
Abstract

Background
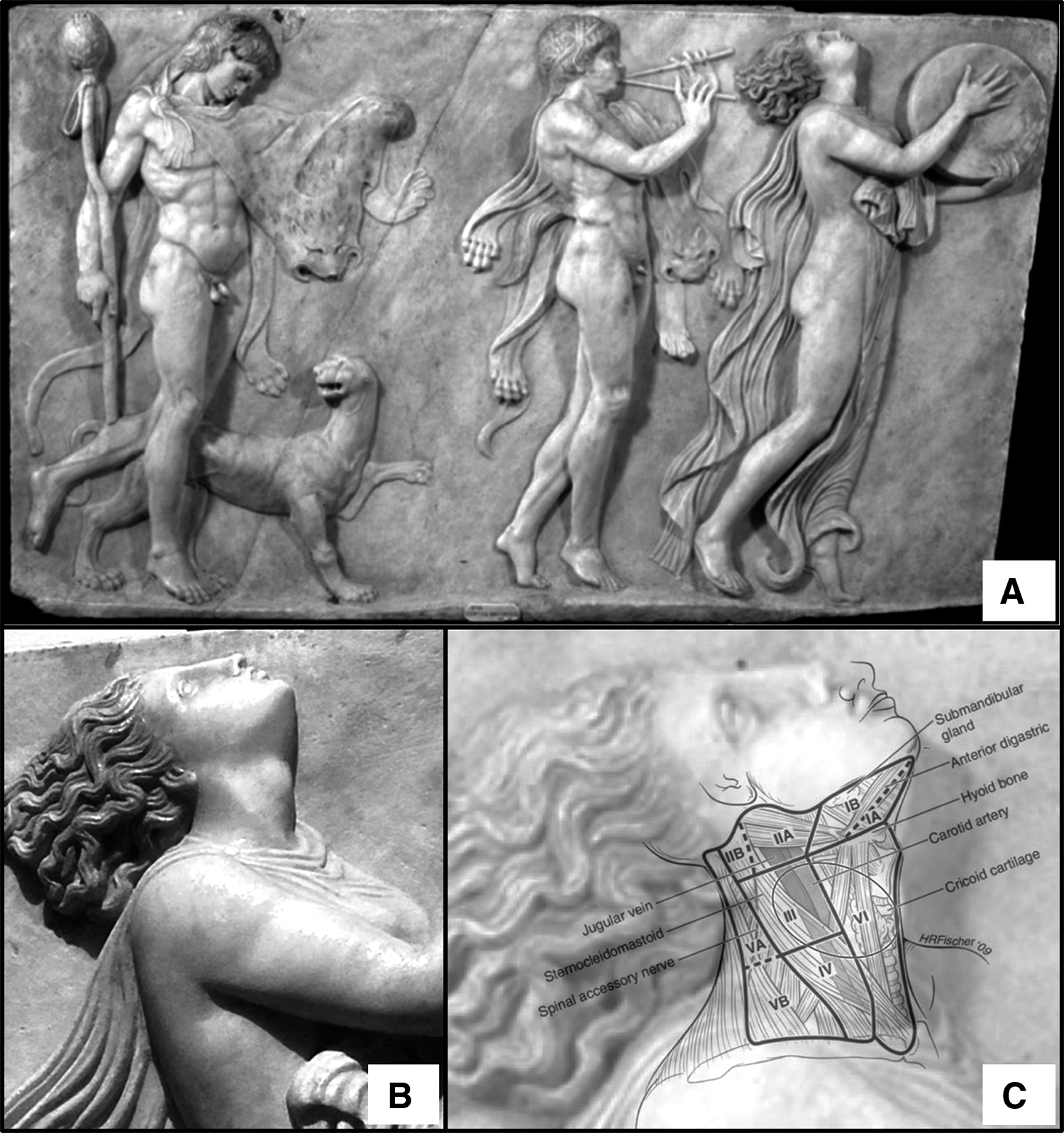
We herein take a voyage back in time to the first century A.D. The woman represented and chosen in this artwork of the first century A.D. by an unknown artist and found in an aristocratic villa in Herculaneum (Naples) (Fig. 1A) has “a tiny nose, beautiful legs, a well-developed tapering hand, with long tapering fingers.” 1 The figure's hair is let down and a protuberance is noted on her neck: we believe this may be of interest to a thyroid audience (Fig. 1B).
Description
Let us analyze this said imperfection with a clinical eye (Fig. 1C). The protuberance is located on the midline of the neck, in a region circumscribed vertically by the hyoid bone and the isthmus, and with the circumference tending to the paramedian region, not surpassing the sternocleidomastoid muscle. The oval shaped projection is seemingly well defined and ∼4.5 cm in longitudinal diameter (length calculated using ratio taking into consideration the length of the figure with the median height 2 of an ancient roman woman). Going more in detail, the prominence is located between the VI compartment (anterior group, containing the anterior jugular vein and cricothyroid notch) and the III compartment (middle jugular group, containing the internal jugular vein, carotid artery, and the anterior cervical chain) on the right side of the neck.
Investigation and Hypothesis
Finding a differential diagnosis for this woman is difficult without laboratory and scan tests. Consequently, we shall analyze the most probable and sensible scenario and leave to the reader, the last word. Notably, this woman does not present with the typical somatic habitus of hypothyroidism. She has a normal body weight, a full head of hair, her face is not swollen, nor shows ocular or pitting edema. Furthermore, one can also cross out the possibility of a hyperthyroidism, due to the lack of exophthalmos. Therefore, already at first sight, we can deem as improbable two of the major thyroid pathologies on a clinical ground. 3
Moving onward, when looking at the patient's epidermis, it is stretched in the same manner of a cyst. This leads us reasoning on different kinds of cysts. To begin with, let us suppose it could be a thyroglossal duct cyst (TDC). These cysts are congenital and almost always benign; they develop during gestation period, due to the thyroglossal tract's inability to close properly. This consequently leaves it filling up with mucous and fluids, becoming a cyst.
A different possibility is that of a dermoid cyst; this kind of cyst is also asymptomatic and congenital, happening during embryonal development when the skin layers do not properly merge. 4 Finally, it could also be a thyroid cyst. In addition, in terms of nodules, this could perhaps be an adenoma or a colloid nodular goiter. Either way, in this first scenario we may exclude the possibility of a toxic adenoma because that would lead to a hyperthyroid phenotype that, as already mentioned, does not look to be the case. As for the second scenario, it could be a colloid nodular goiter caused by the lack of iodine, 5 which is plausible when looking at the diet of the era.
Finally, this could also be a metastatic spread, either from the thyroid or from the nasopharynx. In either case, a metastatic spread would imply an advanced disease state, which in the former case would imply hair loss, fatigue, weight loss, and spread to the lymph nodes. To a matter of probability, in this case a papillary thyroid carcinoma may be thought since it has a relatively high likelihood to metastasize to the neck. 6 Whereas, in the latter case, it would result in difficulty of feeding, consequent weight loss and cachexia, or even ringing in the ears (not possible seeing that the woman is playing a musical instrument).
Finally, another potential diagnosis is that of an acute (bacterial) thyroiditis. However, such an infection would cause great pain, especially upon the hyperextension of the neck; a patient would never perform such a painful movement.
Conclusion
Our conclusion is that this prominence could either be a TDC or a dermoid cyst, or even a thyroid cyst. Having now taken this voyage through time and through a myriad of clinical differential diagnosis, we leave the stage to your thoughts. May you push your mind beyond the limits of time and space to make the most proficient diagnosis?
Footnotes
Authors' Contributions
M.V.M. contributed to conceptualization (equal); writing—original draft (equal), review, and editing (equal); and approval of the final version submitted for publication. P.P. was involved in conceptualization (equal); writing—original draft (equal), review, and editing (equal); and approval of the final version submitted for publication. A.P. was in charge of conceptualization (equal); writing—original draft (equal), review, and editing (equal); and approval of the final version submitted for publication.
Acknowledgment
We are very grateful to Dr. Gregorio Reda, Rome, Italy, who has spotted this sculpture during a visit and notified us.
Ethical approval
Ethical approval is not requested in this case because it refers to a patient who lived 2000 years ago (first century A.D.).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.