
Abstract
Background:
Calcitonin measurement is widely used in the diagnosis, prognosis, and follow-up of patients with medullary thyroid carcinoma (MTC). The prognostic value of undetectable postoperative calcitonin (POCal) in long-term disease outcomes remains uncertain.
Objective:
The aim of this study is to evaluate POCal as a prognostic marker for long-term MTC disease status.
Methods:
A retrospective cohort study was carried out. We collected data from the medical records of patients with MTC attending two tertiary teaching hospitals. Patients were divided according to POCal into two groups: undetectable (below the detection limit) or detectable. The outcome was determined at the last medical visit and defined as disease free (undetectable calcitonin and no evidence of disease on imaging), persistent disease (detectable calcitonin with or without structural disease), or disease-related death.
Results:
Three hundred thirty-four MTC patients were included in the study. The mean age at diagnosis was 41.1 ± 18.6 years; 202 patients (60.5%) were women; and 167 patients (50.0%) had sporadic MTC. The median tumor size was 2.0 cm (1.1–3.5 cm); 164 patients (49.1%) had lymph node metastasis and 63 patients (18.9%) had distant metastasis. At the first postoperative evaluation (3–6 months after surgery), 141 patients had undetectable POCal (mean age = 37.9 years, 70.9% women, median tumor size 1.5 cm [0.7–2.5 cm]; 28 [19.9%] had lymph node metastasis and none had distant metastasis). After a median follow-up of 7.7 years (2.1–13.2 years), 127 (90.1%) of these patients were free of disease, whereas 14 (9.9%) had persistent biochemical disease with stable calcitonin levels. No patient with undetectable POCal died of the disease. In the detectable POCal group (mean age = 42.9 years, 52.8% women, median tumor size 3.0 cm [1.8–4.2 cm]; 136 [70.5%] had lymph node metastasis and 63 [32.6%] had distant metastasis), 18 (9.2%) patients achieved disease-free status, 51 (26.6%) had biochemical disease, and 61 (31.6%) had persistent structural disease. Sixty-three (32.6%) patients died of disease-related events. Further analysis using a multivariate model identified undetectable POCal as an independent prognostic variable for disease-free status (HR = 5.33, CI = 2.86–9.94; p < 0.001).
Conclusions:
POCal is a strong prognostic marker for long-term disease-free survival and might help define follow-up strategies for MTC patients.
Introduction
Medullary thyroid carcinoma (MTC) is a malignant tumor originating in the C cells of the thyroid gland. MTC may occur sporadically (75%) or as part of an inherited syndrome named multiple endocrine neoplasia type 2 (MEN2). The MEN2 syndrome is classified according to the involved organs as MEN2A and MEN2B. 1 –3 Hereditary MTC is caused by activating germline mutations of the RET (REarranged during transfection) proto-oncogene, and genetic screening allows for early diagnosis and treatment.
Although MTC prevalence represents 2–4% of all thyroid malignancies, MTC accounts for 13.4% of all deaths attributable to thyroid cancer, highlighting the importance of identifying prognostic factors for persistent disease. 3 –6 The possibility of complete surgical resection is a key factor leading to a cure for MTC. The tumor-node-metastasis (TNM) classification system is used for postoperative MTC risk stratification and has shown excellent correlation with disease-specific mortality. 7
Additional factors associated with MTC prognosis include age at diagnosis, extrathyroidal invasion, cervical lymph node metastasis, distant metastasis, and delayed or incomplete surgical treatment. 3 –5,8 –11
Calcitonin, a highly sensitive and specific MTC biomarker, is widely used in the diagnosis, prognosis, and follow-up of patients with MTC, and current guidelines recommend its measurement to evaluate patient follow-up. 3,12,13 Neoplastic C cells also produce carcinoembryonic antigen (CEA). Calcitonin and CEA doubling times are excellent tools to predict MTC prognosis. 12 More recently, increased expression of carbohydrate antigen 19.9, a well-established tumor marker in other human neoplasms, has been proposed as a prognostic marker of tumor aggressiveness in MTC. 14,15
Few studies have evaluated the prognostic role of postoperative calcitonin (POCal) in MTC. Jung et al published a 30-year retrospective analysis showing that the postoperative biochemical remission of serum calcitonin is the best predictive factor for recurrence-free survival in MTC. 16 However, the follow-up period (4.6 years) was relatively short, and the authors used the same calcitonin cutoff value regardless of the measurement method, thus reducing external validity.
Saltiki et al 17 showed that POCal levels higher than 4.65 pg/mL were associated with persistent disease (sensitivity, 93.8%; and specificity, 90%), while POCal levels higher than 14.5 pg/mL predicted disease progression (sensitivity, 100%; and specificity, 82%). However, the study only included small tumors. Interestingly, MTC patients who exhibited POCal levels within the reference range of nonthyroidectomized individuals (2–10 pg/mL) had a higher risk of disease recurrence than those with undetectable calcitonin levels. 18
These findings further illustrate that even at low levels, calcitonin might indicate the presence of neoplastic C cells. Biochemical response to surgery was also identified as an important predictor of outcome in a recent retrospective study. 19 Of interest, the POCal value seems to be a reliable marker of response to therapy as early as one month after surgery. 20
In the present study, we investigated the role of undetectable POCal as a marker for long-term disease-free survival in a large cohort of patients with MTC.
Methods
Patients and study design
Four hundred fifty-three patients with MTC, attending the Thyroid Unit at Hospital de Clínicas de Porto Alegre (HCPA) or the Endocrine Oncology Unit at the Brazilian National Cancer Institute (INCA) from 1997 to 2019, were eligible for the study. Both institutions are tertiary care teaching hospitals and referral centers for MTC treatment in Brazil.
Since 1997, HCPA has been a referral center for molecular testing for germline RET mutations in Brazil; therefore, patients referred to HCPA from other Brazilian centers for molecular investigation were also invited. All patients had anatomopathological MTC diagnoses confirmed by immunohistochemistry. Patients without follow-up data after initial therapy (n = 28) and those with only C cell hyperplasia (n = 2) or noncalcitonin-secreting tumors (n = 2) were excluded from the study.
Clinical and oncological data were retrieved from the medical records of 453 MTC patients: 208 patients attending HCPA, 111 at INCA, and 134 from other institutions. POCal and final status data were available for 334 patients (Fig. 1).
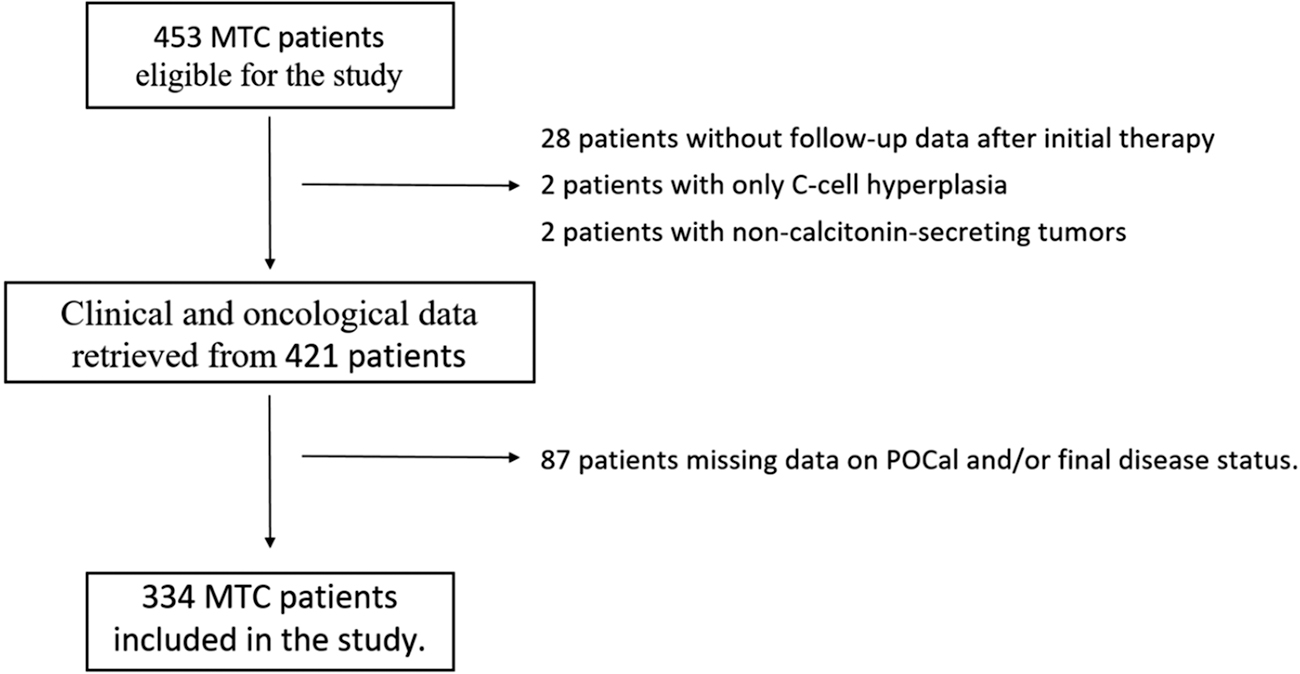
Flow chart showing the individuals included at each stage of the study as well as those excluded (with reasons) for each level.
Institutional Review Board approvals
The study was approved by the Institutional Research Ethics Committee (CAAE 73671717.8.0000.5327), and written informed consent was obtained from each study participant or legal representative. All participants received pretest and post-test genetic counseling. The research was completed in accordance with the Declaration of Helsinki as revised in 2013.
Institutional treatment protocol and follow-up
The MTC treatment protocol in our institution follows the current clinical guidelines. 3,12 All patients underwent total thyroidectomy with central and bilateral neck exploration depending on calcitonin levels and evidence of suspicious lymph nodes on preoperative neck ultrasound (US). Decisions about the extent of cervical lymph node dissection were made at the discretion of the surgical team during surgical exploration.
At the first evaluation, the following data were recorded for each patient: demographics, tumor and disease characteristics (e.g., histological features, tumor size, extension, lymph node involvement, or distant metastasis), and treatment (e.g., surgery, radiotherapy, tyrosine kinase inhibitors, or other interventions).
The follow-up protocol consisted of an initial assessment 3 to 6 months after surgery and included physical examination and neck US, as well as serum calcitonin, CEA, and thyrotropin (TSH) measurements. Patients classified as disease free (see the Outcomes subsection below) were scheduled for annual evaluation, while patients with persistent disease were evaluated at least twice per year.
Patient evaluation included physical examination and neck US, as well as serum calcitonin, CEA, and TSH measurements. Patients with calcitonin levels higher than 150 pg/mL underwent additional imaging studies to evaluate distant metastases (skull, cervical, and thorax computed tomography [CT], abdomen magnetic resonance imaging/CT, and bone scintigraphy). Follow-up duration was defined as the time from thyroidectomy to the last medical visit.
Serum POCal was measured 3 to 6 months after total thyroidectomy. We divided patients according to POCal into two groups: undetectable or detectable calcitonin (below or above the method's detection limit, respectively).
Molecular analysis
Genomic DNA was prepared from peripheral blood leukocytes by standard procedures. RET exons 8, 11, 13, 14, 15, and 16 were analyzed. The DNA fragment of interest was amplified by PCR using specific primers. PCR products were analyzed by gel electrophoresis on 1.5% agarose, purified using the GFX PCR DNA purification kit (GE Healthcare, Buckinghamshire, UK), and submitted to direct sequencing using the Big DyeTM Terminator Cycle Sequencing Ready Reaction Kit (Applied Biosystems, Foster City, CA, USA). 1,21,22
Laboratory analysis
The calcitonin measurement methods have changed over the years as follows: radioimmunoassay (Diagnostic Systems Laboratories-7700) was used from 1997 to 2005 (
Upon implementation of each new technique, the laboratory personnel performed necessary procedures for standardization and validation. TSH levels were measured by electrochemiluminescence immunoassay (ADVIA Centaur XP; Siemens, Tarrytown, NY, USA). For statistical analysis, we considered the reference values for each method in a stratification model that included all measurement methods.
Outcomes
Disease status was defined based on clinical examination, serum calcitonin levels, neck US, and additional imaging tests when indicated. Patients were classified as disease free (undetectable calcitonin and no evidence of structural disease) or having persistent disease. The persistent disease group included patients with biochemical disease (detectable calcitonin without evidence of structural disease), structural disease (evidence of disease on imaging), and disease-related death.
Statistical analyses
Clinical and laboratory data are expressed as the mean (SD) or median and interquartile range (IQR) for continuous variables and absolute numbers and percentages for categorical variables. We performed comparative analyses using unpaired Student's t-test, Mann–Whitney U test, or chi-square test. We estimated survival using the Kaplan–Meier method and compared survival curves across groups with the log-rank test.
We investigated the factors associated with disease status during follow-up by grouping patients into disease-free survival or persistent disease groups. Age at diagnosis, sex, form of the disease, preoperative calcitonin level, POCal, multifocality, tumor size, lymph node metastasis, and distant metastasis were evaluated as MTC prognostic factors using univariate and multivariate regression analyses.
Results
Sample population
Three hundred thirty-four patients were included in the study. The mean age at diagnosis was 41.1 ± 18.6 years, 202 patients (60.5%) were female, and 167 patients (50.0%) had sporadic disease. The median tumor size was 2.0 cm (IQR = 1.1–3.5); 164 patients (49.1%) had lymph nodes and 63 patients (18.9%) had distant metastasis at diagnosis. Multifocal tumors accounted for 96 (28.7%) of cases and 43 (12.9%) cases were associated with C cell hyperplasia.
The clinical and oncological features of patients are shown in Table 1. One hundred sixty-seven (50.0%) patients had sporadic disease and 139 (41.6%) had hereditary MTC. MEN2A was diagnosed in 120 patients from 39 independent kindreds. Nineteen individuals presented the MEN2B syndrome, 13 of whom had a de novo mutation in codon 918. Table 2 shows the identified RET pathogenic variants.
Clinical and Oncological Features in Medullary Thyroid Carcinoma Patients
Data are presented as mean ± SD or median and interquartile range unless otherwise indicated.
Data available for 326 patients.
Data available for 306 patients.
Data available for 181 patients.
Data available for 213 patients.
Data available for 204 patients.
Data available for 249 patients.
Data available for 311 patients.
Data available for 313 patients.
Data available for 321 patients.
Distribution of Families and Affected Individuals According to RET Pathogenic Variants in Hereditary Medullary Thyroid Carcinoma
RET, REarranged during transfection.
Postoperative serum calcitonin
Serum POCal levels were available for 334 patients. At the first postoperative evaluation, 141 patients (42.2%) had undetectable POCal, whereas 193 (57.8%) had detectable POCal (median = 190.0 pg/mL [IQR = 41.8–987.3]).
The clinical and oncological features of patients with detectable versus undetectable POCal are shown in Table 3. Univariate analysis indicated that the group with undetectable POCal had a higher proportion of females (p < 0.001), more patients diagnosed by molecular screening (p < 0.001), a higher proportion of patients with C cell hyperplasia (p = 0.001), lower levels of preoperative calcitonin (p < 0.001), smaller tumors (p = 0.02), and a lower proportion of patients with lymph node metastasis (19.9% vs. 70.5%, p < 0.001). No patient with undetectable POCal had distant metastasis (0% vs. 32.6%, p < 0.001).
Clinical and Oncological Features of 334 Medullary Thyroid Carcinoma Patients in the Undetectable and Detectable Postoperative Calcitonin Groups
Data are presented as median and interquartile range unless otherwise indicated.
Patients with stable persistent biochemical disease.
51 Patients with biochemical disease, 61 patients with structural disease, and 63 disease-related deaths.
POCal, postoperative calcitonin.
Data on the final disease status were available for 334 patients, 141 in the undetectable POCal group and 193 in the detectable POCal group. After a median follow-up of 8.5 years (IQR = 2.0–13.8), 127 (90.1%) patients with undetectable POCal were disease free, whereas 14 (9.9%) had persistent biochemical disease. No patient in the undetectable POCal group progressed to structural disease or disease-related death. All 14 patients with undetectable POCal and persistent biochemical disease persisted with low and stable calcitonin levels after 11.6 years (IQR = 9.89–16.3) of follow-up (Fig. 2A–C).
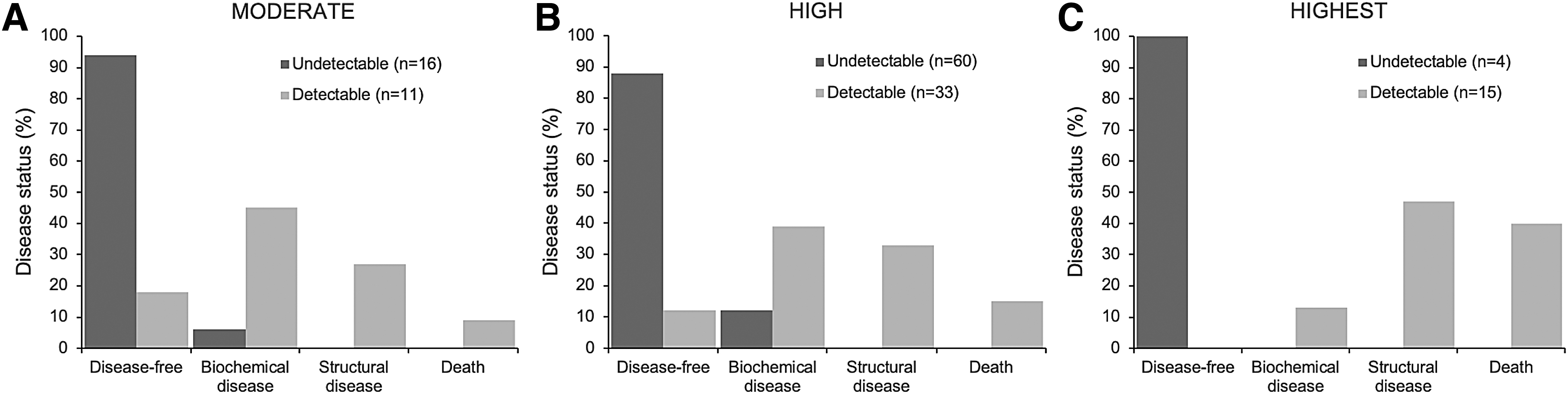
Disease status according to the American Thyroid Association's RET pathogenic variant risk: moderate (
In the detectable POCal group (n = 193), after a median follow-up of 7.0 years (IQR = 2.1–12.6), 18 patients (9.2%) were classified as disease free (11 patients [57.8%] converted spontaneously and 7 [42.2%] underwent additional surgical procedures, 2 of them associated with external radiotherapy), 51 (26.6%) as biochemical disease, 61 (31.6%) as structural disease, and 63 (32.6%) died of disease-related events. Undetectable POCal remained associated with a long-term disease-free status independent of the American Thyroid Association (ATA) RET pathogenic variant risk category (Fig. 2A–C).
As the proportion of hereditary MTC in this study was high (42%), we further analyzed the clinical and oncological features according to hereditary or sporadic disease (Table 4). Patients with hereditary disease were younger at diagnosis (p < 0.001) and had lower preoperative calcitonin levels (p = 0.002), small tumor sizes (p < 0.001), higher rates of C cell hyperplasia (p < 0.001) and tumor multifocality (p < 0.001), and lower rates of lymph node or distant metastasis. Accordingly, the proportions of patients with detectable POCal (p < 0.001) and persistent disease/deaths (p = 0.012) were lower in the hereditary group.
Clinical and Oncological Features of Medullary Thyroid Carcinoma Patients in the Sporadic and Hereditary Disease Groups
Data are presented as mean ± SD or median and interquartile range unless otherwise indicated.
Data available for 306 patients.
Table 5 shows the univariate analyses of prognostic factors for disease-free survival in MTC patients. Younger age at diagnosis, female sex, hereditary disease, preoperative calcitonin levels, small tumor size, absence of lymph node, absence of distant metastasis, and undetectable POCal were all associated with disease-free survival (all p < 0.01).
Univariate and Multivariate Analyses of Prognostic Factors for Disease-Free Survival in Medullary Thyroid Carcinoma Patients
Data are presented as median (interquartile range) unless otherwise indicated.
Data available for 326 patients.
Data available for 306 patients.
Data available for 181 patients.
Data available for 213 patients.
Data available for 249 patients.
Data available for 311 patients.
Data available for 313 patients.
Further analysis using a multivariate model, with disease-free status as a dependent variable and age at diagnosis, sex, hereditary disease, tumor size, absence of lymph node, and undetectable POCal as independent variables, identified undetectable POCal and younger age at diagnosis as the only independent prognostic factors for disease-free status, with the strongest association for undetectable POCal (Table 5).
It was not possible to include the variable—absence of distant metastasis—in the multivariate analysis model because some events had zero occurrences (no patients with distant metastasis with undetectable POCal or disease-free status).
Survival analysis
After a median follow-up of 7.7 years (IQR = 2.1–13.2), the disease-related death rate was 18.9% (63 patients). Most patients died in the first 10 years of disease (65.8%), and all deaths occurred in patients with detectable POCal (Fig. 3A, B). Undetectable POCal was associated with disease survival, irrespective of sporadic or hereditary disease (Fig. 3C, D).
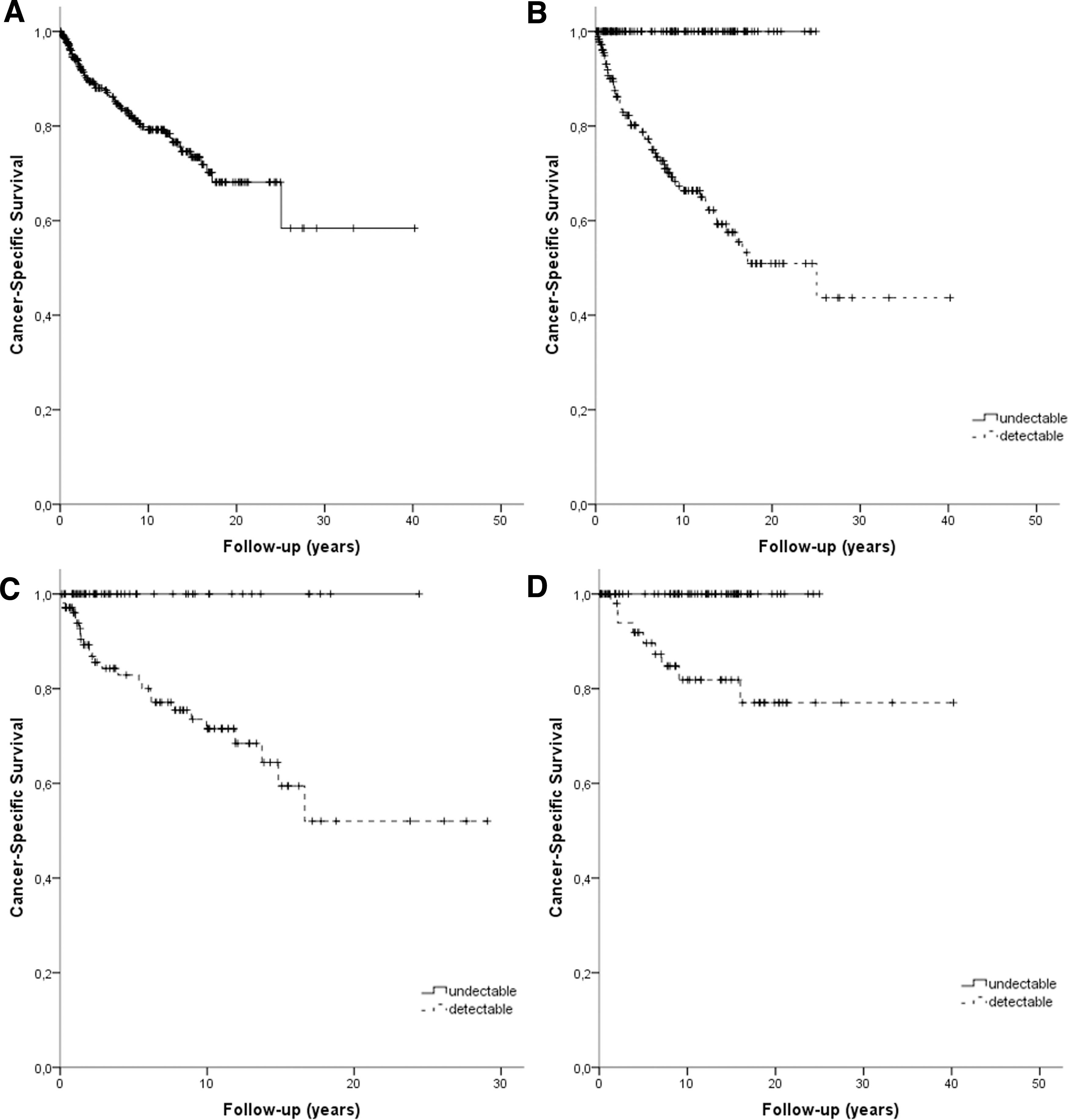
Kaplan–Meier survival curves of patients with medullary thyroid cancer. (
Discussion
The best strategic therapeutic approach for the follow-up of MTC patients remains a matter of debate, particularly for those with low or undetectable calcitonin levels after the surgical procedure. In this study, we show that all patients with undetectable POCal remained disease free or evolved to stable biochemical disease at long-term follow-up. Remarkably, undetectable POCal remained associated with a long-term disease-free status in patients with sporadic or hereditary disease, independent of the ATA RET pathogenic variant risk category.
Well-known prognostic factors for unfavorable MTC outcomes include older age at diagnosis, extrathyroidal invasion, cervical lymph node metastasis, distant metastasis, delayed or incomplete surgical treatment, and calcitonin and CEA doubling times. 3 –5,8 –10 A dynamic risk stratification system based on the best response to initial therapy has been proposed to modify the initial risk estimates by classical TNM staging. 10,23,24
Tuttle et al initially proposed the dynamic risk stratification system for differentiated thyroid carcinoma, showing that updated risk estimates allow tailoring the intensity of follow-up and interventions, providing state-of-the-art individualized management recommendations. 24
Lindsey et al evaluated the response to initial therapy and outcome in 284 MTC patients. 23 The authors observed a recurrence rate of only 4% among patients who achieved an excellent response to initial therapy, in contrast to a death rate of 54% among those with incomplete structural response to initial treatment. However, the median follow-up of 5 years can be insufficient to draw major conclusions due to the indolent nature of the disease. 23
Kwon et al conducted a similar study to evaluate the response to initial therapy and disease status at final follow-up in 120 patients with MTC. Patients with excellent response showed the highest likelihood of achieving disease-free status (88%). In contrast, no patients in the structural incomplete response group had disease-free status after a median 6.2-year follow-up. 10
The present study shows that a single POCal measurement might predict long-term disease status in MTC patients. Remarkably, among patients who had undetectable POCal, 90.1% were disease free and 9.9% had biochemical disease after a median follow-up of 8.5 years. No patient progressed to structural disease or disease-related death. In contrast, in patients with detectable POCal, 9.2% progressed to disease-free status, 26.6% had a persistent biochemical disease, 31.6% had structural disease, and 32.6% died of disease-related events after a median follow-up of 7.0 years.
Of note, previous studies have reported 75–80% agreement between undetectable POCal and disease-free status at the final follow-up using serum calcitonin levels of <5–10 pg/mL as cutoff values for excellent response to initial therapy. 10,23,24 In this study, only patients with calcitonin levels below the detection limit of each method were considered to have undetectable POCal, which may explain the slight difference in results.
We believe that using a more stringent cutoff value based on the detection method increases our data's reproducibility and external validity. Calcitonin doubling time is an independent and broadly used predictor of MTC prognosis, but it requires calculation of at least four measurements over two years. 3,12,13
The survival rates for MTC are lower than those for differentiated thyroid cancers. 25 Mathiesen et al reported 5-, 10-, 15-, and 20-year MTC disease-specific survival rates of 82%, 75%, 71%, and 69%, respectively. 11 Another representative study of MTC patients showed 5- and 10-year survival rates of 86% and 68%, respectively. 26 We observed rates slightly above those reported in previous studies, 88% and 80% at 5 and 10 years, respectively.
Our institutions are reference centers for genetic MTC screening, so our cohort presents a higher than expected proportion of hereditary tumors. As shown in Table 5, a large proportion of those patients are diagnosed at earlier phases of the disease, which might explain the better survival rates. Accordingly, hereditary disease was significantly associated with disease-free survival in the univariate analysis, but not in the multivariate model. Undetectable POCal remained associated with long-term disease survival, irrespective of sporadic or hereditary disease.
The retrospective design is a limitation of this study. Nevertheless, it included a large cohort of patients followed up at referral centers by multidisciplinary teams with expertise in MTC, which ensures a similar therapeutic approach and follow-up strategy, thereby enhancing the validity of our data. The extent of surgery was surgeon dependent, and a large number of patients were referred to us after surgery, which might have affected disease outcomes.
However, it does not jeopardize the conclusions on the POCal prognostic role in long-term disease-free survival. The fact that we employed various calcitonin measurement methodologies with distinct reference values over time may also be a potential limitation. Particularly, the low detection sensitivity of earlier calcitonin assays might have interfered with the initial classification of some disease-free patients who later converted to biochemical disease.
Notwithstanding, we understand that this approach enhances the external validity of our findings given that (i) in clinical practice, multiple calcitonin methods coexist; (ii) each new calcitonin measurement methodology is validated against the previous one; and (iii) the results are based on specific reference values.
Conclusions
In conclusion, undetectable POCal is an independent predictor of disease-free survival in patients with MTC. Since POCal could predict the rate of disease remission and the risk of persistent biochemical/structural disease, it might also reduce the “over follow-up effect” with unnecessary surveillance, diagnostic tests, and medical appointments.
From a practical standpoint, it may contribute to identifying disease-free patients and those who require more careful follow-up at the first postoperative evaluation.
Footnotes
Acknowledgments
This work has been made possible by grants from Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Fundo de Incentivo a Pesquisa (FIPE), and Programa de Apoio a Núcleos de Excelência (PRONEX)/Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (FAPERGS). A part of this work was presented in the XIX Encontro Brasileiro de Tireoide, October 30–31, 2020, and published as an abstract in the Archives of Endocrinology and Metabolism 64, Supp October 1, 2020.
Authors' Contributions
M.A.S.D. was involved in conceptualization (supporting), formal analysis, funding acquisition, and writing—original draft (lead). C.V.F. was involved in conceptualization (supporting), data scrubbing and maintenance of research data, formal analysis, and writing—original draft (lead). L.M. and A.B.Z. were involved in data scrubbing and maintenance of research data and data/evidence collection. J.M.D. was involved in conceptualization (supporting) and formal analysis. M.E., A.F.B., D.B., F.A.A., and P.A.A.J. were involved in data/evidence collection. M.V.C. was involved in data scrubbing and maintenance of research data and genetic analysis. R.C. was involved in data/evidence collection and supervision. F.V. was involved in conceptualization (supporting), data/evidence collection, and supervision. R.S.S. was involved in conceptualization (supporting), formal analysis, and writing—review and editing. A.L.M. was involved in conceptualization (lead), formal analysis, funding acquisition, and writing—review and editing.
Author Disclosure Statement
M.A.S.D., L.M., J.M.D., M.E., A.F.B., M.V.C., D.B., F.A.A., P.A.A.J., R.C., and A.B.Z. have nothing to disclose. C.V.F. has served as a study coordinator in multicenter studies for Sanofi-Genzyme, Exelixis, and Lilly within the past two years. F.V. has served as the principal investigator in multicenter studies for Exelixis, Bayer, Ipsen, and Lilly and Speaker of United Health, Bayer, Ipsen. R.S.S. has served as a subinvestigator in multicenter studies for Sanofi-Genzyme, Exelixis, and Lilly within the past two years. A.L.M. has served as the principal investigator in multicenter studies for Sanofi-Genzyme, Exelixis, and Lilly within the past two years.
Funding Information
M.A.S.D. was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Fundo de Incentivo à Pesquisa (FIPE; n° 2019-0590). C.V.F. was supported by Programa de Apoio a Núcleos de Excelência/Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (PRONEX/FAPERGS; 16/2551-0000486-2). L.M., J.M.D., M.E., M.V.C., D.B., F.A.A., P.A.A.J., R.C., F.V., A.B.Z., and R.S.S. have no funding information to declare. A.F.B. was supported by CAPES. A.L.M. is recipient of scholarship (n° 316323/2021-7) and research grants (No: 408344/2021-0) from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), FIPE n° 2019-0590, and Programa de Apoio a Núcleos de Excelência (PRONEX/FAPERGS; n° 16/2551-0000486-2).