
Abstract
Introduction:
Follicular patterned thyroid nodules with nuclear features of papillary thyroid carcinoma (PTC) encompass a range of diagnostic categories with varying risks of metastatic behavior. Subtypes include the invasive encapsulated follicular variant of PTC (Ienc-fvPTC) and infiltrative fvPTC (inf-fvPTC), with tumors lacking invasive features classified as noninvasive follicular thyroid neoplasms with papillary-like features (NIFTPs). This study aimed to report the clinical and histological features of pediatric cases meeting criteria for these histological subtypes, with specific focus on Ienc-fvPTC and inf-fvPTC.
Methods:
In this retrospective cohort study, pediatric patients with thyroid neoplasms showing follicular patterned growth and nuclear features of PTC noted on surgical pathology between January 2010 and January 2021 were retrospectively reviewed and classified according to the recent 2022 World Health Organization (WHO) criteria. Clinical and histopathologic parameters were described for NIFTP, Ienc-fvPTC, and inf-fvPTC subtypes, with specific comparison of Ienc-fvPTC and inf-fvPTC cases.
Results:
The case cohort included 42 pediatric patients, with 6 (14%), 25 (60%), and 11 (26%) patients meeting criteria for NIFTP, Ienc-fvPTC, and inf-fvPTC, respectively. All cases were rereviewed, and 5 patients originally diagnosed with Ienc-fvPTC before 2017 were reappraised as having NIFTPs. The NIFTP cases were encapsulated tumors without invasive features, lymph node or distant metastasis, or disease recurrence. Ienc-fvPTC tumors demonstrated clearly demarcated tumor capsules and capsular/vascular invasion, while inf-fvPTC tumors displayed infiltrative growth lacking a capsule. inf-fvPTC cases had increased prevalence of malignant preoperative cytology, lymph node metastasis, and distant metastasis (p < 0.01). These cases were treated with total thyroidectomy, lymph node dissection, and subsequent radioactive iodine therapy. Preliminary genetic findings suggest a predominance of fusions in inf-fvPTC cases versus point mutations in Ienc-fvPTC (p = 0.02).
Conclusions:
Pediatric NIFTP and fvPTC subtypes appear to demonstrate alignment between clinical and histological risk stratification, with indolent behavior in Ienc-fvPTC and invasive features in inf-fvPTC tumors.
Introduction
Papillary thyroid carcinoma (PTC) and follicular thyroid carcinoma constitute the predominant histologic subtypes of differentiated thyroid cancer (DTC), with PTC accounting for 90% of new pediatric thyroid cancer cases each year. 1 PTC may be further classified into subtypes—classic, solid, follicular, diffuse sclerosing, and others—with follicular variant of PTC (fvPTC) accounting for 27% of PTC cases. 2 –4 There is an ongoing debate as to the most appropriate stratification of fvPTC for aligning histopathologic features with clinical risk; thus, fvPTC subclassification has undergone significant iteration and continues to evolve. 5
In the 3rd edition of the World Health Organization (WHO) classification guidelines, fvPTC subclassification encompassed two groups—encapsulated and infiltrative—defined by the presence or absence of a well-demarcated capsule circumscribing the tumor. 6 Encapsulated tumors were further classified into invasive and noninvasive subtypes defined by the presence of capsular and/or vascular invasion.
In 2017, the 4th edition of the WHO classification guidelines reclassified noninvasive encapsulated fvPTC (Ienc-fvPTC) as a low-risk neoplasm—noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP)—in accordance with evidence of indolent behavior of these tumors. 7 –9 Subsequent studies and guidelines strengthened classification criteria for NIFTP. 10
Based on this, current adult histopathological practice recognizes three subtypes of follicular patterned lesions with nuclear cytology of PTC: (1) low-risk neoplasm—NIFTP, (2) Ienc-fvPTC, and (3) infiltrative fvPTC (inf-fvPTC). 9,11 –13
Pediatric-specific adoption followed suite with incorporation of NIFTP, Ienc-fvPTC, and inf-fvPTC subtypes in the 2017 WHO classification. 14,15 Subsequent studies in adult and pediatric patients have demonstrated alignment between clinical risk and the fvPTC histopathological spectrum with more clinically invasive features for inf-fvPTC tumors, 14 –17 often in a pattern similar to the diffuse sclerosing variant of PTC (dsvPTC). 18
With fewer malignant subtypes, the current classification system aims to emphasize the invasive clinical characteristics of inf-fvPTC compared with the encapsulated variant (Table 1). 4 Furthermore, this classification implies an opportunity for stratification of clinical management—lobectomy for cases of NIFTP and Ienc-fvPTC compared with total or near-total thyroidectomy (TT) with regional lymph node dissection for inf-fvPTC. 19,20
Morphological Features of Encapsulated and Infiltrative Follicular Variants of Papillary Thyroid Carcinoma in Adults Characterized by the 2022 World Health Organization
ETE, extrathyroidal extension; fvPTC, follicular variant of papillary thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; PTC, papillary thyroid carcinoma; w/w/o, with or without.
Comprehensive clinical guidance, from ultrasound and fine-needle aspiration (FNA) interpretation to surgical recommendations, is continually evolving, although more quickly for adults with these tumors than for children and adolescents. Reporting the clinicopathologic features of the current fvPTC subtypes in pediatrics is necessary to determine follow-up risk-stratified clinical care (e.g., pursuing completion thyroidectomy for Ienc-fvPTC vs. NIFTP).
Additionally, adult studies have reported an association between BRAFV600E mutations and invasive behavior in adult fvPTC, with no reports on somatic oncogenic drivers across the spectrum of pediatric fvPTC. 21 In this study, we expand on a previously published pediatric fvPTC cohort 22 and describe the clinical, pathologic, and preliminary genetic features of NIFTP, Ienc-fvPTC, and inf-fvPTC followed at the Children's Hospital of Philadelphia (CHOP).
Methods
Patients
This retrospective study involving human subjects was reviewed and approved by the Children's Hospital of Philadelphia Institutional Review Board (CHOP IRB #17-014224). Written informed consent from the participant and/or participant's legal guardian was not required as per CHOP IRB; a waiver of consent/parental permission has been approved as per 45 CRF 46.116(d). The CHOP Thyroid Center's clinical registry was screened for patients <19 years of age at the time of surgery between January 2010 and January 2021.
Demographic information; medical history; and cytology, surgical pathology, and treatment information were collected for patients with follicular growth and nuclear features of PTC, as noted on surgical pathology reports. Somatic oncogene data were collected for tumors with molecular analysis performed on Asuragen, ThyroSeq V.3, or CHOP Comprehensive Solid Tumor Panel (CSTP), as previously described. 23 –26
Histologic classification and clinical features
Histology slides were reviewed by two pathologists with subspecialty interest in pediatric (L.F.S.) and adult (Z.B.) thyroid pathology to both further exclude tumors with predominant nonfollicular histology and classify samples according to the established diagnostic criteria and updated 2022 WHO Classification of Tumours of Endocrine Organs. 13
Cases were classified as NIFTP, Ienc-fvPTC, and inf-fvPTC. These classification criteria are summarized for each subtype in Table 1. Capsular invasion was defined as infiltration of tumor cells beyond the tumor capsule. Vascular invasion was defined as infiltration of tumor cells into vascular spaces within the thyroid tissue (<4 foci as focal and ≥4 foci as extensive).
The thyroid tumor size and invasive behavior were defined according to the 8th edition of the American Joint Committee on Cancer (AJCC) guidelines on tumor–node–metastasis (TNM) classification for differentiated and anaplastic thyroid cancer. 27 Postoperative risk stratification was assigned based on the 2015 American Thyroid Association (ATA) Management Guidelines for Children with Thyroid Nodules and DTC. 12 Tumor size (defined as the largest dimension of the dominant tumor), focality, laterality, extrathyroidal extension (ETE), extranodal extension (ENE), and vascular invasion were extracted from surgical pathology reports and confirmed with histology slide rereview (L.F.S. and Z.B.).
Medical records were reviewed by a pediatric endocrinologist specialized in pediatric thyroid cancer care (A.J.B.) for evidence of distant metastasis and one-year remission status, which incorporated evidence of biochemical and structural disease in accordance with Nies et al. 28 When available, preoperative FNA cytology findings and somatic oncogenic drivers were collected and reported according to the 2017 version of The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC). 29
Molecular data were acquired from patient charts from either FNA-based testing (ThyroSeq, Asuragen) or from a research next-generation sequencing panel. 24 –26 The retrospective review was performed under an IRB waiver of consent for retrospective samples, and the CHOP IRB was informed of the study results.
Statistical analysis
Mean (standard deviation [SD]) or median [interquartile range (IQR) = Q1–Q3] was reported for all parametric and nonparametric variables, respectively. Ienc-fvPTC and inf-fvPTC patient clinicopathologic features were statistically compared in R 4.0.5 and R Studio 1.4.1106 using the tidyverse and rstatix packages. 30 –33 Between these groups, median tumor size was assessed using the Mann–Whitney U test, and all categorical variables were assessed using two-tailed Fisher's exact test.
The frequency of malignant cytologic findings between Ienc-fvPTC and inf-fvPTC was compared with two-tailed Fisher's exact test. p Values <0.05 were considered statistically significant.
Results
The initial search revealed 77 of 290 (27%) patients diagnosed with PTC or NIFTP and documented follicular growth pattern on the surgical pathology report. Of these cases, 35 were excluded due to the presence of well-formed papillae resembling cPTC or a growth pattern consistent with Warthin-like, solid, oncocytic, or dsvPTC.
The final case cohort comprised 42 patients, 31 females and 11 males (1:3 M:F) with a mean age at surgery of 16 years (SD = 3.0), including 6 (14%) cases of NIFTP, 25 (60%) cases of Ienc-fvPTC, and 11 (26%) cases of inf-fvPTC (Fig. 1; Table 2).
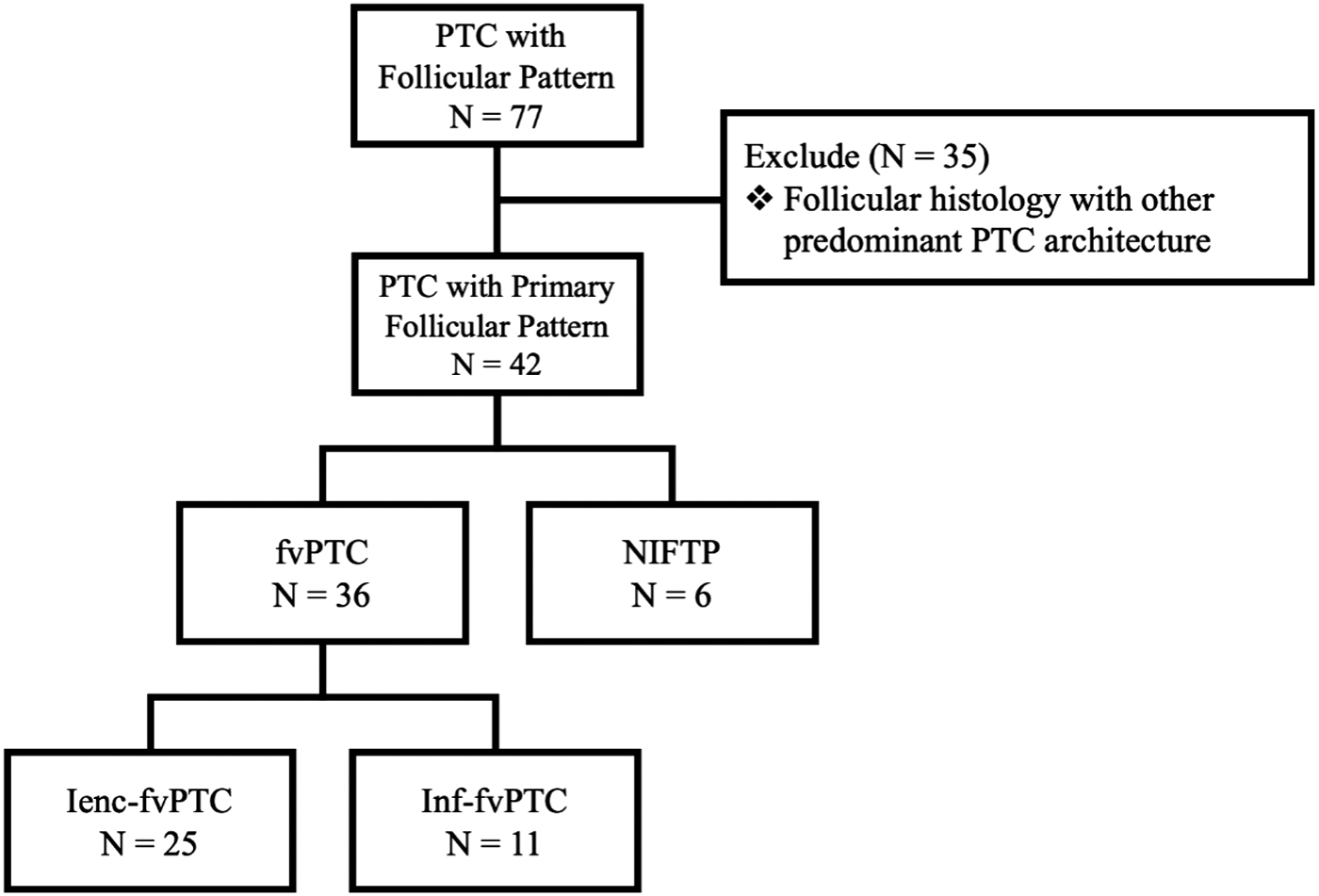
Cohort selection from patients presenting a follicular pattern between 2010 and 2021. fvPTC, follicular variant of papillary thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; Ienc-fvPTC, invasive encapsulated fvPTC; inf-fvPTC, infiltrative fvPTC.
Demographic Features and Treatment for Patients with Encapsulated and Infiltrative Follicular Variants of Papillary Thyroid Carcinoma
SD, standard deviation.
Clinicopathologic features
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features
NIFTP was determined in 6 (14%) cases, including 5 rereviewed cases occurring before 2017 (Fig. 3). Half (3/6) of the patients with NIFTPs had a history of prior childhood malignancy (2 neuroblastoma and 1 acute myeloid leukemia) and received total body irradiation. On preoperative ultrasound, all cases presented as clearly delineated (smooth margin) nodules.
Four patients underwent preoperative FNA and were diagnosed as atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS, TBSRTC III; 1/4, 25%), follicular neoplasm (TBSRTC IV; 2/4, 50%), and suspicious for malignancy (TBSRTC V; 1/4, 25%) cytology according to TBSRTC (Fig. 2A; Table 3). Surgical management included TT ( n = 4), lobectomy (n = 1), or lobectomy with completion thyroidectomy (n = 1). NIFTP tumors had a median tumor size of 0.95 cm (IQR = 0.9–1.1).
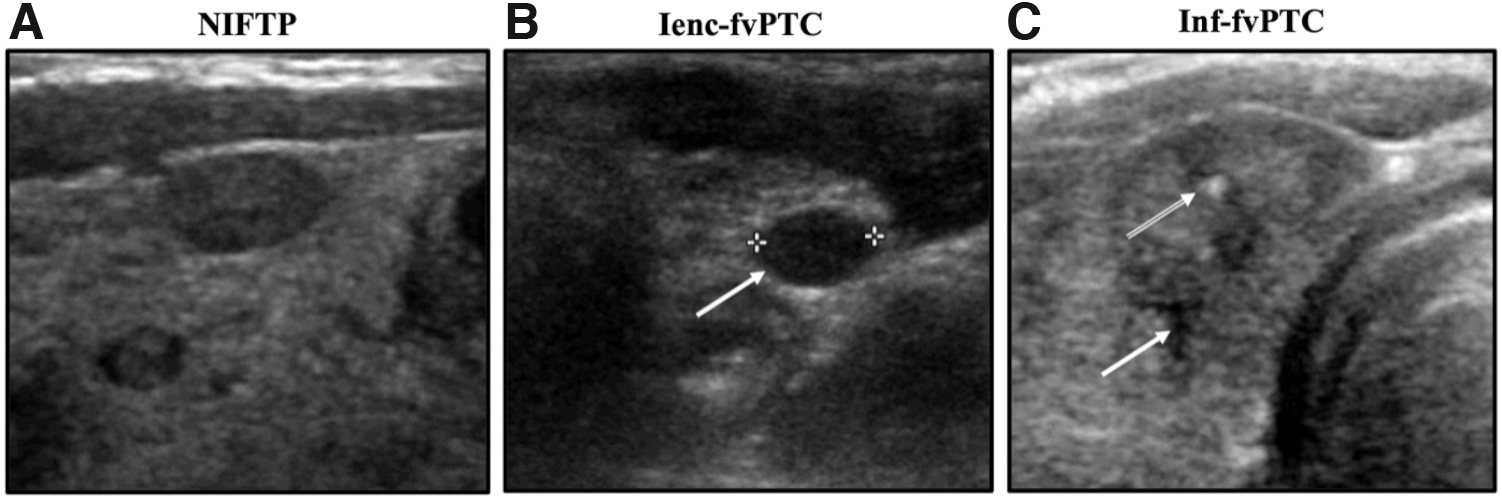
Representative preoperative ultrasound images for NIFTP, Ienc-fvPTC, and inf-fvPTC. (
Fine-Needle Aspiration and the Bethesda Classification for Patients with Encapsulated and Infiltrative Follicular Variants of Papillary Thyroid Carcinoma (N = 37)
A total of 37/42 patients with available FNA reports were studied; NIFTP and invasive encapsulated fvPTC cases without FNA pursued surgery in the setting of prior radiation exposure; infiltrative fvPTC cases without FNA included one patient with unavailable FNA determination performed at an outside institution and one patient with carcinoma identified following definitive surgery for Graves' disease.
§p < 0.01: two-tailed Fisher exact test comparing the frequency of category VI versus noncategory VI findings between encapsulated and infiltrative variants.
AUS/FLUS, atypia/follicular lesion of undetermined significance; TBSRTC, The Bethesda System for Reporting Thyroid Cytopathology.
No lymph node metastases were identified in any patients (AJCC N0a or N0b). One patient elected to pursue radioactive iodine (RAI) therapy secondary to concerns based on prior history of nonthyroid childhood malignancy. All patients remained disease free without evidence of biochemical or anatomical disease (median years between surgery and last clinical follow-up = 3.4 [range = 0.1–7.9]).
Invasive encapsulated follicular variant of papillary thyroid carcinoma
Twenty-five cases (60%) were classified as Ienc-fvPTC. Of these, 3 patients had a history of a primary, nonthyroid childhood malignancy with previous treatment, including total body or cranial radiation, and 1 had a history of Hashimoto's thyroiditis. Representative ultrasound imaging showed well-delineated (smooth margin) nodules (Fig. 2B). Preoperative FNA was performed on 96% (24/25) of patients with Ienc-fvPTC with AUS/FLUS (6/24, 25%), follicular neoplasm (13/24, 54%), suspicious for malignancy (4/24, 17%), and malignant (TBSRTC VI, 1/24, 4%) cytology (Table 3). Surgical resection included TT (14/25, 56%) or lobectomy with/without completion thyroidectomy (11/25, 44%) (Table 4). Ten patients underwent central neck dissection, with lymph node metastasis confirmed in 1 case (AJCC TNM N1a).
Clinicopathologic Features for Patients with Encapsulated and Infiltrative Follicular Variants of Papillary Thyroid Carcinoma
Mann–Whitney U test used to compare nonparametric continuous variables; two-tailed Fisher exact test used to compare categorical variables.
Adopted from 2015 ATA Management Guidelines for Children with Thyroid Nodules and DTC.
Mutational analysis performed on 19 Ienc-fvPTC and 10 inf-fvPTC cases; point mutations: BRAFV600E , N-KRAS, and DICER1; fusions: NTRK3::ETV6, ETV6::MET, RET::NCOA4, RET::CCDC6, and EML4::ALK.
ATA, American Thyroid Association; ENE, extranodal extension; ETE, extrathyroidal extension; Ienc-fvPTC, invasive encapsulated fvPTC; inf-fvPTC, infiltrative fvPTC; ND, not determined; RAI, radioactive iodine; TT, total thyroidectomy.
The majority of Ienc-fvPTC tumors (21/25, 84%) demonstrated unilateral disease, with 4 cases having multifocal bilateral disease. The median size of Ienc-fvPTC tumors was 2.7 cm (IQR = 1.9–4) (Table 4). By microscopic examination, all cases were found to have a well-demarcated tumor capsule; 21 (84%) had capsular invasion (Fig. 3). Four encapsulated tumors without capsular or vascular invasion were classified as Ienc-fvPTC due to the focal papillary growth pattern and architecture, warranting Ienc-fvPTC designation according to Nikiforov et al. 10 Vascular invasion was present in 10 cases (10/25, 40%), including 7 with focal involvement and 3 with extensive involvement. One tumor presented with microscopic ETE.
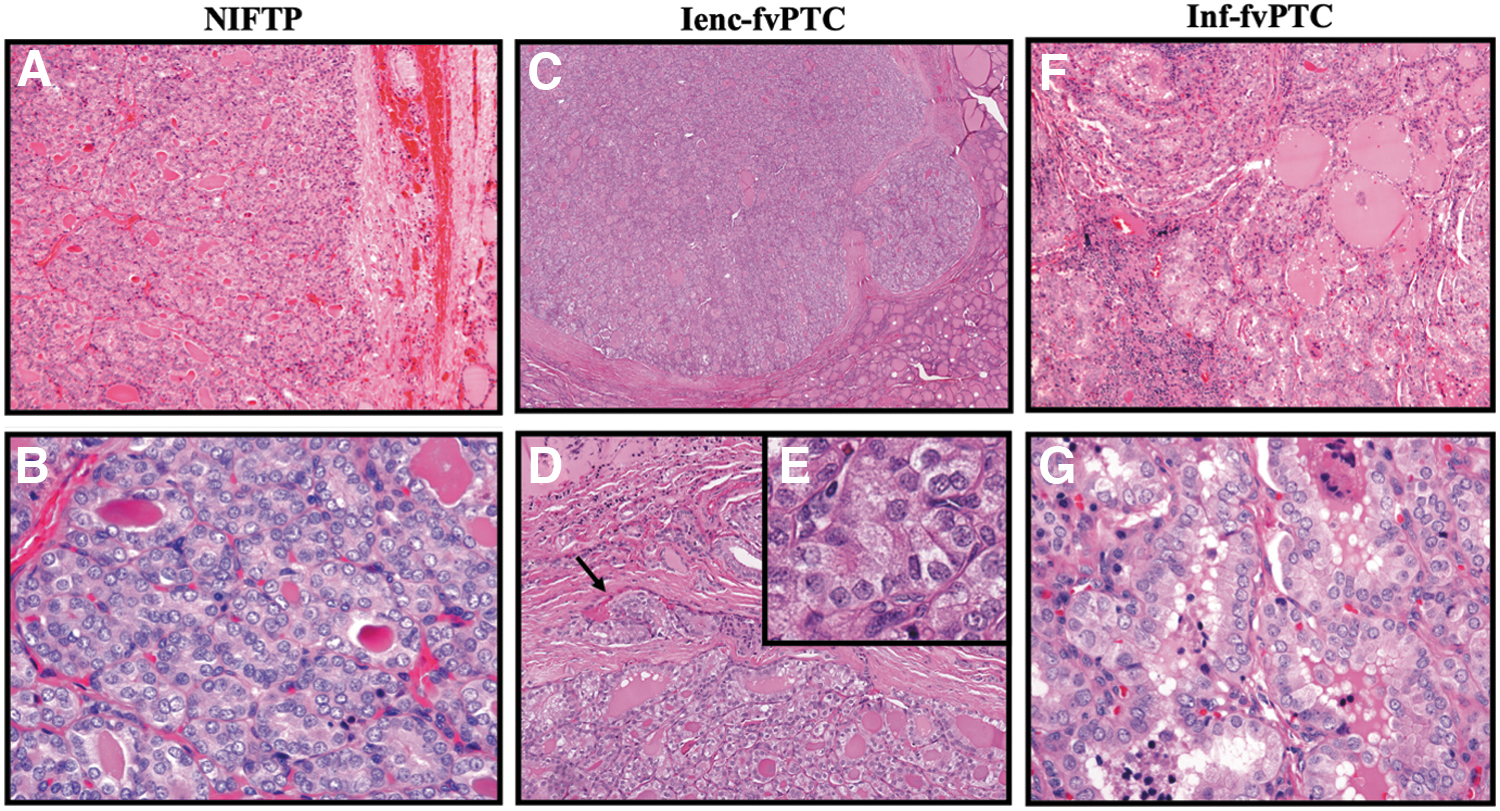
Representative histological images for NIFTP, Ienc-fvPTC, and inf-fvPTC. (
Thirteen patients received RAI therapy without evidence of distant metastasis (M0 staging). One patient was lost to follow-up, and 21 patients (21/25, 84%) achieved biochemical and anatomical remission at 1-year follow-up. All patients who were followed for long-term care/surveillance showed no disease relapse at last follow-up (median years between surgery and last clinical follow-up = 3.3 [range = 0.1–10.7]).
Infiltrative follicular variant of papillary thyroid carcinoma
Eleven cases (11/42, 26%) were classified as inf-fvPTC, including 2 patients who had undergone previous radiation therapy (1 total body and 1 total lung radiation) for their primary nonthyroid childhood malignancy and 2 patients who had a history of autoimmune thyroid disease (1 with Hashimoto's thyroiditis and 1 with Graves' disease). Preoperative ultrasound revealed nodules with irregular margins and punctate echogenic foci (Fig. 2C).
Preoperative FNA was performed on 82% of patients (9/11), revealing predominately malignant cytology (6/9, 67%) as well as 2 (22%) AUS/FLUS cases and 1 (11%) suspicious for malignancy case. A higher frequency of malignant cytology was observed in cases with inf-fvPTC compared with cases with Ienc-fvPTC (p < 0.01, Table 3). The majority of patients (10/11, 91%) with inv-fvPTC were surgically managed with TT, with only 1 undergoing a two-stage surgical approach with lobectomy followed by completion thyroidectomy.
Eight patients underwent regional lymph node dissection, with 2 patients (2/8, 25%) having AJCC TNM N1a disease and 4 patients having AJCC N1b disease (4/8, 50%). The incidence of lymph node metastasis was significantly greater in inf-fvPTC cases compared with Ienc-fvPTC cases (p < 0.01).
The majority of inf-fvPTC tumors were unilateral (7/11, 64%), with 2 cases demonstrating bilateral disease. Histologically, these cases contained a follicular patterned unencapsulated nodule with infiltration of the surrounding thyroid parenchyma (Fig. 3). Five cases (46%) displayed focal vascular invasion, which was comparable with Ienc-fvPTC (40%).
Microscopic ETE (1/11, 9%) and ENE (2/11, 18%) were more frequent in inf-fvPTC cases compared with Ienc-fvPTC cases (p = 0.08, p = 0.09). Eight patients (8/11, 73%) underwent RAI therapy and RAI-avid distant pulmonary metastasis was detected in 4 patients (4/11, 36%) compared with no cases of distant metastasis in the Ienc-fvPTC cohort (p < 0.01).
One patient with inf-fvPTC was lost to follow-up, and 9 patients (9/10, 90%) achieved biochemical and anatomical remission at 1-year follow-up (median years between surgery and last clinical follow-up = 2.3 [range = 0.4–8.5]). One patient continues to have persistent pulmonary metastasis and is being considered for oncogene-specific targeted inhibitor therapy.
Molecular analysis
Two (33%) NIFTP cases had available somatic oncogene data, revealing an NRAS mutation on Asuragen testing and a copy number variation on CSTP. Nineteen (76%) Ienc-fvPTC cases had available somatic oncogene data from Asuragen (9/19, 47%), ThyroSeq (2/19, 11%), and CSTP (10/19, 53%), revealing 8 point mutations (1 BRAFV600E , 2 NRASQ61R , 1 KRASG12V , and 4 DICER1) and 1 fusion (EML4::ALK).
Ten (91%) inf-fvPTC cases had available somatic oncogene data from CSTP, revealing 2 point mutations (BRAFV600E ) and 7 fusions (4 ETV6::NTRK3, 1 ETV6::MET, 1 NCOA4::RET, and 1 CCDC6::RET). The frequency of fusion alterations was significantly higher in inf-fvPTC cases compared with Ienc-fvPTC (p = 0.02, Table 4).
Discussion
In this study, we report our institutional experiences with follicular patterned thyroid lesions classified as NIFTP and fvPTC subtypes in 42 pediatric patients. Studies of large case cohorts have been previously published for adult populations; however, this is the largest sample of combined pediatric NIFTP and fvPTC cases to date (Table 5). Based on our findings and similar reports, Ienc-fvPTC may be more common than NIFTP or inf-fvPTC in children compared with adults, although further studies are needed (Table 5).
Literature Review of Follicular Variant of Papillary Thyroid Carcinoma
Literature review is limited to articles that classify adult or pediatric fvPTC patients into noninvasive enc-fvPTC/NIFTP, Ienc-fvPTC, and inf-fvPTC/widely invasive fvPTC subtypes.
Published before NIFTP diagnostic change.
Kim et al and Mariani et al provide comparable adult and pediatric reports, respectively, with similar histologic classification and study design as this report. 14,34 Considering these reports and this present study, pediatric and adult subtypes present similar histologic and clinical alignment, with more indolent behavior for Ienc-fvPTC and more invasive features for inf-fvPTC. 14,34
The overall prevalence of NIFTP was 14% in the current study, including the 5 reclassified cases on histopathology review, which is similar to adult studies. 35,36 As expected, all NIFTP cases lacked lymph node or distant metastasis and included high disease-free survival similar to adult patients with NIFTPs. 16 Most patients with NIFTPs in this cohort underwent TT, likely reflecting both pre-NIFTP surgical management and high rate of prior radiation exposure in this group where TT is typically preferred over lobectomy.
Current clinical guidelines in adult and associated pediatric studies suggest conservative clinical management with diagnostic lobectomy for cases of suspected NIFTP. 14,37 With relatively high likelihood of indeterminate cytology (AUS/FLUS and follicular neoplasm), NIFTP cannot be diagnosed preoperatively. 38
Therefore, ultrasound nodule characteristics showing a unifocal solid tumor with smooth margins, no punctate echogenic foci, and the absence of abnormal lymph nodes should be integrated with preoperative cytology to select patients for diagnostic lobectomy. Within the pediatric community, there is ongoing discussion about whether the adult criteria for diagnosing NIFTP apply within the pediatric age group as well as what the clinical implications are in regard to management. 39
In this pediatric cohort, Ienc-fvPTC and inf-fvPTC were histopathologically and clinically distinct entities. On preoperative FNA, inf-fvPTC cases displayed more malignant cytology compared with Ienc-fvPTC, and postoperative findings revealed significantly more lymph node and distant metastases among the inf-fvPTC cases. These findings are consistent with a report of pediatric fvPTC cases by Mariani et al, yet notable differences in T staging exist between studies due to the difficulties in providing an exact tumor size for lesions with infiltrative rather than nodular presentation. 14
Consequently, inf-fvPTC cases in this cohort were more likely to receive TT, additional lymph node dissection, and follow-up RAI compared with Ienc-fvPTC cases. Importantly, in our cohort, this apparent surgical and clinical stratification translated to similar rates of one-year follow-up and total disease-free survival. Preoperative invasive sonography features with multiple punctate echogenic foci and evidence of abnormal lymph nodes should raise suspicion for an invasive PTC subtype, of which classic PTC, dsvPTC, and inf-fvPTC are the most common.
While an analysis of SEER data by Zeng et al found a higher incidence of invasive clinical features among classic PTC versus fvPTC cases, this current report highlights a need to consider the invasive potential of inf-fvPTC tumors similar to that of classic PTC tumors. 40
While BRAFV600E mutations are associated with invasive disease in adult populations, pediatric PTCs harboring genetic fusions often present with invasive features, including regional and distant metastases. 21,41 –43 A recent report from our group supports previous publications showing an association between somatic oncogenic fusion drivers (RET, NTRK, and ALK) and clinically invasive behavior in pediatric PTC. 23
Specific to pediatric fvPTC, Lee et al report two cases of infiltrative pediatric fvPTC harboring ETV6::NTRK3 fusions, yet no studies have characterized the genetic landscape of pediatric Ienc- or inv-fvPTC. 42 While analysis is ongoing, preliminary genetic findings in this study suggest that the presence of somatic fusion oncogenes is associated with an increased likelihood of invasiveness in pediatric fvPTC. This is in contrast to previous reports of invasiveness in BRAFV600E -positive adult inf-fvPTC. 23
This study is retrospective in nature and limited to a single-institution experience and may not completely align with the current clinical guidelines for managing pediatric thyroid cancer, which have been evolving over the past decade. In addition, somatic oncogene data are complicated by varying panels with differing sequencing coverage.
Current efforts are focused on uniform fusion testing and expanded genomic characterization of this cohort. While the findings in this study support correlation between fvPTC subtype and clinical risk stratification, future studies must continue refining treatment stratification based on preoperative data, which should include US and cytology, as well as somatic oncogene analysis.
Conclusions
This report showcases the alignment of histological stratification and clinically advanced disease across NIFTP and fvPTC subtypes in pediatric patients. Pediatric NIFTP, Ienc-fvPTC, and inf-fvPTC exist along a gradient of increasing invasiveness. In particular, inf-fvPTC is associated with higher rates of lymph node and distant metastases compared with its encapsulated counterpart as well as presence of fusion oncogenes.
Our findings are similar to those reported in adult patients; however, multicenter studies with sizable case cohorts are warranted to corroborate these findings and prospectively evaluate preoperative treatment stratification for pediatric PTC patients to optimize clinical management and follow-up.
Footnotes
Authors' Contributions
S.H. and J.A.B. were involved in conceptualization, writing—original draft, investigation, formal analysis, and visualization. A.J.B. was involved in conceptualization, writing—original draft, investigation, supervision, funding acquisition, and project administration. J.C.R.-F, A.I., and A.T.F. were involved in conceptualization, investigation, and writing—review and editing. T.P. was involved in conceptualization, investigation, and data curation. S.M.-M., N.S.A., K.K., and T.R.B. were involved in conceptualization and writing—review and editing. Z.B. and L.F.S. were involved in conceptualization, writing—original draft, investigation, supervision, funding acquisition, and project administration.
Statement of Ethics
This retrospective study involving human subjects was reviewed and approved by the Children's Hospital of Philadelphia Institutional Review Board (CHOP IRB #17-014224). Written informed consent from the participant and/or participant's legal guardian was not required as per CHOP IRB; a waiver of consent/parental permission has been approved as per 45 CRF 46.116(d).
Author Disclosure Statement
This research was conducted in the absence of commercial or financial conflicts. A.T.F. is on the Board of Directors for the American Thyroid Association.
Funding Information
This work was supported, in part, by NIH R01CA21451 (A.T.F.) and a Children's Hospital of Philadelphia Frontier Program Grant.