
Abstract
Background:
It is uncertain whether the presence of autoimmune thyroiditis (AIT) increases the risk of thyroid cancer in children with thyroid nodules. This study evaluated the association between AIT and thyroid cancer in pediatric patients with thyroid nodules.
Methods:
A cross-sectional study was performed of pediatric patients (<19 years old) with a thyroid nodule (≥1 cm) who underwent fine-needle aspiration in an academic pediatric thyroid center. AIT was defined by the presence of thyroid autoantibodies or diffusely heterogeneous sonographic echotexture. The primary outcome was diagnosis of thyroid cancer. The association of AIT with thyroid cancer was evaluated with univariable and multivariable logistic regression. Associations of AIT with subject and nodule characteristics were also assessed.
Results:
Four hundred fifty-eight thyroid nodules in 385 patients (81% female) were evaluated at a median age of 15.5 years (interquartile range 13.5–17.0). Thyroid cancer was present in 108 nodules (24%). AIT was present in 95 subjects (25%) and was independently associated with an increased risk of thyroid cancer (multivariable odds ratio [OR] 2.19, 95% confidence interval [CI] 1.32–3.62). Thyroid cancer was also independently associated with younger age, nodule size, and solitary nodules, but was not associated with serum thyrotropin concentration. AIT was not associated with the likelihood of subjects undergoing thyroid surgery (p = 0.17). AIT was less commonly associated with follicular thyroid carcinoma than with papillary thyroid carcinoma (OR 0.22, CI 0.05–1.06). Among papillary thyroid carcinomas, AIT was strongly associated with the diffuse sclerosing variant (OR 4.74, CI 1.33–16.9). AIT was not associated with the extent of local, regional, or distant disease at thyroid cancer diagnosis.
Conclusions:
AIT is independently associated with an increased risk of thyroid cancer in children with thyroid nodules. These findings suggest that the evaluation of thyroid autoantibodies and thyroid echotexture may inform thyroid cancer risk assessment and surgical decision-making in children with thyroid nodules.
Introduction
Autoimmune thyroiditis (AIT) is the most common thyroid disorder in the pediatric population, occurring in ∼5–6% of children. 1 AIT consists of chronic cell-mediated autoimmune inflammation of the thyroid, and affected individuals may develop goiter or thyroid dysfunction. 2 Chronic inflammation contributes to the development of cancer in some tissues, such as the liver (hepatitis C) and colon (inflammatory bowel disease). 3 –5 An association between AIT and thyroid cancer has been suggested, but supporting data are inconsistent. 6,7 Some studies have reported a higher prevalence of thyroid cancer in children with AIT than in healthy children, but these studies may be limited by ascertainment bias. 2,8 –11
Thyroid nodules are more common in children with AIT (4–19%) 2,8 –11 than in children without AIT (0.5–2%), 12 but it is unclear whether the presence of AIT increases the risk of thyroid cancer in children with thyroid nodules. AIT is associated with elevated thyroid cancer risk in adults with thyroid nodules, 13 but studies of this association in children have been conflicting. 14,15 Clarifying whether AIT is associated with thyroid cancer in children could inform cancer risk assessment and surgical decision-making in children with thyroid nodules.
An important consideration in studying AIT and cancer risk is the criteria used to diagnose AIT. Definitive diagnosis of AIT is based on characteristic histopathological findings. 13 However, because histological confirmation is impractical and unnecessary in most cases, AIT usually is diagnosed clinically by the presence of circulating autoantibodies to thyroperoxidase (TPO) or thyroglobulin (Tg) and/or diffusely heterogenous thyroid echotexture on ultrasonography. 13,16 Therefore, a clinically relevant definition of AIT for studies of cancer risk should include all features (autoantibodies and/or sonographic heterogeneity) that could identify AIT preoperatively. 17 A definition of AIT that includes histopathology cannot guide decisions regarding surgery for possible cancer, but may elucidate potential pathophysiological relationships between autoimmunity and thyroid cancer.
This cross-sectional study investigated whether AIT was associated with thyroid cancer in a large cohort of children who underwent evaluation for thyroid nodules in an academic pediatric thyroid center over 23 years. Based on data from adult studies, we hypothesized that the presence of AIT was associated with an increased risk of thyroid cancer in children with thyroid nodules. In particular, we sought to determine whether clinically diagnosed AIT, defined by parameters available preoperatively, was associated with thyroid cancer risk in this population.
Materials and Methods
Subjects
We reviewed the medical records of all patients <19 years old who underwent fine-needle aspiration (FNA) of a nonautonomous thyroid nodule ≥1 cm in diameter between 1998 and 2020 in the Thyroid Center at Boston Children's Hospital and Brigham and Women's Hospital. Subjects with a genetic condition associated with thyroid neoplasia were excluded. Thyroid ultrasounds were interpreted by radiologists with expertise in thyroid ultrasonography. All ultrasound reports utilized a standardized reporting system in which the presence of diffusely heterogenous echotexture was documented, if present. FNA cytology, interpreted by experienced thyroid cytopathologists, was reported according to the Bethesda System for Reporting Thyroid Cytopathology. 18 Although the Bethesda System was formally published during the study period, cytopathologists used diagnostic criteria and terminology consistent with the Bethesda System throughout the study period. Serum concentrations of thyrotropin (TSH), TPO antibodies, and Tg antibodies were measured at the discretion of the treating provider using institution-specific assays.
This study was approved by the Institutional Review Boards of Boston Children's Hospital and Brigham and Women's Hospital (protocol M10-08-0444).
Data collection
Demographic and clinical characteristics of subjects were abstracted from the medical record. Thyroid ultrasound reports were reviewed for thyroid echotexture and the presence and size of thyroid nodules. Ultrasound images were reviewed by a radiologist with expertise in thyroid ultrasound (D.M.R.) when needed for clarification. The FNA cytology of each nodule was recorded. The most recent serum concentrations of TSH, TPO antibodies, and Tg autoantibodies before the date of thyroid ultrasound were recorded, if available. TPO or Tg autoantibodies were considered to be present if their concentration exceeded the assay-specific reference range. Subjects in whom TPO or Tg autoantibodies were not measured were presumed to be negative. Levothyroxine treatment at the time of FNA was recorded.
The presence of AIT was classified using two definitions. Clinical AIT (cAIT) was defined by the presence of at least one of the following: (1) autoantibodies to TPO or Tg, or (2) diffusely heterogenous thyroid echotexture. Aggregate AIT (aAIT) was defined by the presence of either cAIT or findings of diffuse lymphocytic thyroiditis on surgical histopathology. 13
The presence or absence of thyroid cancer was defined by histopathology for resected nodules. Histopathology was reviewed by an experienced thyroid pathologist (M.L.H.) for clarification, if needed. Unresected nodules with malignant cytology (Bethesda VI) were considered to be cancer. Unresected nodules were considered to be benign if they had benign cytology (Bethesda II) and no increase in size by ultrasound for one year or more, or if they had nondiagnostic (Bethesda I) or indeterminate cytology (Bethesda III, IV, or V) and no increase in size for two years or more. Nodules for which the presence or absence of thyroid cancer could not be assessed by these criteria were excluded from analysis. Differentiated (nonmedullary) thyroid cancers were classified according to the tumor, node, metastasis (TNM) staging system of the American Joint Committee on Cancer, 8th Edition. 19 Study data were managed using REDCap Software Version 11.1.17. 20
Statistical analysis
The primary study outcome was the presence of thyroid cancer. Associations of subject and nodule characteristics with the primary outcome were evaluated by univariable logistic regression. Characteristics associated in univariable analysis (p < 0.1) were included in multivariable logistic regression to identify independent risk factors for thyroid cancer. The primary analysis evaluated the association of cAIT with thyroid cancer. Both subject-level and nodule-level analyses were performed. All analyses were then repeated using aAIT in place of cAIT. Associations of cAIT and aAIT with subject and nodule characteristics, FNA cytology, thyroid cancer type, and TNM stage were evaluated using chi-squared or Fisher exact analysis for categorical variables and Student's t-test or Mann–Whitney U test for continuous variables.
To evaluate the diagnostic accuracy of cAIT, considering histopathological thyroiditis as the gold standard, a subanalysis was performed of subjects who underwent thyroid surgery and had at least one of the following: (1) diffusely heterogeneous echotexture, or (2) positive antibodies to TPO and/or Tg, or (3) both TPO and Tg antibodies measured and negative. Analyses were performed using SPSS version 27 (IBM Corp).
Results
Subject characteristics
During the study period, 609 thyroid nodules in 491 pediatric patients underwent FNA. One hundred fifty-one nodules in 105 patients were excluded due to nodule autonomy (n = 28), size <1 cm (n = 17), genetic risk of thyroid neoplasia (n = 60), or insufficient data to determine the presence of thyroid cancer (n = 46, Fig. 1). Therefore, 458 nodules in 385 subjects were included in the analysis (Table 1). The median age at FNA was 15.5 years (range 3.8–18.9, interquartile range 13.5–17.0) and most subjects were female (81%). A history of radiation exposure was present in 26/385 subjects (7%), and 76/385 subjects (20%) had multiple nodules. Thyroid surgery was performed in 187/385 subjects (49%). Malignancy was present in 104/385 subjects (27%) and in 108/458 nodules (24%).
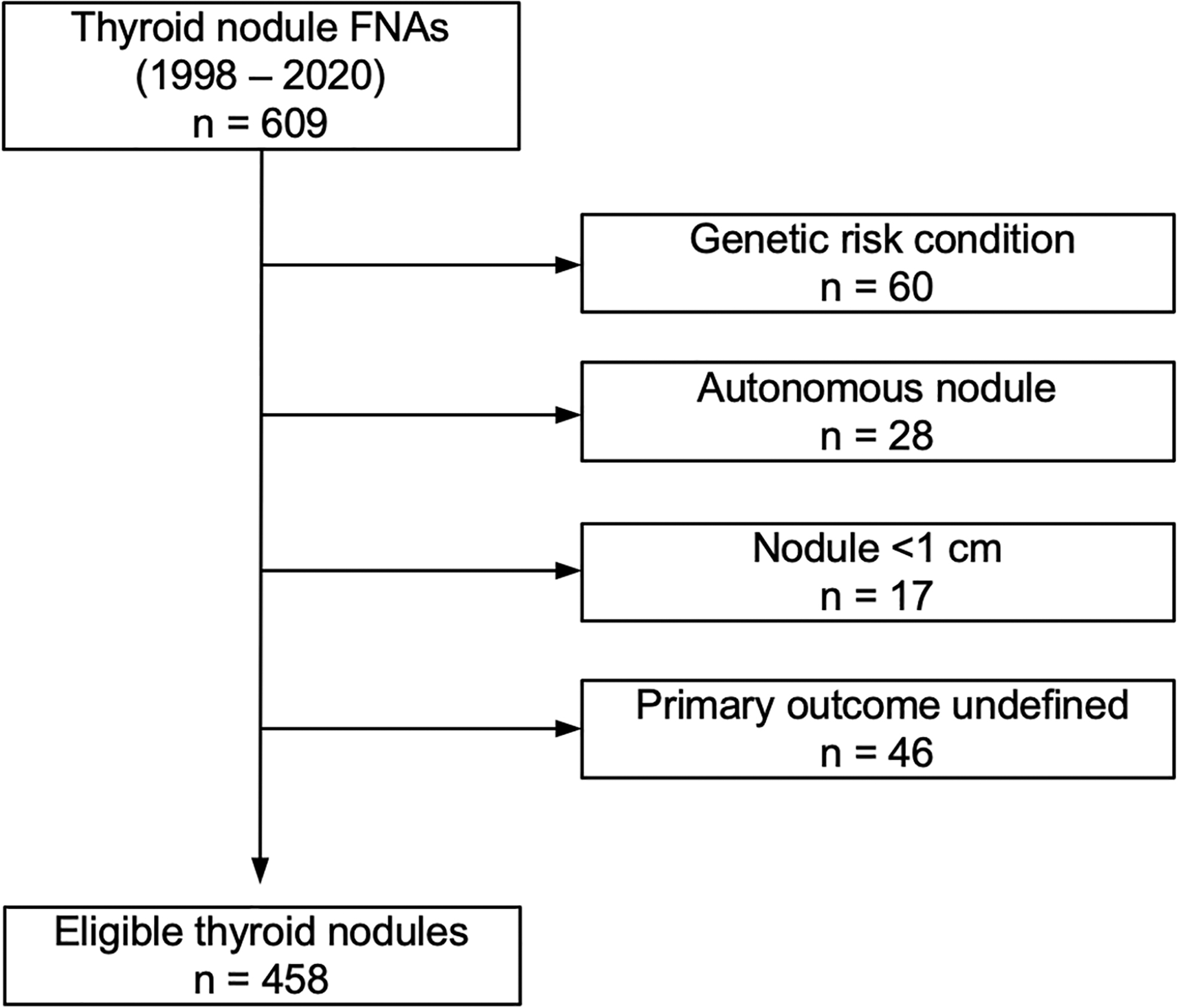
Flowchart of nodules in the cohort that met the inclusion/exclusion criteria.
Characteristics of Pediatric Patients with Thyroid Nodules and Associations of Subject and Nodule Characteristics with the Presence of Clinical Autoimmune Thyroiditis or Aggregate Autoimmune Thyroiditis
cAIT was defined by the presence of thyroid autoantibodies or diffusely heterogeneous thyroid echotexture. aAIT was defined by the presence of cAIT or histopathological chronic lymphocytic thyroiditis. Values are expressed as n (%) or median (interquartile range).
Data not available for 27 nodules in 22 subjects.
aAIT, aggregate autoimmune thyroiditis; cAIT, clinical autoimmune thyroiditis; TSH, thyrotropin.
cAIT was present in 95/385 subjects (25%) and aAIT was present in 109/385 (28%). Subjects with cAIT had a higher median serum TSH concentration than subjects without cAIT (2.5 mIU/L vs. 1.3 mIU/L, p < 0.001) (Table 1). Subjects with cAIT were more likely to be treated with levothyroxine (19% vs. 5%, p < 0.001). The presence of cAIT was not associated with median nodule size (20 mm vs. 22 mm, p = 0.10) or with the likelihood of subjects undergoing thyroid surgery (55% vs. 47%, p = 0.17). cAIT was associated with a decreased prevalence of radiation exposure (2% vs. 8%, p = 0.04). Similar associations were found for aAIT, except that aAIT was associated with a higher rate of thyroid surgery (63% vs. 43%, p < 0.001). Similar results were obtained in nodule-level and subject-level analyses (Table 1).
AIT and thyroid cancer
cAIT was associated with an increased risk of thyroid cancer in thyroid nodules (odds ratio [OR] 2.08, 95% confidence interval [CI] 1.30–3.36, p = 0.002) (Table 2 and Fig. 2). Thyroid cancer was directly associated with nodule diameter (OR 1.05, CI 1.03–1.06, p < 0.001) and inversely associated with age (OR 0.90, CI 0.83–0.97, p = 0.007) and the presence of multiple nodules (OR 0.37, CI 0.21–0.63, p < 0.001). Thyroid cancer was not associated with subject sex, radiation exposure, or serum TSH concentration (Table 2). There was no association between levothyroxine treatment and the presence of thyroid cancer (p = 0.16).
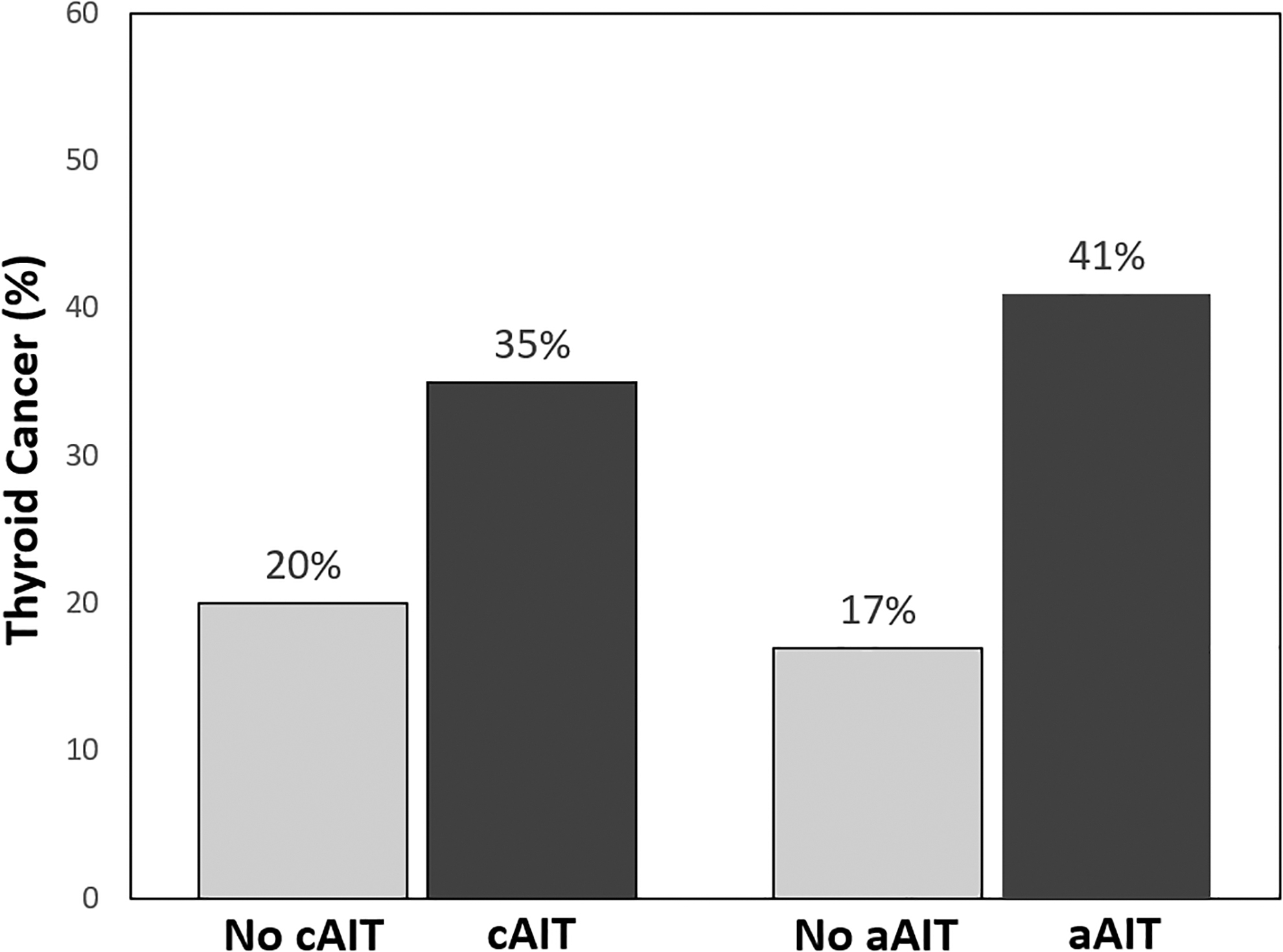
Prevalence of malignancy in pediatric thyroid nodules in the presence or absence of clinical autoimmune thyroiditis (p = 0.002) or aggregate autoimmune thyroiditis (p < 0.001).
Associations of Subject and Nodule Characteristics with Malignancy Among Children with Thyroid Nodules
cAIT was defined by the presence of thyroid autoantibodies or diffusely heterogeneous thyroid echotexture. aAIT was defined by the presence of cAIT or histopathological chronic lympocytic thyroiditis. Values are expressed as n (%) or median (interquartile range).
Data not available for 27 nodules in 22 subjects.
CI, 95% confidence interval; OR, odds ratio.
In multivariable analysis, thyroid cancer was independently associated with cAIT (OR 2.40, CI 1.42–4.03, p = 0.001) and with a larger nodule diameter (OR 1.05, CI 1.03–1.07, p < 0.001). Female sex (OR 0.53, CI 0.29–0.92, p = 0.02) and the presence of multiple nodules (OR 0.48, CI 0.27–0.85, p = 0.01) were independently associated with a lower risk of thyroid cancer (Table 2).
In subject-level analyses, cAIT had a similar independent association with thyroid cancer (OR 2.19, CI 1.32–3.62, p = 0.002). Thyroid cancer was not associated with sex or multiple nodules, but its inverse association with age remained significant (OR 0.92, CI 0.84–0.99, p = 0.03) (Table 2). The findings were similar in secondary analyses evaluating aAIT in place of cAIT. The presence of aAIT was independently associated with thyroid cancer (OR 3.79, CI 2.30–6.24, p < 0.001) (Table 2 and Fig. 2).
FNA cytology
Most thyroid nodules had benign cytology (299/458, 65%). cAIT was associated with a higher likelihood of cytological results that were malignant (OR 2.63, CI 1.37–5.05, p = 0.004) or suspicious for malignancy (OR 2.27, CI 1.05–4.93, p = 0.04) (Table 3); similar associations were observed for aAIT. Within individual cytological categories, there was no association between the presence of cAIT and thyroid cancer (Table 4). All Bethesda IV and V nodules, and 33/36 Bethesda III nodules (92%), were resected.
Associations of Pediatric Thyroid Nodule Cytology with Clinical Autoimmune Thyroiditis or Aggregate Autoimmune Thyroiditis
cAIT was defined by the presence of thyroid autoantibodies or diffusely heterogeneous thyroid echotexture. aAIT was defined by the presence of cAIT or histopathological chronic lymphocytic thyroiditis. Values are expressed as n (%).
AUS, atypia of undetermined significance; SFN, suspicious for follicular neoplasm; SUSP, suspicious for malignancy.
Association of Thyroid Cancer Risk with Clinical Autoimmune Thyroiditis or Aggregate Autoimmune Thyroiditis, Within Cytopathological Categories in Children with Thyroid Nodules
cAIT was defined by the presence of thyroid autoantibodies or diffusely heterogeneous thyroid echotexture. aAIT was defined by the presence of cAIT or histopathological chronic lymphocytic thyroiditis. Values are expressed as n (%).
Thyroid cancer characteristics
The most common type of thyroid cancer was papillary thyroid carcinoma (PTC, 86/105, 82%), followed by follicular thyroid carcinoma (FTC, 15/105, 14%). FTC was associated with a decreased prevalence of cAIT (OR 0.22, CI 0.05–1.06, p = 0.04) (Table 5). Among PTCs, the diffuse sclerosing variant (DSV) was associated with a higher prevalence of cAIT compared with the classical (OR 4.74, CI 1.33–16.9, p = 0.02) or follicular variant (OR 15.0, CI 2.80–80.4, p = 0.002) (Table 5). Among differentiated thyroid cancers, cAIT was not associated with TNM stage at diagnosis, including advanced local invasion (T3b or T4), lateral cervical lymph node metastasis (N1b), or distant metastasis (M1) (Table 6). Similar results were observed for aAIT.
Association of Pediatric Thyroid Cancer Type with Clinical Autoimmune Thyroiditis or Aggregate Autoimmune Thyroiditis
cAIT was defined by the presence of thyroid autoantibodies or diffusely heterogeneous thyroid echotexture. aAIT was defined by the presence of cAIT or histopathological chronic lymphocytic thyroiditis. Excludes unresected malignancies (n = 3). Values are expressed as n (%).
FTC, follicular thyroid carcinoma; HCC, Hürthle cell carcinoma; MTC, medullary thyroid carcinoma; PTC, papillary thyroid carcinoma.
Association of Differentiated Thyroid Cancer Disease Extent with Clinical Autoimmune Thyroiditis or Aggregate Autoimmune Thyroiditis
cAIT was defined by the presence of thyroid autoantibodies or diffusely heterogeneous thyroid echotexture. aAIT was defined by the presence of cAIT or histopathological chronic lymphocytic thyroiditis. Excludes subjects with unresected malignancies (n = 3) or nonthyroid malignancies (n = 2). Values are expressed as n (%).
Diagnostic accuracy of cAIT
The diagnostic accuracy of cAIT compared with the gold standard of histological thyroiditis was assessed in 77 subjects in whom histopathology, sonographic echotexture, and thyroid autoantibodies were evaluated. cAIT had a sensitivity of 94% (43/46) and specificity of 71% (22/31) for histological thyroiditis. The positive predictive value of cAIT for histological thyroiditis was 83% (43/52) and its overall diagnostic accuracy was 84% (65/77). Of subjects with histological thyroiditis who did not have cAIT, one had a 2.7 cm classical variant of PTC and two had benign nodules. Of the nine subjects without histological thyroiditis who had cAIT, five had diffusely heterogeneous echotexture (including one with both TPO and Tg antibodies), and four had positive TPO or Tg antibodies (both in one case) with normal echotexture. High interobserver reliability for evaluating thyroid sonographic echotexture in our institution has been reported previously (κ = 0.78). 21
Discussion
In this large cross-sectional study of pediatric patients with thyroid nodules, the presence of AIT was independently associated with an increased risk of thyroid cancer. This association was consistent in nodule-level and subject-level analyses and was present whether the definition of AIT included the gold standard of histopathology or was based on clinical factors that can be assessed preoperatively. The presence of cAIT was associated with a twofold increase in cancer risk, which suggests that evaluating thyroid autoantibodies and thyroid echotexture during thyroid nodule evaluation in children may provide useful information to guide cancer risk assessment and surgical decision-making.
Several lines of evidence have suggested an association between AIT and thyroid cancer in children. Histopathological studies in adults 22,23 and children 24 have demonstrated such an association, but studies limited to resected nodules may suffer from ascertainment bias because individuals with AIT may be more likely to undergo ultrasound evaluation or thyroid surgery that leads to a thyroid cancer diagnosis. Uncontrolled studies of children with AIT and thyroid nodules have observed thyroid cancer rates (6–28%) 2,8 –11 similar to rates reported among thyroid nodules in the general pediatric population (19–39%). 25 –28 In contrast, a prospective study of 9851 adults with thyroid nodules reported an increased risk of thyroid cancer among individuals with AIT. 13
In this study, a direct comparison of children with and without AIT who underwent standardized evaluation for thyroid nodules confirms an association of AIT with thyroid cancer. This is consistent with the results of a study of 219 children with thyroid nodules that found a 1.9-fold increased risk of cancer in subjects with AIT; however, this association was not statistically significant, perhaps because of the smaller cohort size. 15
In contrast, another study of 241 children found no association of thyroid cancer with AIT. 14 These discrepancies may be caused partly by differences in study size and cohort selection, since some studies have included children with smaller nodules (≥5 mm) or have defined AIT solely by the presence of thyroid autoantibodies. By analyzing clinically significant nodules (≥1 cm) and using an inclusive definition of cAIT based on serology or sonographic heterogeneity, we sought to reflect more accurately the clinical practice of thyroid nodule evaluation in children.
TSH is a proposed mediator of an association between AIT and thyroid cancer. AIT-induced hypothyroidism can cause increased serum TSH concentration, which has been associated with an increased risk of cancer in adults with thyroid nodules. 29,30 However, evidence for an association between TSH and cancer among children with thyroid nodules has been conflicting.8,14,15,25,31,32 In this study, TSH concentrations were higher in subjects with AIT, but TSH concentration was not associated with thyroid cancer. This suggests that the association of AIT with thyroid cancer in children is not mediated by elevated TSH concentrations and perhaps may be related more directly to thyroid inflammation.
In this cohort of children evaluated for thyroid nodules, AIT was associated with a higher prevalence of FNA cytological results in the malignant and suspicious for malignancy categories, which is consistent with the observed association of AIT with thyroid cancer. However, it remains unclear whether the presence of cAIT may influence the assessment of cancer risk within specific cytological categories, as has been demonstrated in adults. 13 Such an association would be useful to evaluate in children and might help refine the assessment of thyroid cancer risk that guides surgical decision-making, particularly in cytologically indeterminate nodules with intermediate cancer risk. However, larger pediatric sample sizes will be necessary because of the rarity in children of nodules in the relevant indeterminate categories.
As in other pediatric and adult studies, PTC was the most common type of thyroid cancer in this cohort, followed by FTC. The prevalence of AIT was higher among PTCs than among FTCs, although this difference was of borderline statistical significance. Among subjects with PTC, the DSV was associated with a much higher prevalence of AIT than either the classical or follicular variant. This association is not surprising given the prominent lymphocytic infiltration that is characteristic of the DSV. 33 This variant has been associated with more advanced disease at presentation, including increased rates of regional and distant metastasis, 34,35 although whether this advanced presentation is associated with a poorer prognosis is unclear. 36 –39 Despite the association of AIT with the DSV of PTC in this study, no association was observed between the presence of AIT and the extent of local invasion or regional or distant metastasis at thyroid cancer diagnosis.
The strengths of this study include its consecutive design and the standardized assessment of thyroid nodules in a large cohort of pediatric subjects. In addition, avoiding surgical ascertainment bias was an important goal of the study design. 40 Because cAIT was not associated with the likelihood of undergoing thyroid surgery, the association of cAIT with thyroid cancer is not likely to be influenced by ascertainment bias. On the contrary, the observed association between aAIT and the likelihood of thyroid surgery was expected because aAIT was defined, in part, by surgical histopathology.
The limitations of this study are primarily related to its retrospective nature. By design, not all cases of AIT were confirmed by the gold standard of histopathology. However, the diagnosis of cAIT by serologic and sonographic criteria more closely reflects the clinical practice of thyroid nodule evaluation, in which decisions regarding thyroid surgery must be made before obtaining histopathology. Moreover, the diagnosis of cAIT was highly accurate with respect to the histopathological standard in the subset of subjects in whom this could be assessed.
Another limitation is that thyroid autoantibodies were not measured in all subjects, which could have resulted in misclassification of AIT in some subjects. However, such misclassification would be expected to bias the results toward finding no association and so is unlikely to affect the validity of these results. In addition, the causality of the association between AIT and thyroid cancer cannot be demonstrated in this observational study. Because this study was performed in subjects with identified thyroid nodules, it does not provide data regarding the prevalence of thyroid nodules or thyroid cancer among all children with AIT, which have been reported in other studies. 2,8 –11 Therefore, these data should not be interpreted as direct evidence to support routine ultrasound screening of children with AIT who have no clinical evidence of thyroid nodules.
Finally, this study did not have sufficient power to assess whether the presence of AIT was associated with an increased risk of thyroid cancer among nodules within individual cytological categories.
Conclusions
In this cohort of children with thyroid nodules, the presence of AIT was associated with an increased risk of thyroid cancer, but not with thyroid cancer stage at diagnosis. A clinical diagnosis of AIT based on the presence of thyroid autoantibodies or diffusely heterogeneous thyroid echotexture may inform the assessment of thyroid cancer risk and surgical decision-making in children with thyroid nodules.
Footnotes
Authors' Contributions
G.K.: Methodology, investigation, writing—original draft, and visualization. K.C.: Methodology, investigation, and writing—review and editing. C.E.C.: Methodology, investigation, and writing—review and editing. J.R.S.: Methodology, investigation, and writing—review and editing. B.Z.: Investigation and writing—review and editing. R.C.S.: Conceptualization, investigation, and writing—review and editing. D.M.R.: Methodology, investigation, and writing—review and editing. M.L.H.: Conceptualization, methodology, investigation, and writing—review and editing. B.P.M.: Conceptualization, methodology, investigation, supervision, and writing—review and editing. A.J.W.: Conceptualization, methodology, investigation, formal analysis, data curation, writing—review and editing, visualization, and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.