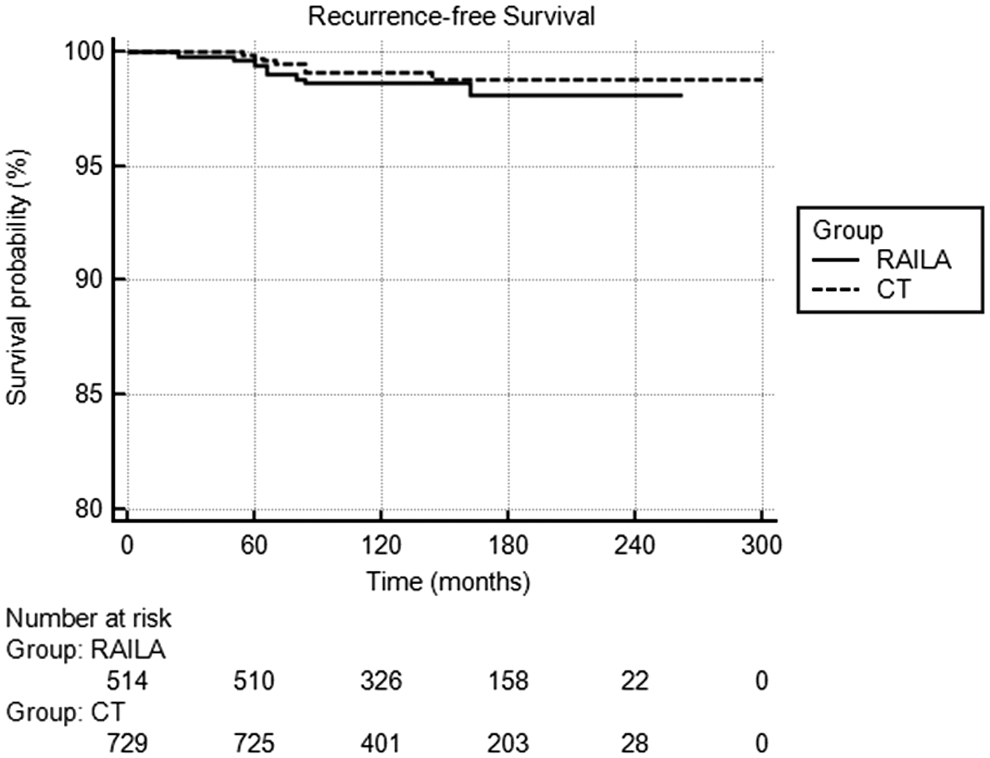
Kaplan–Meier curves showing the recurrence-free survival in the two groups. CT, completion thyroidectomy group.
Adverse events
Patients in the completion thyroidectomy group had higher rates of grade 1/2 hypocalcemia (178/729, 24.4% vs. 22/514, 4.3%, respectively, p < 0.001) and RLN palsy (31/729, 4.3% vs. 13/514, 2.5%, respectively, p = 0.090) compared with the upfront RAILA group. Furthermore, the incidences of permanent hypocalcemia and permanent RLN palsy were 10/729 (1.4%) and 5/729 (0.7%), respectively, in the completion thyroidectomy group, while none of the patients in the upfront RAILA group experienced such events (p = 0.006 and p = 0.080, respectively). A higher proportion of patients in the RAILA group (25/514, 4.9% vs. 3/729, 0.4% in completion thyroidectomy group, p < 0.001) experienced grade 1/2 neck pain, which was attributed to radiation thyroiditis owing to the higher residual thyroid tissue in these patients (median 24-hour RAIU = 13.7%, range: 1.2–29.8%).
Nevertheless, these patients were managed with short courses of oral prednisolone (10–40 mg/day, tapered over 15–20 days) and/or nonsteroidal anti-inflammatory drugs. None of the patients experienced xerostomia or xerophthalmia following 131I administration, although one patient in the completion thyroidectomy group had dysgeusia following remnant ablation (Table 4).
Adverse Events in the Two Groups
Included one patient each with dysgeusia, respiratory distress due to postoperative hematoma, and foreign body sensation in the throat.
AE, adverse event.
Nine patients, four in the upfront RAILA group and five in the completion thyroidectomy group, developed secondary primary malignancies in the course of their follow-up (breast cancer, n = 3; non-Hodgkin's lymphoma, n = 1; gall bladder cancer, n = 1; prostate cancer, n = 1; colorectal cancer, n = 1; cervix cancer, n = 1; meningioma, n = 1). The incidence of secondary malignancies was not significantly different between the two groups (p = 0.839). The median cumulative 131I activity administered to these patients was 2.22 GBq (range: 1.11–8.51 GBq, over 1–3 cycles) with the median interval between the first 131I administration and development of secondary malignancy being 86 months (range: 21–120 months) (Table 5).
Characteristics of Patients Developing Second Primary Malignancies
CT, completion thyroidectomy; F, female; HT, hemithyroidectomy; M, male; NHL, non-Hodgkin's lymphoma; SPM, second primary malignancy.
Subgroup analyses
Higher initial administered 131I activity resulted in higher successful ablation rates in both groups, although with higher proportion of patients experiencing radiation thyroiditis (Table 6). Thus, an initial 131I activity of 1.11–1.85 GBq is a reasonably good estimate for successful lobar ablation with minimal radiation-induced thyroiditis. Supplementary Table S1 summarizes the outcomes in groups stratified by indication (clinicopathological characteristics vs. preference) for contralateral lobe ablation.
Subgroup Analyses
Propensity score matching
On propensity score analysis (Supplementary Table S2), 497 matched pairs were generated, and the outcomes in the matched pairs were similar to that in the overall cohort. The ablation rate following the first cycle of 131I was significantly higher in the completion thyroidectomy group compared with that in the upfront RAILA group (84.1% [CI 80.5–87.1] vs. 75.9% [CI 71.8–79.5], respectively, p = 0.001). The recurrence rate was not significantly different between the two groups (1.4% [CI 0.6–3.0] in the RAILA group vs. 1.0% [CI 0.4–2.5] in the completion thyroidectomy group, p = 0.561). The 10-year RFS rates were also similar in the two groups (98.7% vs. 99.1%, respectively) (Table 7).
Matched Pair Analysis by Propensity Score Method
Matched for age, sex, and histopathological variant.
IQR, IQR (1st quartile to 3rd quartile).
Discussion
Completion thyroidectomy has been considered as the conventional standard of care for most patients with DTC after having undergone initial hemithyroidectomy. 13 Few prior studies have evaluated the early outcomes following RAILA as an alternative in this setting, and reported ablation rates of 54–90%. 5 –11 A recent meta-analysis comprising five articles reported a pooled successful ablation rate of 69%, although with high heterogeneity. 14 The initial ablation rate with RAILA reported in this study is, thus, similar to that reported in literature. The results of the current study further establish RAILA as a viable alternative for such patients with excellent long-term outcomes. Being a noninvasive procedure, RAILA is well suited for patients with various comorbidities, who would otherwise be considered at increased risk on resurgery. Furthermore, obviating the need for a second surgery also avoids complications, namely hypocalcemia and RLN injury, as reflected in the results of this study. With favorable long-term results, RAILA can be considered as an acceptable noninvasive alternative to completion thyroidectomy, when such treatment is necessary.
An obvious disadvantage with upfront RAILA is the higher number of cycles required for achieving complete ablation in a quarter of the patients. Given the significantly higher residual functioning thyroid tissue present in these patients, this is expected. One could argue that higher administered activities in the first cycle could lead to higher success rates. However, there is an increased chance of radiation thyroiditis with use of such higher activities. 11 Interestingly, <5% of the patients experienced radiation thyroiditis post-RAILA in our cohort, which could be attributed to the lower activities administered in most patients. We, therefore, believe an activity of 1.11–1.85 GBq per cycle to be optimal for RAILA. The use of repeated cycles of low activities seems to be safe and effective with no increased risk of secondary malignancies. While prior studies have clearly demonstrated no significant increase in cancer risk following 131I therapy over that of the general population, the observed incidence of secondary malignancies was even lower in our cohort. 15 –17
Low-risk DTC usually has excellent long-term outcomes with recurrence rates of only 1–3% reported in literature. 4 Lack of adequate long-term outcomes with upfront RAILA has been a major hurdle in its large-scale acceptability as an alternative to completion thyroidectomy. In this context, the current study is noteworthy since it comprises the largest series of such patients to date with a median follow-up of >10 years. The recurrence rates as well as the 10-year RFS rates in patients undergoing upfront RAILA were not seen to be significantly different from those undergoing completion thyroidectomy. Furthermore, the results were validated by separate analyses in matched pairs generated by propensity score method. While a randomized trial evaluating outcomes with RAILA versus completion thyroidectomy would have been desirable, the same is difficult given the considerably long follow-up required for an indolent cancer such as low-risk DTC. On the contrary, retrospective studies, while having a good follow-up, have several inherent biases. The use of propensity score matching adjusts for possible known confounders in a retrospective study, and therefore, enhances the validity of our study.
The incidence of temporary and permanent hypocalcemia after completion thyroidectomy in this study was similar to that reported after total thyroidectomy in literature. 18,19 Patients experiencing such events often require calcium ± calcitriol supplementation, which presents a significant financial burden, especially in low-to-middle-income countries. This coupled with an increased risk of RLN palsy or other intraoperative complications can result in substantial deterioration in the quality of life of patients undergoing completion thyroidectomy. Upfront RAILA avoids these complications, and can prove to be a cost-effective strategy while also preserving the quality of life of patients.
One argument in favor of completion thyroidectomy is the possibility of the residual lobe also harboring malignancy. In such a scenario, completion thyroidectomy ensures complete removal of the tumor at once. However, only 16.2% of such procedures yielded samples positive for malignancy in our study cohort, all of which were microcarcinomas. Given the low positive yield and the uncertain clinical relevance of incidental papillary microcarcinoma, we see RAILA as an acceptable noninvasive alternative to completion thyroidectomy especially since our study did not show any significant difference in long-term recurrence rates.
The current study has the following limitations: (i) The present series is retrospective and not randomized. (ii) The reported rates of AEs could have been underestimated due to recall bias. (iii) Given the long duration over which the study data were acquired, it was not possible to categorize responses according to the recent ATA guidelines. (iv) Since the present cohort has no control arm of patients who were not ablated after initial hemithyroidectomy, the present study allows no conclusion regarding the potential benefits of ablative therapy beyond the noninferiority of RAILA versus completion thyroidectomy followed by radioiodine ablation. This is especially important in the light of recent evidence where contralateral lobe ablation has been deemed unnecessary for most patients with low-risk DTC. 4 Furthermore, the mentioned indications for contralateral lobe ablation in this study are no longer universally accepted. However, the large sample size and adequate long-term follow-up constitute strengths of the present study, which is further enhanced by matched pair analysis using the propensity score method.
Conclusion
In conclusion, upfront RAILA is shown to be a noninvasive, safe, and effective alternative to completion thyroidectomy in low-risk DTC patients undergoing initial hemithyroidectomy, especially in the absence of macroscopic malignancy in the remaining thyroid lobe.
Footnotes
Authors' Contributions
C.B.: Conception, data acquisition, data analysis, interpretation, article writing, and critical revision. S.S.: Data acquisition, data analysis, interpretation, article writing, and revision. S.B. and A.T.: Data acquisition and article revision.
Author Disclosure Statement
All the authors declare no conflicts of interest.
Funding Information
There are no sources of funding.
Supplementary Material
Supplementary Table S1
Supplementary Table S2