
Abstract
Introduction:
Pediatric Graves' disease (GD) is associated with hyperthyroid symptoms that impact psychosocial and physical functioning. Total thyroidectomy (TT) is a definitive treatment option that replaces antithyroid medication. While studies have examined health-related quality of life (QOL) in adults, there are no data describing impacts of TT in pediatrics. In this prospective longitudinal study, we explored the impact of TT on disease-specific QOL and satisfaction with TT and scar appearance in adolescent patients with GD undergoing TT.
Methods:
Patients 12–19 years old pursuing TT for GD and their parents were recruited to complete surveys before and at least 6 months after TT. Surveys assessed motivations for pursuing TT, QOL, perceived stigmatization, self-esteem, scar appearance, and surgery satisfaction. Paired scores were compared using Wilcoxon signed-rank tests, and subscore associations were assessed using Spearman association tests.
Results:
Thirty-seven patient–parent dyads completed baseline surveys, including 20 patient–parent dyads completing pre- and post-TT surveys. At baseline, patients reported physical and cognitive symptomology, including tiredness, anxiety, and emotional susceptibility through ThyPRO. Psychosocial functioning at school was low through PedsQL. Disease-specific QOL significantly improved after TT, with notable improvements associated with resolution of goiter (median change = −26.14, p = 0.003), hyperthyroid symptoms (median change = −43.75, p = 0.002), tiredness (median change = −26.79, p = 0.017), cognitive impairment (median change = −14.58, p = 0.035), anxiety (median change = −33.33, p = 0.010), and emotional susceptibility (median change = −28.99, p = 0.035). Physical (median change = 18.75, p = 0.005) and school-related functioning (median change = 30.00, p = 0.002) also significantly improved post-TT. Reported GD-associated eye symptomology (thyroid eye disease) was the second lowest scoring ThyPRO subscore at baseline and improved after surgery (median change = 14.06, p = 0.03). Families reported median recovery by two months, high satisfaction with the outcomes of TT, and minimal concerns over scar appearance. No permanent surgical complications (i.e., recurrent laryngeal nerve damage or hypoparathyroidism) were sustained.
Conclusions:
In the setting of a high-volume surgeon with low complication rates, TT for GD in pediatric populations may have substantial beneficial effects on disease-specific QOL and psychosocial functioning, with minimal adverse complaints about scar appearance.
Introduction
Graves' disease (GD) is an autoimmune disorder with an estimated prevalence of 1:10,000, equating to ∼8600 patients under 21 years of age in the United States. 1,2 Children and young adults with GD experience significant symptomology, including emotional lability, hyperactivity, decreased ability to focus, poor sleep, palpitations, and/or warmth intolerance, and other physical manifestations, such as fidgetiness, weight loss, goiter, proptosis, and eyelid retraction, which can have personal and social ramifications. 2,3
Treatment options for GD include antithyroid medications (ATDs) or definitive treatments with either radioactive iodine ablation (RAI) or total thyroidectomy (TT). 4,5 Most pediatric patients are placed on ATDs at diagnosis to normalize their biochemical abnormalities and decrease symptomatic hyperthyroidism. 5 Unfortunately, the 5-year remission rate for pediatric patients treated with ATD is 30–35%. 6,7 While pediatric patients often continue medical therapy for 5–10 years or longer, a significant number of pediatric patients pursue definitive therapy during adolescence to trade the unpredictable course of GD for a more stable hypothyroid state. 2
Patients are selected for definitive therapy based on age, the presence of thyroid eye disease (TED), the size of the thyroid gland, the presence or absence of thyroid nodules, family preference, and local experience of the treatment team. 3 Avoidance of exposure to radioactive iodine and the more predictable and rapid ability to achieve hypothyroidism are factors for selection of TT over RAI. However, scar size and appearance, as well as the risk of surgical complications, including hypoparathyroidism and damage to the recurrent laryngeal nerve, are opposing concerns associated with TT.
Several studies report reduced health-related quality of life (QOL) in adult patients with GD. 8 –11 For adults with GD, definitive treatment through TT is associated with significant improvement in patient-reported symptoms and overall QOL. 11 –13 No studies to date have explored QOL in pediatric patients with GD in the context of TT. With on-going debate about the risks and benefits of RAI versus surgery for adolescents, consideration of patient-perceived QOL is essential for appropriate clinical education and consent between definitive therapy options.
In addition, scar appearance and eye symptoms from Graves' orbitopathy (GO), also referred to as TED, are important factors for TT, yet no studies have assessed their impact alongside QOL in pediatrics. 14 –17
This prospective study sought to explore and describe psychosocial and developmental functioning among patients undergoing TT for GD in the Children's Hospital of Philadelphia (CHOP) Thyroid Center. We aimed to explore (1) patient disease-specific QOL and psychosocial functioning before and after TT and (2) satisfaction with TT and scar appearance.
Materials and Methods
Recruitment and procedures
Patients 12–19 years old who pursued definitive surgical therapy for GD between January 2016 and March 2022 and a parent/care provider were included in this prospective study, which was reviewed and approved by CHOP's Institutional Review Board. Consent and assent of eligible subjects were obtained during clinic visits or through phone. Patients underwent TT at CHOP by a high-volume pediatric thyroid-surgeon (K.K., N.S.A), defined as a surgeon completing 25 or more thyroid surgeries annually. 18 Participants completed a set of surveys before and at least six months after TT and corrective eye surgery for GO, if applicable. Compensation was provided after completion of each survey set.
Surveys
Parents provided information on patient and parent demographic information. Preoperatively, parents reported perceived severity of their child's condition, perceptions of and satisfaction with their child's appearance, and their thoughts about potential treatments on a Likert-type scale (e.g., 1 = not severe, 5 = very severe). Parents also rated motivations for surgery from a list of potential factors on a Likert-type scale (e.g., 1 = not important, 5 = very important). These surveys were similar to rating scales used in studies by CHOP's Division of Plastic and Reconstructive Surgery and were selected with input from CHOP divisions of psychology and endocrinology. 19
Disease-specific QOL, psychosocial functioning, and appearance and stigmatization concerns were assessed using questionnaires completed pre- and post-TT:
Pediatric Quality of Life Scales (PedsQL)—Parents and patients completed this validated 23-question PedsQL survey to assess general QOL.
20
–22
Subscales include physical emotional, social, and cognitive functioning. Likert-type responses (e.g., 1 = never, 5 = almost always) were inverse scored and reported on a 0 to 100 scale with higher scores indicating better QOL.
Quality of Life Questionnaire for Patients with Thyroid Disease (ThyPRO)—Patients completed this 85-question survey to assess thyroid-specific functioning and well-being.
23
Subscales included goiter symptoms, hypothyroid symptoms, hyperthyroid symptoms, eye symptoms, tiredness, cognitive complaints, anxiety, depressivity, emotional susceptibility, impaired social life, impaired daily life, cosmetic complaints, and a single item rating overall impact of disease on disease-specific QOL. Some items were reverse scored for whole-survey consistency, and Likert-type responses (e.g., 1 = not at all, 5 = very much) were reported on a 0 to 100 scale, with higher scores indicating greater impact of disease. A composite score was calculated from tiredness, cognitive complaints, anxiety, depressivity, emotional susceptibility, impaired social life, and single item overall impact subscores.
24
Perceived Stigmatization Questionnaire (PSQ)—Patients and parents completed this 21-question survey to assess perceptions of being stigmatized by others based on appearance differences.
25
Responses were on a Likert-type scale (e.g., 1 = never, 5 = almost always), and subscales included absence of friendly behavior, confused/staring behavior, and hostile behavior.
Body Esteem Scale for Adolescents and Adults (BESAA)
European Group on Graves' Orbitopathy GO Quality of Life Questionnaire (EUGOGO-QOL)—Patients completed this 15-question survey to assess the self-reported impact of GO on appearance and self-confidence.
27
Subscales included appearance and social interaction/perception. Likert-type responses are reported 0 to 100, with higher scores indicating greater eye health/less impact of disease.
Patients and parents completed surveys postoperatively to assess satisfaction with TT and scar appearance. The Postoperative Surgical Satisfaction Scale recorded patient and parent treatment outcome satisfaction. Responses were reported on a Likert-type scale (e.g., 1 = very dissatisfied, 5 = very satisfied). This survey was developed based on clinical satisfaction measures utilized in quality improvement initiatives at CHOP's Division of Plastic and Reconstructive Surgery. 19
The Patient and Observer Scar Assessment Scale (POSAS) assessed surgical scar pain, itching, color, stiffness, thickness, irregularity, and overall opinion/satisfaction. 16,28 The scale items are answered on a Likert-type scale (e.g., 0 = normal skin, 10 = worst scar imaginable). The first six items answered by patients addressing scar features are summed for a total patient POSAS score.
Reporting and statistical analysis
Patients' electronic medical records were reviewed for demographic information, symptoms of hyperthyroidism, ATD information, surgical complications and thyroid function tests (TFTs), (thyrotropin [TSH], free thyroxine [fT4], total triiodothyronine [TT3]). Median responses (interquartile range [IQR] = first quartile–third quartile) were reported for continuous variables. Missing responses are noted where applicable and were excluded from analyses in listwise or pairwise manners. Cronbach alpha coefficients were calculated to evaluate internal consistency.
All completed patient surveys were accompanied by respective parent responses. Pre- and postoperative survey responses were compared using Wilcoxon signed-rank test with Bonferroni–Holm p-value correction for family-wise error rate within survey subscales and Cliff's delta effect size with CIs. Associations within ThyPRO and PedsQL survey subscales were assessed using Spearman association test with Benjamin–Hochberg p-value correction for false discovery rate (FDR) of multiple comparisons. Additional survey, TFT, and clinical feature associations were assessed using Spearman association.
p-Values <0.10 (FDR = 0.1 for exploratory analyses) for ThyPRO/PedsQL associations were considered statistically significant, and all other p-values <0.05 were considered statistically significant. Analyses were performed with R 4.0.5 and R Studio 1.4.1106 using packages tidyverse, rstatix, fmsb, corrplot, Hmisc, RcmdrMisc, ltm, and forestplot. 29 –38
Results
Baseline clinical information
Thirty-seven patient and parent dyads completed respective survey sets before TT (Fig. 1). Of this baseline patient cohort, the majority were female (33/37, 89%) with a median age of 16.1 years (IQR = 14.5–17.1). Seventeen (17/37, 46%) patients had poorly controlled GD (elevated fT4 and TT3 with suppressed TSH), resulting in clinical hyperthyroidism-related symptomology as well as cognitive impairments contributing to difficulties in school (Table 1 and Fig. 2). Eleven (11/20, 55%) patients completing surveys at both timepoints had poorly controlled GD preoperatively.
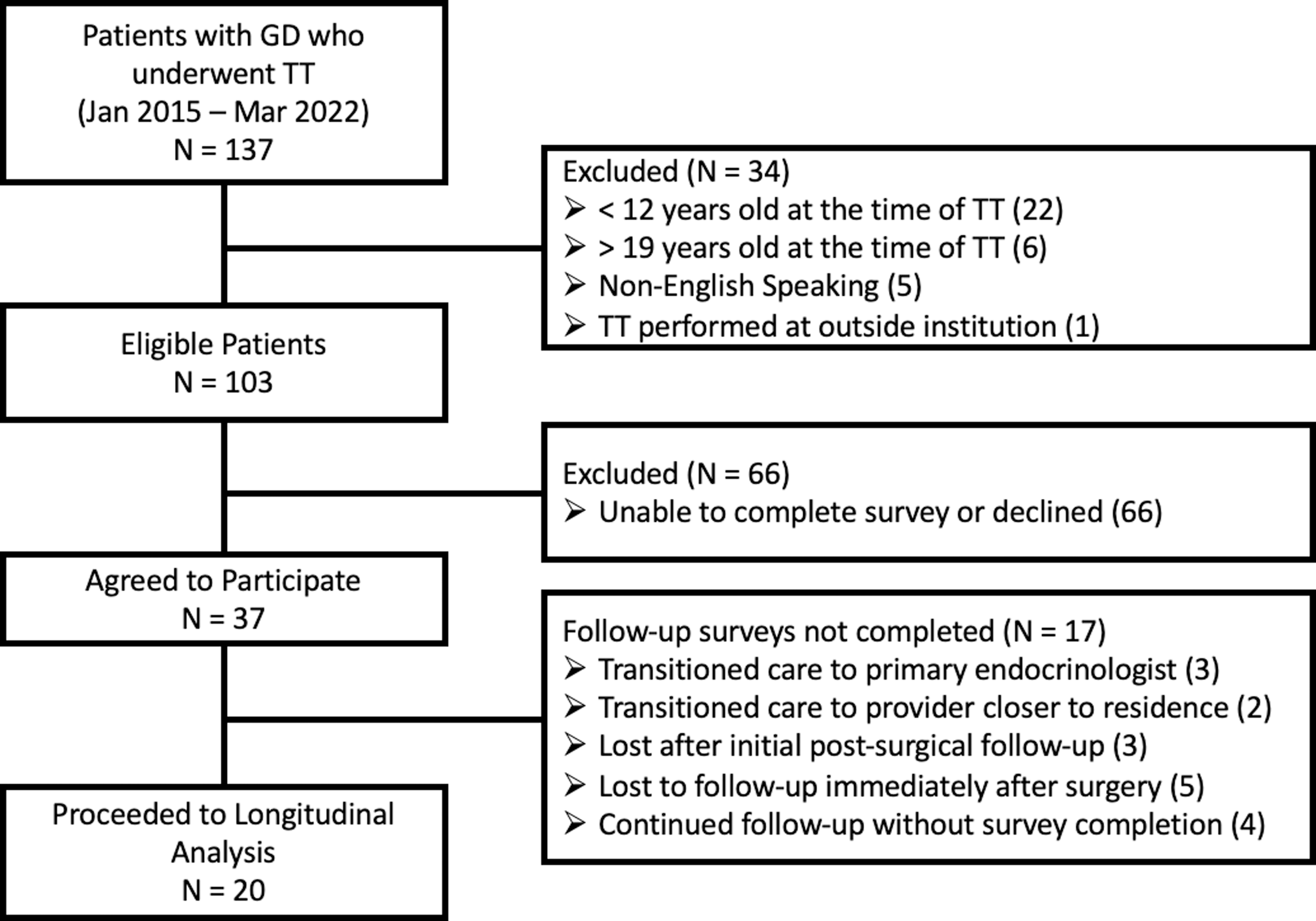
Recruitment of study cohort. Flow diagram of eligible, screened, and included participants with exclusionary documentation. GD, Graves' disease; TT, total thyroidectomy.
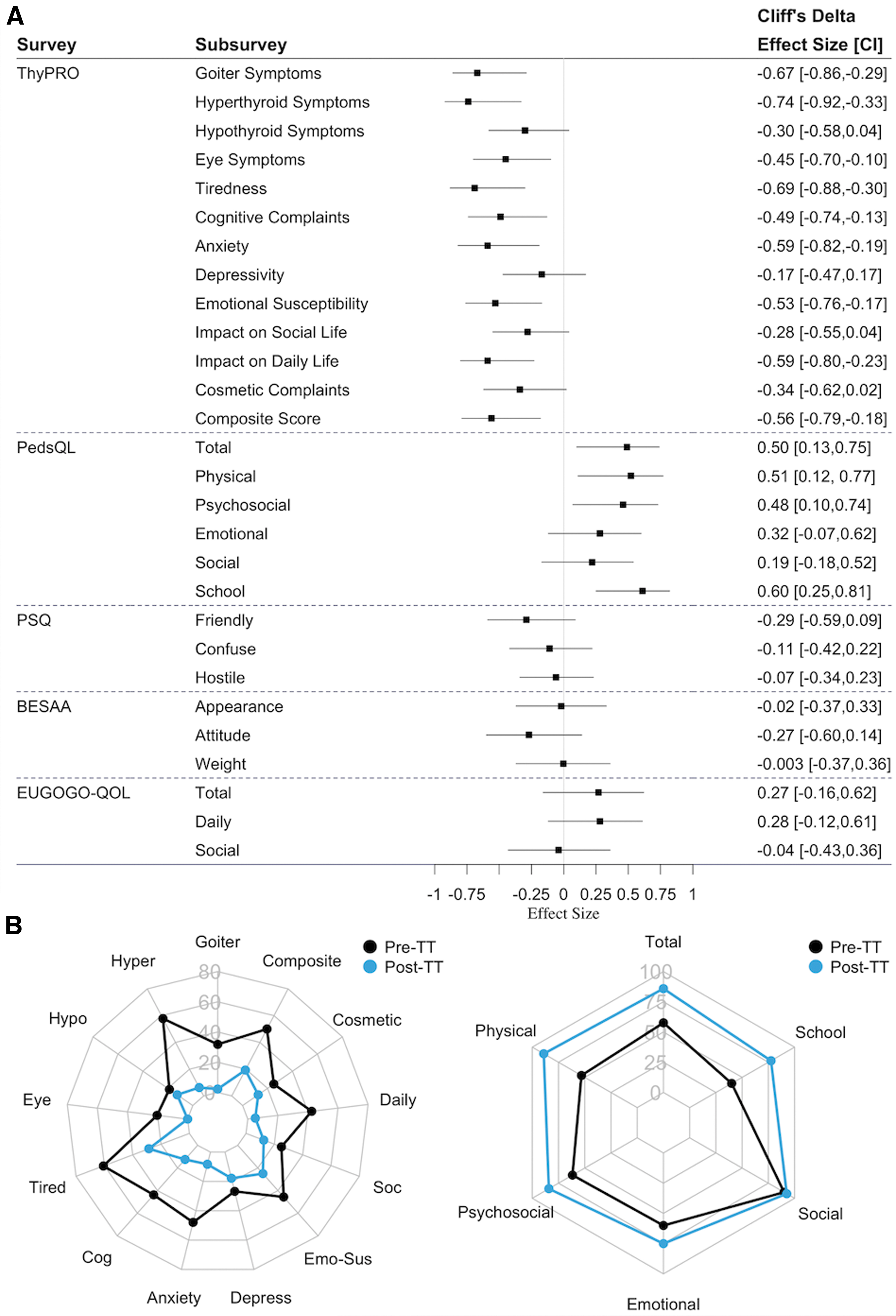
Visualized survey effects before and after TT. (
Demographic and Clinical Features
Reference range for assessment of TSH biochemical control: 0.50–4.50 mUI/L.
Reference range for assessment of fT4 biochemical control: 0.80–1.40 ng/dL.
Reference range for assessment of TT3 biochemical control: 86–192 ng/dL.
ATD, antithyroid medication; fT4, free thyroxine; IQR, interquartile range; TSH, thyrotropin; TT, total thyroidectomy; TT3, total triiodothyronine.
Sixteen patients presented with GD-related proptosis in clinic with 17 (46%) patients experiencing symptoms consistent with TED (Table 1). All 37 patients were treated with methimazole with a median interval of 18.4 months (IQR = 9.3–31.8) between ATD initiation and TT (Table 1). Parents reported ease of monitoring postsurgical hypothyroidism, access to a “high-volume” thyroid surgeon, and avoidance of RAI as primary motivations for pursuing TT (Supplementary Fig. S1).
Disease-specific QOL, psychosocial functioning, stigmatization, and body perceptions
Twenty patient and parent dyads completed respective pre- and postoperative survey sets with a median interval between surveys of 9.5 months (IQR = 6.0–11.8). Median baseline survey responses in the patient cohort completing pre- and postoperative surveys were statistically comparable (sensitivity analysis) with the median baseline responses in the total cohort (Table 2). Patients had significant physical and psychosocial distress per PedsQL responses with 24 patients (24/37, 65%; 12/19, 63% completing both survey timepoints) scoring below 1 standard deviation (SD) of the general population mean. 21
Characteristics of Disease-Specific Health-Related Quality of Life, Psychosocial Functioning, Social Stigmatization, and Body Appearance Perceptions Pretotal Thyroidectomy and Post-Total Thyroidectomy
One participant did not complete the PedsQL, 1 participant did not complete the BESAA, and 7 participants did not complete the EUGOGO-QOL at baseline. One participant did not complete the BESAA and five participants did not complete the EUGOGO-QOL at follow-up. All subscores demonstrated acceptable Cronbach alpha coefficients (>0.70) except ThyPRO Hypothyroid Symptoms (α = 0.67) and EUGOGO-QOL Daily (α = 0.64). p-Values were adjusted within survey subscores by Bonferroni–Holm method: bold indicates p-value <0.05.
QOL, quality of life.
Within the ThyPRO measures at baseline, patients reported high symptom burden related to tiredness (median = 64.29), hyperthyroidism (median = 59.39), emotional lability (median = 55.56), anxiety (median = 54.17), cognitive complaints (median = 39.58), and negative impact on daily life (median = 37.50, Table 2). Baseline eye symptomology (median = 25.00), depression symptoms (median = 35.71), and cosmetic complaint (median = 29.17) scores were lower by comparison. TFT values were not significantly associated with total PedsQL, ThyPRO hyperthyroidism, or ThyPRO 1-question overall scores (Supplementary Table S1).
Thirteen (13/20, 65%) patients completing both survey timepoints reported improvements in at least 10 of the ThyPRO subscales, and 15 (15/19, 79%) reported improved total PedsQL score (Table 2 and Fig. 2). Nine (9/13, 69%) ThyPRO measures showed improvement, including goiter (median change = −26.14, p = 0.003), hyperthyroid symptoms (median change = −43.75, p = 0.002), eye symptoms (median change = −14.06, p = 0.026), tiredness (median change = −26.79, p = 0.017), cognitive complaints (median change = −14.58, p = 0.035), anxiety (median change = −33.33, p = 0.010), emotional susceptibility (median change = −28.99, p = 0.035), impact on daily life (median change = −22.50, p = 0.015), and overall impact (median change = −25.00, p = 0.035) subscales.
Physical (median change = 18.75, p = 0.005) and school-related (median change = 30.00, p = 0.002) functioning through PedsQL, as well as the total PedsQL score (median change = 18.48, p = 0.005), significantly improved, while changes in emotional (median change = 15.00, p = 0.074) and social (median change = 0.00, p = 0.361) functioning were not significant. Of the 12 patients scoring 1 SD below the PedsQL total general population mean preoperatively, 7 (7/12, 58%) reported improved PedsQL scores above that cutoff. PSQ and BESAA scores were unremarkable at baseline and did not show statistically significant improvement after TT.
Parents rated desire to reduce eye symptomology as a minimal motivating factor for surgery (Supplementary Fig. S1), and GD-associated eye symptomology was the second lowest scoring ThyPRO subscale at baseline (Table 2). Eye symptomology resolved after TT with 15 (15/20, 75%) patients reporting improvements in ThyPRO eye symptoms. Responses to the EUGOGO-QOL questionnaire revealed high eye-specific daily and social QOL at baseline with nonstatistical improvement in the daily EUGOGO-QOL score (Table 2 and Fig. 2). Four patients (4/37, 11%) underwent orbital decompression for GO, but only one patient completed surveys before and after eye surgery.
ThyPRO and PedsQL subscores displayed internal direct association at baseline and change due to surgery (Supplementary Fig. S2). Notably, improvements in school-related functioning were moderately associated with resolution of hyperthyroid and cognitive symptoms, and total PedsQL improvement was moderately associated with decreasing anxiety burden (Supplementary Fig. S2). The interval between ATD initiation and TT was inversely associated with improvements in total PedsQL (ρ = −0.48, p = 0.039) and one-question overall ThyPRO (ρ = 0.48, p = 0.031).
Of patients with available TFT data at time of postoperative survey completion, only one patient demonstrated low fT4 and TT3. Only change in fT4 was associated with a survey subscore of interest, total PedsQL score (ρ = −0.66, p = 0.017; Supplementary Table S1).
Satisfaction with TT and scar appearance
Patients and parents reported high overall satisfaction after TT with perceived improvements in reported GD symptoms, school performance, and appearance (Table 2, Figs. 2 and 3). Median reported recovery period from TT was 2 months (range = 1 to 5 months). Clinically, all patients achieved remission from their GD with no patients experiencing permanent surgical complications (i.e., no recurrent laryngeal nerve damage or permanent hypoparathyroidism). Overall scar appearance satisfaction after surgery was high; 9 patients (9/14; 64%) rated each individual scar appearance item in the POSAS at or under 3 out of 10 (Fig. 3).
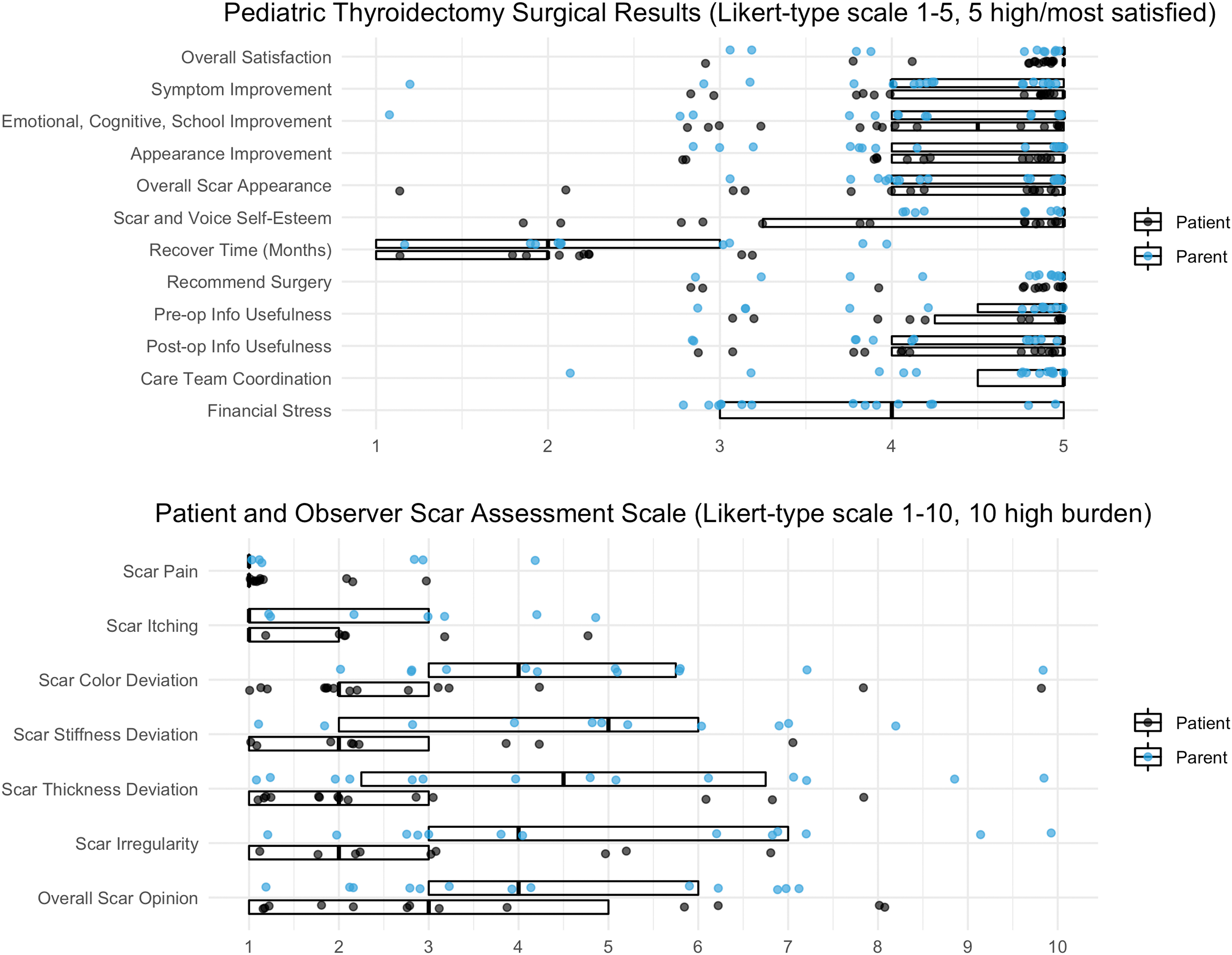
Satisfactions with definitive surgery outcomes. Patient and parent categorical responses to Pediatric Thyroidectomy Surgical Results (N = 18) and POSAS (N = 14) are reported with dots representing individual responses. Boxes provide median and interquartile range (first quartile–third quartile). Responses are scattered around Likert-type integers for distribution visualization. POSAS, Patient and Observer Scar Assessment Scale.
However, 3 patients (3/14; 21%) rated significant deviation (7 out of 10 or higher) in at least 1 POSAS item. Four patients (4/18; 22%) reported dissatisfaction (three out of five or lower) on the scar satisfaction measure of the Postoperative Surgical Satisfaction Scale. Parents rated more significant scar appearance deviations than patients with only 3 (3/12, 25%) parents rating each item at or under 3 out of 10 (Fig. 3). The total patient POSAS score (M = 11, IQR = 8.3–16.2, N = 14, possible score range = 6–60) was moderately associated with postoperative ThyPRO cosmetic complaints (ρ = 0.53, p = 0.049).
Discussion
Adolescent patients demonstrated significant disease-specific QOL and physical functioning improvements after TT for GD. These results mirror a recent study of patient-reported outcomes after definitive survey for adults in which patients experienced marked reduction in GD-associated symptom burden after TT. 11 However, this report is the only study of disease-specific reported outcomes and psychosocial functioning in adolescent patients undergoing TT. Overall satisfaction with TT was high with patient-reported improvements in symptomology and cognitive and mental functioning with minimal scar appearance concerns.
The findings of our study show significant GD-associated school-related and physical functioning burden that improved after TT. Poor patient-reported school functioning at baseline was associated with hyperthyroid symptoms, tiredness, cognitive impairment, depressive symptoms, and emotional lability with negative social impact. Resolution of the hyperthyroidism symptoms and cognitive impairment after TT was significantly associated with improvements in school-related functioning.
The baseline findings from our cohort extend the results of a recent study by Lane et al reporting depressed psychosocial functioning among adolescents and young adults with GD 39 and are impactful considering the importance of high school performance on future education and/or employment. 2 Furthermore, shorter interval between TT and ATD initiation was associated with greater reported symptom and physical/psychosocial functioning improvement, suggesting that TT may be preferred over sustained ATD maintenance for some patients, especially those with poorly controlled hyperthyroidism and TED.
Pediatric GD is associated with a low incidence of acute inflammatory TED and associated risk to vision, yet 30% of patients have GD-associated proptosis. 17 This study suggests that GD-associated eye symptomology is relatively low compared with other physical and cognitive manifestations of pediatric GD, yet there was a decrease in symptoms after TT (Table 2 and Fig. 2). These findings are significant considering potential exacerbation of TED from RAI and the negative impact that proptosis may have on physical appearance and self-esteem. 12,40
Surgical intervention for GO is uncommon, 41 –43 and this study is insufficient for assessing the impact of eye surgery on adolescent disease-specific QOL, warranting future exploration of the effects of orbital decompression on adolescent psychological functioning. In addition, with the recent FDA approval of teprotumumab for GD-associated TED in patients >18 years of age, the impact of nonsurgical treatment options for adolescent patients who have reached final height should be explored. 44,45
Patients and parents reported overall satisfaction and minimal concerns with the thyroidectomy scar. Scar appearance satisfaction may be due to the quality-of-care and low rate of complications associated with high-volume surgeons. However, it is important to counsel patients and their caregivers that ∼20–25% of patients may report intermediate or high scar irregularities and dissatisfaction with scar appearance (Fig. 3). High total patient POSAS scores were associated with greater cosmetic complaints, suggesting that some patients considered their surgical scar as a burden that affected their QOL after TT.
This observation highlights a need to further explore opportunities to reduce the size of the surgical scar and further investigate ways to reduce or eliminate scar formation. 46 Scarless surgical approaches for thyroid removal are being increasingly performed and may be an option for adolescent patients seeking to avoid RAI and prominent or unpleasant surgical scars. 47
Limitations of the study include sample size, which limited deeper exploratory analyses, especially survey associations with TFTs. There is also potential bias as 17 (46%) patients enrolled in the study did not complete the postoperative surveys. Attrition bias was observed in response rate drops for surveys appearing later in the questionnaire, specifically with items in the EUGOGO-QOL and POSAS surveys. PSQ and BESAA did not show considerable changes after TT, presumably from the nonspecific nature of the questionnaire items to thyroid-specific QOL.
While qualitatively screened for content validity, the ThyPRO, PSQ, and EUGOGO-QOL instruments have not been validated in adolescents and may not match content validity of the PedsQL and BESAA surveys. The Parent Rating Scale, Motivations for Definitive Surgical Treatment Questionnaire, and Postoperative Surgical Satisfaction Scale are unvalidated measures that may suffer from acquiescence bias. Without a control group and randomization between GD treatment options, conclusions about QOL improvements specific to TT cannot be definitive. Further studies are needed to compare the impact of TT versus RAI on pediatric QOL. 13
Conclusions
This study of adolescent patients with GD identifies significant improvements in disease-specific QOL and psychosocial functioning after TT with overall patient and family satisfaction. TED symptoms and scar appearance concerns from surgery were minimal in this cohort. These results suggest that TT is a good option for adolescents with GD that carries minimal scar appearance concerns when performed at a high-volume surgical thyroid center with low-complication rates.
Statement of ethics
This prospective study involving human subjects was reviewed and approved by the Children's Hospital of Philadelphia Institutional Review Board (CHOP IRB No. 15-012163). Written informed consent from the participant and/or participant's legal guardian was attained per CHOP IRB.
Footnotes
Authors' Contributions
S.H. contributed to conceptualization, writing—original draft, investigation, formal analysis, and visualization. J.A.B. carried out conceptualization, writing—original draft, investigation, and data curation. A.I. was involved in conceptualization, investigation, and writing—review and editing. T.P. took charge of conceptualization, investigation, and data curation. L.S. carried out conceptualization, investigation, and data curation.
K.K. was involved in conceptualization and writing—review and editing. N.S.A. contributed to conceptualization and writing—review and editing. W.R.K. undertook conceptualization and writing—review and editing. L.M. was in charge of conceptualization, writing—review and editing, supervision, and project administration. A.J.B. was in charge of conceptualization, writing—original draft, investigation, supervision, funding acquisition, and project administration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by The Children's Hospital of Philadelphia Frontier Program's Grant (GRT-00000495).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1