
Abstract
Background:
It has been suggested that small metastatic lymph nodes (LNs) detected after initial surgery in patients with differentiated thyroid cancer (DTC) can be managed with active surveillance (AS). However, there is still concern regarding the clinical outcomes of these patients. The main aims of our study were as follows: (1) to assess the frequency of growth and the need of additional treatment in a group of patients with LN recurrences selected for AS, and (2) to determine predictive factors of LN progression.
Methods:
We retrospectively reviewed 856 clinical records from our DTC patient's database (May 2010 to January 2022). Eighty patients had suspicious cervical LNs on consecutive ultrasound (US) after initial surgery, but we included 50 patients with cytological confirmation of metastatic disease and at least 12 months follow-up. Exclusion criteria were as follows: any LN ≥2 cm or multiple LNs ≥1.5 cm in size, proximity to vital structures, PET-positive disease (standard uptake value ≥5), aggressive histology, and distant metastasis. Patients were followed with thyroglobulin (Tg) and thyroglobulin antibodies measurements on suppressive therapy and neck US every 6–12 months. LN growth was defined as an increase of ≥3 mm in any of its diameters.
Results:
A total of 50 patients had a median age of 41 years (range, 18–75). Most patients were women (80%) and had classical papillary thyroid cancer (86%). The mean size of the LNs was 10.1 ± 4.4 mm. After a median follow-up of 29 months (range, 12–144), 12 patients (24%) had an increase in size of the metastatic LN, 7 (58%) of whom were surgically removed. None of these seven patients had a structural incomplete response at the end of follow-up. The only variable that predicted an increase in LN size was a rise in Tg levels ≥0.5 ng/mL (p = 0.016). Based on a multivariate analysis, patients with increase in Tg levels ≥0.5 ng/mL had a significantly higher chance of developing LN growth (odds ratio [OR] 16.2 [confidence interval, CI 1.5–120.2], p = 0.020). The median progression-free survival rate was 6.6 years [CI 5.6–9.5].
Conclusion:
AS of small LNs could be a feasible alternative to immediate surgery in properly selected patients.
Introduction
Up to 30% of patients with differentiated thyroid cancer (DTC) have persistent or recurrent metastatic cervical lymph nodes (LNs) after the initial surgery. 1 This often leads to one or more additional surgeries. Even when these procedures are performed by expert thyroid surgeons, they are associated with a high risk of hypoparathyroidism and vocal cord paralysis owing to recurrent laryngeal nerve injury (up to 19% and 6%, respectively). 2
While the resection of large cervical LNs has been demonstrated to improve long-term prognosis, 3 the clinical benefit of an early intervention in small-volume nodal recurrences is still uncertain. Observational studies suggest that small metastatic LNs detected after initial surgery for DTC can be managed with active surveillance (AS). 4 –6 The decision to follow with mere observation or to perform surgery in these cases should balance the possibility of local complications, surgical risks, and patient anxiety. 7 Therefore, in clinical practice, the timing of salvage surgery is not always clear. Moreover, reports of this AS approach are scarce.
The main aims of our study were: (1) to assess the frequency of growth and the need of additional treatment in a group of patients with LN recurrences selected for AS, and (2) to determine predictive factors for these outcomes. Secondary objectives included to assess the presence of local complications related to tumor growth, the development of distant metastasis, and to estimate the progression-free survival in this cohort.
Methods
Patients
We retrospectively reviewed our database containing 856 records of patients with DTC who were followed from May 2010 to May 2020 in the Division of Endocrinology, Hospital de Clínicas-University of Buenos Aires. We initially included 80 patients who presented suspicious cervical LNs on consecutive neck ultrasound (US) after the initial surgery and had at least 12 months of follow-up. We considered the following as suspicious characteristics for the LNs: round shape, hypoechogenicity, absence of hilum, cystic changes, presence of microcalcifications, and increased vascularity. The exclusion criteria were patients with any LN ≥2 cm or multiple LNs ≥1.5 cm, proximity to vital structures, PET-positive disease (standard uptake value ≥5), aggressive histology, and distant metastasis. Of 34 patients in whom a PET scan was performed, 24 patients were excluded owing to SUV ≥5. Finally, we included 50 patients with cytological confirmation of metastatic LNs by US-guided fine-needle aspiration (FNA). A flow chart of patient selection is given in Figure 1.
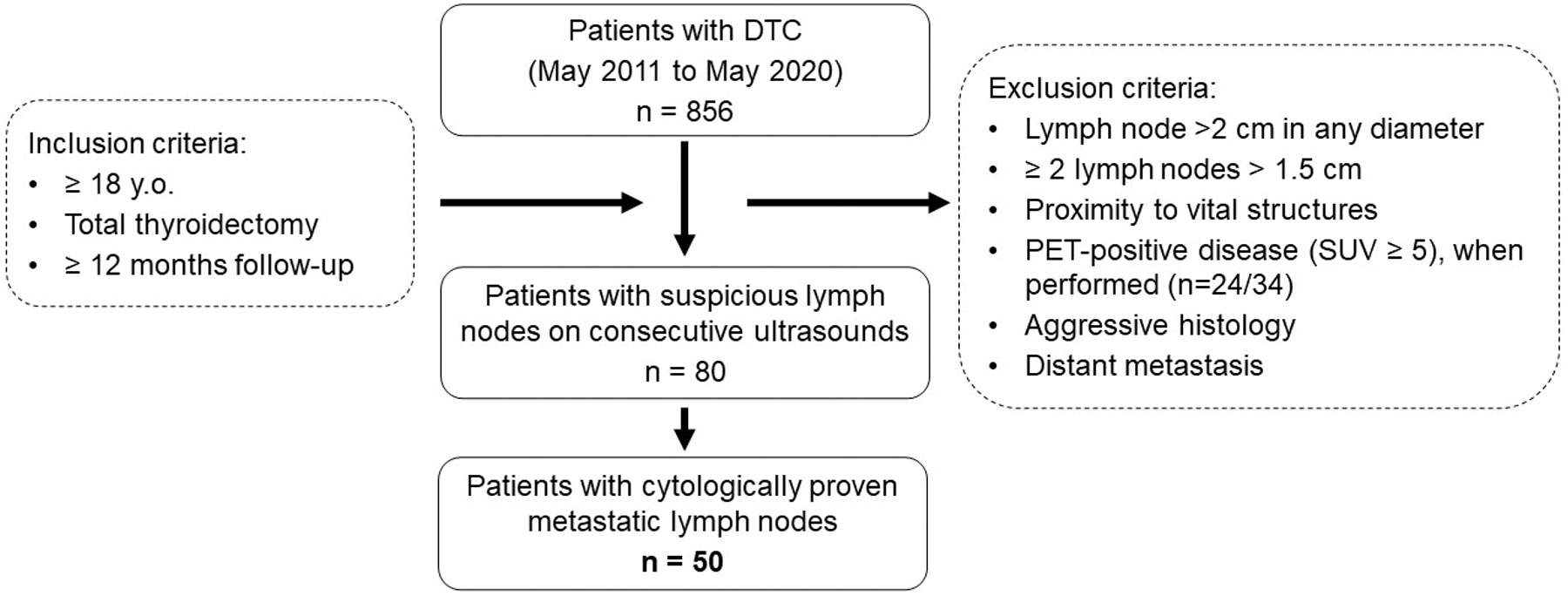
Patient flow chart.
We classified each patient according to the eighth edition of the American Joint Committee on Cancer/International Union against Cancer (AJCC/UICC) staging system and assessed the risk of recurrence using the risk stratification system proposed by the American Thyroid Association (ATA) guidelines (low, intermediate, or high). 7
The study was evaluated by the Teaching and Research Committee at the Hospital de Clínicas, University of Buenos Aires (Comité de Docencia e Investigación) who decided that informed consent was not mandatory owing to the observational and retrospective design of the study and that it did not represent any risk for the participants and the data were anonymized. The study was conducted in accordance with the National Law 25.326 of Personal Data Protection, and the principles expressed in the Declaration of Helsinki.
Clinical management during the follow-up
Patients were followed-up with thyroglobulin (Tg) and thyroglobulin antibodies (TgAb) measurements on suppressive therapy and neck US every 6–12 months. US examinations were performed by the same radiologist with expertise in thyroid cancer at our institution using a 13-MHz linear transducer (Aplio 400; Toshiba, Tokyo, Japan). The Tg electrochemiluminescence (EQLIA) Cobas e 411 assay (Roche Diagnostics GmbH, Mannheim, Germany) was used to measure Tg levels. The analytical and functional sensitivities were 0.04 and 0.1 ng/mL, respectively. For a mean value of 0.147 ng/mL, the intra-assay and interassay coefficient of variation provided by the manufacturer was 2.2% and 3.2%, respectively. The TgAb Electrochemiluminescence Cobas e411 assay (Roche Diagnostics GmbH) was used to measure TgAb levels. A value <40 IU/mL was considered negative. 18F-FDG-PET/CT is not routinely performed in our clinical practice and we consider using it in patients with aggressive histology or biochemical incomplete response with conflicting findings in standard diagnostic procedures. 8
Outcomes
Our main outcome was LN growth. A significant growth was defined as an increase of ≥3 mm in any dimension, but we also used a more specific cutoff of ≥5 mm growth as reported by previous investigations. 5,9 In the case of multiple LNs, we analyzed the data of all LNs and selected the most representative one (the LN with the greater diameter and/or the one that had an increase of ≥3 mm) to calculate the changes in size. We also analyzed the percentage of patients who needed salvage surgery and/or radioactive iodine treatment. To evaluate the presence of local complications related to LN growth (invasion or compression to vital structures), we reviewed the neck US reports and the pathology reports of the patients who underwent salvage surgery.
Statistical analysis
Categorical data were presented as frequencies and percentages (%) and were compared using a chi-squared test or Fisher's exact test, when appropriate. Quantitative data were presented as mean ± standard deviation or median and range. To compare mean levels, Student's t-test was used for parametric variables and Mann–Whitney U-test for nonparametric variables. The normal distribution of continuous data was assessed using the Kolmogorov–Smirnov or Shapiro-Wilks test when appropriate. For multivariable analysis, a multiple logistic regression was performed. Progression-free survival was estimated using the Kaplan–Meier method and was defined as time since the patient initiated AS to the time of LN growth (≥3 mm). Differences between groups were analyzed by the log-rank test. A value of p < 0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS software (version 20.0; SPSS Inc., Chicago, IL, USA).
Results
Patients' characteristics
We included 50 patients with cytological confirmation of metastatic LNs in whom we decided AS. The baseline characteristics of these patients are summarized in Table 1. The median age at diagnosis of the DTC was 41 years (range, 18–75). Most patients were women (80%) and had a classical papillary thyroid carcinoma (86%). The initial surgery included central and lateral neck dissections in 44% of cases and only central dissections in 26%. Most patients had an intermediate risk of recurrence (60%) and received radioactive iodine ablation (84%, median radioactive iodine activity 100 mCi; interquartile range, 100–150).
Baseline Characteristics of Patients Included in the Study (N = 50)
AJCC, American Joint Committee on Cancer; AS, active surveillance; ATA, American Thyroid Association; IQR, interquartile range; PTC, papillary thyroid carcinoma; RAI, radioactive iodine; SD, standard deviation; Tg, thyroglobulin; TgAb, thyroglobulin antibodies.
Metastatic LN characteristics
Table 2 provides the US features of the metastatic LNs. Most patients had 1 metastatic LN under AS (72%), but we also included 12 (24%) patients who had 2 LNs and 2 (4%) patients with 3 LNs. At least 2 suspicious ultrasonographic findings were found in 64% of our patients and the most frequent were hypoechogenicity (78%), absence of hilum (32%), and microcalcifications (32%). Most of them were located in region IV (44%) and VI (32%) of the neck compartments.
Lymph Nodes Characteristics (Per Patient, N = 50)
LNs, lymph nodes.
The mean size of the LNs was 10.1 ± 4.4 mm (median 8.5, range: 5–20) on first assessment and 10.7 ± 6.1 mm (median 9.5, range: 5–34) at the end of the study, in the largest diameter. In short axis, the initial and final mean size were 5.4 ± 2.1 (median 5, range 3–11) and 5.6 ± 2.8 (median 5, 3–12). In half the patients the LN measured ≥1 cm.
Clinical outcomes
After a median follow-up of 29 months (range, 12–144), 12 patients (24%) had an increase in size of at least 3 mm of the metastatic LN. Of these patients, 4 showed an increase of ≥5 mm (8% of the total cohort). The median increase in size was 3.75 mm (range, 0–16).
Of the 12 patients who demonstrated increase in LN, 7 (58%) were surgically removed. None of them had a structural incomplete response at the end of follow-up after the salvage neck dissection: two achieved an excellent response to therapy and five had an indeterminate response with slightly elevated Tg levels. The remaining five patients who experienced LN growth continued with observation owing to the small volume of disease (median size, 10 mm). During AS, four patients received radioactive iodine. Three of them remained stable in size and one showed an LN decrease of 3 mm in size.
In the majority of our patients (38/50, 76%) the LN size remained stable and 43/50 (86%) were followed-up without the need of surgery. None of the patients in the total cohort developed local complications or distant metastasis during follow-up.
The relationships between the LN growth and various clinical and ultrasonographic variables are given in Table 3. The only predictive factor for metastatic LN growth was the increase of Tg level ≥0.5 ng/mL (p = 0.016). Based on a multivariate analysis, patients with increase in Tg level ≥0.5 ng/mL had a significantly higher chance of developing LN growth (OR, 16.2 [confidence interval; CI 1.5–120.2] p = 0.020) (Table 4).
Univariate Analysis for Factors Predictive of Lymph Node Growth
Bold values denote statistical significance (p < 0.05).
Quantitative variables are expressed as mean ± standard deviation and categorical variables are expressed as number and percentage.
Student's t-test (variable with normal distribution).
Fisher's exact test.
Chi-square test.
Mann–Whitney U-test (variable without normal distribution).
RAI, radioactive iodine.
Multiple Logistic Regression for Factors Predicting Lymph Node Growth (>3 mm)
CI, confidence Interval.
The median progression-free survival rate was 6.6 years [CI 5.6–9.5] (Fig. 2). The progression-free survival rate was significantly shorter in patients who demonstrated an increase in the Tg level ≥0.5 ng/mL (28% at 40 months) in comparison with patients with a Tg increase of <0.5 ng/mL (82% at 40 months) (p = 0.036) (Fig. 3).

Progression-free survival of the overall cohort.

Comparison of progression-free survival groups according to the Tg increase. At 40 months, the estimated progression-free survival was 28% in patients with an increase in Tg levels ≥0.5 ng/mL (dotted line) versus 82% in patients with Tg increase <0.5 ng/mL (plain line) (p = 0.036). Tg, thyroglobulin.
Discussion
The detection of small-volume LN recurrences is a common situation in patients with DTC. 4 In this scenario, there is uncertainty whether the patient should be followed-up with clinical observation or undergo surgery. A major concern is to know which factors could predict LN enlargement and therefore the need for a new surgery. In our study, we demonstrated that, in properly selected patients for AS of metastatic LNs, only 24% experienced at least a 3 mm growth over a median follow-up of 29 months. The only clinical factor that could predict this outcome was an increase in Tg levels of >0.5 ng/mL.
The natural history of suspicious LNs detected after initial therapy for papillary thyroid cancer (PTC) were assessed in some retrospective studies. 5,6 Similar to our study, Robenshtok et al, in a cohort of 177 PTC patients with ≤2 cm abnormal LNs detected after initial surgery and followed-up for a median time of 3.5 years, demonstrated a ≥ 3 mm and a ≥ 5 mm increase in the size of the LN in 20% and 9% of the patients, respectively. 5 The same study group also reported, from a cohort of 191 patients with ≤11 mm thyroid bed nodules detected on the first postoperative US, that only 8% increased in size (≥3 mm) over a median follow-up of 5 years. 6
Because the probability of having a false-positive result on postoperative neck US is high, 10 we decided to include only cytological proven metastatic LNs. In the two mentioned studies, 5,6 the percentage of progression increased when only patients with pathological FNA cytologically proven were included. In the study from Robenshtok et al, 4 of 22 patients (18%) with cytological-proven metastatic LNs had an increase in size of at least 5 mm versus 15 of 166 (9%) from the total cohort of patients with suspicious LNs. 5 Similarly, in the study from Rondeau et al, an increase of 3 mm was demonstrated in 3/9 (33%) patients with metastatic thyroid bed nodules (vs. 8% in the entire cohort). 6 In a larger cohort (n = 83) including patients with metastatic LNs, the authors reported an increase in size in 20.5% (at least 3 mm) and 8.4% (at least 5 mm). 9 These results were all consistent with the findings obtained in our investigation.
Based on the above data, we believe that, in clinical practice, there is no need to obtain FNA results in most patients with highly suspicious LNs that will be selected for AS. Indeed, the ATA guidelines recommend that small (5–8 mm in shortest diameter) abnormal cervical LN are probably best managed with AS (observation) with serial cross-sectional imaging, reserving FNA and subsequent intervention for documented structural disease progression. 7 Moreover, larger (>8–10 mm) metastatic LNs can be carefully observed in properly selected patients with serial clinical and radiographic follow-up, with surgery being offered if they progress during follow-up and conservative follow-up being maintained if they are stable over time. 7
Although tumor growth of metastatic LNs was selected as a main outcome in our study, this is not a single indication for surgery, and other factors should be taken into account such as the proximity to vital structures, presence of macroscopic gross extranodal extension, and rate of tumor progression. 5 –7 In the study from Maciel et al, including 89 patients with LNs metastasis under AS, the percentage of progression was 49.4% but only 16.9% required radiotherapy (4.5%) or surgery (12.4%). 11 In our study, 24% had LN progression and 14% required surgery. It is worth noting that in the mentioned study, patients with aggressive histology and distant metastases were included. 11 This could explain the higher percentages of progressive disease in comparison with our cohort.
Many studies have failed to find a predictive factor for LN enlargement. 5,9 In our study, the only clinical factor that was able to predict LN growth was the increase of Tg levels of >0.5 ng/mL. Similarly, Rondeau et al found that the increase in Tg levels over time was also more likely to be observed in association with growing nodules in the thyroid bed (24% vs. 7%, p = 0.05). 6 Therefore, to monitor Tg levels along with periodic US seems a reasonable approach for these patients. 7
An important issue to consider is that ∼30% of DTC patients have serum TgAb that might interfere with Tg measurement. 12 TgAb trend has been proven to be useful in predicting structural incomplete response. 7 In our cohort, 13 (26%) patients had positive TgAb. An increase in ≥50% of basal values was not predictive of disease progression. However, because only 3 patients demonstrated at least a 50% increase in TgAb levels, a larger sample size would be needed to assess whether TgAb trend could predict LN growth. Molecular testing was not available in our patients. As genomic interrogation is becoming more widely available, we believe that, in the future, molecular profile could be an interesting variable to test as a predictor of LN growth.
One of the main concerns in patients with local recurrences is that they have to confront the risk of surgical complications at every intervention. At least one neck dissection after initial therapy was performed in 26% of our patients. Cervical re-explorations commonly imply higher risks of hypoparathyroidism and recurrent laryngeal nerve paralysis owing to scarring from previous surgery. 13 Less frequently, postsurgical hematomas and infections may be found among other complications. 14 These events could significantly diminish the quality of life of patients with DTC. 15 In addition, these patients usually carry a lot of emotional concerns regarding a new intervention. 16
Most of the metastatic LNs reported in our study were located in the lateral neck compartment. Similar to other studies, 5 our investigation focused mainly on lateral cervical metastatic LNs detected during postoperative cancer follow-up.
Our study has several limitations. First, this is a retrospective study and the indications of surgery or continue observation were made based on specific characteristics of the patients. In this real-life scenario, the physician–patient relationship has many variables that are difficult to evaluate. Second, there is a selection bias for the patients included. Our cohort represents a small group of patients selected for AS and presumed to have a low risk of progression. Indeed, patients with aggressive histologic variants were excluded and our cohort reflects a young patient population (median age 41 years). Therefore, our results could underestimate the real rate of progression of all metastatic LNs in DTC. In addition, presurgical neck US were not available and some patients would have presurgical LNs that were missed in the preoperative setting. Third, the time of follow-up was relatively short for some patients, which could also underestimate the rate of progression. Fourth, the small sample size may have prevented us from finding additional variables that may correlate with LN growth.
Conclusion
In a carefully selected cohort of thyroid cancer patients, only 24% with small loco-regional recurrences selected for AS showed a growth of ≥3 mm, with no evidence of local complications or new metastatic sites. AS of small LNs could be a feasible alternative in properly selected patients.
Footnotes
Acknowledgment
We want to thank Dr Raúl Chervín for collaborating with the clinical data of one patient in the cohort.
Authors' Contributions
F.J.: Data curation, formal analysis, writing—original draft preparation. E.A.: Data curation, writing—reviewing and editing. F.B.: Data curation, writing—reviewing and editing. L.G.: Data curation. F.P.: Conceptualization, supervision, writing— reviewing and editing. All authors were responsible for the final approval of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.