
Abstract
Background:
Physical activity is a protective factor against several types of cancers. However, evidence for the association between physical activity and thyroid cancer (TC) is still inconclusive.
Methods:
We used prospectively collected data from the Korea National Cancer Screenee Cohort, which consisted of 30,435 participants from 20 years who received health examinations at National Cancer Center between June 2007 and December 2014. Participants' follow-up data up to December 2019 was used to identify new TC cases. Demographic characteristics of the subjects were collected using a self-administered questionnaire. Physical activity measurement was analyzed from 15,175 participants using International Physical Activity Questionnaire—Short Form. Physical activity data included frequency (days per week) and duration (minutes per day) of their exercises in three intensity levels (walking, moderate, and vigorous-intensity). The association between physical activity levels and TC risk was examined by Cox proportional hazards regression models.
Results:
We identified 234 new TC cases among 15,175 eligible participants during the follow-up period. Participants with the highest physical activity level had a reduced risk of TC (hazard ratio [HR] = 0.65 [confidence interval, CI = 0.44–0.94], p-trend = 0.028) than participants with the lowest physical activity level. The significant associations were stronger among female subjects with a body mass index ≥25 kg/m2 (HR = 0.38 [CI = 0.16–0.93], p-trend = 0.034), subjects with household income >4 million won/month (HR = 0.53 [CI = 0.30–0.94], p-trend = 0.034), subjects without a first-degree family history of TC (HR = 0.66 [CI = 0.45–0.96], p-trend = 0.040), and subjects who did not drink alcohol (HR = 0.48 [CI = 0.26–0.88], p-trend = 0.018) or smoke (HR = 0.61 [CI = 0.40–0.95], p-trend = 0.030).
Conclusion:
This prospective Korean cohort study suggests that increased physical activity may be protective for development of TC. These findings require confirmation in other populations.
Introduction
In 2020
To date, the cause of TC is poorly understood. The only substantial evidence is that childhood exposure to ionizing radiation is a risk factor for TC, 3 although overweight, obesity, and radiation exposure may play roles in increasing its risk. 4 In contrast, the consumption of vegetables and fruits may protect against the development of TC, 5 and the consumption of iodine-rich food such as fish or shellfish might reduce TC risk in populations with iodine insufficiency. 6,7 However, the association between physical activity and TC remains controversial.
The World Cancer Research Fund/American Institute for Cancer Research report defines physical activity as any movement using skeletal muscles and requiring more energy than resting. 8 Physical activity may affect several systems in the human body, including endocrinologic, immunologic, and metabolic processes, and is related to the risk of cancer development. 8 Recently, solid and consistent evidence has supported the protective role of increased physical activity in the progression of several types of cancer (esophageal adenocarcinoma, gastric cardia, colon, breast, endometrial, and bladder cancers). 9 While physical activity is reported that it has inversely associated with TC risk, 10,11 some studies have revealed a positive correlation 12 or a nonsignificant relationship between physical activity and TC. 13 –15
Our aim was to determine the association between quantity of physical activity and the development of TC in a Korean population using prospectively collected cohort data.
Materials and Methods
Study population
The eligible participants in our study were properly selected from the Cancer Screenee Cohort at Korean National Cancer Center (KNCC). Details of the cohort were described elsewhere. 16 Briefly, the cohort data included 30,435 participants from 20 years of age who underwent evaluation of their health status at the Center for Cancer Prevention and Detection of the KNCC from June 2007 to December 2014. Data were included from participants who completed the baseline questionnaires and were followed until December 2019 for a new diagnosis of TC. The exclusion criteria were subjects with incomplete questionnaire data and those with a previous cancer diagnosis of any type. We selected 15,175 participants with available self-reported physical activity data, including the frequency (days per week) and duration (minutes per day) of their exercises in three intensity levels (walking, moderate, and vigorous) (Fig. 1). Written informed consent was obtained from all participants, and the study protocol was approved by the Institutional Review Board of the KNCC (No. NCCNCS-07-077).
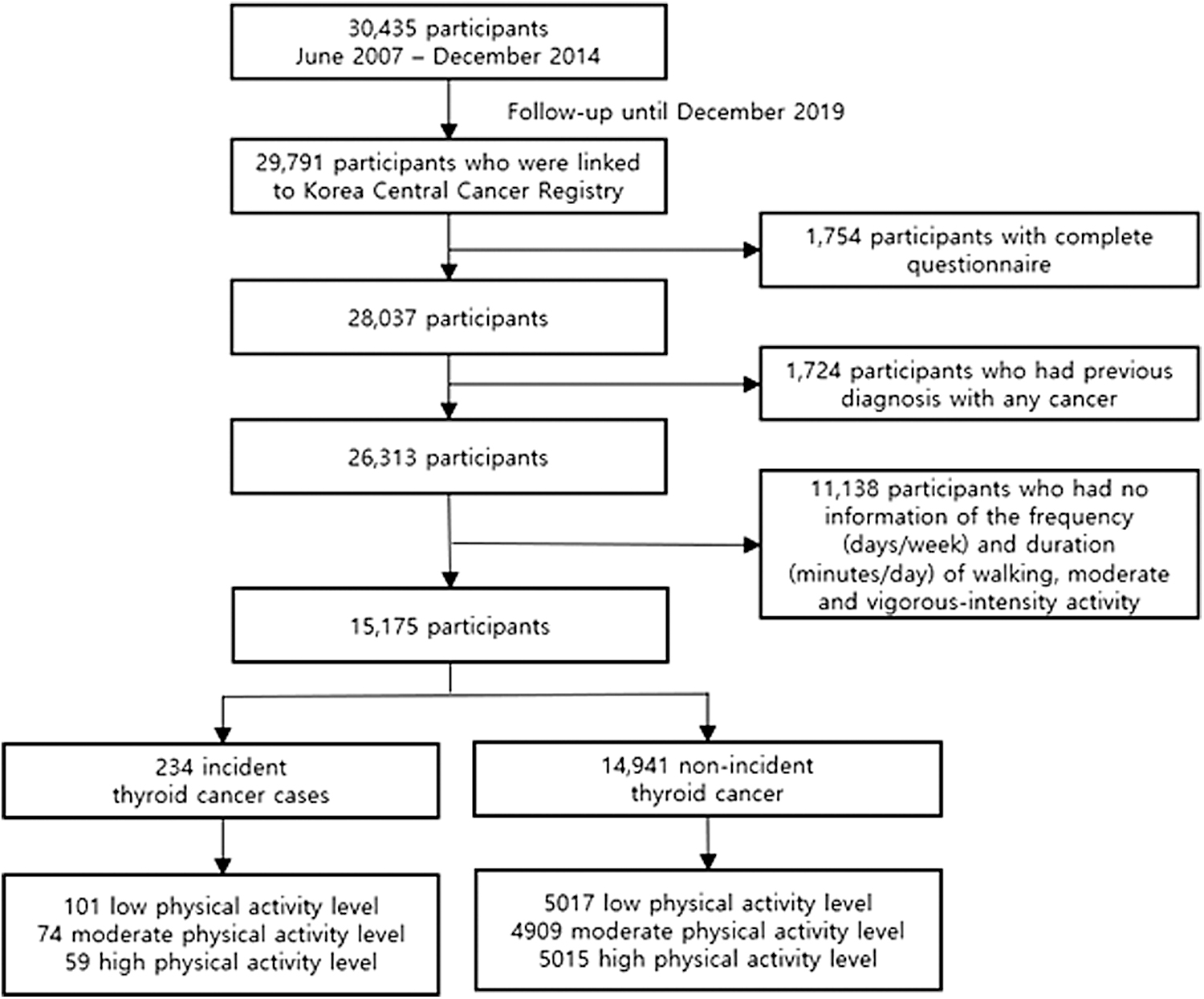
Flowchart of collecting participants in the cohort study.
TC incidence was determined through linkage with the 2019 Korea National Cancer Incidence Database of the Korea Central Cancer Registry. Most patients were ultimately diagnosed with TC through a biopsy procedure. The International Statistical Classification of Disease and Related Health Problems 10th revision (ICD-10) (C73), was considered the criterion to identify TC cases in the KCCR database. Patients diagnosed with primary TC after enrollment were identified as incident cases.
Data collection
Demographic information of the study participants was extracted from the Cancer Screenee Cohort of the KNCC, including sex, age, body mass index (BMI; kg/m2; <18.5, 18.5 to <25, ≥25), education level (high school or less, college or higher), monthly household income (10,000 won/month; <200, 200–400, and >400), marital status (married or cohabitating, others), first-degree family history of thyroid cancer (FHTC; yes, no), alcohol consumption (nondrinkers, former drinkers, and current drinkers), and smoking status (nonsmokers, former smokers, and current smokers).
For the purpose of our study, we used the International Physical Activity Questionnaire—Short Form (IPAQ-SF) to measure levels of physical activity of eligible subjects. 17 This questionnaire was previously validated across 12 countries. 18 The frequency (days per week) and duration (minutes per day) of walking, moderate- and vigorous-intensity physical activity were extracted. For extreme exercise durations, we recoded durations <10 minutes/day as 0 and truncated durations >180 minutes/day as 180. The metabolic equivalent of task (MET) minutes per week in each type of physical activity were estimated by multiplying the weekly minutes engaged (frequency × duration) by the average MET score of an activity (3.3 for walking, 4.0 for moderate-intensity, and 8.0 for vigorous-intensity activity). We summed these MET minutes per week to obtain the total MET minutes per week. We categorized physical activity levels of the study population into three groups (“low,” “moderate,” and “high”) according to tertiles of their weekly total MET minutes.
We also measured sedentary behavior separately, which was computed as weekly minutes of sitting. Similar to the physical activity levels, sitting behavior was categorized into tertiles.
Statistical analyses
Demographic characteristics of the cohort participants were compared between three physical activity groups by performing analyses of variance tests for continuous variables and chi-square tests for categorical variables. The person-year of each subject was determined when they completed our baseline questionnaire to the date they were diagnosed with cancer, died, or ended the follow-up (December 31, 2019), whichever occurred first. We utilized a Cox proportional hazards regression model to evaluate the association between physical activity levels and TC occurrence. Multivariable models were adjusted for potential confounders such as age, sex, BMI, education level, monthly household income, marital status, FHTC, alcohol consumption, and smoking status. All statistical analysis processes were implemented in SAS software (version 9.4; SAS Institute, Cary, NC), and the statistical significance was set as a two-sided p-value <0.05.
Results
Out of 15,175 subjects, we identified 234 TC cases (Fig. 1). The median duration of follow-up was 9.5 years with interquartile range being 4.1 years, and the total person-years followed was 140,844.45. Table 1 shows the demographic characteristics of the study participants. Among the subjects, 5118 reported a low physical activity level, 4983 exercised at a moderate level, and 5074 exercised at a high level. Compared with participants with the lowest physical activity level, participants with higher levels were older (50.4 ± 9.0 vs. 51.6 ± 9.0 and 52.5 ± 8.6 years, p < 0.001), more likely to be current alcohol drinkers (52.8% vs. 54.9% and 59.7%, p < 0.001), and spent more time walking (75.5 ± 71.2 vs. 273.3 ± 171.8 and 585.8 ± 391.0 minutes/week, p < 0.001), as well as participating in moderate- (6.0 ± 21.2 vs. 76.5 ± 109.9 and 306.7 ± 325.4 minutes/week, p < 0.001) and vigorous-intensity activities (1.4 ± 7.8 vs. 38.8 ± 65.2 and 278.7 ± 293.2 minutes/week, p < 0.001).
Baseline Characteristics of the Study Participants by International Physical Activity Questionnaire Physical Activity Continuous Score
Bold values are significance at p < 0.05.
Chi-square test and ANOVA test were used for categorical variables and continuous variables, respectively.
ANOVA, analysis of variance; BMI, body mass index; IPAQ, International Physical Activity Questionnaire; IQR, interquartile range; MET, metabolic equivalent of task; PA, physical activity; SD, standard deviation.
Participants with higher physical activity levels also included a lower proportion of current smokers than those with the lowest physical activity level (14.9% and 15.6% vs. 18.8%, p < 0.001). Moreover, compared with subjects reporting lower physical activity levels, the most active individuals had a higher BMI (23.7 ± 3.1 and 23.6 ± 3.0 vs. 23.9 ± 2.8 kg/m2, p < 0.001), lower education level (45.3% and 51.7% vs. 43.3%, p < 0.001), and spent less time sitting per week (2786.9 ± 1561.5 and 2564.3 ± 1411.2 vs. 2192.0 ± 1303.8 minutes/week, p < 0.001).
The relationship between physical activity level and TC incidence is shown in Table 2. A reduced risk of TC was observed among participants reporting the highest physical activity level (hazard ratio [HR] = 0.65 [confidence interval, CI = 0.44–0.94], p-trend = 0.028) than among participants reporting the lowest level. After stratification by sex, this inverse relationship remained among both sexes; however, it was only significant in women (HR = 0.63 [CI = 0.41–0.95], p-trend = 0.035).
Association Between Thyroid Cancer Risk and Physical Activity (International Physical Activity Questionnaire Continuous Score, Metabolic Equivalent of Task Minutes/Week)
Bold values are significance at p < 0.05.
Model 1: crude model.
Model 2: multivariate model adjusted for age, BMI, alcohol consumption, smoking status, household income, marital status, education, and family history of thyroid cancer. In the overall subjects, model 2 was additionally adjusted for sex.
CI, confidence interval; HR, hazard ratio.
Notably, 12,633 eligible participants had sufficient information on sitting behavior for exploratory analysis. A higher risk of TC was observed among subjects who spent more time sitting, and this trend was constant in the female subgroup but not in the male subgroup. However, this association was not statistically significant (Supplementary Table S1).
In this study, we also clarified the potential relationship between other lifestyle factors and TC risk. While subjects without FHTC were associated with a reduced TC incidence (HR = 0.47 [CI = 0.23–0.96]), a positive association was observed between nonsmokers and the risk of this malignant disease (HR = 3.11 [CI = 1.32–7.35]). However, other risk factors did not show any significant association (Supplementary Table S2). Therefore, in our secondary analysis, we investigated the association between physical activity and TC with stratification by potential confounders. Apart from FHTC and smoking status, we also considered BMI, household income status, and alcohol consumption as confounding factors because of their effects on TC incidence in previous studies. 4,19 –25
For the participants with BMI ≥25 kg/m2, the highest physical activity level was significantly associated with TC risk reduction compared with the subjects with the lowest level, but this difference was only observed in women (HR = 0.38 [CI = 0.16–0.93], p-trend = 0.034) (Table 3). Similarly, participants with a household income >4 million won/month reporting the highest physical activity level were found to have a reduced risk of TC (HR = 0.53 [CI = 0.30–0.94], p-trend = 0.034). However, no significant association was observed among participants with a lower monthly income (less than 4 million per month) (Table 4). There was also a significant association between active lifestyle and a reduction in the TC risk among nondrinkers (HR = 0.48 [CI = 0.26–0.88], p-trend = 0.018) (Supplementary Table S3), nonsmokers (HR = 0.61 [CI = 0.40–0.95], p-trend = 0.038) (Supplementary Table S4), and subjects without FHTC (HR = 0.66 [CI = 0.45–0.96], p-trend = 0.040) (Supplementary Table S5).
Association Between Thyroid Cancer Risk and Physical Activity (International Physical Activity Questionnaire Continuous Score, Metabolic Equivalent of Task Minutes/Week) Stratified by Body Mass Index Level
Bold values are significance at p < 0.05.
Model 1: crude model.
Model 2: multivariate model adjusted for age, family history of thyroid cancer, smoking status, alcohol consumption, household income, marital status, and education. In the overall subjects, model 2 was additionally adjusted for sex.
Association Between Thyroid Cancer Risk and Physical Activity (International Physical Activity Questionnaire Continuous Score, Metabolic Equivalent of Task Minutes/Week) Stratified by Income Status of the Study Participants
Bold values are significance at p < 0.05.
Model 1: crude model.
Model 2: multivariate model adjusted for age, BMI, alcohol consumption, smoking status, marital status, education, and family history of thyroid cancer. In the overall subjects, model 2 was additionally adjusted for sex.
Discussion
The current study identified an inverse association between physical activity level and development of TC in Korean screening study participants. After stratification by confounding variables, the inverse association between physical activity and TC risk was significant among female subjects with BMI ≥25 kg/m2, participants with a household income higher than 4 million won/month, without FHTC, nondrinkers, and nonsmokers.
Previous studies reported the effect of physical activity on the development of TC with inconsistent results. While some studies suggested that the risk of TC was reduced among people engaging in physical activity or daily walking, 10,11 a study by Kim et al 12 reported a positive relationship between a higher physical activity level and TC occurrence. However, since their study design was cross-sectional, it was impossible to conclude a temporal relationship of exercise and TC risk. 12 A potential hypothesis is that after being diagnosed with TC, patients participate in physical activity to improve their health and combat the disease. 12 No significant association was observed between exercise and the development of TC in studies by Kabat et al, 13 Leitzmann et al, 14 and Schmid et al. 15 Kabat et al 13 reported findings that were limited to postmenopausal women, which may limit generalizability to other groups. Furthermore, physical activity measurement in their study was restricted to recreational physical activity, 13 which may limit the statistical power to detect an association between total physical activity and TC.
Several biological mechanisms have already been introduced to underly this association, such as improved metabolic function, the prevention of chronic inflammation, 9 and an altered balance between reactive oxygen species and antioxidant defenses. 26 First, physical activity has been demonstrated to protect against cancer progression through contributing to decrease insulin-like growth factor 1 (IGF-1) level. 26 IGFs are mitogens with a critical effect on regulating cell proliferation, differentiation, and apoptosis. 27 IGFs signal through their receptor, which induces cell transformation upon activation by tumor virus proteins and oncogene products. 27 The role of IGFs in cancer has been replicated in several studies, which have shown that circulating IGF-1 level is positively related to the development of the most diagnosed cancers, including lung, colorectal, breast, and prostate cancers. 27 Furthermore, physical activity is related to lower levels of plasma insulin, higher insulin sensitivity, and better glucose metabolism, even in high-risk individuals. 26 Second, regular exercise is suggested to be an anti-inflammatory factor. 28
This effect of physical activity might be regulated through reducing visceral fat mass and generating an anti-inflammatory environment. 28 Clinical studies have reported that by reducing adiposity, physical activity decreases the accumulation of proinflammatory biomarkers and raises the levels of anti-inflammatory factors. 28 In adipocytes present in adipose tissue, bioactive signaling molecules, such as proinflammatory adipokines and cytokines, are secreted that may lead to cancer progression. 9 For example, leptin is a hormone predominantly secreted by adipocytes that helps to regulate energy expenditure 29 ; previous studies have revealed that high circulating leptin levels are associated with the development of cancers. 30 Leptin is reported to affect tumor growth by modulating several pathways involved in proliferation, angiogenesis, cell survival, and cancer progression. 29
Last, evidence from recent studies has indicated that physical activity enhances antioxidant defenses. 31 An active lifestyle could help enable a response to oxidative stress before damage of cellular structures. 28 Furthermore, the relationship between active lifestyle and TC might be mediated by reducing obesity, which is a well-known risk factor for TC development. 32 –34
In the current study, we further examined the relationship of physical activity and the risk of TC incidence after stratification by confounding variables, including BMI, FHTC, alcohol consumption, and smoking status. First, several studies have suggested that a higher BMI classification is a well-established risk factor for TC development. 4,10,19 –22 After controlling for this variable through stratification, we identified a significant role of physical activity in TC risk reduction in female subjects with BMI ≥25 kg/m2. Overdiagnosis of TC is a critical issue due to cancer screening in Korea. It was reported that incidence of TC in 2011 was 15 times higher than that in 1993, 35 while, its mortality rate was generally stable. We considered that a high income may be associated with a high TC screening rate. 23
Recent Korean studies have reported associations of alcohol consumption, 21,22,24,25 smoking status, 21,22,25 and FHTC with the risk of developing this disease. 21 Thus, when evaluating the effect of exercises against TC occurrence, we stratified the study participants into groups according to these established confounders in the Cox proportional hazards regression models. Interestingly, the protective association was significant among subjects with the highest household income level, without FHTC, nondrinkers, and nonsmokers.
Our study has several strengths. Selection and recall biases were addressed because of a prospective design in our cohort study. We obtained sufficient information on almost all possible confounding variables and were able to control for their effects on the association by adjustment and stratification. TC cases were ascertained from a central cancer registry. However, our study has some limitations. First, there were many missing data. Second, when investigating the association between physical activity and the risk of TC stratified by the confounders, the small sample size of various strata led to a low statistical power to detect a significant relationship. Third, radiation exposure is a well-known risk factor for TC, but this information was not investigated among the subjects included in this study. The limitation may be a source of bias in estimating the association. Fourth, physical activity information was obtained by interviewing the study participants rather than by direct measurement by accelerometer.
Inconsistency in self-reporting of the subjects might lead to the under- or overestimation of physical activity levels. Fifth, new cases of TC in our study could not be verified from the medical records and charts. Information regarding the TC new cases was obtained from linkage with the KCCR database based on the ICD-O. Therefore, the TC subtypes of each patient were not classified, and false negatives may also occur in our data, which might lead to an underreported association between physical activity levels and the risk of TC. Finally, overdiagnosis of TC still occurred in Korea when the study was conducted. Some TC incident cases in our study may have resulted from overdiagnosis and may bias the findings.
Conclusion
The results of this study supported the hypothesis that a high level of physical activity is inversely associated with development of TC in the Korean population. This association was strengthened among female subjects with BMI ≥25 kg/m2, participants with a household income ≥4 million won/month, without FHTC, and those who did not drink alcohol or smoke. Future prospective studies are needed to confirm our findings on the association between physical activity levels and the prevention of TC in other populations. Our results may be helpful for future planning and implementation of physical activity programs for TC prevention and control.
Footnotes
Authors' Contributions
A.Q.B., E.K.L., and J.K. designed and conducted the research; J.L., E.K.L., and J.K.: collected the data; A.Q.B. and J.L. analyzed the data; A.Q.B. wrote the article draft; M.G., E.K.L., and J.K. revised the article. All authors read and approved the final article.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
This work was supported by grants from the International Cooperation & Education Program (NCCRI•NCCI 52210–52211, 2022) of the National Cancer Center, Korea and the National Cancer Center, Korea (2210990).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5