
Abstract
Background:
High body mass index (BMI) has previously been associated with increased risk of differentiated thyroid cancer (DTC); however, only few studies have investigated the association with BMI in a large cohort assessed at a young age and with sufficient data on confounding factors. We assessed the association between excess body weight and the risk of DTC and papillary thyroid cancer (PTC) in a large cohort of young Danish women with substantial confounder control.
Methods:
We included all parous Danish women registered with a prepregnancy BMI ≥18.5 kg/m2 during 2004–2016 in the Danish Medical Birth Registry in the study population. Cox proportional hazards regression models were used to estimate the hazard ratios (HRs) with confidence intervals (CIs) of DTC according to BMI. In subanalyses, we investigated PTC as a separate group. Analyses were adjusted for calendar time, education, smoking status, benign thyroid disease (BTD), type II diabetes, parity, and oral contraceptive use. In addition, we examined the association with increasing BMI stratified for previous BTD.
Results:
A total of 443,403 women were included in the study population, and the median age at baseline was 30.0 years. Altogether, 463 women were diagnosed with DTC during follow-up. Excess body weight was associated with a higher rate of DTC (overweight, BMI 25–29.9 kg/m2: HR = 1.54; CI 1.25–1.90. Obese, BMI ≥30 kg/m2: HR = 1.32; CI 1.00–1.75) compared with normal weight. Results were similar in PTC. In addition, we found an increased rate of DTC with increasing BMI, when investigating BMI as a continuous variable per 5 kg/m2 increase (HR = 1.17; CI 1.07–1.27). The results were similar in women without previous BTD.
Conclusions:
Our study confirms that excess body weight is associated with an increased incidence of DTC and PTC in women.
Introduction
Thyroid cancer is the most common endocrine malignancy with an estimation of more than 580,000 new cases per year worldwide. 1 Thyroid cancer is nearly three times more common in women than in men with incidence rates peaking around 40–49 years in women and 60–69 years in men. 2 Although thyroid cancer only represents 2.1% of all malignancies globally, 3 and the mortality is relatively low, the rate of disease recurrence or persistence is high, and the treatment of thyroid cancer is associated with lifelong side effects. 4
Differentiated thyroid cancer (DTC; comprising papillary and follicular thyroid cancer) accounts for the vast majority of histological subtypes. 5 DTC differs from other histological subtypes (e.g., anaplastic and medullary thyroid cancer) in terms of a relatively good prognosis. 6 In Denmark, the incidence of thyroid cancer increased on average by 8% per year from 2005 to 2014. 6 The substantial increase is found not only in Denmark but globally. 7 –9 Obesity is also an increasing health issue. Worldwide, an estimated 640 million adults were obese in 2014. 10 It is well established that excess body weight is a risk factor in the development of cancer. 11 Therefore, obesity has also been proposed to contribute to the observed increase in thyroid cancer incidence. 12,13
Indeed, previous studies have found that excess body weight was associated with increased incidence of thyroid cancer. 14 An increased risk of thyroid cancer has also been observed among patients with benign thyroid disease (BTD). 15 Patients with BTD may experience thyroid dysfunction, which affects the basic metabolic rate and thereby body mass index (BMI; e.g., hyperthyroidism is associated with weight loss, while hypothyroidism is associated with weight gain). 16,17 Large cohort studies investigating the association between excess body weight and thyroid cancer with sufficient data on BTD are missing.
In this large and nationwide study, including more than 440,000 young Danish women, we aimed to assess the association between excess body weight and subsequent incidence of DTC and, in subanalyses, papillary thyroid cancer (PTC) controlling for age, calendar time, BTD, diabetes type II (DT2), education, smoking, oral contraceptive use, and parity.
Materials and Methods
Data sources
In Denmark, all citizens are assigned a unique 10-digit civil registration number (CPR) at birth or migration into Denmark. 18 The Danish National Health Service guarantees tax-supported health care for all citizens, and the use of health care is registered by multiple nationwide registries. In the present study, the CPR was used in retrieval of data and secured valid linkage between the following four national registries: Danish Medical Birth Register, Danish National Patient Register, Danish Cancer Registry, and the Danish National Prescription Registry.
Study population
The study population was identified from the Danish Medical Birth Registry, which contains data on all Danish women who have given birth, and it includes information such as maternal characteristics. 19 The identification of the study population is presented in Figure 1. We identified all Danish women registered with a valid prepregnancy BMI ≥18.5 kg/m2 from 2004 to 2016 (n = 461,150). Baseline was defined as the birth date of the first child for whom we had the mother's prepregnancy BMI registered. We only included women registered with a BMI <60 kg/m2, or height of 120–210 cm and a weight of 25–210 kg, to account for potential registration errors. First prepregnancy BMI was used for analysis if the women had several registrations. Women with a cancer diagnosis (except nonmelanoma skin cancer, n = 2326) and/or a thyroidectomy before baseline (n = 178) were excluded. In the primary analyses we also excluded women with missing information on smoking and/or education (n = 17,747) (Fig. 1).
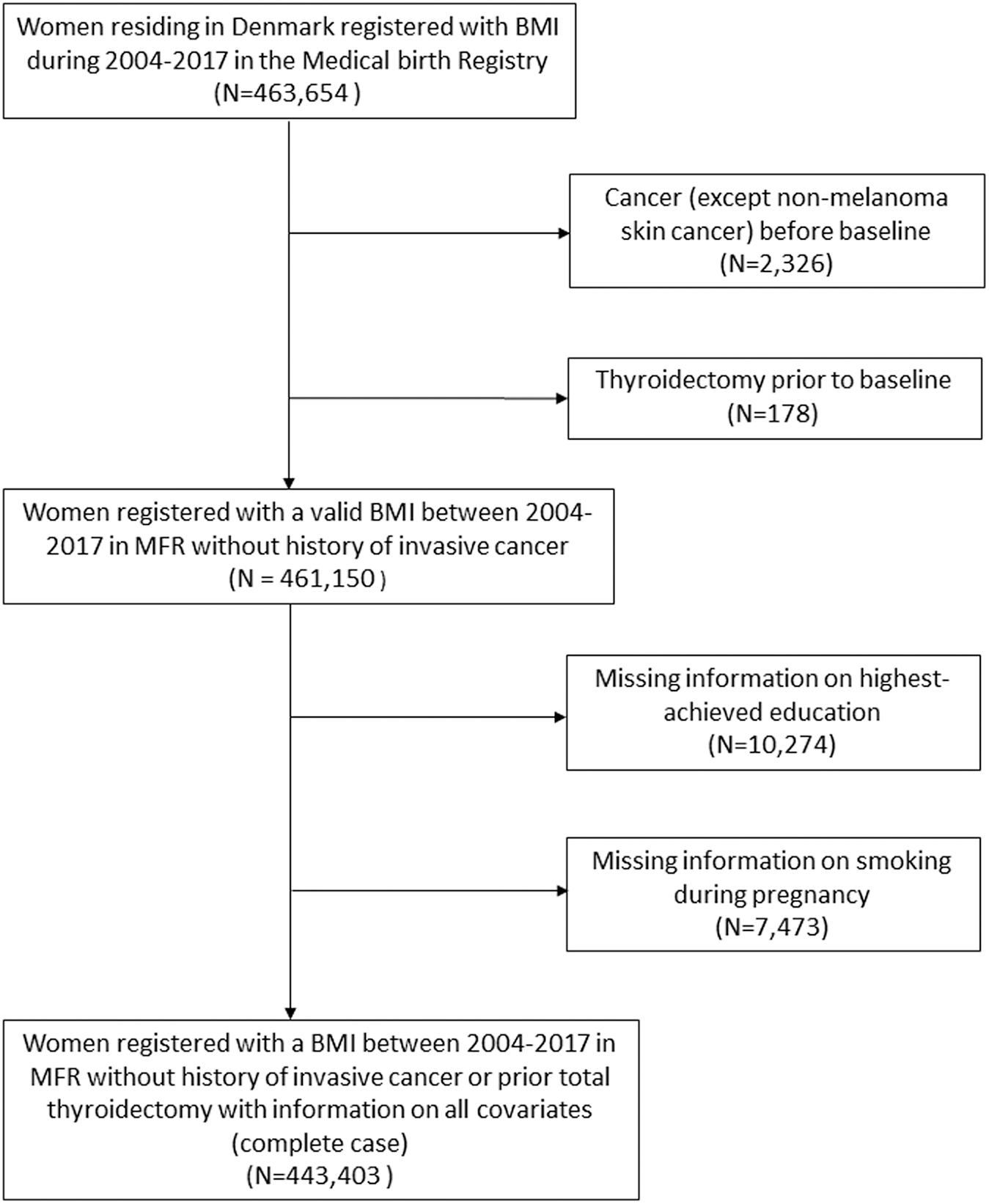
Flow chart of the study population.
Definition of outcome
Outcome was defined as a diagnosis of DTC (i.e., PTC or follicular thyroid cancer) or PTC during follow-up. We identified all thyroid cancer cases in the Danish Cancer Registry, which holds information on virtually all new cases of cancer in the Danish population since 1943. 20 We used topography code C73 and morphology codes (papillary: 82603, 83413, and 83403; follicular: 82903, 83303, 83313, and 83353) from the International Classification of Diseases for Oncology, 3rd edition, ICD-O-3 to identify all incident cases of histologically confirmed DTC. Information on stage at diagnosis was also retrieved from the Danish cancer registry and categorized into the following: Localized stage (including TNM stages T1–T3a,N0,M0), nonlocalized stage [including T3b–T4b,N0,M0, T(any),N1,M0, and T(any),N(any),M1], and unknown stage. 21 Information was available up until December 31, 2019.
Definition of other variables
We obtained information on other variables shown to potentially affect the risk of thyroid cancer by linking our cohort with various national registries. Data were collected both at baseline (main analyses) and during follow-up (sensitivity analyses).
Data regarding parity and prepregnancy smoking were obtained from the Medical Birth Registry. Parity was defined as the total number of live births, including the birth of the child for whom we had the mother's prepregnancy BMI registered. Data were available up until December 31, 2016. Information on diagnosis of other cancers (except nonmelanoma skin cancer) was retrieved through The Danish Cancer Registry. Information was available up until December 31, 2019. We retrieved information on diagnoses of BTD (including hyperthyroidism, hypothyroidism, nontoxic goiter, thyroiditis, and adenoma), thyroidectomy, and DT2 through the National Patient Register, 22 which holds information on all hospital admissions since 1977, and all hospital outpatient contacts in Denmark since 1995 in form of admissions, treatments, procedures, and diagnoses according to the International Classification of Diseases ICD-8 or ICD-10 systems. ICD-8 and ICD-10 codes used are listed in Supplementary Table S1. Data were available up until December 31, 2017.
Highest achieved education was obtained from Statistics Denmark. 23 If possible, it was defined at baseline, if not 1 year before or after baseline. It was divided into three categories: short (≤7 years for individuals born before 1958 and ≤9 years for individuals born from 1958); medium (8–12 years for individuals born before 1958 and 10–12 years for individuals born from 1958), and long (≥13 years). Information regarding oral contraceptive use was assessed through the Danish National Prescription Registry, which holds data on all drugs sold on prescription at Danish community pharmacies since 1995. 24 Finally, information on vital status and migration (and dates) during follow-up was obtained from the Civil Registration System.
Statistical analyses
Follow-up began at the birth date of the first child for whom we had the mother's prepregnancy BMI registered and ended at the date of DTC diagnosis, total thyroidectomy, thyroid cancer diagnosis with other morphology than differentiated, other cancer diagnosis (except nonmelanoma skin cancer), death, emigration, or December 31, 2019, whichever came first. Women were categorized into three groups according to their BMI: Normal weight (18.5–24.9 kg/m2); overweight (25–29.9 kg/m2); and obesity (≥30 kg/m2). Women were also categorized according to previous BTD assessed at baseline (ever/never and by type of BTD: hyperthyroidism, hypothyroidism, and nontoxic goiter. Due to a low number of cases, it was not possible to assess adenoma and thyroiditis as separate groups).
The absolute risk of DTC according to BMI was estimated using the nonparametric Aalen-Johansen estimator treating total thyroidectomy, non-DTC, and death as competing events.
Associations between BMI and incidence rates of both DTC and PTC were assessed using Cox-proportional hazards models with age as the underlying time scale applying delayed entry at age of birth of the child where the prepregnancy BMI was registered and reported as hazard ratios (HRs) with confidence intervals (CIs).
In addition, we performed analyses evaluating the association between BMI and DTC/PTC incidence rates stratified by previous BTD measured at baseline (ever/never and by type of BTD). Due to low numbers, we investigated BMI as a continuous variable and not in categories in this analysis. Models were adjusted for calendar time (continuous) alone or in combination with BTD (ever, never), DT2 (ever, never), parity (1, 2, 3, or 4+), oral contraceptive use (ever, never), smoking (ever, never), and highest achieved education (short, medium, high) measured at baseline. These variables were selected a priori based on the literature and availability in the registers. 15,25 –28 For detailed description of the statistical methods used, please be referred to the Methods Supplement section in the Supplementary Data.
We conducted the statistical analyses using the statistical software SAS version 9.4 (SAS, Cary, NC), with a statistical significance level of 5%.
Results
Our total study population comprised 443,403 women (Table 1) of whom 67.0% were normal weight, 21.2% were overweight, and 11.8% were obese. The median age at baseline was 30.0 years (interquartile range: 26.8–33.5). There was no marked difference between prepregnancy BMI groups according to age, parity, oral contraceptive use, smoking, DT2, and previous BTD. A larger proportion of obese women had a short education (25.3%) compared with the remaining BMI groups (Table 1).
Characteristics of the Study Participants (N = 443,403) at Baseline According to Prepregnancy Body Mass Index Categories
Including: hyperthyroidism, hypothyroidism, nontoxic nodular goiter, simple goiter, unspecified goiter, thyroiditis, and adenoma.
BMI, body mass index; IQR, interquartile range.
During follow-up, 623 exited due to death, 16,599 emigrated, 383 had a total thyroidectomy performed and no prior DTC diagnosis, and 8198 exited due to a diagnosis of other cancer than DTC. Four hundred sixty-three women were diagnosed with DTC during follow-up, of whom 391 women were diagnosed with PTC (84.4%). In women with DTC, 269 were normal weight, 132 overweight, and 62 were obese, according to their prepregnancy BMI. At diagnosis, the stage distribution among women with DTC (localized stage, nonlocalized stage, and unknown stage) was similar when comparing BMI groups (Supplementary Table S2). It should be noted that a large percentage of cases had unknown stage (33.3%). The median follow-up time was 10.5 years (range: 0–16 years).
The absolute risk of DTC was similar between BMI groups before the age of 40. After around age 45, the absolute risk was higher in overweight and obese women than in normal weight women. At age 50, women of normal weight had an absolute risk of DTC of 0.19% compared with overweight and obese women, where the absolute risks were ∼0.32% (Fig. 2).
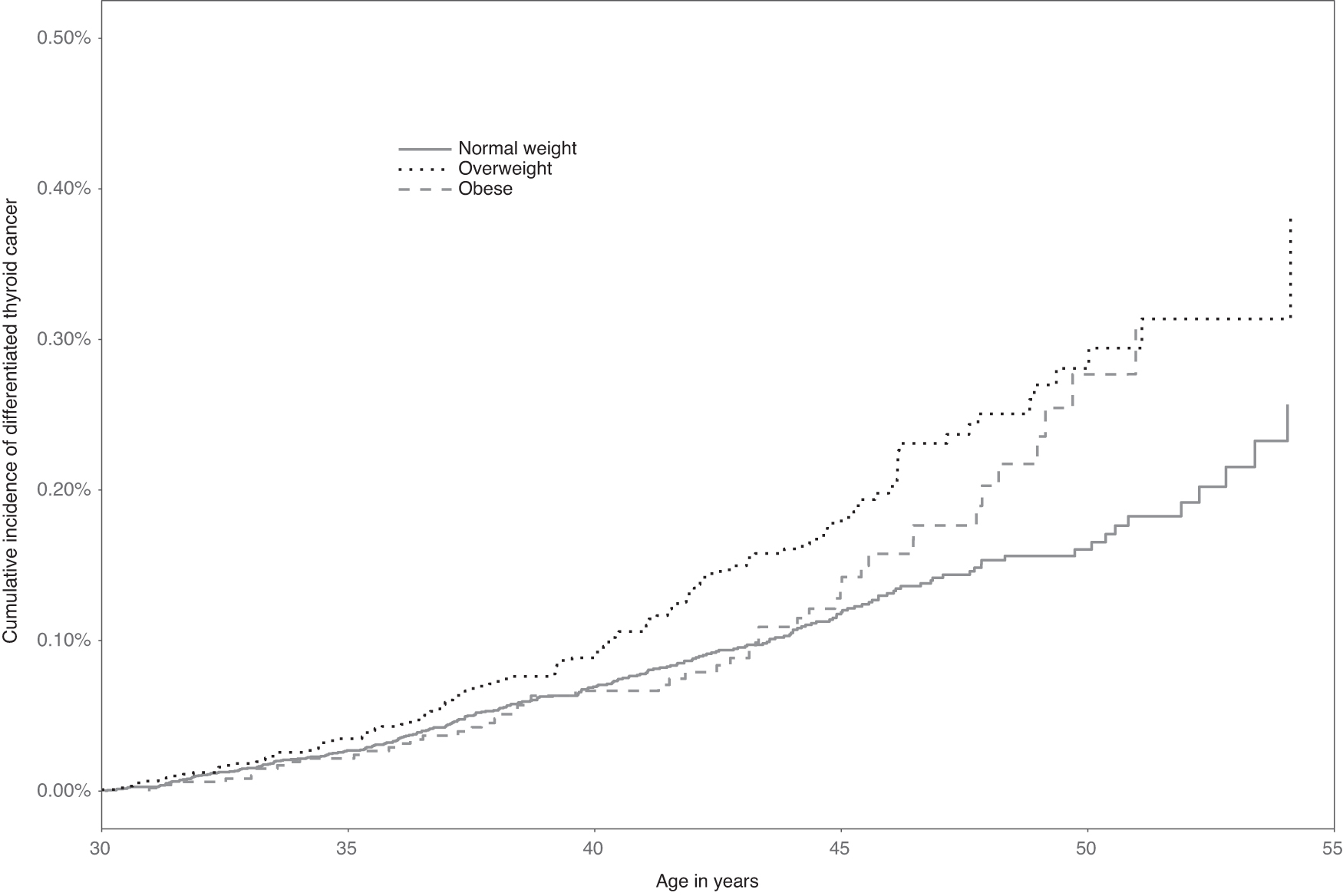
Cumulative incidence of differentiated thyroid cancer according to BMI categories. BMI, body mass index.
In the adjusted analyses, we found that overweight was associated with a 1.54-fold [CI 1.25–1.90] higher rate of DTC compared with normal weight. The corresponding adjusted HR for obese women to develop DTC was 1.32 [CI 1.00–1.75] (Table 2).
Estimated Hazard Ratios of Differentiated Thyroid Cancer (n = 463) and Papillary Thyroid Cancer (n = 391) Among 443,403 Women According to Prepregnancy Body Mass Index
Model 1: Adjusted for age (underlying time scale), calendar time (continuous). Model 2: Adjusted for age (underlying time scale), calendar time (continuous), education (short, medium, high), smoking status (ever, never), benign thyroid disease (ever, never), type II diabetes (ever, never), parity (1,2,3,4+), and oral contraceptive use (ever, never).
CI, confidence interval; DTC, differentiated thyroid cancer; HR, hazard ratio; PTC, papillary thyroid cancer; WHO, World Health Organization.
We assessed PTC as a separate outcome and found similar results. Overweight was associated with an adjusted 1.52-fold [CI 1.21–1.90] higher rate and obesity with a 1.27-fold [CI 0.93–1.72] higher rate of PTC compared with normal weight (Table 2). We also investigated BMI as a continuous variable per 5 kg/m2 increase and found an increased rate of DTC with increasing BMI (HR = 1.17; CI 1.07–1.27) when adjusted for calendar time, education, smoking status, previous BTD, DT2, parity, and oral contraceptive use (Table 2).
When stratified by previous BTD, increasing BMI (per 5 kg/m2) was associated with an increased rate of both DTC and PTC in women without previous BTD (HRDTC = 1.19; CI 1.09–1.31. HRPTC = 1.17; CI 1.06–1.30). In contrast, we found no association between increasing BMI and the rate of DTC or PTC (N DTC = 44, HRDTC = 0.89; CI 0.63–1.26. N PTC = 39, HRPTC = 0.96; CI 0.68–1.35) in women with previous BTD. When further stratified by type of BTD (hyperthyroidism, hypothyroidism, and nontoxic goiter), the results were largely identical. Analyses were adjusted for calendar time, education, smoking status, DT2, parity, and oral contraceptive use (data not shown).
We performed sensitivity analyses also including women with missing values on smoking and/or education (Supplementary Table S3); adjusting for previous BTD, DT2, parity, oral contraceptive use as time varying variables (Supplementary Table S4); ending follow-up at December 31, 2017 (Supplementary Table S5); only including women born from 1980 and onward (Supplementary Table S6); and applying delayed entry 2 years after start of follow-up (data not shown). The results were overall similar to those reported in Table 2 and did not affect our conclusions. In addition, we estimated the association with continuous BMI and incidence of DTC according to age. The overall estimated association tended to be slightly nonproportional showing a less pronounced association in younger age at diagnosis (HR<40 = 1.09; CI 0.97–1.21; HR40–50 = 1.27; CI 1.11–1.46; HR50+ = 1.32; CI 0.86–2.01). Furthermore, a more detailed categorization of BMI did not indicate that the association with BMI declined or leveled off at high values (Supplementary Table S7).
Discussion
In this nationwide register-based cohort study we found an association between excess body weight and higher incidence of DTC and PTC in a population of young Danish women.
Supporting our findings, some other studies reported higher risk of thyroid cancer associated with overweight and obesity, both for PTC, 29,30 DTC 31,32 and thyroid cancer as one combined group. 14,33,34
When investigating BMI as a continuous variable, we observed a positive linear association between BMI and the incidence of thyroid cancer in line with previous studies. 14,31,34 This may suggest a tendency toward increasing risk of thyroid cancer with increasing BMI.
Interestingly, our results showed that the absolute risk of DTC was somewhat similar between BMI groups up until age 45. From around age 45 the absolute risk increased predominantly among overweight and obese women compared with normal weight. This age pattern was supported in the adjusted analysis allowing the association with BMI to vary with age. The effect of BMI on the risk of thyroid cancer may be associated to the period of time, the individual is exposed to the extra body weight, or there may be a latency period between excess body weight and the development of thyroid cancer. Alternatively, the increased risk around age 45 may be related to biological alterations associated with menopause, although this is unknown. Studies investigating the association between reproductive factors and thyroid cancer are equivocal. 35
Several biological pathways may explain the link between obesity and thyroid cancer. Studies focusing on thyroid cancer specifically are somewhat sparse, although research on how obesity affects cancer in general is rapidly advancing. The expansion of adipose tissue and enlargement of adipocytes associated with obesity lead to several metabolic disturbances, including chronic inflammation, insulin resistance, alterations in production of adipokines, and changes in synthesis and bioavailability of sex steroids. 36 Inflammation is thought to link obesity and cancer through pro-inflammatory cytokines such as TNF-α and IL-6. 37,38 In thyroid cancer, an increased risk has been associated with IL-10 but not TNF-α and IL-6. 39
Insulin resistance results in hyperinsulinemia, which promotes a cellular environment that favors carcinogenesis partly through increased levels of free IGF-1 and decreased levels of IGF binding protein. 40 In thyroid cancer, studies reported increased risk associated with both elevated IGF-1 levels and insulin resistance. 41,42
The plasma levels of adiponectin, which is an adipokine exclusively produced in adipocytes, are reduced in obesity. Adiponectin has insulin-sensitizing and anti-inflammatory effects, and studies suggest an increasing risk of several cancers with decreasing levels of adiponectin. 43,44 Focusing on DTC, Dossus et al found an increased risk associated with reduced adiponectin levels in women. 39
Some argue that the association between obesity and thyroid cancer may be explained by enhanced detection among patients with chronic conditions linked to obesity such as BTD or DT2, as these patients have more frequent contact to the health care system. 45 In a recent study, Fussey et al found no causal role for obesity in DTC using Mendelian randomization approaches. 46 The authors suggested DT2 as a potential confounding factor, as DT2 is associated with both obesity and thyroid cancer, further supported by their results pointing toward a possible causative role of DT2 in thyroid cancer. However, in our analyses we adjusted for both BTD and DT2 with no marked effect on the estimates. Furthermore, when stratified by previous BTD, women without previous BTD still showed an increased rate of DTC and PTC with increasing BMI. In addition, we found a similar stage distribution among DTC cases when comparing BMI groups. Therefore, enhanced detection may not be the only explanation of the association between a BMI higher than normal and DTC found in this study. However, enhanced detection as an explanation cannot entirely be ruled out.
An explanation on why women with previous BTD have no increased risk of thyroid cancer with increasing BMI may be that these women already have a high risk of thyroid cancer 15 and the impact of increasing BMI may not be as significant.
In a pooled analysis of 22 prospective studies investigating the risk of thyroid cancer in relation to anthropometric factors measured in different ages, Kitahara et al found that women with a BMI higher than normal measured at age 17–21 years had an increased risk of thyroid cancer (HR = 1.50, CI: 1.14–1.96), while the estimate for women with a BMI higher than normal measured at a mean age of 56.7 years was HR = 1.02 [CI: 0.93–1.14]. 47 This may suggest that being obese in young adulthood results in a greater risk of thyroid cancer compared with being obese in older ages. Indeed, Kitahara et al state that BMI specifically in young adulthood has been associated with increased risk of thyroid cancer.
The present study is based on a large cohort of women with their BMI registered at a young age. This was possible due to the Danish Medical Birth Register that holds prepregnancy BMI registration from 2003. This registry has a coverage of 98% of all births in Denmark and only ∼6% with missing information on BMI. 19,48 In addition, to our knowledge we are the first cohort study to obtain information on both previous BTD and DT2 making it possible to adjust the analyses for these often debated and potentially confounding factors.
Our study also has some limitations. In most cases, BMI was registered based on self-reported height and weight, potentially resulting in social desirability bias; it is most likely to cause a lower prevalence of overweight and obesity and thereby lead to a slight underestimation of the association with obesity. Second, as the women in our cohort were all parous, our results may not necessarily apply to nulliparous women. Third, women with BTD represented a small group. This should be taken into consideration when interpreting the results of our analyses stratified by BTD. Finally, due to a low number of cases, we were not able to assess follicular thyroid cancer as a separate group.
In summary, the findings of our study provide further support to the existence of an association between excess body weight and an increased rate of DTC and PTC in women. Overweight and obesity may contribute to the rising incidence of thyroid cancer, and efforts made to prevent excess body weight could possibly have a beneficial effect on the increasing rates.
Ethical Approval
The study was approved by Statistics Denmark's Scientific Board (project number 707066) and registered internally at the Danish Cancer Society Research Center (project number 2020-DCRC-0049). Ethical approval was not required for this registry-based study, according to Danish law. 49 All data were stored on a secure platform at Statistics Denmark, which can be accessed given obtainment of the relevant permissions.
Footnotes
Author Confirmation Statement
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in THYROID.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
No specific funding was obtained for this project.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7