
Abstract
Background:
The actual rates of suspicious thyroid nodules (TNs) and confirmed thyroid cancer (TC) in putatively “at-risk” selected populations (e.g., individuals with family history of TC) are still uncertain.
Methods:
Our aim was to explore the prevalence of TC and TN in a cross-sectional study of a consenting population of unaffected individuals (10 years of age or older) with a first-degree relative known to have non-medullary TC (NMTC). Enrolled subjects underwent ultrasonographic studies of the neck between 2009 and 2018. Nodules considered suspicious according to current guidelines were subjected to fine-needle aspiration biopsy (FNAB) for cytology.
Results:
The screenee population comprised 1176 individuals (median age 42 [26–56] years, 650 females, 55.3%) from 473 kindreds (346 with 1 established NMTC diagnosis at entry, 103 with 2 established NMTC diagnoses, and 24 with 3 or more established NMTC diagnoses at entry). Screening revealed TNs in 500 screenees (42.5%; confidence interval [CI] 39.7–45.4%). Ninety-seven of these (19.4%; CI 16.2–23.1%) underwent FNAB. Only 11 cases of TC were diagnosed in the whole population (0.9%; CI 0.5–1.7%). The prevalence of TC in screenees from kindreds with ≥3 cases (3/24, 12.5%) was higher than that for kindreds with one affected member (6/346, 1.7%; p = 0.01, odds ratio [OR] 7.99; CI 1.21–40.75) and for those with two affected members (2/103, 1.9%; p = 0.05, OR 7.05; CI 0.76–89.44). The prevalence of TNs was 61.8% (CI 56.6–66.8%), 75.7% (CI 66.6–83%), and 66.7% (CI 46.7–82%) in the kindreds with 1, 2, and ≥3 cases, respectively (p = 0.03).
Conclusions:
On the whole, ultrasound-based screening of unaffected relatives of individuals with established diagnoses of NMTC is likely to reveal a high prevalence of TN and a low prevalence of TC. However, a significantly higher prevalence of TC may be found among screenees from kindreds with at least three established NMTC diagnoses before screening, suggesting that closer surveillance may be warranted in kindreds with this level of familiality.
Introduction
Non-medullary thyroid cancers (NMTCs), which originate from the follicular cells of the thyroid epithelium, are among the most common malignancies in women of all ages and in young adults of both sexes. The vast majority of these tumors are sporadic, but ∼3–10% of all cases are associated with familial origin. 1,2 Familial NMTC (FNMTC) should be suspected when a kindred includes two or more first-degree relatives with NMTC and no evidence of other hereditary syndromes known to cause a predisposition to these tumors (e.g., Cowden disease, familial adenomatous polyposis). 2 –5 The genetic underpinnings of FNMTC have yet to be fully defined. 5 –7
Clinically speaking, it is also unclear whether or not FNMTCs are more aggressive or have worse outcomes than their sporadic counterparts and what effect their presence in a kindred has on unaffected kindred members' risk of developing thyroid cancer (TC).
Answers to these questions are crucial for deciding whether or not TC screening should be proposed for currently healthy individuals in FNMTC kindreds. 8
Thus far, however, the clinical implications of NMTC familiality remain largely obscure. Several studies suggest that the FNMTC phenotype is more aggressive than its apparently sporadic counterparts, 9 –12 and a meta-analysis of 12 studies published in 2015 found that FNMTCs are indeed associated with a higher risk of recurrence and lower rates of disease-free survival. 13 However, other studies have failed to find any substantial difference in the behavior of these two NMTC subsets. 14 –17
It is also unclear whether individuals with a family history of NMTC are actually at increased risk for developing TC, since reports on the results of large screening programs in at-risk family members are lacking. And finally, little is known about the actual frequency of thyroid nodules (TNs) and TCs in first-degree relatives of patients with NMTC. The few studies undertaken to explore these questions were conducted in small cohorts 18 –20 or focused exclusively on individuals with only one NMTC-affected relative, 21 or only two or more relatives. 22 Based on this evidence, today's guidelines cannot recommend for or against TC screening in people with FNMTC. 23,24
To shed light on this issue, we analyzed the results of screening sonographic examinations of the neck performed in a large group of presumably healthy individuals with at least one first-degree relative who had been diagnosed with NMTC. Our primary objective was to estimate the prevalence of TC in this population. Our secondary aims were to estimate the prevalence of TNs in the whole study population and the prevalence of TC and TN in screening-population subgroups defined by the number of established NMTC diagnoses in the kindred of origin at study enrolment.
Methods
Screening population enrolment
A prospective cross-sectional study was conducted from January 1, 2009, through December 31, 2018, in the Thyroid Cancer Outpatient Clinic of a large teaching hospital in Rome, Italy (Policlinico Umberto I, Department of Translational and Precision Medicine, Sapienza University of Rome). The protocol was pre-approved by the institutional review board (identification No. 1901), and written, informed consent was obtained from all participants.
During the study period, patients consecutively seen in the clinic for their initial postoperative assessment following surgery for an NMTC were approached by study team physicians, who explained the study goals and methods and invited the patients and their family members to take part in it. The patients who agreed were designated as contact patients for their respective kindreds. Their responsibilities included assisting the study team in recruiting and collecting data on the unaffected members of their kindred (as specified below).
Each contact patient's pedigree was reviewed by the study team to identify the following: (1) the proband (i.e., the first kindred member diagnosed with NMTC—often, but not always the contact patient himself/herself); (2) characteristics of the proband's and affected members' tumors (patient age at diagnosis, tumor focality, and histological diagnosis)—data that, when necessary, were obtained for the team by the contact patient; and (3) other affected kindred members (individuals other than the proband with established diagnoses of NMTC at study enrolment). The remaining members of the kindred (i.e., those who had not been diagnosed with TC at the time of study enrolment) were classified as unaffected at study enrolment.
With the aid of the contact patient, the study team invited each of these unaffected kindred members to take part in a screening program involving sonographic examination of the thyroid and neck (detailed below). The sole eligibility criteria for inclusion of an unaffected kindred member in the screening population were as follows: (1) written informed consent; (2) no history of previous thyroidectomy; and (3) age ≥10 years. The age threshold for enrolment was chosen on the basis of the findings of Sippel et al, who suggested that screening for FNMTC be offered to individuals 5–10 years below the youngest age at NMTC diagnosis within the individual's kindred, 3 and on practices adopted in previous studies that included pediatric patients. 20 Eligible kindred members 10–17 years of age were enrolled with their own approval as well as with the consent of their parents or guardians.
Study procedures
The screening protocol used by the study team consisted of a color-Doppler ultrasound examination of the thyroid gland and all neck lymph node compartments. All examinations were done by clinicians with specific training in the sonographic assessment of these structures, 25 –27 using an Hitachi Avius HI VISION scanner equipped with multifrequency probes (5–13 MHz). In the absence of discrete thyroid lesions, the screenee was classified as TN negative. Screenees were classified as TN positive if their scan revealed at least one discrete lesion with measurable diameters in both the transverse and longitudinal planes. Lesions with a cystic component of ≥75% and a maximum diameter of <3 mm were considered pure microcysts, and the presence of these lesions alone was not sufficient to classify the screenee as TN positive.
In some cases, the examination described above could be deferred for screenees who had recently (≤24 months before study enrolment) undergone sonographic screening in a facility other than the study center. In these cases, the images and diagnosis obtained at the other facility were carefully reviewed by the study team and the results accepted as valid for analysis if the diagnosis reached was unequivocally documented by high-quality ultrasound images. These participants were definitively classified as TN negative or TN positive solely on basis of findings obtained before their enrolment. If instead the externally obtained images provided by the participant did not meet the criteria listed above, the screenee was re-examined by the study team and classified according to the criteria specified above.
All screened participants definitively classified as TN positive (regardless of when it had first been detected) had serum thyrotropin (TSH) assays with reflex free thyroxine (T4) testing (data not collected for analysis), and the sonographic features of their TNs were reviewed and classified by the study team to identify those that warranted fine-needle aspiration biopsy (FNAB) for cytological assessment. From 2009 through 2014, decisions to biopsy were based on the presence of sonographic features considered “suspicious” by American Thyroid Association (ATA) guidelines. 28 Thereafter, nodules requiring FNAB were identified in accordance with the risk stratification system included in the current set of ATA guidelines. 23 Given our interest in the possible role of family history as a risk modifier in the screening population, during the whole study period, it was established to perform FNAB on all suspicious nodules, even if subcentimeter (5–9 mm).
Cytological findings were classified according to the Italian Consensus on Thyroid Cytology. 29 In screenees whose nodules were cytologically indeterminate (corresponding to Bethesda class III or IV), calcitonin testing was also done to exclude the possibility of medullary TC. 30 Surgery was performed on screenees whose nodules were cytologically classified as suspicious for malignancy or malignant (i.e., Bethesda class V or VI) and on selected screenees with indeterminate nodules (i.e., those with high-risk cytological features, sonographic features that were suspicious or displayed changes or evidence of growth over time, and from 2017 onward, suspicious findings in molecular testing). 31
Analysis of data
As noted above, our primary aim was to estimate the prevalence of TC in the screened population (i.e., histologically confirmed TC of any type discovered during the study period in kindred members classified at entry as unaffected). For the purposes of our secondary aims (i.e., to estimate the prevalence of TNs and of TC in screenee-population subgroups defined by the number of established NMTC diagnoses in their kindreds of origin at study enrolment), evaluated kindreds (i.e., those in which at least one member underwent screening) were divided into three groups: Group 1 (those with only one affected member [the proband] at study entry); Group 2 (those with the proband and one other affected member at study entry); and Group 3 (kindreds with three or more affected members, including the proband, at study entry).
Statistical analyses
Continuous variables were expressed as medians and interquartile ranges (IQR), and categorical variables as numbers and percentages. Differences involving categorical variables were assessed with the chi-squared or Fisher exact test, when appropriate; those involving continuous variables were assessed with the Mann-Whitney or Kruskal-Wallis test. The Wilson method was used to calculate confidence intervals (CIs) for proportions. Missing clinical and demographic data are reported in the relevant tables; no imputation or statistical correction was adopted.
Results
Enrollees and their kindreds of origin at study entry
A total of 2289 eligible individuals from 515 kindreds were invited to undergo screening for TC. The invitation was accepted by 1176 (51.4%) of these subjects, representing 473 (91.6%) of the eligible kindreds (Fig. 1). As shown in Supplementary Table S1, the 1176 individuals who agreed to undergo screening were significantly younger (median [IQR]: 42 years [42–56]) and more frequently female (n = 650, 55.3%) than the 1113 who declined our invitation, and these patterns were also evident within the population subgroups composed of individuals from Group 2 and Group 3 kindreds.
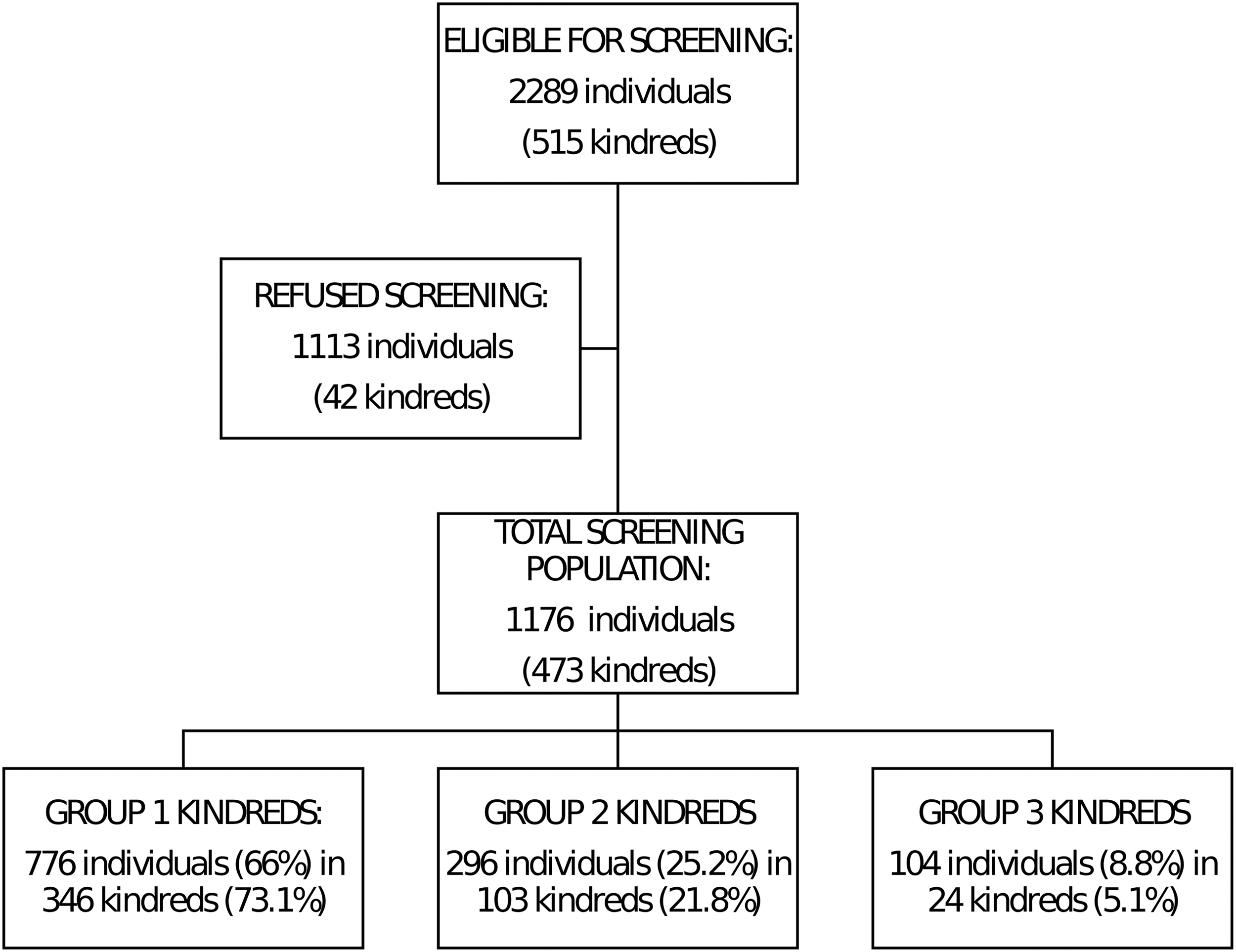
Flow chart showing selection of the screening population. A total of 473 were represented in the screening population (i.e., at least 1 eligible member of the kindred had agreed to screening). These kindreds were grouped according to the number of affected members (those with established NMTC diagnoses) at study enrolment: Group 1 (one affected individual, i.e., the proband); Group 2, two affected individuals (including the proband); and Group 3 (those in which with three or more members (including the proband) had already been diagnosed with thyroid cancer at the time of enrolment. NMTC, non-medullary thyroid cancer.
Enrollees were also significantly more likely to report a pre-enrolment diagnosis of TN (not always confirmed by the study team's review of imaging documentation) and/or to be the offspring (rather than a parent or sibling) of an affected relative. A median of 2 members per kindred was screened in Groups 1 and 2 (range 1–7 and 1–10, respectively). Screening rates in Group 3 kindreds were higher (median: 3 members per kindred; range 1–12).
The main features of the enrolled screening population are summarized in Table 1.
Characteristics of the Study Population at Enrolment and After Screening
Age was unavailable for 14/676 individuals who were TN negative and 15/489 individuals who were TN positive, TC negative. The difference is significant between TN negative and TN positive; not significant between TC positive and the other subgroups.
IQR, interquartile range; NMTC, non-medullary thyroid cancer; TC, thyroid cancer; TN, thyroid nodule.
Sonography results
As shown in Supplementary Table S1, 212 (18%) of the 1176 individuals reported pre-enrolment diagnoses of TN. In 11 of these cases, however, the reported TN diagnosis was not adequately supported by the previously obtained images or by the scans performed by the study team. The final imaging-based diagnoses in these cases were thyroiditis or small, microcystic lesions. Therefore, these 11 screenees were definitively classified as TN negative. In the remaining 201 (94.8%) cases, the pre-enrolment diagnosis of TN positivity was unequivocally confirmed by the study team's review of recent (≤2 years), high-quality ultrasound images obtained elsewhere or, in the absence of the latter documentation, by a new ultrasound examination performed by the study team itself.
All 201 were thus classified as TN positive. The remaining screenee (964/1176) subjects had never been diagnosed with TN, but the study team's ultrasound examination revealed one or more nodules in 299 (31%; CI 28.2–34%). Therefore, a total of 500 (42.5%; CI 39.7–45.4%) of the 1176 enrollees were sonographically classified as TN positive. As shown in Table 1, these 500 individuals were older and more frequently females than the 676 screenees classified as TN negative.
In 97 (19.4%; CI 16.2–23.1%) of the 500 TN-positive subjects, FNAB was performed for cytological examination. In most cases (62/97, 63.9%), the biopsied nodules were cytologically benign. Nine (9.3%) other samples were classified as inadequate for diagnosis. These cases were managed with surveillance and repeat biopsy if indicated. Nineteen (19.6%) biopsies were reported as cytologically indeterminate, and the remaining seven (7.2%) were classified as malignant (n = 3) or suspicious for malignancy (n = 4). These seven screenees and seven of those whose biopsies were indeterminate underwent surgery. In four of these cases (all cytologically indeterminate nodules), the surgical diagnosis was thyroid adenoma. In the other 10 (cases 1–10 in Table 2 32), TC was histologically diagnosed.
Participants Whose Study Ultrasound Scan Revealed Previously Undetected Thyroid Cancers
No. of proband's relatives with thyroid cancer at kindred enrolment.
According to the AJCC TNM Cancer Staging Manual, 8th Edition. 32
Son of second affected member.
AJCC, American Joint Committee on Cancer; ATA, American Thyroid Association; ATC, anaplastic thyroid carcinoma; DTC, differentiated thyroid cancer; NED, no evidence of disease; PTC, papillary thyroid carcinoma; TNM, tumor, node, metastasis.
All 10 of these TCs were discovered during our suggested screening. The eleventh case listed in Table 2 (that of an anaplastic TC [ATC]) is an exception. The patient in question belonged to a Group 3 kindred. He had originally been classified as TN positive by our screening team based on sonographic images obtained at an external facility and reviewed by our study team. The diagnosis (multinodular goiter with no nodules that were suspicious) was confirmed by the study team's review. The patient was advised to undergo repeat sonographic study 1 year later in his hometown, but to our knowledge, this advice was not taken. Two years later, he was referred to our clinic for a clinically evident neck mass and severe dyspnea. Death occurred before any treatment could be performed. An FNAB performed on admission revealed high-grade malignancy, and the suspicion of ATC was confirmed at autopsy.
The prevalence of TC was therefore 11/1176 (0.9%; CI 0.5–1.7%) in the entire screening population and 11/500 (2.2%; CI 1.2–3.9) in the screenees classified as TN positive.
Table 3 summarizes the screening results for all 1176 participants and for subgroups defined by the number of affected kindred members at study entry. Compared with screenees from Group 1 and Group 2 kindreds, those from Group 3 kindreds were significantly more likely to report a pre-enrolment diagnosis of TN, and their relation to an affected kindred member was significantly more likely to be that of a parent or sibling (rather than an offspring).
Baseline Characteristics and Neck Ultrasound Results for the Study Population and Subgroups Defined by Number of Affected Members in the Kindred at Baseline
Subgroups defined by number of affected members at study entry: one (subgroup 1), two (subgroup 2), or three or more (subgroup 3).
Age was unavailable for 29 individuals: 8/776 individuals in group 1 kindreds, 20/296 in group 2 kindreds, and 1/104 in group 3 kindreds.
Focality of the proband's tumor was unavailable for 44 individuals: 19/776 individuals in group 1 kindreds, and 25/296 in group 2 kindreds.
CI, confidence interval.
The definitive rates of TN positivity (those discovered or confirmed by the study team) in the three subgroups were not significantly different (42.3% [CI 38.8–45.8%], 43.2% [CI 37.7–48.9%], and 42.3% [33.2–51.9%] for Groups 1, 2, and 3, respectively; p = 0.96). As for TC, it was discovered in only 6 (0.7%; CI 0.4–1.7%) of the 776 Group 1 subjects and in 2 (0.7%; CI 0.2–2.4%) of the 296 Group 2 kindreds. The proportion of screenees in Group 3 kindreds who were found to have TC (3/104, 2.9%; CI 1–8.1%) was appreciably higher than those in Group 1 and 2 kindreds, but the difference was not statistically significant.
None of the 131 screenees younger than 18 years was diagnosed with TC. (A subgroup analysis of these cases is provided in Supplementary Table S2.)
Table 4 summarizes the screening results grouped by kindred. TN positivity was confirmed or revealed in 308 (65.1%; CI 60.7–69.3%) of the 473 kindreds evaluated, but there was no clinically meaningful difference between the definitive TN rates recorded in the three subgroups (61.8% [CI 56.6–66.8%], 75.7% [CI 66.6–83%], and 66.7% [CI 46.7–82%] in Groups 1, 2, and 3, respectively).
Study Results per Kindreds Grouped According to Number of Affected Members Before Screening
Subgroups defined by number of affected members at study entry: one (subgroup 1), two (subgroup 2), or three or more (subgroup 3).
A statistically significant difference was detected between the TN prevalence in Groups 1 and 2 (p = 0.03). As for TC, it was discovered in only 6 (1.7%; CI 0.8–3.7%) of the 346 Group 1 kindreds and in 2 (1.9%; CI 0.5–6.8%) of the 103 Group 2 kindreds. The proportion of Group 3 kindreds in which one or more screenees were diagnosed with TC (12.5%; CI 4.3–31%) was significantly higher than that recorded for Group 1 (odds ratio [OR] 7.99; CI 1.21–40.75, p = 0.01), but not significant if compared with group 2 kindreds (OR 7.05, CI 0.76–89.44, p = 0.05).
Discussion
Our study suggests that aggressive case finding with high-resolution ultrasonography in families with at least one known case of NMTC can be expected to identify a high number of individuals with TN (42.5% of the screenees we examined), most of which are likely to be benign and persistently asymptomatic. The overall prevalence of confirmed TCs in this population was far lower (<1% in the study population as a whole).
A truly comparable control group for our study was not available, but it is worth noting that the TN and TC prevalence in our screening population as a whole are consistent with—or even lower than—those reported for general populations in various parts of the world. TNs, for example, were found in up to the 68% of healthy individuals in Germany who underwent high-resolution ultrasonographic examinations of the neck. 33 In a large-scale health checkup study conducted in Korea, the overall prevalence of TNs was 34.2%, with higher figures observed in women (41.7%) and older age groups (54.9% in individuals ≥70-year old). 34
As for TC, a recent cohort study undertaken in Germany detected malignancy in 1.1% of individuals with nodules, whose diameters exceeded 1 centimeter. 35 Higher rates have emerged in general populations examined in the United States (8.8% according to Angell, 36 9.2% according to Frates). 37 Several studies that focused exclusively on nodules submitted for cytological assessment revealed variable malignancy rates, with a range (from 2.4% to 23.7%) 35 –38 that comfortably comprises the 10.3% rate observed in the subset of screenees who had FNAB in our study (10/97; 10.3%, CI 5.67–17.9%).
Ten of the malignancies diagnosed in our screening population were differentiated thyroid cancers (DTCs), and, as shown in Table 2, half of these were classified as having an intermediate risk of recurrence, as defined by ATA criteria. 23 This proportion is slightly higher than might be expected on the basis of current figures for Italy, where an ATA intermediate risk of recurrence is reportedly assigned to only about one out of three of all the DTCs. 39,40 (The vast majority of DTCs in Italy are low-risk cancers, and only 5–6% are classified as high risk for recurrence. 39,40 )
The percentage of DTCs diagnosed in our screening population with extrathyroidal extension or cervical lymph node metastases is consistent with reports from the Korean Thyroid Cancer Screening Campaign, which was conducted in the general, asymptomatic adult population and documented the above features in about half the cancers disclosed by screening. 41 None of the screenees with DTCs in our series had any evidence of disease 12 months after the primary treatment (i.e., total thyroidectomy).
Notably, 3 of the 10 DTCs turned out to be papillary TCs with a very low risk of recurrence (intrathyroidal primaries with a maximum diameter <1 centimeter and no evidence of suspicious neck lymph nodes). 42 The significance of such early diagnoses in a setting of potentially familial disease deserves further exploration, 8 but active surveillance is probably still a reasonable alternative to immediate treatment or even immediate biopsy. 43 It is obviously impossible to speculate on what the outcomes of any of the 11 cases of cancer would have been in the absence of our early case-finding efforts. However, in case 11, it seems reasonable to conclude that early sonography had little or no favorable impact on the outcome of this aggressive ATC.
A genetic predisposition to FNMTC is reportedly more likely in kindreds with 3 or more affected members, 44 and a study of 15 kindreds with 2 or more affected members 22 found TC in 19.7% of those screened. Our experience with the substantially larger population described above—over 1000 enrollees—suggests that the likelihood of TC is increased only when 3 or more members are affected (0.8% vs. 0.7% and 2.9% in group 1, 2, and 3 kindreds, respectively).
There was also no association between the likelihood of a TC diagnosis and the generation of the subjects screened. Admittedly, almost half (46.5%) of the 1176 screenees in our study were the son or daughter of an affected relative, and this may have reduced the detection of TC in the older generations. However, the association with screenee generation also failed to emerge in kindreds with three or more affected members, where only 32% of the screenees were the offspring of an affected relative.
It is important to note that, despite our active, targeted efforts to recruit at-risk kindred members for screening, only about half of the eligible relatives contacted agreed to undergo ultrasonography. As noted above, males and older individuals of either sex were more prone to refuse the examination. Although this may conceivably have caused a selection bias, it is a common feature of almost all screening programs. In screening programs recommended to the population at risk, adherence rates rarely exceed 50–60% (e.g., colorectal examination: 54.6% 45 ; annual lung cancer screening: 40.2%). 46
For women enrolled in the 2016 Korean Study of Women's Health-Related Issues, the overall rate of TC screening was 39.2%. 47 In the general population, older patients are more likely to have TN, 34,35 but their risk of thyroid malignancy is lower compared with their younger counterparts. 35,48 Therefore, the age-related selection bias in our screening population may have led us to underestimate the prevalence of TN among unaffected individuals with a family history of NMTC, but it is unlikely to have had any impact on the prevalence of TC in these subjects.
Moreover, ultrasonography is capable of disclosing a subclinical condition, but it cannot predict whether other TCs will develop in the enrolled relatives in the future. Unfortunately, although the past 20 years have witnessed major advances in our knowledge of the clinical presentations 13,49 and genetic alterations associated with FNMTC, there is still no reliable genetic test for FNMTC. 2,5 This might have led to some underestimation of the TC prevalence found within a limited timeframe using sonographic screening.
We did not collect long-term follow-up data on our screenees. However, all those classified as TN positive were advised to have a repeat thyroid ultrasound in 12–24 months, and those classified as TN negative were advised to get a repeat scan in 5 years. We also asked the contact patients and the screenees themselves to notify us if new diagnoses of TC emerged within their kindreds. The low number of TCs that was found precluded a more robust statistical analysis of their clinical data.
Furthermore, our findings cannot provide any data for a cost-effectiveness evaluation of a screening program because the potential benefits on health outcomes, for example, quality-adjusted life years gained and disability-adjusted life years averted, are not evaluable. 50 Neither did we collect data on the potential adverse effects of screening, which include complications from FNAB, 51 surgery-related sequelae (hypothyroidism, hypoparathyroidism, hematoma, and laryngeal nerve palsy), 52 psychological issues, 53,54 and financial problems. 55
In conclusion, systematic case-finding with neck ultrasonography for individuals with a family history of NMTC can be expected to identify a substantial number of patients with TNs, which in most cases are benign and clinically insignificant. The results of our study do not support the view that a family history of NMTC limited to one or two relatives puts unaffected relatives at an increased risk for TC. Kindreds with three or more affected members may warrant closer surveillance, although much more work is needed before cost-effective tools and time schedules for such surveillance can be prescribed.
Footnotes
Acknowledgments
Writing support was provided by Marian Everett Kent, BSN. We thank the following residents and fellows of the Sapienza University of Rome, School of Medicine, for contributing to this project: Marco Ammendola, Laura Ciotti, Cristiano Lomonaco, Stefania Lupo, Alessandra Paciaroni, and Katia Plasmati.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
The study was supported by research grants from The Umberto Di Mario Foundation and from the Banca d'Italia.
Supplementary Material
Supplementary Table S1
Supplementary Table S2