
Abstract
Background:
Thyroid dysfunction has been observed among some patients with coronavirus disease (COVID-19). It is unclear whether severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection (or its severity) leads to the development of thyroid dysfunction, or vice versa. In this study, we examined the bi-directional causal relationship between host genetic liability to three COVID-19 phenotypes (including SARS-CoV-2 infection, hospitalized and severe COVID-19) and three thyroid dysfunction traits (including hyperthyroidism, hypothyroidism, and autoimmune thyroid disease [AITD]) and three continuous traits of thyroid hormones (including thyrotropin [TSH] and free thyroxine [fT4] within reference range, and TSH in full range).
Methods:
Summary statistics from the largest available meta-analyses of human genome-wide association studies were retrieved for the following variables: SARS-CoV-2 infection (n = 1,348,701), COVID-19 hospitalization (n = 1,557,411), severe COVID-19 (n = 1,059,456), hyperthyroidism (n = 51,823), hypothyroidism (n = 53,423), AITD (n = 755,406), TSH within reference range (n = 54,288), fT4 within reference range (n = 49,269), and TSH in full range (n = 119,715). Using a two-sample Mendelian randomization (MR) approach, the inverse-variance weighted (IVW) method was adopted as the main MR analysis. Weighted median, contamination mixture, MR-Egger, and MR pleiotropy residual sum and outlier (MR-PRESSO) methods were applied as sensitivity analyses.
Results:
Host genetic susceptibility to SARS-CoV-2 infection was causally associated with hypothyroidism in the main IVW analysis (per doubling in prevalence of SARS-CoV-2 infection, odds ratio [OR] = 1.335; 95% confidence interval [CI]: 1.167–1.526; p = 2.4 × 10−5, surpassing the Bonferroni multiple-testing threshold). Similar causal estimates were observed in the sensitivity analyses (weighted median: OR = 1.296; CI: 1.066–1.575; p = 9 × 10−3; contamination mixture: OR = 1.356; CI: 1.095–1.818; p = 0.013; MR-Egger: OR = 1.712; CI: 1.202–2.439; p = 2.92 × 10−3, and MR-PRESSO: OR = 1.335; CI: 1.156–1.542; p = 5.73 × 10−4). Host genetic liability to hospitalized or severe COVID-19 was not associated with thyroid dysfunction or thyroid hormone levels. In the reverse direction, there was no evidence to suggest that genetic predisposition to thyroid dysfunction or genetically determined thyroid hormone levels altered the risk of the COVID-19 outcomes.
Conclusions:
This bi-directional MR study supports that host response to SARS-CoV-2 viral infection plays a role in the causal association with increased risk of hypothyroidism. Long-term follow-up studies are needed to confirm the expected increased hypothyroidism risk.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first identified to cause clusters of fatal pneumonia in Wuhan, China, in December 2019 (1). Two years after announcement of the coronavirus disease (COVID-19) outbreak as a pandemic by the World Health Organization (WHO) on March 11, 2020, there have been more than 500 million confirmed cases of COVID-19 and more than 6 million deaths globally as of April 2022.
Since SARS-CoV-2 enters human cells via the angiotensin converting enzyme 2 (ACE2) receptor (2), which is highly expressed in the thyroid tissue (3), the thyroid has been considered a potential direct target of the viral infection (4). Alternatively, SARS-CoV-2 might indirectly induce thyroid gland inflammation through triggering abnormal immune-inflammatory responses and cytokine storm (4).
Subacute thyroiditis (SAT) has been reported in COVID-19 patients (5 –8). The SAT is defined as an inflammatory disorder of the thyroid gland, likely originating from a viral infection, characterized by self-limiting thyrotoxicosis followed by hypothyroidism with variable duration, before resumption to normal thyroid function (9). In general, permanent hypothyroidism has been observed in 15% patients with SAT after a 28-year follow-up (10). Moreover, autoimmune thyroid disease (AITD), including Graves' disease (11) and Hashimoto thyroiditis (12), have been reported after a diagnosis of SAT. It remains unclear whether SARS-CoV-2 induced SAT would induce long-term thyroid dysfunction. Case reports and cohort studies revealed that patients with COVID-19 experienced thyroid dysfunction, including AITD (7,13 –16), thyrotoxicosis (8,15,17,18), hypothyroidism (5,8,15,17 –19), and nonthyroidal illness syndrome (14,15,19). Nevertheless, the cohort studies to date were limited by small sample sizes with short follow-up periods, and they could not infer causality. Whether SARS-CoV-2 infection or COVID-19 severity would cause long-term thyroid dysfunction warrants further investigation.
In the reverse direction, a meta-analysis (20) and three retrospective studies (21 –23) provided contradictory evidence for the association of pre-existing thyroid disease with risk of COVID-19-related outcomes. It remains unknown whether thyroid dysfunction alters the susceptibility to SARS-CoV-2 infection and COVID-19 severity.
Mendelian randomization (MR) analysis makes use of genetic variants as instruments to represent the exposure, aiming at examining the causal association of the exposure with the lifelong risk of the outcome (24). In this two-sample MR study, we evaluate the bi-directional causal relationship of host genetic liability to three COVID-19 phenotypes (including SARS-CoV-2 infection, hospitalized COVID-19, and severe COVID-19) with three binary thyroid dysfunction traits (including hyperthyroidism, hypothyroidism, and AITD), and three continuous thyroid hormone level traits (including thyrotropin [TSH] and free thyroxine [fT4] within reference range, and TSH in full range).
Materials and Methods
Study design
This is a two-sample bi-directional MR study assessing the causal relationship of host genetic liability to COVID-19 phenotypes with thyroid-related traits. The study design and assumptions of MR analysis are illustrated in Figure 1. In the forward direction with COVID-19 phenotypes as exposure and thyroid-related traits as outcome, we determined whether host genetic liability to COVID-19 phenotypes had causal effects on the thyroid traits. In the reverse direction, we assessed whether genetically determined thyroid traits are causally associated with COVID-19 phenotypes.
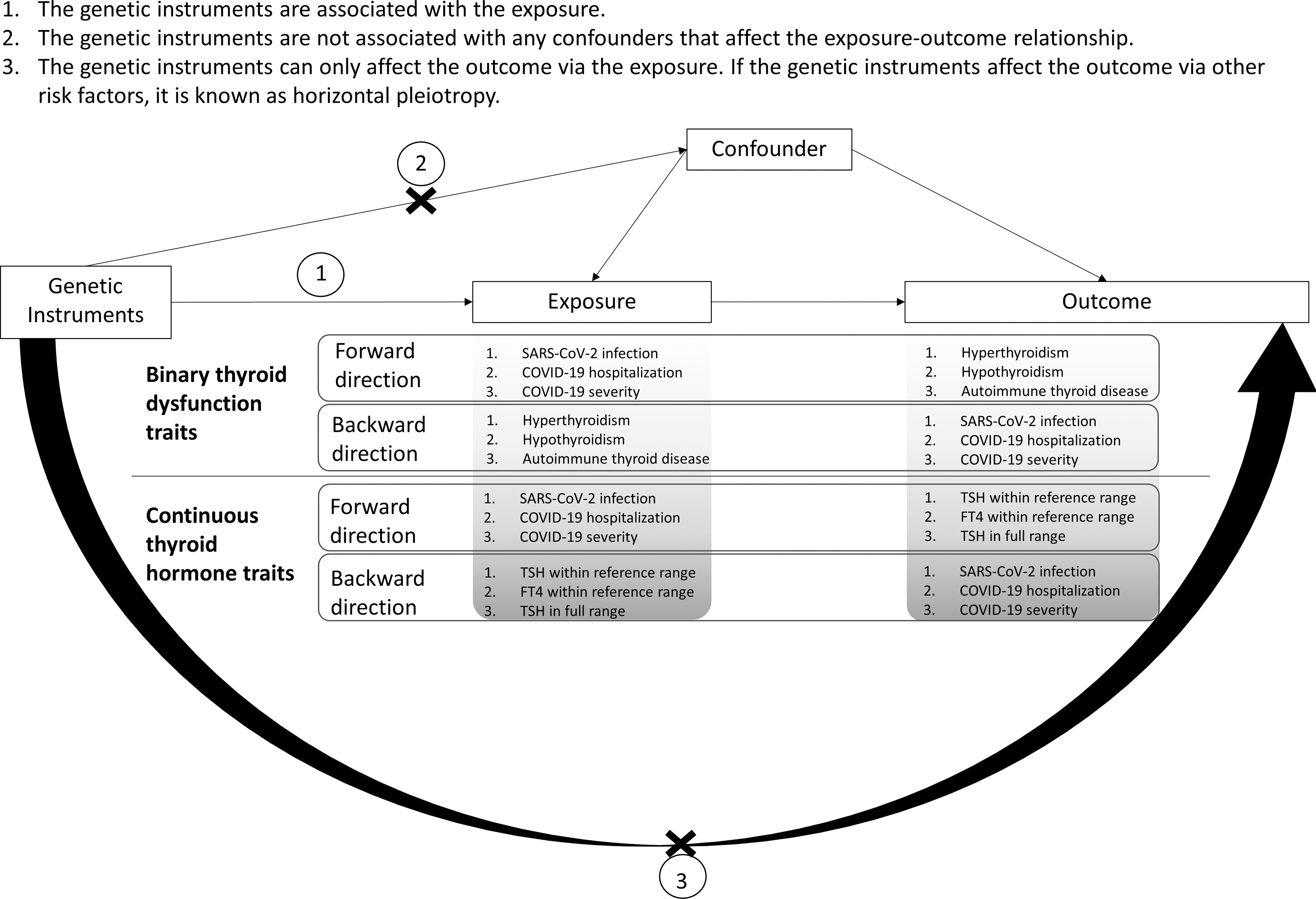
Study design and assumptions of Mendelian Randomization.
Data sources and genetic instruments
The largest possible meta-analyses of genome-wide association studies (GWAS), which were conducted in Europeans, were selected as the data sources (Supplementary Methods S1). The details of each data source, including the eligibility criteria of study participants, sample size, ancestry, and analytical procedures, are presented in Table 1. Ethics approval of all the relevant GWAS was obtained from the respective institutional review boards, and additional ethics review was not required for this MR study using previously reported data. The protocol for selection of genetic instruments is detailed in Supplementary Methods S2.
Data Sources Used in Mendelian Randomization Analysis
COVID-19, coronavirus disease; fT4, free thyroxine; GWAS, genome-wide association studies; MGI, Michigan Genomics Initiative; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SNPs, single nucleotide polymorphisms; TSH, thyrotropin.
In the forward direction, independent single nucleotide polymorphisms with suggestive significance(p < 5 × 10−6) were selected as the initial genetic instruments for the three COVID-19 phenotypes in the primary MR analysis. If a significant causal relationship was revealed in the primary analysis, sensitivity analysis using instruments with a more stringent threshold at genome-wide significance (p < 5 × 10−8) was performed. The F-statistics, a measure of the strength of genetic instruments, were computed for each MR analysis. Together with the number of genetic instruments adopted in each MR analysis, these figures are listed in Table 2. Methods of calculating power (Supplementary Figs. S1 and S2) and bias (Supplementary Table S1) due to sample overlap are detailed in Supplementary Methods S3.
Summary of Genetic Instruments Adopted in the Mendelian Randomization Analyses
Number of genetic instruments adopted in MR analysis = Total number of independent genetic variants identified in GWAS of exposure − number of genetic variants excluded due to lack of proxies − number of outliers identified by MR-PRESSO.
MR, Mendelian randomization; MR-PRESSO, MR pleiotropy residual sum and outlier.
Mendelian randomization
The main MR analysis was the conventional inverse-variance weighted (IVW) method (25), with the random-effects model selected to address heterogeneity that was assessed using the Cochran's Q test. Sensitivity analyses included weighted median (26), MR-Egger regression (27), contamination mixture (28) methods, and the outlier test of MR pleiotropy residual sum and outlier (MR-PRESSO) (29) method. To check for the presence of directional pleiotropy, we applied the MR-Egger intercept (27) and MR-PRESSO global (29) tests. If pleiotropic outliers were identified by MR-PRESSO, the main and sensitivity analyses were repeated on exclusion of the outliers. Details of these MR methods are described in Supplementary Methods S4. Conservative Bonferroni correction for 36 tests (α = 0.05/36 = 1.39 × 10−3) was used to account for multiple testing.
Results
MR in evaluating the causal effects of host genetic liability to COVID-19 phenotypes on thyroid-related traits (forward direction)
In the primary analyses, we identified 19, 28, and 40 genetic instruments at p < 5 × 10−6 for SARS-CoV-2 infection (Supplementary Table S2a), hospitalized COVID-19 (Supplementary Table S2b), and severe COVID-19 (Supplementary Table S2c), respectively. Genetic liability to SARS-CoV-2 infection was associated with an increased risk of hypothyroidism in the main IVW analysis after correction for multiple testing (per doubling in prevalence of SARS-CoV-2 infection, odds ratio [OR] = 1.335; 95% confidence interval [CI]:1.167–1.526; Fig. 2a). Similar causal estimates were obtained from sensitivity analyses of weighted median method (OR = 1.296; CI: 1.066–1.575), contamination mixture method (OR = 1.356; CI: 1.095–1.818), MR-Egger regression (OR = 1.712; CI: 1.202–2.439), and MR-PRESSO (OR = 1.335; CI: 1.156–1.542; Fig. 2a). Leave-one-out analysis confirmed that the causal association was not driven by any individual instrument (Supplementary Fig. S3).
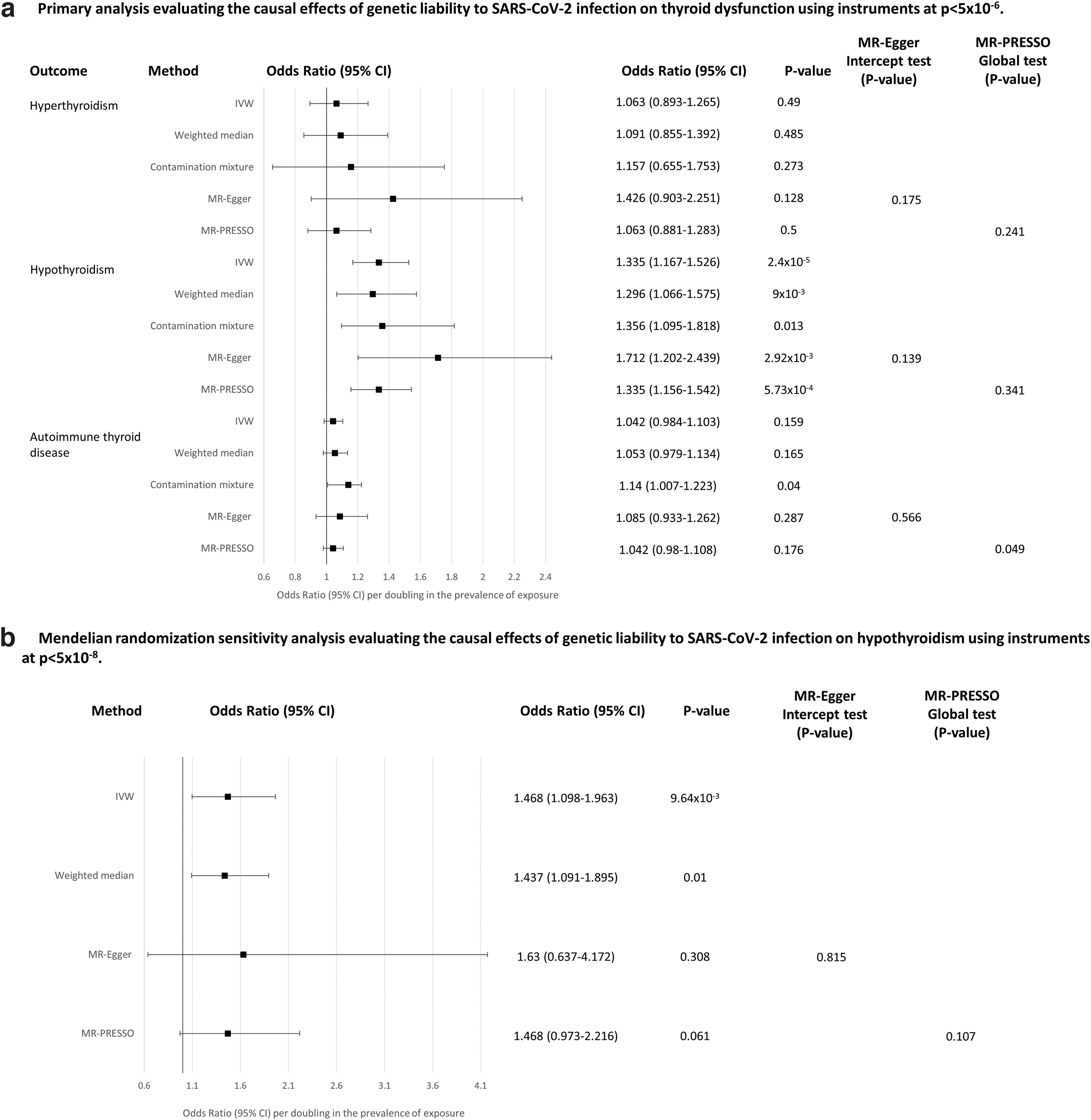
Mendelian randomization analysis evaluating the causal effects of host genetic liability to SARS-CoV-2 infection on thyroid dysfunction. (
In the sensitivity analysis using five independent instruments at p < 5 × 10−8 (Supplementary Table S2d), a similar causal association was observed for the IVW (OR = 1.468; CI: 1.098–1.963) and weighted median methods (OR = 1.437; CI: 1.091–1.895), while wider CIs crossing the null were observed for other sensitivity analyses (Fig. 2b). No association was observed for genetic liability to SARS-CoV-2 infection with hyperthyroidism and AITD (Fig. 2a), as well as the three thyroid hormone level traits (Supplementary Fig. S4). MR-Egger intercept and MR-PRESSO global tests were not statistically significant (Fig. 2a, b and Supplementary Fig. S4).
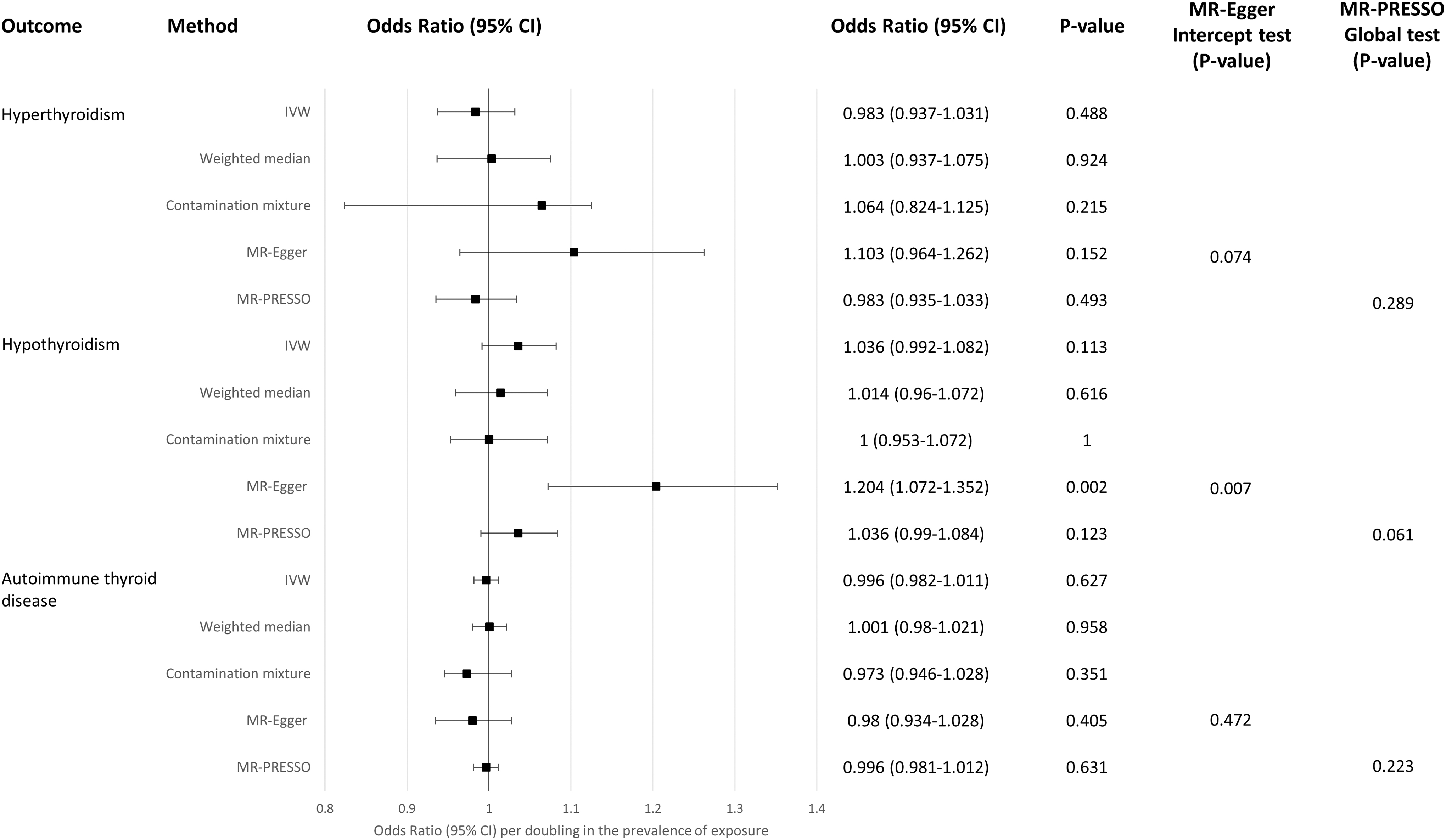
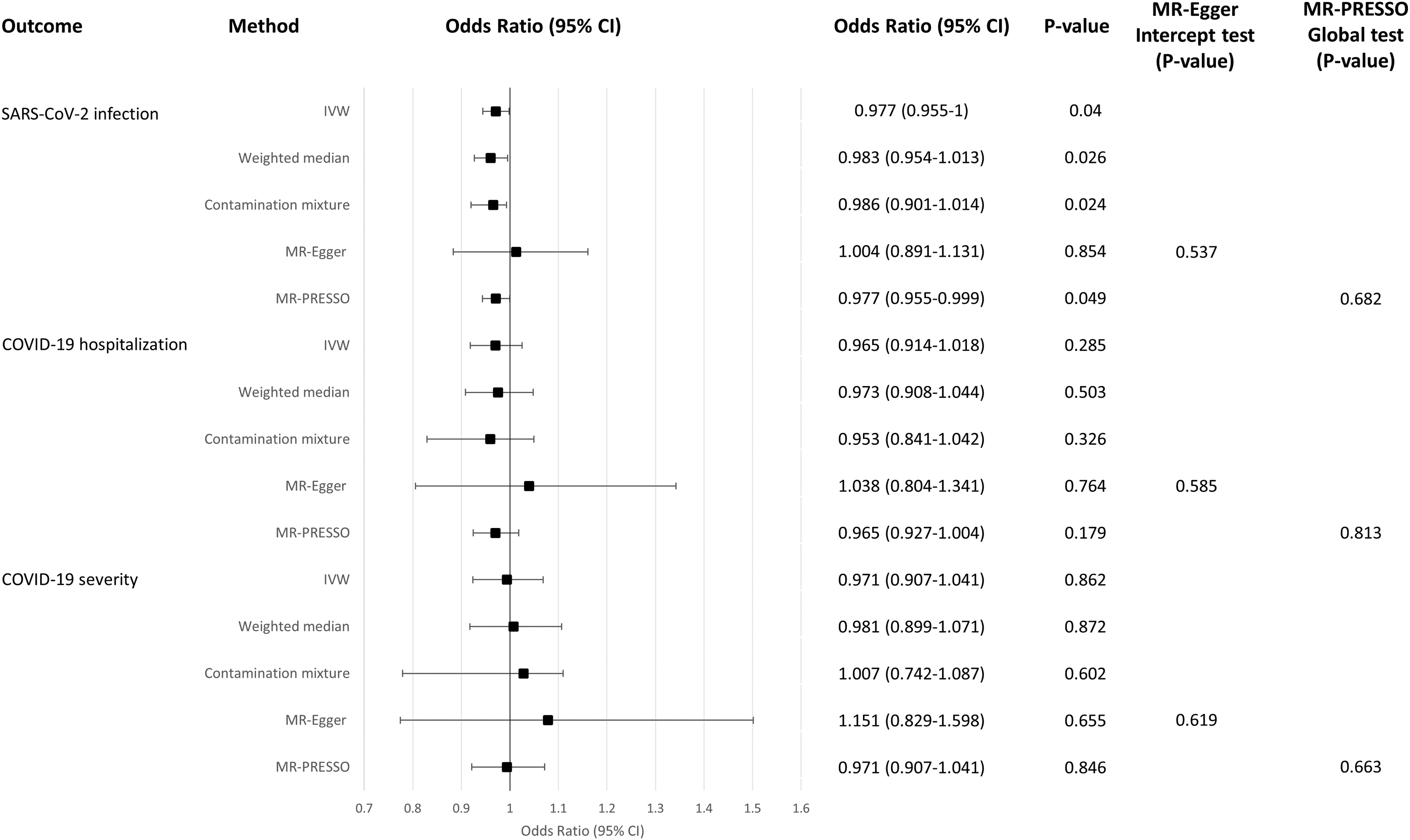
We observed null causal effects of genetic liability to COVID-19 hospitalization (Fig. 3 and Supplementary Fig. S5) and severe COVID-19 infection (Fig. 4 and Supplementary Fig. S6) on all thyroid traits examined, as reflected by all the main IVW analyses. Although nominal significance was obtained in MR-Egger regression and/or contamination mixture methods for the causal association of genetic liability to hospitalized COVID-19 with increased risk of hyperthyroidism and hypothyroidism (Fig. 3), and genetic liability to severe COVID-19 with increased risk of hypothyroidism (Fig. 4), lower TSH level (within reference range), and higher TSH level (in full range) (Supplementary Fig. S6), the MR-Egger intercept tests were significant. Despite the insignificant MR-PRESSO global tests (Figs. 3 and 4 and Supplementary Fig. S6), the possibility of horizontal pleiotropy could not be ruled out unequivocally.

Mendelian randomization analysis evaluating the causal effects of genetic liability to COVID-19 hospitalization on thyroid dysfunction. COVID-19, coronavirus disease.
Mendelian randomization analysis evaluating the causal effects of genetic liability to COVID-19 severity on thyroid dysfunction.
MR analyses in evaluating the causal association of genetically determined thyroid-related traits with COVID-19 phenotypes (reverse direction)
In the main IVW analyses, there was no evidence to support that genetic predisposition to hyperthyroidism (Fig. 5), hypothyroidism (Fig. 6), and AITD (Fig. 7) had causal effects on any COVID-19 phenotypes. Although nominal significance was obtained for genetically susceptibility to hyperthyroidism with reduced risk of SARS-CoV-2 infection, the multiple testing threshold was not surpassed (Fig. 5). Genetically determined TSH and fT4 levels within reference range (Supplementary Figs. S7 and S8), and TSH level in full range (Supplementary Fig. S9), also had null association with the COVID-19 phenotypes in the main IVW analyses.
Mendelian randomization analysis evaluating the causal effects of genetic predisposition to hyperthyroidism on COVID-19 phenotypes.
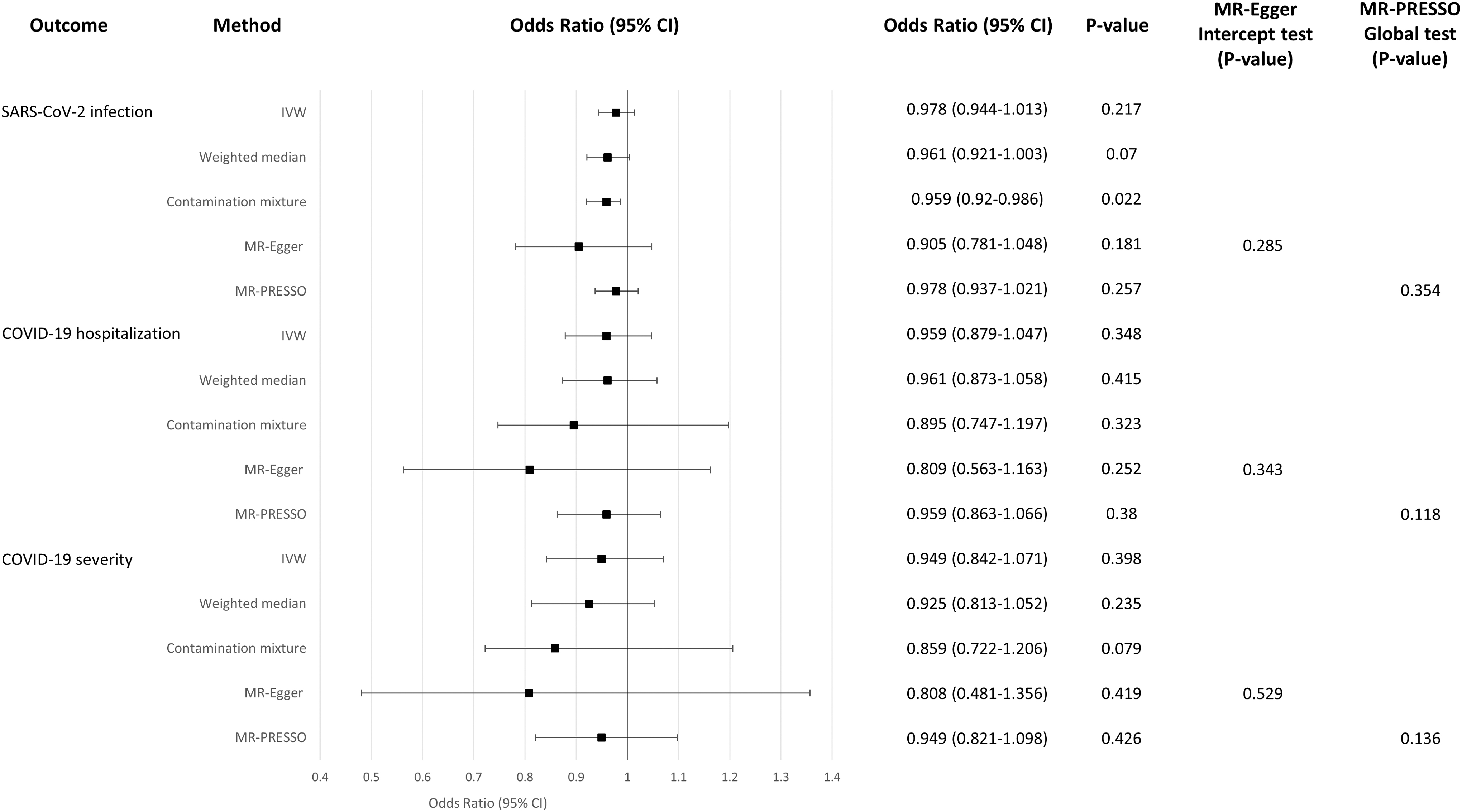
Mendelian randomization analysis evaluating the causal effects of genetic predisposition to hypothyroidism on COVID-19 phenotypes.
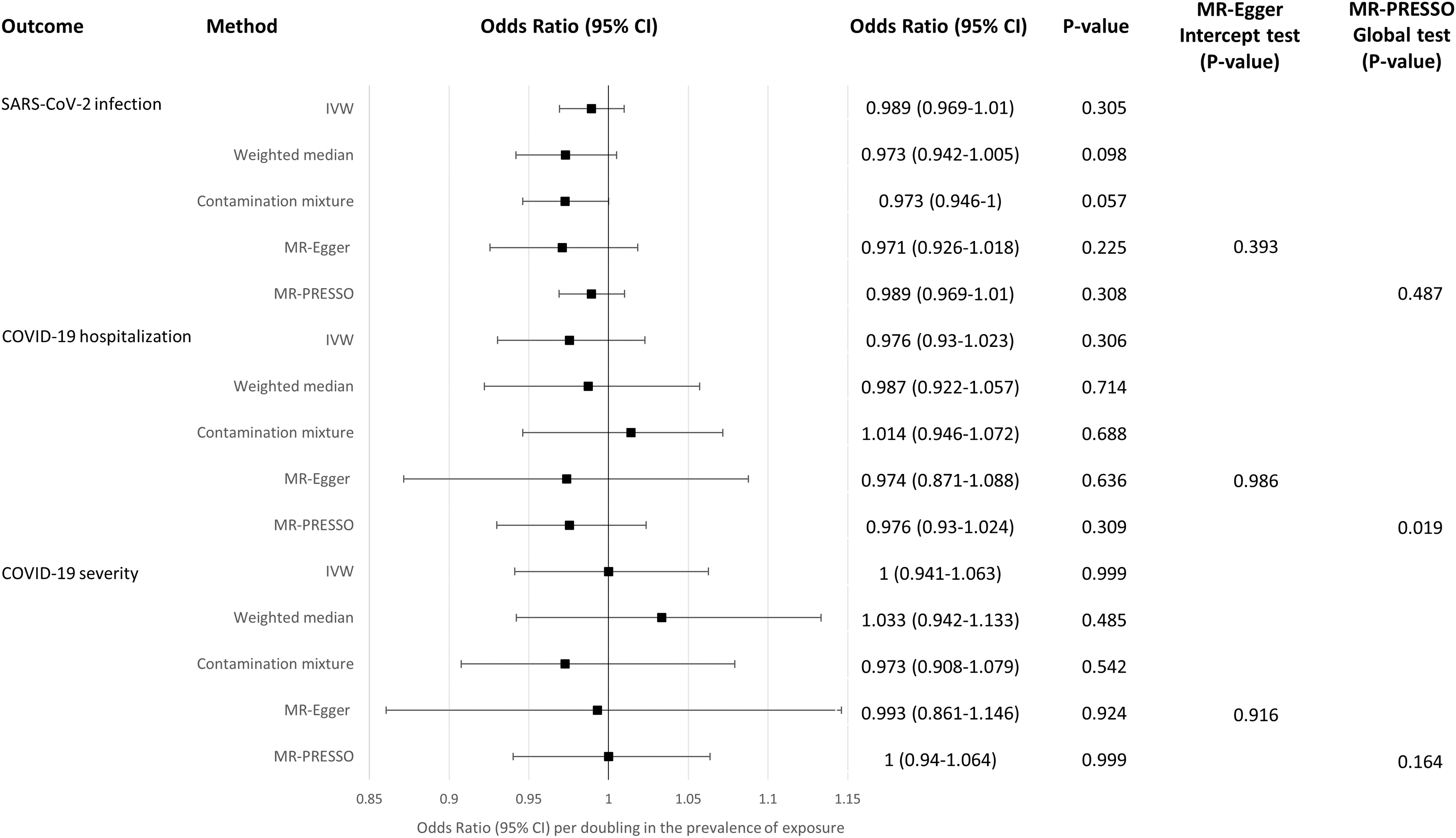
Mendelian randomization analysis evaluating the causal effects of genetic predisposition to autoimmune thyroid disease on COVID-19 phenotypes.
Majority of the MR analyses were not subjected to directional pleiotropy, with insignificant MR-Egger intercept and MR-PRESSO global tests. Exceptions were seen for the MR analysis of AITD with COVID-19 hospitalization (Fig. 7), TSH level within reference range with SARS-CoV-2 infection and COVID-19 hospitalization (Supplementary Fig. S7), and TSH in full range with hospitalization (Supplementary Fig. S9) that the MR-Egger intercept and/or MR-PRESSO global tests were significant, even though no significant pleiotropic outliers were identified. We also observed heterogeneity in these four analyses (Cochrane's Q test heterogeneity p < 0.05), but not for others (Supplementary Table S3).
Discussion
To our knowledge, this is the first MR study evaluating the casual relationship between host genetic liability to COVID-19 phenotypes and thyroid-related traits. In this bi-directional two-sample MR study, we observed that genetic susceptibility to SARS-CoV-2 infection was associated with increased risk of hypothyroidism. In the reverse direction, we found no evidence that genetic predisposition to thyroid-related traits would alter the susceptibility to SARS-CoV-2 infection, COVID-19 hospitalization, or severity.
Our primary analysis using genetic instruments at p < 5 × 10−6 provided strong evidence supporting that genetic susceptibility to SARS-CoV-2 infection, or host response to the viral infection, increased the risk of hypothyroidism. Assuming the incidence rate of hypothyroidism among individuals without SARS-CoV-2 infection was similar to that in the European population before the pandemic [226.2 per 100,000 person-year (30)], the absolute risk difference of hypothyroidism between individuals with and without infection is estimated to be 75.8 incident cases per 100,000 person-year per doubling the prevalence of SARS-CoV-2 infection.
Consistent and robust causal estimates were attained in the sensitivity analyses using instruments with p < 5 × 10−8. Notably, in the original GWAS meta-analysis, hypothyroidism was defined as TSH level above the reference range such that both overt and mild subclinical hypothyroidism was included (31). Therefore, our MR findings implied that the risk of both overt and subclinical hypothyroidism might be elevated in individuals who were genetically susceptible to SARS-CoV-2 infection, which was consistent with previous studies that SARS-CoV-2-infected patients experienced subclinical (5,15,19) or overt hypothyroidism (17) up to 108 days after hospital admission (19).
Given that most of the participants (>80%) in these studies had a mild course of COVID-19 infection treated outside the intensive care unit (ICU) (5,15,17,19), these observations aligned with our findings in SARS-CoV-2 infected individuals. One possible explanation for the development of hypothyroidism in individuals with SARS-CoV-2 infection is the development of SAT, which is prevalent among COVID-19 patients (5 –8). Permanent hypothyroidism was observed in ∼15% of individuals with SAT at the 28-year follow-up (10). Nevertheless, only low prevalence rates of hypothyroidism (≤5.2%) have been observed among prospective studies of COVID-19 patients to date (17,18), which may be attributed to a short follow-up period (≤108 days). Notably, SARS-CoV-2 infection might cause symptoms even after the infection was resolved, which is known as long COVID. Symptoms may include fatigue (32), cognitive problems (i.e., memory and concentration) (33), and mood problems (e.g., depression and anxiety) (34). Further, fatigue is commonly observed among hypothyroid patients, and hypothyroidism is associated with increased risk of cognitive impairment (35) and depression (36,37). Taking together our MR findings suggesting that genetic liability to SARS-CoV-2 infection might increase the risk of hypothyroidism, future investigation in long-term cohort studies examining thyroid function and long covid are warranted.
Genetic susceptibility to SARS-CoV-2 infection was causally associated with increased risk of hypothyroidism, but not other thyroid-related traits. Although AITD cases included a substantial proportion of individuals with subclinical and overt hypothyroidism, a null association was observed for host genetic liability to SARS-CoV-2 infection with AITD in our MR study. One plausible reason was the different selection criteria of cases. Although the GWAS meta-analysis of hypothyroidism (31) selected cases as those with TSH level above the reference range irrespective of the causes, the GWAS meta-analysis of AITD specifically excluded hypothyroidism cases with non-autoimmune causes (38). Another reason might be due to the dilution effects by including individuals with Graves' disease and Hashimoto thyroiditis as AITD (38). We also found that genetic liability to SARS-CoV-2 infection had null causal effects on the continuous traits of TSH levels. The TSH within reference range included euthyroid individuals only (31), while the TSH in full range included patients with euthyroidism, hyperthyroidism, or hypothyroidism. Notably, our MR study suggested a link of genetic liability to SARS-CoV-2 infection with risk of hypothyroidism, but not hyperthyroidism. The different study participants included in the MR analysis of hypothyroidism and TSH might explain why discrepant results were observed.
There was insufficient evidence to suggest any causal association of genetic liability to hospitalized and severe COVID-19 with hypothyroidism. One plausible explanation is that different host response mechanisms exist in affecting the susceptibility to SARS-CoV-2 infection and progression to more severe COVID-19. Based on the GWAS meta-analysis conducted by COVID-19 Host Genetics Initiative (HGI), only 4 out of 13 genome-wide significant loci identified for the 3 COVID-19 phenotypes were shared between SARS-CoV-2 infection and hospitalized COVID-19 (39). In addition, these four loci had stronger links to SARS-CoV-2 infection than progression to severe COVID-19 (39). The presence of causal association with hypothyroidism for individuals genetically susceptible to SARS-CoV-2 infection does not necessarily imply that the same causal association exists for those liable to hospitalized or severe COVID-19. Even though such causal association exists, the genuine causal effect on hypothyroidism might be too small to be detected (Supplementary Fig. S1a–c). To detect a causal association with small effect, the MR analyses might be re-visited when summary statistics from better-powered GWAS of hypothyroidism, hospitalized, and severe COVID-19 become available.
There was insufficient evidence to suggest a causal association of SARS-CoV-2 infection with hyperthyroidism, but this should be interpreted with caution. The statistical power in evaluating this association was the lowest among all other analyses in the current study, as the proportion of variance explained by the genetic instruments on SARS-CoV-2 infection was small (<1%) and the outcome dataset was of medium sample size only. We had 80% power to detect a genuine causal association if hyperthyroidism had an OR ≥2.4 per standard deviation increase in the exposure (Supplementary Fig. S1a). Therefore, the MR analysis investigating the causal relationship of SARS-CoV-2 infection with hyperthyroidism should be re-visited when genetic instruments explaining higher proportion of variance on SARS-CoV-2 infection, or a higher-powered GWAS of hyperthyroidism, become available.
We saw no significant causal association of genetically determined thyroid-related traits with COVID-19 phenotypes. This finding is consistent with three retrospective studies that reported that pre-existing hyperthyroidism (21) and hypothyroidism (21 –23) were not associated with increased risk of SARS-CoV-2 infection, COVID-19-associated hospitalization, ICU admission, and mortality. Although a meta-analysis suggested that individuals with pre-existing thyroid abnormalities and hypothyroidism had poorer COVID-19-related outcomes in terms of severity, ICU admission, hospitalization, and mortality (20), the discrepancy might be explained by the different study designs, sample size, and unavailability of covariates in some of the included studies. Importantly, our findings support the current assumption that patients with AITD are unlikely more susceptible to SARS-CoV-2 infection or more severe COVID-19 (40).
This study has several clinical implications. It has been suggested that SARS-CoV-2 might directly infect the thyroid gland, indirectly cause inflammation of the thyroid via triggering abnormal immune-inflammatory responses, or both (4,19). Our study findings support that host response to SARS-CoV-2 infection might increase the risk of overt and subclinical hypothyroidism. It may be beneficial if clinicians are aware of the possible occurrence of overt or subclinical hypothyroidism among individuals who are genetically susceptible to SARS-CoV-2 infection. Appropriate prevention, monitoring the thyroid function for individuals with previous infection of SARS-CoV-2, and thus timely treatment, might mitigate the risk of undiagnosed symptomatic hypothyroidism. However, whether physiological changes caused by SARS-CoV-2 infection altered the risk of hypothyroidism requires future investigation.
Our study has several strengths. We investigated the causal relationship between two diseases using the MR approach, which is infeasible to be assessed by the randomized clinical trials. Moreover, the MR approach enables the evaluation of lifelong effect of the exposure on the outcome. In our study, relatively high F-statistics were observed for the instruments (Table 2), indicating that weak instrument bias is unlikely. We adopted different MR methods that are based on different assumptions. However, similar causal estimates were attained for the causal association of host genetic liability to SARS-CoV-2 infection with hypothyroidism, demonstrating the robustness of the finding.
There are also limitations. First, bias might arise due to participant overlap in two-sample MR analysis (41), which was present in the exposure-outcome pairs of AITD-COVID19-hospitalization (17.62%), hyperthyroidism-SARS-CoV-2-infection (0.331%), hypothyroidism-SARS-CoV-2-infection (0.331%), TSH within reference range-SARS-CoV-2 infection (0.636%), fT4-SARS-CoV-2 infection (0.331%), and TSH in full range-SARS-CoV-2 infection (1.4%). The bias and Type I error were 0 and 0.05, respectively for all the overlapping pairs (Supplementary Table S1), which is considered minimal. Second, SARS-CoV-2 infection can be asymptomatic, contributing to under-diagnosis of COVID-19, subsequently leading to misclassification of the SARS-CoV-2 infection status in the GWAS meta-analysis of SARS-CoV-2 infection conducted by COVID-19 HGI. Hence, the power of the GWAS meta-analysis and our MR study were reduced. As aforementioned, the statistical power for the MR analysis assessing the causal association of genetic susceptibility to SARS-CoV-2 infection with hyperthyroidism was particularly low. Nevertheless, the current study had sufficient power for the remaining MR analyses that suggested null association, indicating that even if a causal association exists, the causal effect on the outcome may not be clinically meaningful. Third, the GWAS meta-analysis of hyperthyroidism and hypothyroidism conducted by ThyroidOmics Consortium (31) did not differentiate the overt and subclinical cases. Thus, we cannot provide the risk estimates and absolute risks that genetic susceptibility to SARS-CoV-2 infection had on overt and subclinical hypothyroidism, respectively. Fourth, this MR study utilized summary statistics derived from GWAS meta-analyses conducted in Europeans. Whether the findings could be generalized to other ethnicities warrant future investigations. Fifth, genetic instruments might act on the outcome via pathways other than the exposure, violating the third MR assumption (Fig. 1). However, we have adopted the MR-Egger intercept and MR-PRESSO global tests to detect the presence of directional pleiotropy. For the association of SARS-CoV-2 infection with hypothyroidism, both tests were insignificant, implying that horizontal pleiotropy was unlikely, although the possibility cannot be completely excluded.
In conclusion, this study revealed that genetic susceptibility to SARS-CoV-2 infection is causally associated with an increased risk of hypothyroidism. The MR approach using instruments of host genetics supports that host response to viral infection plays a role in this causal relationship.
Data and Data Sharing
The present MR study uses publicly available summary statistics from GWAS/GWAS meta-analysis that can be downloaded from the websites of the corresponding consortiums. The references of these GWAS/GWAS meta-analysis are provided in Table 1.
Footnotes
Authors' Contributions
G.H.-Y.L. and C.-L.C. conceptualized and designed the study. G.H.-Y.L. and C.-M.T. conducted the statistical analysis. G.H.-Y.L. drafted the article. All authors were involved in interpreting the data and revising the article for final submission.
Acknowledgments
The authors would like to express their gratitude to all study participants of the respective GWAS from which the summary statistics of this MR study were obtained.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
The work was supported by the Start-up Fund for Research Assistant Professors under the Strategic Hiring Scheme of The Hong Kong Polytechnic University, granted to G.H.-Y.L. (P0036047).
Supplementary Material
Supplementary Methods S1
Supplementary Methods S2
Supplementary Methods S3
Supplementary Methods S4
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9