
Abstract

A
However, the probability of survival changes over time, especially when patients have survived for a certain period of time. Our study is the first to estimate the survival of patients with ATC using annual hazard rate of cancer mortality and conditional survival (CS). The death hazard depicts the death hazard at any instant among the remaining individuals at risk, enabling a better understanding of the time-specific risk of death. 4 CS estimates the probability that a patient will survive some additional time, given that the patient has already survived for a period of time. 5
We used data from the Surveillance, Epidemiology, and End Results (SEER) database of the National Cancer Institute. We identified patients diagnosed with ATC between 2004 and 2019 using the histopathology codes of the International Classification of Disease for Oncology (3rd edition; ICD-O-3; code 8021/3 [carcinoma, anaplastic, not otherwise specified]). Patients with more than one type of primary cancer, uncertain TNM stage, or unknown survival times were excluded. Because the data in the SEER database were anonymized and publicly available after obtaining permission, this study was considered exempt from review by the Institutional Review Board of the First Hospital of China Medical University. The primary endpoint was disease-specific survival (DSS), which was measured from the time of diagnosis to death due to ATC.
Actuarial DSS was estimated using the Kaplan–Meier method and compared using the log-rank test. Annual hazard rates were evaluated using the maximum likelihood estimate from a piecewise exponential model, and graphics were displayed using the kernel smoothing method. CS was defined as the probability of surviving another year or month, given that a person has already survived for x years or months, and can be expressed mathematically as follows: CS(x|y) = S(x+y)/S(x), where S(x) represents overall survival at x years or months. CS was calculated using life-table survival data. All statistical analyses were performed using the Stata statistical software package (version 16.0; Stata Corporation Ltd., College Station, TX, USA). A two-tailed p-value <0.05 was considered statistically significant.
We included 1080 patients, followed for a median of 3 months (interquartile range [IQR], 1–7 months). The median age at diagnosis was 69 years (IQR, 60–79 years). In terms of demographic characteristics, 59.8% were females and 78.4% were White. According to the 8th edition of the TNM staging system, the majority of patients had stage IVB (21.9%) and IVC (71.8%) disease. Only 6.3% patients had stage IVA disease. In total, 595 (55.1%) patients underwent thyroidectomy, whereas 609 (56.4%) and 486 (45.0%) patients received radiation therapy and chemotherapy, respectively. Of the 1080 patients, 832 (77.0%) died due to ATC.
Moreover, 92.9% of deaths occurred within the first year after diagnosis, with the majority (78.6%) within the first 6 months. The 1-month, 6-month, and 1-year DSS rates of the overall population were 83.1% ± 1.2%, 37.5% ± 1.6%, and 21.0% ± 1.4%, respectively (Fig. 1a). The 1-month DSS rates of patients with stage IVA, IVB, and IVC disease were 91.0% ± 3.5%, 90.6% ± 1.9%, and 80.1% ± 1.5%, while the 1-year DSS rates were 53.3% ± 6.6%, 36.5% ± 3.4%, 13.1% ± 1.4%, respectively (Fig. 1b). There were statistically significant differences among different TNM stages (p < 0.001). Age at diagnosis, TNM stage, surgery, radiation therapy, and chemotherapy were found to be independent prognostic factors for DSS in a Cox proportional hazards regression model.
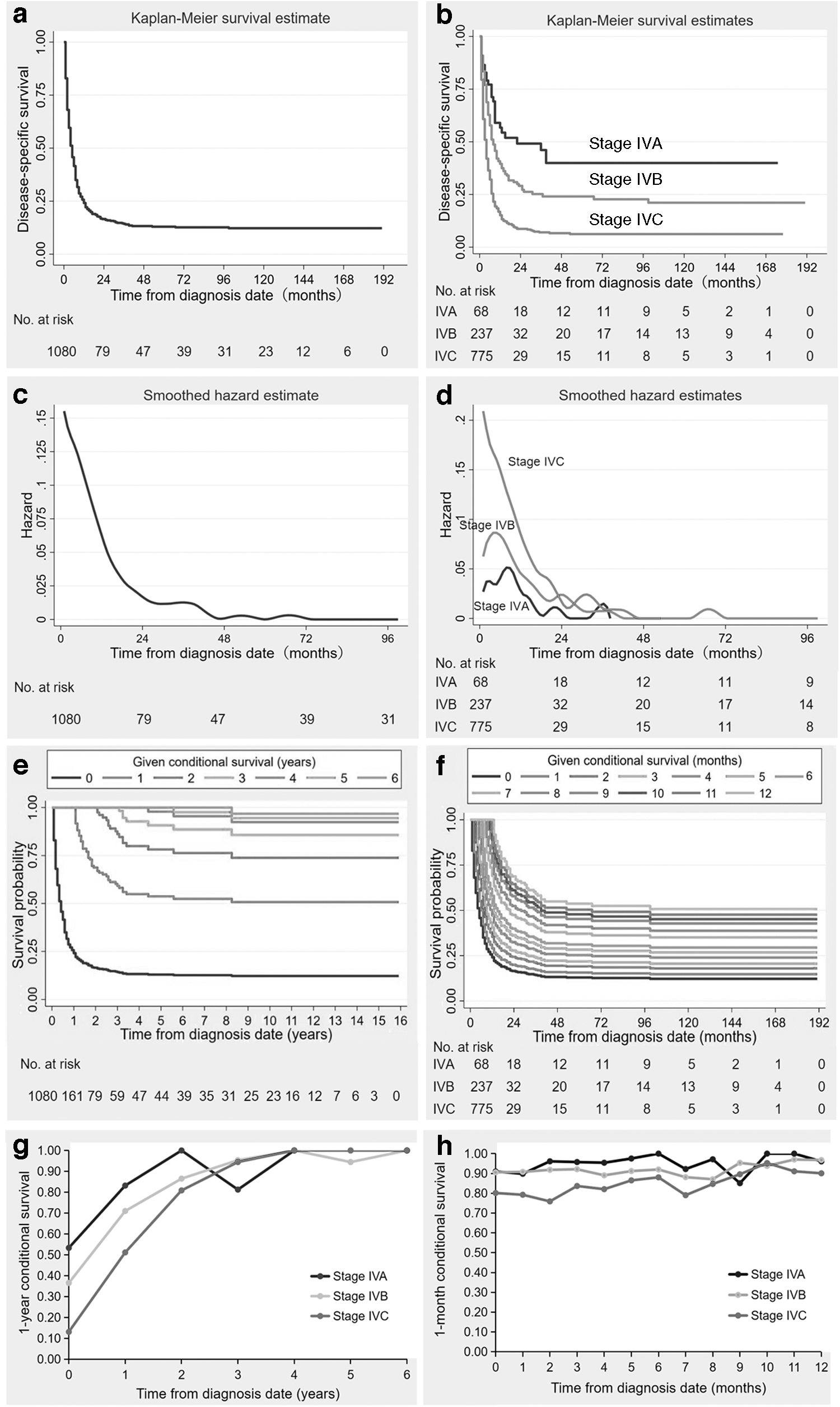
Kaplan–Meier curves for actuarial DSS of the entire cohort (
The annual hazard curve of ATC-specific mortality for the entire study population showed a downward trend from fast to slow without an obvious peak. It fell rapidly from the beginning until about 1.5 years after diagnosis, followed by a relatively slow decline until the end. When stratified based on TNM stage, the death hazard curve of patients with stage IVC disease was the highest and declined more rapidly and obviously than that of patients with stage IVB and IVA disease until two years after diagnosis. Subsequently, the three curves intersect each other. This means that patients with more aggressive disease were more likely to die in the first two years after diagnosis; thereafter, this trend was not sustained (Fig. 1c, d).
The probability of survival increased per year relative to the total survival time. Considering that the majority of patients died within the first year, we estimated the one-year and one-month conditional DSS, respectively. The probability of achieving 1-year conditional DSS increased from 21.0% [CI: 19.8–22.3] directly after diagnosis to 64.1% [CI: 60.9–67.3], 87.6% [CI: 83.2–92.0], 91.1% [CI: 86.5–95.7], 97.8% [CI: 92.9–99.8], and 97.6% [CI: 92.7–99.6] per additional year (i.e., 1, 2, 3, 4, and 5 years), respectively. Thus, for example, for ATC patients who have survived one year, the DSS for the subsequent year was estimated to be 64.1%. The 1-month conditional DSS decreased from 83.1% directly after diagnosis to 82.8% at 1 month, and then increased to 87.3% and 91.1% at 3 and 6 months, respectively.
The probability of conditional DSS for patients who survive up to a certain time point, based on how long they have already survived, is shown in Figure 1e and f. The curve of one-year conditional DSS showed a more rapid upward trend, whereas the curve of one-month conditional DSS exhibited a slow and fluctuating upward trend. Furthermore, changes in conditional DSS over time were more substantial in patients with advanced TNM stages. The one-year and one-month conditional DSS at different time points for patients with different TNM stages are presented in Figure 1g and h.
One of the most important findings of this study is that the annual hazard curve of cancer mortality showed a downward trend from fast to slow without an obvious peak. The death hazard curve of ATC differs from that of papillary thyroid cancer (PTC) reported in our previous study, 6 which presented a double-peaked distribution. The death hazard rate of ATC was significantly higher than that of PTC. 6 In addition, a steeper curve was observed in patients with a more advanced TNM stage, which is consistent with the findings in other malignancies. 7,8
Another important finding is that our results demonstrated that improved survival probability of ATC patients was strongly dependent on the time elapsed after diagnosis. In our study, the 1-year conditional DSS increased from 21.0% directly after diagnosis to 64.1% 1 year after diagnosis. This indicates that if the disease could be effectively controlled within one year after diagnosis, whether it is due to less aggressive disease or treatment, there would be a higher probability of surviving another year. Moreover, this possibility increases with increased survival time. It is encouraging to note that both the one-year and one-month conditional DSS exhibited an upward trend. Furthermore, we observed that patients with advanced TNM stage showed the greatest improvement. This phenomenon has also been observed in other types of thyroid cancer 9 and other malignancies. 10,11
The strengths of our study include its large cohort with a sufficient sample size, nationally representative population, and long-term follow-up. However, there are several limitations. The time span of patients included in this study is relatively long (2004–2019) to enable inclusion of a larger number of patients, but this may also create treatment heterogeneity in the data set. Treatment information recorded in SEER is limited (i.e., no radiotherapy dose or chemotherapy regimen is recorded); therefore, we did not attempt a subgroup analysis by treatment modality.
The changes in treatment patterns for ATC, including the use of more novel targeted therapies, were also not incorporated in the analyses. To explore the impact of time frame of diagnosis, we compared subgroups of patients. We observed that more recently diagnosed patients (2017–2019) had a better prognosis than those treated in prior years (2004–2016; median DSS: 5 months vs. 3 months, p < 0.001). Finally, this was a retrospective study based only on a U.S. population, which may be subject to selection bias and limits generalization to other populations.
Using data from the SEER registry, we have shown the improving conditional DSS for ATC. This information is valuable in considering survivorship care of ATC patients beyond the first year after diagnosis.
Footnotes
Authors' Contributions
W.D., T.O., and H.Z. participated in the design. W.D., X.J., J.X., D.Z., and P.Z. contributed to data collection, data analysis, visualization, and interpretation of the results. W.D. wrote the article. All the authors reviewed the article, contributed to the discussion, and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.