
Abstract
Background:
During treatment for differentiated thyroid carcinoma (DTC), patients go from euthyroidism to severe hypothyroidism to subclinical hyperthyroidism induced by thyroid hormone suppression therapy (THST). Severe hypothyroidism may induce a tendency toward bleeding, whereas hyperthyroidism is thrombogenic. Therefore, treatment for DTC may increase the risk of bleeding during thyroid hormone withdrawal, and thrombosis during THST. This study aims to provide prospective analysis of changes in the hemostatic system from euthyroidism to hypothyroidism, and during THST, in patients treated for DTC.
Methods:
This is a secondary study in a larger Dutch prospective cohort. Consecutive samples were obtained from 20 patients (18 female [90%]; median age 48 [interquartile range 35.8–56.5] years) throughout their treatment for DTC during euthyroidism (n = 5), severe hypothyroidism (n = 20), and THST (n = 20). We measured selected hemostatic proteins and C-reactive protein (CRP), performed functional tests of hemostasis (a thrombin generation test and a plasma-based clot lysis test), and assessed markers of in vivo activation of hemostasis (thrombin–antithrombin complexes, plasmin–antiplasmin [PAP] complexes, and D-dimer levels).
Results:
During hypothyroidism, the majority of measured parameters did not change. During THST, plasma levels of nearly all measured hemostatic proteins were higher than during hypothyroidism. Additionally, CRP significantly increased from 1.3 (0.5–3.3) to 3.2 (1.3–5.1) mg/L during THST (p < 0.01). Ex vivo thrombin generation increased from 626.0 (477.0–836.3) to 876.0 (699.0–1052.0) nM × min (p = 0.02), and ex vivo clot lysis time increased from 60.6 (55.6–67.4) to 76.0 (69.7–95.0) minutes during THST (p < 0.01). PAP levels reduced from 266.5 (211.8–312.0) to 192.0 (161.0–230.0) μg/L during THST (p < 0.01); other markers of in vivo activation of coagulation remained unaffected.
Conclusions:
During THST-induced hyperthyroidism, a shift toward a more hypercoagulable and hypofibrinolytic state occurred. However, in vivo activation of hemostasis did not increase. The rise in CRP levels suggests the presence of a low-grade inflammation in patients during THST. Both a hypercoagulable and hypofibrinolytic state and a low-grade inflammation are associated with an increased risk of cardiovascular diseases (CVD). Therefore, the subtle changes found during THST could potentially play a role in the pathogenesis of CVD as observed in DTC patients.
Clinical Trial Registration:
This study is part of a larger clinical trial registered at the Netherlands Trial Register (NTR ID 7228).
Introduction
During treatment for differentiated thyroid carcinoma (DTC), patients are exposed to unphysiological thyroid hormone (TH) levels, which can have adverse cardiovascular effects. In DTC patients, each 10-fold decrease in mean thyrotropin (TSH) level is independently associated with a 3.1-fold increase in cardiovascular mortality. 1 However, the relevant pathophysiological mechanism remains largely unknown. Therefore, interest is increasing regarding how different aspects of DTC treatment may contribute to the risk of cardiovascular diseases (CVD). Treatment for high-risk DTC generally consists of a thyroidectomy, a period of TH withdrawal to enable ablation with radioactive iodine (131I; RAI), followed by thyroid hormone suppression therapy (THST). During this treatment, patients go from euthyroidism to hypothyroidism to subclinical hyperthyroidism within a few weeks. As TH levels influence gene transcription of hemostatic proteins in endothelial and hepatic cells, abnormal TH levels are associated with changes in hemostasis. 2,3
Hypothyroidism is associated with a risk of bleeding. 4,5 Studies mainly including patients with autoimmune hypothyroidism indicate that hypothyroidism causes a prolonged skin bleeding time, prolongations in clotting tests such as the prothrombin time and activated partial thromboplastin time, 4,6 impaired platelet function as measured with the platelet function analyser (PFA-100), 7 and low levels of von Willebrand factor (VWF) and factor (F)VIII. 5,6 In addition, hypothyroidism is associated with a shortening of plasma-based clot lysis time (CLT). 8 Changes in tissue plasminogen activator (tPA) and plasminogen activator inhibitor-1 (PAI-1) have been reported, but with contradictory results. 4 Clinical effects of hypothyroidism are easy bruising, mucocutaneous bleeding, and menorrhagia; indeed, even major bleeding problems necessitating blood transfusion have been reported. 4,5
Conversely, hyperthyroidism caused by (auto-)inflammatory conditions or exogenous administration of TH to healthy volunteers induces a hypercoagulable and hypofibrinolytic state. 9,10 Platelet function measured with the PFA-100 is enhanced, 7 and increased levels of VWF, 6,7,9,11 fibrinogen, 9,11,12 FVIII, 7,9,11 and FIX 9,11 have been reported. Fibrinolysis is impaired, as indicated by a prolonged CLT, 11 as well as increased plasma levels of PAI-1 9,11,13 and thrombin-activatable fibrinolysis inhibitor. 8 In addition, in a Mendelian randomization study, genetically increased free thyroxine (fT4) may be associated with increased synthesis of VWF. 14
TH level-related changes in hemostasis also occur in patients treated for DTC. 15 –17 During TH withdrawal in 22 DTC patients, decreased levels of VWF and FVIII have been reported. 15 Furthermore, in 2 studies with respectively 20 and 90 DTC patients, 16,17 THST was associated with prothrombotic changes. However, as data on fibrinolytic factors and functional hemostatic changes in DTC are incomplete, the extent and clinical relevance of changes in hemostasis during treatment for DTC remain unclear.
We aim to provide further insight into hemostatic changes during treatment for DTC by measuring hemostatic parameters, ex vivo function, and in vivo activation of hemostasis during euthyroidism, hypothyroidism, and subclinical hyperthyroidism.
Materials and Methods
Study population
In this prospective cohort study, patients with a histopathologically confirmed DTC, between 18 and 75 years old, and treated at the University Medical Center of Groningen (UMCG), Groningen, the Netherlands, were eligible to participate. Treatment was offered according to the Dutch guidelines for DTC treatment. 18 Exclusion criteria were as follows: history of cerebrovascular or coronary events, atrial fibrillation, heart failure, pregnancy, diagnosis of an additional malignancy, treatment with recombinant human TSH, and treatment deviating from standard protocol. Where possible, an extra visit during euthyroidism (V0) took place with patients who had initially undergone a hemithyroidectomy but for whom, after histopathologically confirmed DTC, a completion thyroidectomy was indicated. For these subjects, an extra exclusion criterion was the use of TH medication. All eligible patients treated between October 2016 and August 2018 were invited to participate, and all participants gave written informed consent.
This study is a preplanned secondary study part of a larger Dutch clinical trial evaluating cardiovascular effects of hypothyroidism and hyperthyroidism during treatment for DTC. This trial was powered on the primary endpoint measured with cardiac magnetic resonance imaging. 19 This clinical trial was approved by the Medical Ethics Committee (METc) of the UMCG (Registration No. 2015/116) and registered at the Netherlands Trial Register (NTR ID 7228).
Study visits
This study consisted of three outpatient study visits. The first study visit (V1) took place 4–6 weeks after patients had undergone a total or completion thyroidectomy, and 1 day before RAI therapy. Between the thyroidectomy and RAI, patients received no thyroid medication and were therefore hypothyroid during V1. After RAI, THST was started, with liothyronine (75 μg daily) or levothyroxine (150–200 μg daily), aimed at achieving TSH suppression. Study measurements were repeated 10 (V2) and 20 weeks (V3) after initiation of THST. TSH was targeted at ≤0.10 mU/L, comparable to a state of subclinical hyperthyroidism. If possible, an extra visit (V0) during euthyroidism was included, before a completion thyroidectomy. An overview of the study timeline can be found in the Supplementary Data S1.
Study definitions
Medical records were used to retrieve medical history, therapy details, histopathological data, and data on disease progression. Treatment was based on Dutch risk stratification, dividing patients into a low-risk group and a not-low-risk group. 18 Tumors were staged in accordance with the eighth edition of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) tumor–node–metastasis (TNM) classification. 20 Tumor risk classification was based on the 2015 American Thyroid Association (ATA) Guidelines for Adult Patients with Thyroid Nodules and DTC. 21
Laboratory methods
During all study visits (V0, V1, V2, and V3), blood was taken in the morning after an overnight fast. Immediately after blood was drawn, plasma levels of TSH were assayed in all samples, and from V0, V1, and V3, plasma levels of VWF, FVIII, D-dimer, and C-reactive protein (CRP) were determined in citrated plasma. Remaining samples were prepared by double centrifugation at 2000 g for 10 minutes, and 10,000 g for another 10 minutes. Blood plasma was stored in 1 mL tubes and frozen at −80°C until batch analysis. For logistical reasons, batch analysis was performed on samples from V0, V1, and V2. Parameters analyzed from these samples were fibrinogen, FV, FIX, FXI, FXII, tPA, PAI-1, thrombin generation assay, plasma-based CLT, thrombin–antithrombin (TAT) complexes, and plasmin–antiplasmin (PAP) complexes.
Selected hemostatic and fibrinolytic parameters
Fibrinogen was determined with the Clauss fibrinogen assay on an ACLTOP 550 coagulation analyzer, using HemosIL Q.F.A. Thrombin Fibrinogen Kit (Werfen, Barcelona, Spain). VWF–antigen levels were determined with an enzyme-linked immunosorbent assay (ELISA) with reagents from DAKO/Agilent (CA). FVIII, FIX, FXI, and FXII were analyzed using a one-stage coagulation assay on a CS-2100i coagulation analyzer with activated partial thromboplastin time reagents and factor-deficient plasma (Siemens, Marburg, Germany). For FV, a similar coagulation assay was used, based on the prothrombin time (PT) and determined on a CS-2100i coagulation analyzer with PT and factor-deficient plasma (Siemens, Marburg, Germany). PAI-1 and tPA were determined by ELISAs using Asserachrom PAI-1 Kit and Asserachrom tPA-KT from STAGO (Asnières sur Seine Cedex, France).
Ex vivo function of hemostasis and fibrinolysis
Thrombin generation was measured using calibrated automated thrombinography in clotting plasma in the presence of soluble thrombomodulin, as previously described. 22 Plasma fibrinolytic capacity was estimated by studying lysis of a clot by exogenous tPA, and monitoring formation and subsequent lysis of the clot, as previously described. 23
In vivo activation of hemostasis and fibrinolysis
Plasma levels of TAT (Siemens, Den Haag, Netherlands) and PAP (Technoclone, Vienna, Austria) were quantified using commercially available ELISAs. TAT complexes reflect in vivo thrombin generation and activation of coagulation, whereas PAP complexes reflect in vivo plasmin generation and activation of fibrinolysis. D-dimer was determined using a Roche Modular P Analyzer (Roche Diagnostics, Manheim, Germany).
Other measured parameters
TSH was assayed in serum using the Roche Modular E170 Analyzer (Roche Diagnostics). CRP was determined with a particle-enhanced immunoturbidimetric assay using the Roche Modular C501 Analyzer (Roche Diagnostics).
Statistical analysis
Parameters were analyzed using either a paired T-test or the Wilcoxon signed-rank test for paired data, as appropriate. Data are presented as median (interquartile range). The V2 and V3 groups were merged as some parameters were already measured from samples taken at V3, while only samples from V2 were available for measurements of additional parameters. Two separate analyses were performed, one comparing V0 with V1 and one comparing V1 with either V2 or V3, depending on which parameter was available. Two-sided p-values of <0.05 were considered statistically significant. SPSS 23 (version 23.0; IBM Corp., Armonk, NY) was used for data analysis. The differences in relative change between medians of measured parameters from V1 to V2/V3 were calculated in percentages.
Results
Characteristics of the study population
For this study, 27 patients participated; a total of 20 patients completed the study, including 5 who participated in the extra measurement (V0) (Fig. 1). Six patients withdrew from the study because they found participation along with their regular DTC treatment too demanding. One patient was not taking thyroid medication during V3 and was included in the analysis of samples from V0, V1, and V2. One patient was not taking thyroid medication during V2 and was excluded. Samples from 4 patients from V2 had been stored inadequately and were not measurable; therefore, only samples from 15 patients from V2 could be measured. Ultimately, 5 patients were analyzed during euthyroidism (V0) and 20 patients were analyzed during hypothyroidism (V1). During THST-induced hyperthyroidism, parameters from V2 were measured in 15 patients, and parameters from V3 were measured in 20 patients.
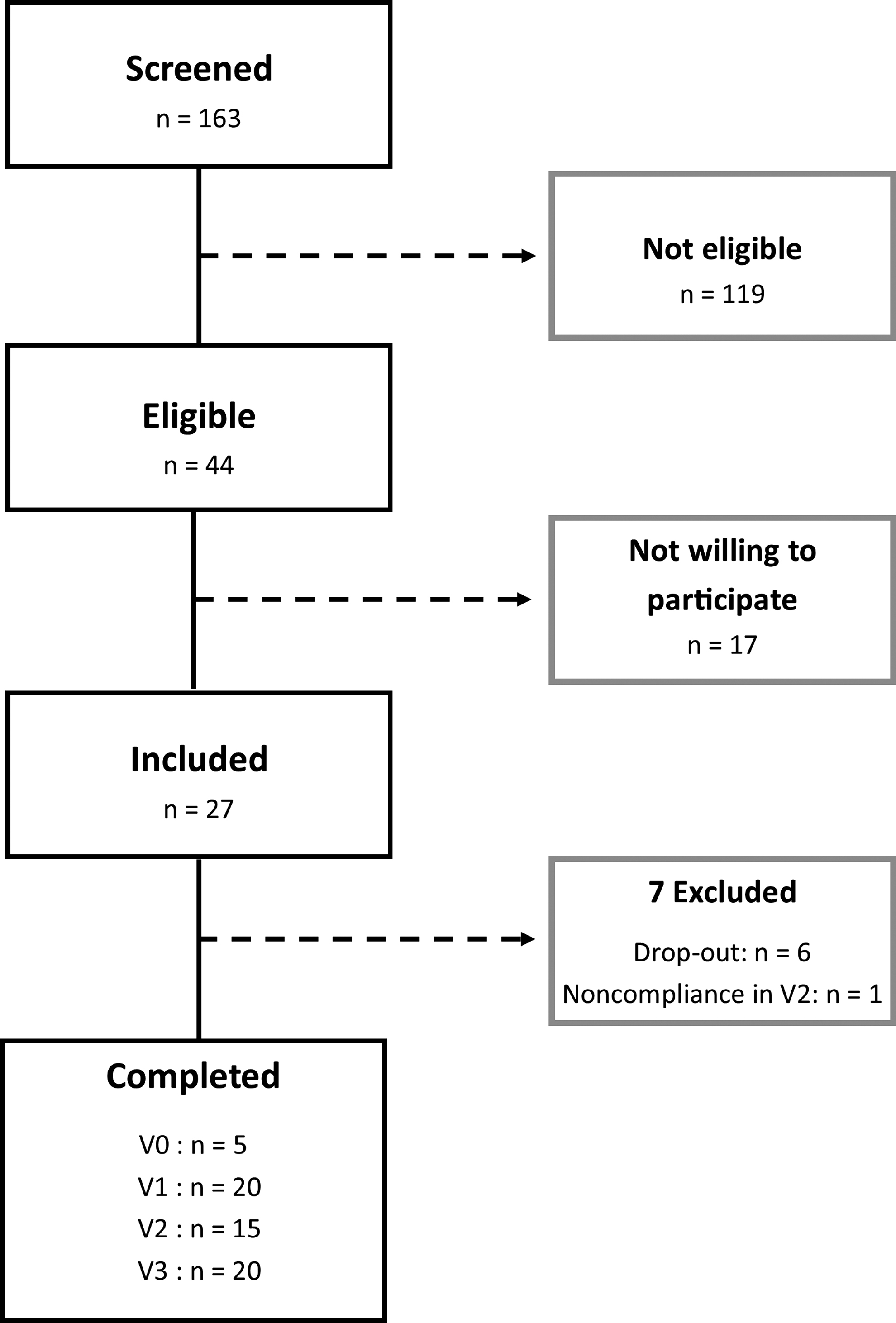
Flow of participants throughout the trial. One hundred four patients received thyroid surgery for (suspected) DTC, from which 44 were eligible for participation. Seventeen patients were not willing to participate, and 27 patients were initially included. From this, 6 patients withdrew from the study and 1 patient did not take thyroid hormone medication during study visit 2. A total of 5 patients were included for the extra visit during euthyroidism (V0), 20 patients were analyzed during hypothyroidism (V1), and during THST (V2 and V3), samples from 15 and 20 patients were analyzed, respectively. Completed study visit 1–3. DTC, differentiated thyroid carcinoma; THST, thyroid hormone suppression therapy.
The characteristics of the study population are reported in Table 1. Their median age was 48.5 years. Sixteen patients were diagnosed with papillary thyroid carcinoma (PTC), and four patients were diagnosed with follicular thyroid carcinoma (FTC). None of the included patients had distant metastases. The mean follow-up was 7 (4.0–15.0) weeks between V0 and V1, 10 (9.0–10.0) weeks between V1 and V2, and 9.5 (9.0–10.0) weeks between V2 and V3. The characteristics of the study population compared with excluded patients can be found in the Supplementary Data S2.
Characteristics of the Study Population
Data are presented as n (%) or median (IQR).
Only including oral contraceptives containing estrogen.
One patient had a history of VTE; this patient used a vitamin K antagonist.
ATA, American Thyroid Association; BMI, body mass index; IQR, interquartile range; TNM, tumor–node–metastasis; VTE, venous thromboembolism.
Selected hemostatic and fibrinolytic parameters
After TH withdrawal, plasma levels of FVIII and FXI were decreased, and FXII levels were increased compared with euthyroid values (Table 2 and Fig. 2). We did not demonstrate changes in other measured hemostatic and fibrinolytic parameters. After 10–20 weeks of THST, significant changes (p < 0.01) were observed in plasma levels of VWF (median relative change 79.0%), fibrinogen (28.2%), FV (9.9%), FVIII (53.2%), FIX (28.2%), and FXI (32.4%) compared with levels measured after TH withdrawal (Table 3 and Fig. 2). Plasma levels of FXII were decreased with a median relative change of 5.5% (p < 0.01) after 10 weeks of THST compared with values after TH withdrawal. Levels of fibrinolytic parameters tPA and PAI-1 showed a median relative increase of respectively 22.7% and 82.7% after 10 weeks of THST (p < 0.01).
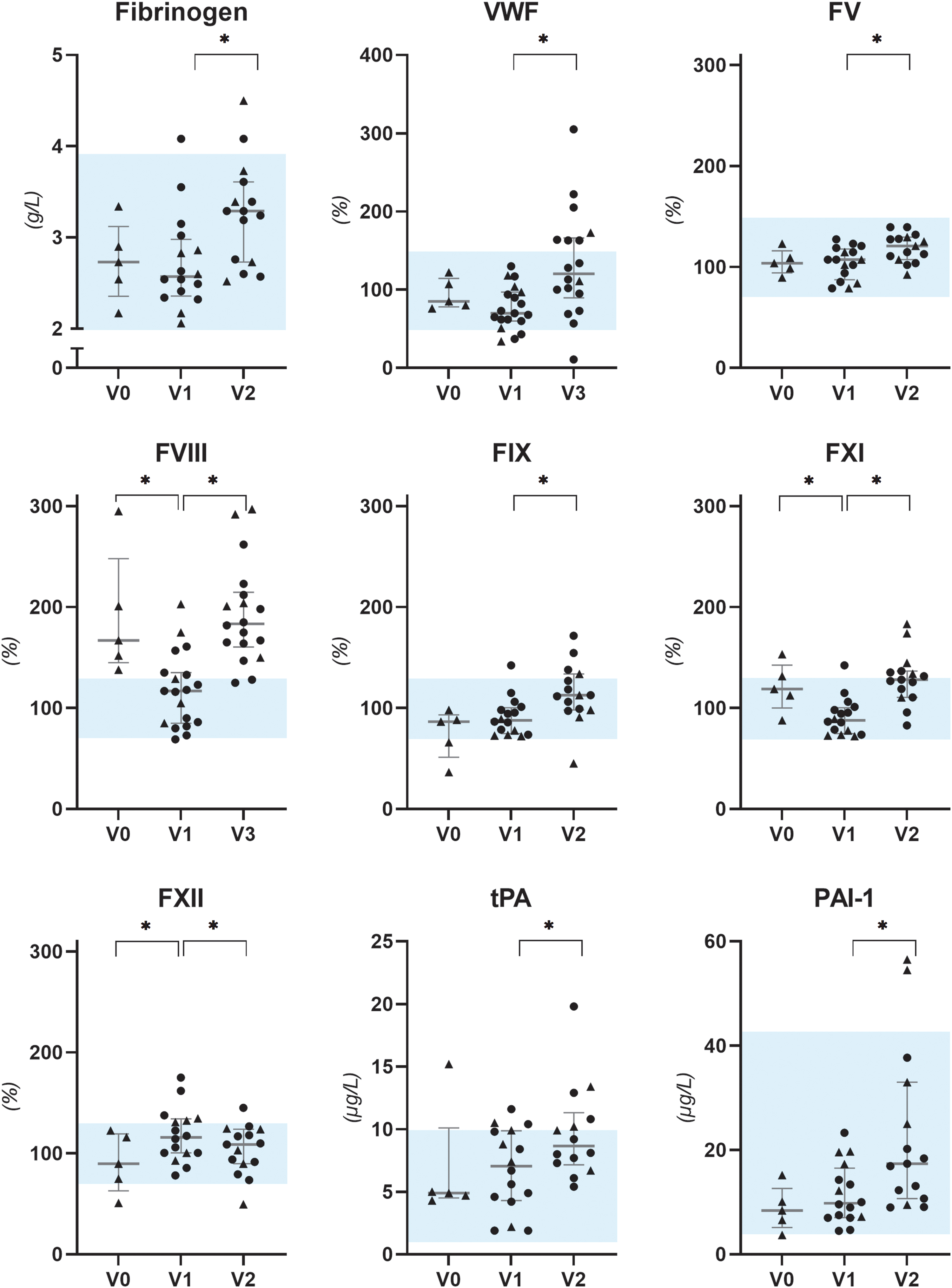
Scatter plots with median (IQR) of measured hemostatic parameters. Parameters were measured during euthyroidism (V0, n = 5), after 4–6 weeks of TH withdrawal (V1, n = 20), and after 10 or 20 weeks of TSH suppression therapy (V2, n = 15 and V3, n = 20). Significance is shown as *p < 0.05. Blue areas represent reference values. Note that the data in this figure are merged from two separate analyses; the comparison between V0 to V1 and V1 to V2/3 entailing only 5 patients, and the comparison between V1 and either V2 or V3 entailing 15 or 20 patients, respectively. So, while the groups overlap, they are not completely the same. Therefore, the triangles represent the comparison between V0 to V1 and V1 to V2/3 (n = 5), and the rounds represent the patients only participating in V1 and V2/V3. The triangles in V1 and V2/3 overlap and are included in the comparison between V1 and V2/3. F, factor; IQR, interquartile range; PAI-1, plasminogen activator inhibitor-1; TH, thyroid hormone; tPA, tissue plasminogen activator; TSH, thyrotropin; VWF, von Willebrand factor.
Changes in Hemostatic and Fibrinolytic Parameters in Differentiated Thyroid Carcinoma Patients Throughout Their Treatment for Differentiated Thyroid Carcinoma Experiencing Euthyroidism, Hypothyroidism, and Thyroid Hormone Suppression Therapy-Induced Subclinical Hyperthyroidism
Parameters were measured during euthyroidism, after 4–6 weeks of TH withdrawal, and after 10 or 20 weeks of TSH suppression therapy. Data are presented as median (IQR).
p-Values represent comparison of euthyroid values and hypothyroid values.
Relative change and p-values represent comparison of hypothyroid values and values during THST, comparable to a state of subclinical hyperthyroidism.
These parameters were measured after 10 weeks of THST.
CLT, clot lysis time; CRP, C-reactive protein; ETP, endogenous thrombin potential; F, factor; PAI-1, plasminogen activator inhibitor-1; PAP, plasmin–antiplasmin complexes; TAT, thrombin–antithrombin complexes; TH, thyroid hormone; tPA, tissue plasminogen activator; THST, thyroid hormone suppression therapy; TSH, thyrotropin; Vel. In., velocity index; VWF, von Willebrand factor.
Changes in Hemostatic and Fibrinolytic Parameters in Differentiated Thyroid Carcinoma Patients Going from Hypothyroidism After Thyroid Hormone Withdrawal to Subclinical Hyperthyroidism Induced by Thyroid Hormone Suppression Therapy
Parameters were measured after 4–6 weeks of TH withdrawal (n = 20) and after 10 or 20 weeks of TSH suppression therapy (n = 15 and n = 20, respectively). Data are presented as median (IQR).
These parameters were measured after 10 weeks of THST; n = 15.
RC, relative change.
Ex vivo function of hemostasis and fibrinolysis
After TH withdrawal, we found no differences in thrombin generation parameters (lag time, velocity index, peak height, endogenous thrombin potential [ETP]) or CLT compared with euthyroid values (Table 2 and Fig. 3). After 10 weeks of THST, ETP levels increased with a median relative change of 40.0% from 626.0 (477.0–836.3) to 876.0 (699.0–1052.0) nM × min (p = 0.02). Although other parameters from the ex vivo thrombin generation tests were numerically higher, they did not achieve statistical significance. Ex vivo CLT showed a median relative increase of 25.4% from 60.6 (55.6–67.4) minutes after TH withdrawal to 76.0 (69.7–95.0) minutes after 10 weeks of THST (p < 0.01).
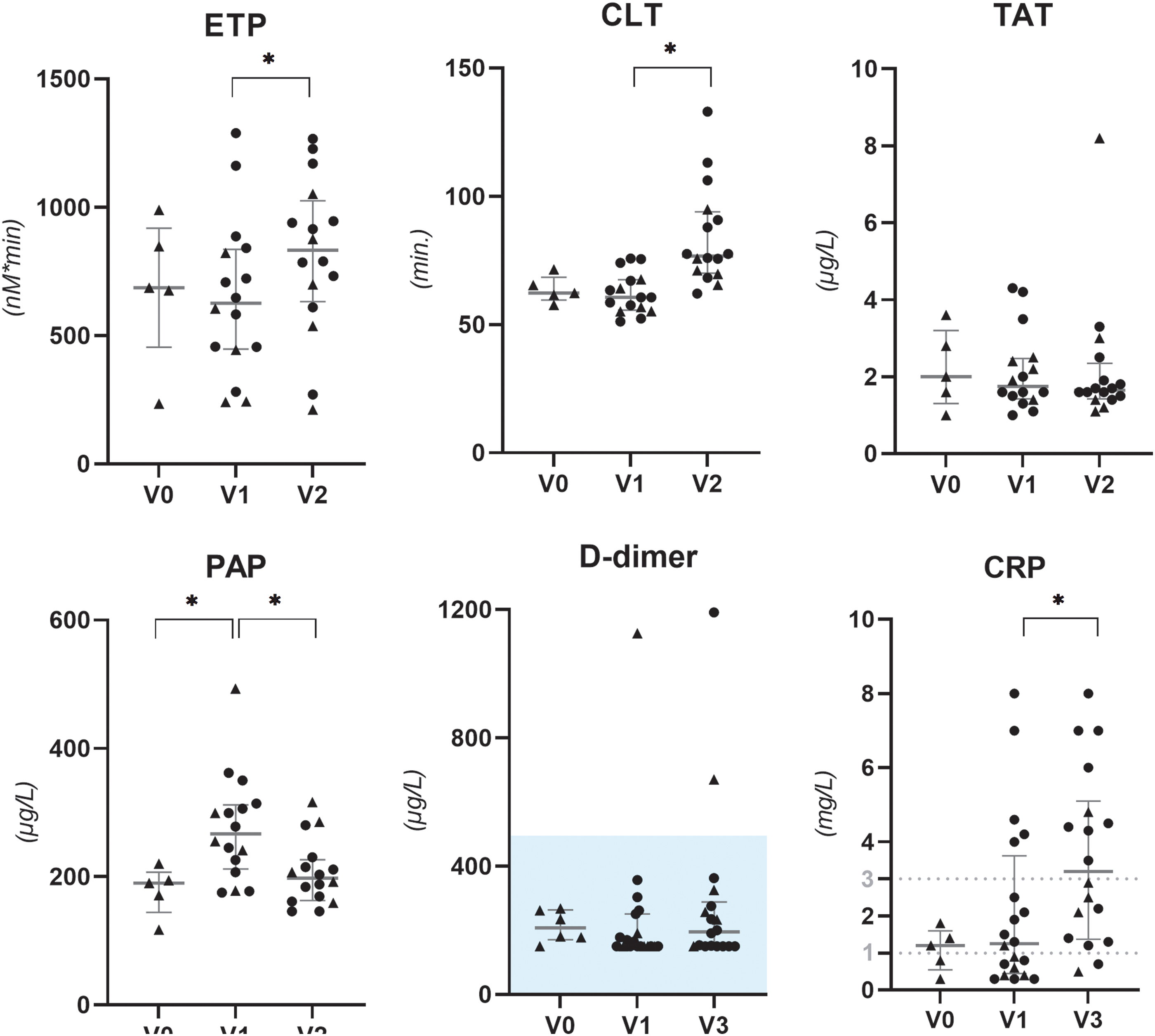
Scatter plots with median (IQR) of ex vivo and in vivo function of hemostasis and CRP. Parameters were measured during euthyroidism (V0, n = 5), after 4–6 weeks of TH withdrawal (V1, n = 20), and after 10 or 20 weeks of TSH suppression therapy (V2, n = 15 and V3, n = 20). Significance is shown as *p < 0.05. Blue areas represent reference values, the lines in the CRP figure represent CRP values associated with moderate (>1 mg/L) and high (>3 mg/L) risk for cardiovascular disease, respectively. Note that the data in this figure are merged from 2 separate analyses; the comparison between V0 to V1 and V1 to V2/3 entailing only 5 patients, and the comparison between V1 and either V2 or V3 entailing 15 or 20 patients, respectively. So, while the groups overlap, they are not completely the same. Therefore, the triangles represent the comparison between V0 to V1 and V1 to V2/3 (n = 5), and the rounds represent the patients only participating in V1 and V2/V3. The triangles in V1 and V2/3 overlap and are included in the comparison between V1 and V2/3. CLT, clot lysis time; CRP, C-reactive protein; ETP, endogenous thrombin potential; PAP, plasmin–antiplasmin; TAT, thrombin–antithrombin.
In vivo activation of hemostasis and fibrinolysis
After TH withdrawal, PAP levels were higher compared with euthyroid values (Table 2 and Fig. 3). After 10 weeks of THST, PAP levels decreased with a median relative change of 28.0% (p < 0.01) (Table 3 and Fig. 3). From euthyroidism to TH withdrawal to THST, TAT and D-dimer levels did not significantly differ.
Other measured parameters
The median TSH values were 81.0 (65.5–100.0) mU/L during TH withdrawal and decreased to 0.02 (0.01–0.09) mU/L after 10 weeks (p < 0.01) (Table 3).The median TSH remained 0.02 (0.01–0.12) mU/L after 20 weeks of THST (not shown in Table 3). After 20 weeks of THST, CRP was significantly increased with a median relative change of 146.2% compared with values after TH withdrawal (p < 0.01) (Table 3 and Fig. 3).
Discussion
The results of this study suggest that THST-induced hyperthyroidism causes a higher thrombogenic potential but does not initiate active coagulation. The increased plasma levels of hemostatic parameters and increased ex vivo function of coagulation demonstrated an increased potential to clot (Fig. 4). However, the in vivo function of hemostasis and fibrinolysis remained unchanged, indicating that the subjects had no active formation nor breakdown of blood clots. After TH withdrawal, during short-term hypothyroidism, measured hemostatic parameters remained largely unaltered compared with euthyroid values (Fig. 4).
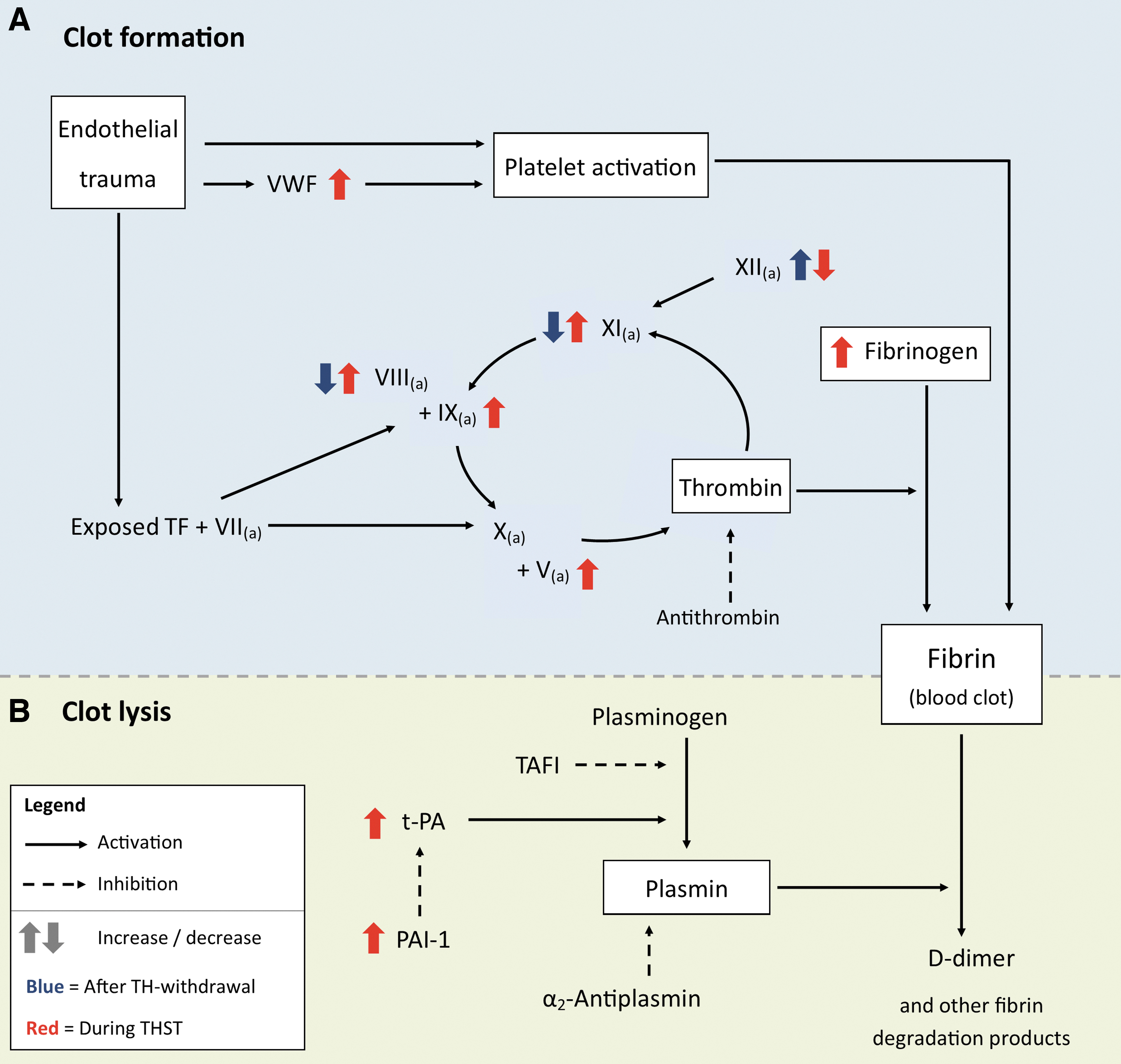
Simplified schematic overview of the coagulation pathway. (
A similar study in DTC patients during TH withdrawal and THST reported comparable increases in plasma levels of procoagulants. 17 Additionally, our study measured ex vivo function of thrombin generation (ETP), demonstrating a shift toward a more procoagulant environment. In our study, the effect on ETP was more pronounced than previously described in a study with 12 healthy volunteers receiving levothyroxine for 14 days. 11 This could be explained by the fact that the change in TSH levels from hypothyroidism to subclinical hyperthyroidism is metabolically more pronounced than in euthyroid volunteers receiving levothyroxine.
A second change during THST was impaired fibrinolysis, indicated by a considerably prolonged CLT. The relatively larger increase of PAI-1 compared with tPA is in line with earlier findings, suggesting that the hypofibrinolytic state during THST results from a shift in the PAI-1:tPA ratio. 16 Despite these alterations, no in vivo activation of coagulation occurred during THST. Therefore, THST may set the stage for a thromboembolic event but seems not to provoke it.
For decades, severe hypothyroidism has been associated with acquired VWD. 24 –27 Studies of hypothyroidism in DTC patients have reported that VWF plasma levels significantly decreased after four to six weeks of TH withdrawal. 15 In our study, the sample size during euthyroidism was too small to detect statistically significant differences. However, VWF levels were numerically lower after TH withdrawal, and a total of 3 patients had plasma VWF levels <50%, compared with none during euthyroidism. VWF levels <50% may cause a small risk of bleeding in some individuals, often in combination with other risk factors. 28
Our research and that of others 16 showed an increase in CRP during THST for DTC. This, along with increases in acute phase proteins VWF, fibrinogen, FVIII, tPA, and PAI-1 and a decrease in FXII, indicates a low-grade inflammatory state. This may result from a direct action of TH on synthesis of inflammatory proteins. 2 However, in healthy volunteers, levothyroxine exposure was not associated with increases in proinflammatory cytokines and inflammatory mediators. 29 The immune and coagulation systems are closely related, and the above results raise the question of which of these systems activates the other. Nevertheless, irrespective of whether the increase in CRP levels is caused by direct or indirect actions of TH, a CRP >1 mg/L is associated with a moderate risk of a future cardiovascular event, and even a high risk if it becomes >3 mg/L. 30,31 These changes could therefore contribute to the increased cardiovascular mortality observed in DTC survivors.
As demonstrated in earlier studies, this prothrombotic environment could indicate a higher clinical risk of deep vein thrombosis (DVT). 23,32 –35 And indeed, an elevated fT4 has been associated with an increased risk of DVT in a case–control study. 36 However, in a second case–control study only including patients with a recent history of DTC, TSH was not a risk factor for DVT. 37 Therefore, the effect of THST on the incidence of DVT remains unclear. Similarly, studies investigating thyroid function and cardiovascular events also showed mixed results. 38,39
The increased risk of CVD established in patients treated for DTC may be attributed partly to changes in coagulation factors, as reported in our study. tPA and PAI-1 are associated with an increased risk of arterial thrombosis. 40,41 Elevated plasma levels of FIX, FXI, and prolonged CLT are associated with ischemic heart disease, and fibrinogen and VWF have even been identified as independent predictors of ischemic heart disease and myocardial infarction. 40 –43 Therefore, cardiovascular risk management remains important for patients during THST. 44
Our study has some limitations. First, because of the small sample size, small differences could have been missed. Second, we included two patients using oral estrogenic contraceptives, and one patient using a vitamin K antagonist; however, performing consecutive measurements with unchanged medication limited any effects on our study outcomes. Additionally, analyses excluding these patients provided comparable results, suggesting limited influence of these medications (Supplementary Data S3). The same applies to potential interference by the malignancy itself, as DTC is a relatively stable tumor, and the follow-up time was short. Third, we measured some hemostatic parameters after 10 weeks of THST and others after 20 weeks of THST. It is unknown whether the duration of THST affects the degree of hemostatic changes. However, as median TSH levels between 10 and 20 weeks of THST were similar, we assume that results from 10 or 20 weeks are comparable. Fourth, we did not extensively measure anticoagulant factors. However, we did measure ETP, which resembles the balance between procoagulants and anticoagulants, and this test has been associated with venous thrombosis risk. 45 Last, we did not conduct long-term measurements of coagulation parameters, although these could be relevant for evaluating risks of thrombosis and CVD. Nevertheless, despite these limitations, we have provided new insights into functional coagulation during treatment for DTC.
In conclusion, we found a higher thrombotic potential during THST, as evidenced by a hypercoagulable and hypofibrinolytic state. However, we did not detect in vivo activation of coagulation and fibrinolysis. Additionally, we observed an acute phase reaction, suggesting a low-grade inflammatory state. Both a hypercoagulable and hypofibrinolytic state and a low-grade inflammation are associated with an increased risk of CVD. Therefore, the subtle changes found during THST could potentially play a role in the pathogenesis of CVD as observed in DTC patients. However, in contrast, during hypothyroidism, we found no pronounced changes in hemostasis.
Footnotes
Acknowledgments
We would like to thank J. Adelmeijer from the Department of Surgery of the University Medical Center Groningen for the laboratory analyses performed in the Surgical Research Laboratory. And, we would like to thank H. Breukelman from the Central Freezer Facility of the University Medical Center Groningen for providing storage of samples.
Institutional Review Board Approval Statement
This study was approved by the Medical Ethics Committee (METc) of the UMCG (Registration No. 2015/116) and registered at the Netherlands Trial Register (NTR ID 7228). We confirm that this study was completed in accordance with the Declaration of Helsinki as revised in 2013.
Author's Contributions
M.H.L.: Formal analysis (lead), data curation (lead), writing of original draft (lead), writing—review and editing (lead), visualization (lead), and final approval of the article (equal). J.D.L.: Conceptualization (lead), methodology (lead), writing—review and editing (supporting), and final approval of the article (equal). T.L.: Formal analysis (supporting), resources (supporting), writing—review and editing (supporting), visualization (supporting), and final approval of the article (equal). T.v.d.B.: Conceptualization (lead), methodology (lead), investigation (lead), data curation (lead), writing—review and editing (supporting), funding acquisition (lead), and final approval of the article (equal). M.V.L.: Resources (supporting), writing—review and editing (supporting), and final approval of the article (equal).
K.M.: Formal analysis (supporting), writing—review and editing (supporting), and final approval of the article (equal). T.P.L.: Conceptualization (lead), methodology (lead), formal analysis (lead), investigation (supporting), writing—original draft (lead), writing—review and editing, visualization (lead), supervision (supporting), and final approval of the article (equal). W.T.Z.: Formal analysis (lead), writing—original draft (lead), writing—review and editing (lead), visualization (lead), supervision (lead), and final approval of the article (equal).
Author Disclosure Statement
M.H.L., J.D.L., T.L., T.v.d.B., M.V.L., T.P.L., and W.T.Z. declare no competing interest. K.M. reports speaker fees from Alexion, Bayer, and CSL Behring, participation in trial steering committee for Bayer, consulting fees from Uniqure, participation in data monitoring, and endpoint adjudication committee for Octapharma. All fees were paid to her institution.
Funding Information
This work was funded by Junior Scientific Masterclass Groningen (to Trynke van der Boom).
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3