
Abstract
Background:
Before the development of antithyroid drugs in the 1940s, treatment of Graves' hyperthyroidism was primarily surgical. Surgical mortality was quite variable, but a significant minority of patients died during or after surgery.
Summary:
In 1936, Karl Compton, President of the Massachusetts Institute of Technology, in a lecture attended by Massachusetts General Hospital physicians, suggested that artificially radioactive isotopes might be useful for studying metabolism. By 1942, Hertz and Roberts reported on the successful use of radioactive iodine (RAI) to treat Graves' hyperthyroidism. RAI uptake was subsequently demonstrated in well-differentiated thyroid cancer metastases. In 1948, Seidlin demonstrated stimulation of uptake in thyroid cancer metastases by thyrotropin (TSH). By 1990, 69% of endocrinologists in North America recommended RAI for Graves' hyperthyroidism. Currently RAI is less frequently used for Graves' hyperthyroidism, related to concerns about exacerbation of thyroid eye disease, about radiation exposure, and about potential adverse consequences of permanent hypothyroidism. Similarly, RAI was administered to the majority of patients with thyroid cancer for decades, but its use is now more selective.
Conclusions:
RAI is a remarkable example of interinstitutional cooperation between physicians and scientists to transition from bench to bedside in only three years. It is the model for a theranostic approach to disease (the simultaneous use of a radioactive drug for diagnosis and therapy). The future of RAI is less certain; inhibition of TSH receptor stimulating antibodies in Graves' disease and more precise targeting of genes that drive thyroid oncogenesis may diminish the use of RAI. Alternatively, redifferentiation techniques may improve the efficacy of RAI in RAI-refractory thyroid cancer.
The Prelude
In the early 1930
Other therapies for hyperthyroidism were of uncertain efficacy. The Massachusetts General Hospital (MGH) Thyroid Clinic began studying external beam radiation in 1917, reporting cures in up to one-third of patients and improvement in another third (1924). However, the practice was largely abandoned by 1930. Hyperthyroid patients received 80–120 r (cGy) weekly for 8–10 weeks or 300 r (cGy) every other week for 8–12 cycles, either as a stand-alone therapy or (after an additional 3-week wait) as a prelude to surgery. Multiple courses of therapy might be administered. Debilitated patients were sometimes treated with radium to little effect (2,3). In contrast, modern external beam radiation for head and neck cancer delivers 5000–6000 r (cGy), causing hypothyroidism in most patients.
Pharmacological (6 mg) doses of iodine produced variable but rapid (often within hours) improvement in symptoms and basal metabolic rate (BMR), with a peak effect at 10 days. Inhibition of thyroid hormone release is the likely mechanism. Higher doses of iodine did not have added benefit. BMR was the definitive laboratory test for hyperthyroidism. Unfortunately, Dr. James Howard Means noted that continuation of iodine might result in “intensification of the thyrotoxic picture” (4).
It was also well known that iodine was contraindicated for toxic nodular goiter. Preoperative iodine therapy became standard around 1922 (see last paragraph of “The Prelude”), which coincided with abandoning of iodine as stand-alone Graves' therapy. Currently, iodine therapy for Graves' hyperthyroidism is being revisited in Japan and other countries (5).
Subtotal thyroidectomy (defined as removal of four-fifth of the thyroid) was the definitive therapy for Graves' disease and was clearly effective, but patient mortality, initially due to uncontrollable hemorrhage and subsequently to thyroid storm and infections, was highly variable due to varying surgical skill.
Highly skilled surgeons such as the Australian surgeon Dunhill, the legendary Johns Hopkins' surgeon Halsted, and the Mayo Clinic surgeon Charles Mayo reported mortality of 2% to 6% in the early 1900s compared with a 33% mortality among those less skilled (6,7). More than 50% of the procedures were “staged,” with initial removal of one lobe and subsequent removal of the other. Prolonged bed rest, isolation in a dark room, circulation of ice water externally around the heart, injecting boiling water into the thyroid, and administration of thyroidectin were unsuccessful attempts to improve surgical outcome. Thyroidectin, an extract of milk or blood from thyroidectomized animals, was given orally in a futile attempt to mirror the successful use of thyroid extract in hypothyroidism.
In 1922, the addition of preoperative iodine (Lugol's solution 10 drops 2 or 3 times daily) by Plummer at the Mayo Clinic proved to be a turning point for Graves' surgery (7,8). Mortality at the Mayo Clinic decreased from 4% to 1–2% and the percentage of staged operations decreased from 50% to 2%. Pharmacological doses of iodine decreased thyroidal blood flow and inhibited thyroid hormone release. Plummer incorrectly hypothesized that iodinating putatively toxic poorly iodinated thyroxine would be beneficial. Despite preoperative use of iodine, in the 1930s, surgical mortality was still 8–10% at some institutions (9), and at 1 hospital, it varied from 2% to 7% depending upon the surgeon (2).
Discovery of Radioactive Iodine
In this context, on November 12, 1936, as part of a weekly lecture series at Harvard Medical School, Karl Compton, President of Massachusetts Institute of Technology (MIT), gave a lecture to students and faculty members entitled “What physics can do for Biology and Medicine.” Robley Evans, an MIT physicist, suggested discussing “artificially radioactive isotopes” and their potential for studying metabolism (10).
Remarkably, this was only two years after the description of the first artificially produced radioactivity by the married team of Frederic Joliot and Irene Curie (daughter of Marie Curie), publication of the first description of a cyclotron by Ernest Lawrence, and production of several short half-life (t½) radioisotopes by Enrico Fermi who used a radon–beryllium neutron source to bombard all known available elements. All four scientists subsequently were awarded the Nobel Prize.
Much of the following information is gleaned from Sawin and Becker (9,11). Four members of the MGH Thyroid Unit attended the lecture: James Howard Means (founder of the thyroid unit and chief of medicine at the MGH), Saul Hertz (head of the thyroid clinic), Earle Chapman, and Jacob Lerman (a thyroid unit clinicians in private practice). At the end of the lecture, Dr. Hertz asked whether iodine could be made radioactive. Compton was uncertain. In December 1936 he wrote to Hertz apologizing for his tardy response and confirmed that in 1934 Enrico Fermi had produced 128I, an isotope with a t½ of 25 minutes and a beta ray spectrum. By May 1937, Hertz announced research plans to study thyroid metabolism in rabbits and ultimately to treat Graves' disease.
Subsequent therapeutic plans included treating thyroid cancer. Thus began a remarkable collaboration between MGH physicians and MIT physicists to study radioactive iodine (RAI). Evans produced 128I by irradiating ethyl iodide with neutrons. Separating radioactive from nonradioactive ethyl iodide proved much easier than anticipated, as the energy of the 128I ruptured the ethyl iodide bond, releasing water-soluble iodide that was easily separated from the polar water-insoluble ethyl iodide.
Hertz and Evans demonstrated uptake of iodine in rabbit thyroids (using Geiger–Mueller counter) that was increased after injection of pituitary thyrotropin (TSH) extracts, in hyperplastic thyroids, and in early pregnancy. Their results were reported in 1938 only 1.5 years after the Compton lecture (12). They emphasized the importance of using as little carrier (“cold”) iodine as possible to maximize iodine uptake.
Physiological studies with RAI were performed in humans by Hamilton at Berkeley and by Leblond in Paris. Thyroid uptake of RAI was limited because Hamilton used a large amount (14 mg) of “cold” iodine. During a chance encounter in 1938, Hamilton asked the future Nobel laureate physicist/chemist Glenn Seaborg whether he could produce longer lived iodine isotopes. Seaborg asked how long a half-life he would like, and Hamilton answered “one week.” Within 8 days Livingston and Seaborg produced 3 (fortuitously) longer lived isotopes: 130I (t½ 12 hours), 131I (t½ 8 days), and 126I (t½ 13 days). Seaborg subsequently wrote: “And for me, it has a very personal meaning. Doctors used it to save my own mothers' life when she contracted hyperthyroidism, a disease similar to the one that killed her sister in the 1930s” (13). As a footnote to history, the University of Michigan had previously produced 131I but misidentified it as 131Te.
Initial MGH/MIT clinical studies were performed with 130I posted from Berkeley to the MGH by first class mail (Fig. 1). The Boston team soon realized that a cyclotron was necessary for more sophisticated studies with radioisotopes. In 1938, Compton and Roberts traveled to New York City to request funds from the New York-based John and Mary Markle Foundation. The same day they received a check for $30,000 that was sufficient to build a cyclotron. The MIT cyclotron was completed in 1940, the first cyclotron built exclusively for biological and medical use.

Dr. Saul Hertz using a multicounter that he designed to analyze the distribution of radioactive iodine in a volunteer. With permission from the Dr. Saul Hertz Archives.
Initially Hertz administered 130I to study Graves' patients before surgery. However, in January 1941, the first hyperthyroid patient was treated with a “radioactive cocktail” (i.e., RAI treatment) in a glass of water with MIT-manufactured 130I (contaminated with a bit of 131I). Although Hertz and colleagues assumed that the rapid discharge of energy from 130I was an advantage, ultimately the longer t½ of 131I made it the therapy of choice. At the insistence of Dr. Means, pharmacological doses of “cold” iodine (super saturated potassium iodide [SSKI] 6 drops twice daily) were administered 1–3 days to several weeks after RAI to “protect the patients against the mischief from thyrotoxicosis (when a) treatment of unknown efficacy was being tried out” (14).
The BMR returned to normal after several months. Twenty-two of the first 29 RAI-treated hyperthyroid patients had a “successful” outcome, defined as normalization of BMR several months after stopping “cold” iodine. The importance of “cold” iodine in the successful outcome was uncertain. The practice of administering “cold” iodine (SSKI twice daily beginning one week after RAI) continued at the MGH for many decades and appears to shorten the time to euthyroidism compared with RAI alone (15).
Hertz and Hamilton (who also successfully treated a series of hyperthyroid patients) presented abstracts at the American Society of Clinical Investigation meeting in 1942. The American Thyroid Association (ATA) (then the American Goiter Association) annual meetings had been cancelled for the duration of World War II. Although Dr. Hertz was particularly enthusiastic about RAI therapy for hyperthyroidism, Dr. Hamilton was more circumspect about the long-term effects of this “potentially lethal agent.” Preliminary results were published in 1942 (16).
When Hertz volunteered for naval duty in 1943, he asked Chapman to continue his clinical studies. Between May 1943 and March 1945, Chapman treated an additional 22 patients with RAI (primarily 130I with around 10% 131I). Using a higher dose of RAI (up to 79 mCi), without “cold” iodine, Chapman noted more radiation thyroiditis, radiation sickness, and early hypothyroidism.
Although Means asked Hertz to publish his study in 1943, Hertz declined believing that longer follow-up was necessary. In 1946, the studies of Hertz and Chapman were published separately in the same issue of the Journal of the American Medical Association (JAMA) (17,18). Fishbein, the JAMA editor, was suspicious of duplicate publication but was reassured by Means that these were separate studies; an editorial by Means was requested and was published anonymously (19). Coming full circle, a commentary by Dr. Compton was also included in that issue (20).
Amid accusations of misunderstanding, misappropriation, and academic fraud, the relationships between Hertz, Chapman, and Means were permanently fractured (for details see reference 9). Consequently, in 1946, Hertz moved to Boston's Beth Israel Hospital where RAI was being used to treat angina (21).
It may surprise the reader to learn that 2 of the first 29 patients were 9-year-old girls. In an era that long antedated the Geneva Conventions and institutional review boards, the guiding principles for clinical research were “the personal ethical standard of responsible physicians” (10). The experience of AD (one of these girls) is detailed by Daniels (22). She remembers her mother being told that the treatment might cause cancer, a concern that is currently resurfacing (see RAI for Hyperthyroidism). Seventeen years later (1958), AD had a thyroidectomy for a nodular goiter with recurrent hyperthyroidism; in 1996 she had surgery for a parathyroid adenoma causing hyperparathyroidism. Hyperparathyroidism is now a recognized long-term consequence of RAI therapy for Graves' hyperthyroidism (23). AD lived well into her 80s.
In 1942, RAI uptake was detected in a metastatic focus of well-differentiation thyroid cancer but not in coexisting poorly differentiated metastases (24). One of the coauthors of that report was Virginia Kneeland Frantz, the first woman president of the ATA (1961). A famous but unusual case of thyroid cancer was recounted in Life Magazine (1949) (Fig. 2) after its scientific publication (25). Post thyroidectomy, the patient had metastatic thyroid carcinoma with intractable life-threatening hyperthyroidism as well as debilitating bone pain. All the known metastatic areas took up RAI (using a Geiger counter) and several additional areas were discovered after RAI administration.
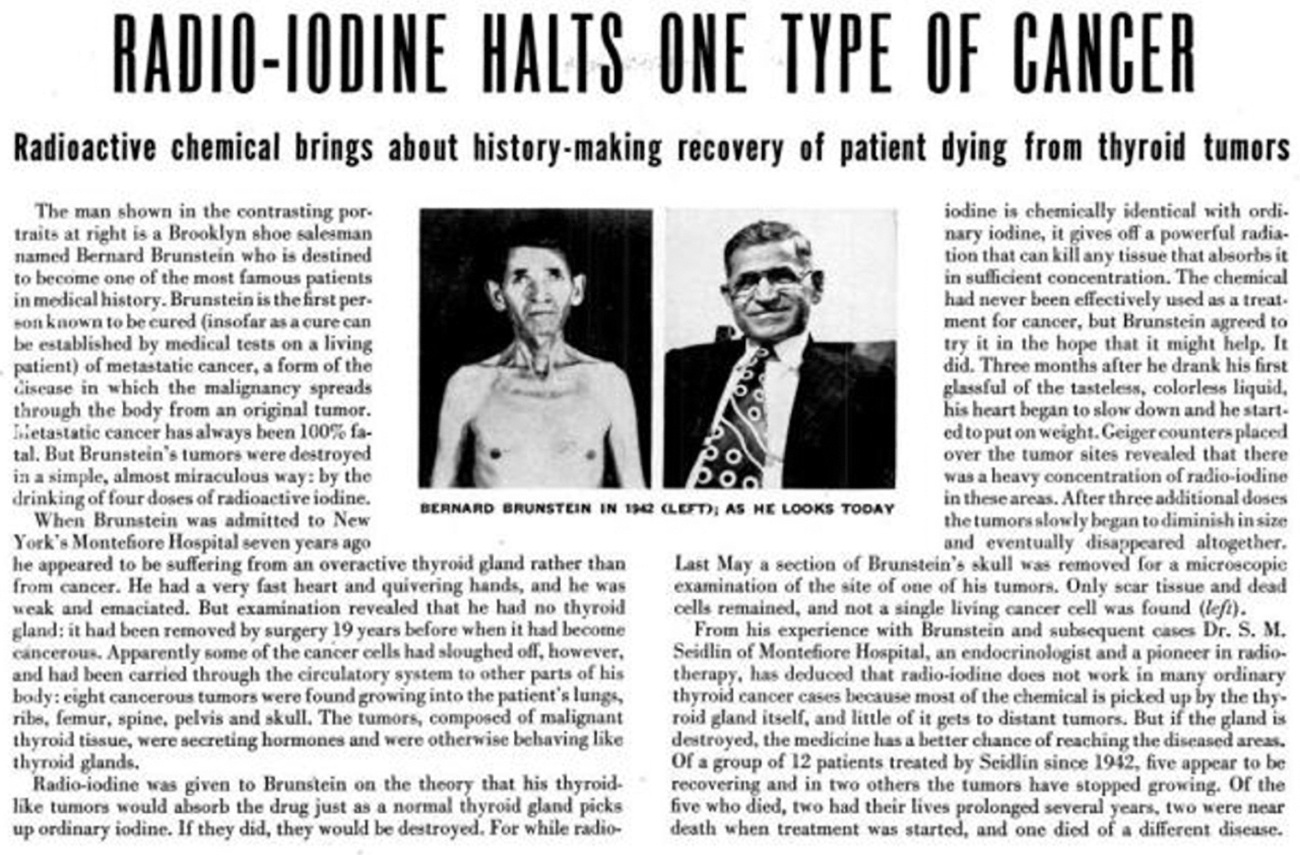
Radioiodine halts progression of thyroid cancer.72
After radioiodine administration, the patient's pain resolved, he gained weight, his BMR became normal, and some tumor shrinkage and resolution of radioiodine uptake by the tumor were achieved. In 1948, Seidlin demonstrated TSH induced stimulation of RAI uptake in metastases, a seminal observation (26).
In 1946 after World War II, 131I became generally available when the U.S. Atomic Energy Commission began to supply pure fission product 131I. RAI was approved by the Food and Drug Administration in 1972. There are currently 20 known radioactive isotopes of iodine. It is fortuitous that 3 of these isotopes are almost perfect for their purposes: 131I for therapy (t½ 8 days), 123I (t½ 13.2 hours) for scanning, and 125I (t½ 60 days) for sealed source brachytherapy, in vitro iodination and protein, and immunoglobulin iodination for imaging.
131I is primarily a beta emitter with a short path length that prevents damage to surrounding tissue; its gamma emissions (10%) permit post-therapy imagining. 123I is an almost pure high-energy gamma emitter, whereas 125I has low-energy photon emissions. Although the Berkeley group planned on testing the longer lived 126I, those studies never materialized.
Thyroid Imaging with RAI
In the early 20th century, there was no sensitive method of detecting radioactivity. The Geiger–Mueller tube (counter) was introduced in 1928 but was still quite insensitive. In 1949 Cassen and colleagues designed the first detector (scintillation counter) to record the “scintillations” that occur when gamma radiation is absorbed by certain crystals (27). Automated scintillation counters were primarily used in the 1950s to image the thyroid and to quantitatively calculate the thyroid RAI uptake to plan hyperthyroidism therapy. A thyroid image could take up to 90 minutes. Subsequent modifications included a variable light source proportional to scintillations developed by Kuhl, and focused collimators developed by Newell and colleagues.
Rectilinear scanners for imaging 131I, such as those developed by Picker International Corporation, were considered revolutionary but their use peaked in 1973. The rectilinear scanner was replaced by the Anger camera in the late 1970s. Currently gamma cameras are used for planar thyroid images (123I), while single-photon emission computed tomography is used for three-dimensional imaging for thyroid cancer (131I or 123I).
RAI for Hyperthyroidism
The efficacy of RAI for hyperthyroidism is no longer in doubt. The question of safety remains an important one.
Early clinical experience with RAI confirmed that high doses were associated with late-onset hypothyroidism, whereas lower doses failed to control the hyperthyroidism in many patients (28). The hypothyroidism incidence increased progressively over time even when initial rates were relatively low. Attempts to improve the outcome included “compensated low-dose RAI therapy” (29), dose calculations based on the thyroid gland size and RAI uptake (30), and fixed dose RAI (31). Ultimately, however, the goal of therapy for Graves' hyperthyroidism was near complete ablation of the thyroid gland, with permanent hypothyroidism as the desired final effect, as noted by the current ATA guidelines (32).
This may be particularly important for children, in whom neoplastic change may occur in nonablated remnant thyroid tissue (33,34). In addition, while increased mortality (primarily cardiovascular) was initially reported in patients who received radioiodine for hyperthyroidism, subsequent analysis found that excess mortality was found only during the period of ongoing treatment of hyperthyroidism with thionamides, and among patients who did not become hypothyroid (35).
Patient AD already mentioned developed recurrent hyperthyroidism with a large benign nodular thyroid. Currently, hypothyroidism is considered an effect rather than a “side effect” of RAI therapy. Additional RAI safety concerns include worsening Graves' ophthalmopathy (36) and late-onset primary hyperparathyroidism (23).
Despite initial concerns about malignancies post-RAI, the data of Ron et al. from the Cooperative Thyrotoxicosis Therapy Follow-up Study (CTTFUS) reassuringly found no link between RAI and cancer mortality (37). Ron did note an increase in thyroid cancer mortality after RAI treatment for toxic nodular goiter. However, the cancer controversy was reignited by a series of publications by Kitahara and colleagues (38,39) also utilizing the CTTFUS database.
They found a dose–response relationship between RAI dose and solid cancer mortality, although the solid cancer standard mortality ratios were the same among patients treated with radioiodine, surgery, or antithyroid drugs (39). Although not all investigators confirm these data (40), we support Kim's conclusion that Kitihara's studies “constitute a mandate for further research!” (41).
Declining Use of RAI for Hyperthyroidism
Whereas 69% of endocrinologists in North American recommended RAI for Graves' hyperthyroidism in 1990 (42), by 2011 the number was 60% (43) with a further decline to 33% by 2020 (44). At the MGH, hyperthyroidism treatment with RAI declined by 85% between 2006 and 2019. There are several potential reasons why patients are reluctant to choose RAI. One major concern is the risk of new or worsening Graves' orbitopathy (36). The post-RAI rise in thyrotropin receptor antibodies (TRAb) is the likely culprit; in contrast TRAb tend to decline after surgery or anti-thyroid drugs (ATD) (45). Evidence to support a protective role of glucocorticoids post-RAI has not stemmed this tide (46).
The decline in RAI use largely occurred before the Kitahara publications (38,39), but our patients increasingly report a nonspecific fear of radiation. Concern among our patients regarding the adverse consequences of permanent hypothyroidism may be an additional factor; our patients frequently cite internet articles that highlight patient dissatisfaction with treatment of hypothyroidism (47).
On the positive side, more patients are pleased with the option of long-term ATD therapy (48) or the opportunity for a remission, while avoiding hypothyroidism (49). Fortunately, studies show that severe ATD toxicity (agranulocytosis and liver failure) occurs almost exclusively in the first few months of therapy, thus mitigating some fears about long-term ATD use. Additional studies confirm the long-term (>10 years) safety of ATD (50).
RAI for Toxic Adenoma and Toxic Multinodular Goiter
Unlike Graves' hyperthyroidism, the goal of radioiodine in toxic adenoma is to ablate the autonomous tissues and preserve normal thyroid function (51). Given the low RAI uptake in nonautonomous areas due to suppression of TSH, one would anticipate a low risk of hypothyroidism after RAI for toxic adenomas and toxic nodular goiters, unless pretreatment with ATD normalized the serum TSH. Thus rates of hypothyroidism after RAI depend upon absorbed dose, goiter size, and prior antithyroid drug administration; the rate of hypothyroidism in one long-term study was 8%, 28%, 46%, and 60% after 1, 5, 10, and 20 years, respectively (52).
In addition, Graves' disease develops in up to 4% of RAI-treated patients with toxic nodular goiter (53) presumably due to an immune response to released thyroid antigens. After RAI administration, toxic nodules develop suspicious ultrasound features, including calcifications with increasing (more suspicious) European-Thyroid Imaging, Reporting, and Data System scores reported by one year post-RAI (54).
RAI and Thyroid Cancer
One cannot deny the spectacular success of RAI in treating some patients with thyroid cancer, particularly those with low-volume distant metastatic disease. Despite certainty by those arguing for and against RAI in certain situations, it remains uncertain as to who should receive RAI and will likely benefit from it, and what dose is appropriate. A randomized controlled trial of RAI for important cancer outcomes (structural or radiographic evidence of recurrence, or increased thyroglobulin) has finally been published (55) but not for the lack of effort in the past. In the 1970s, Dr. Leslie DeGroot applied to the National Institute of Health to fund randomized-controlled trials of RAI for thyroid cancer. Despite a high score for these proposals, funding was denied.
It may be instructive to review some of the history of the RAI thyroid cancer controversy. Between 1960 and 1975, fewer than 10% of papillary thyroid cancer (PTC) patients at the Mayo Clinic (PTC) received RAI, based on their experience with low-risk patients who had a 99% disease-specific survival without RAI (56). Mazzaferri's et al.'s 1977 and 1981 landmark studies (57,58) reported decreased recurrences and mortality after RAI for PTC >1.5 cm. Subsequently almost 70% of the Mayo Clinic PTC patients received RAI, a practice not necessarily supported by their data.
A striking example of the divergent opinions is the commentaries of two North American nuclear medicine “giants” from Ann Arbor based on the same database: Beierwalters “…there is no question today that we should ablate normal thyroid tissue as part of the treatment of well-differentiated thyroid carcinoma” (59) and Sisson “…the aggregate of evidence does not convincingly demonstrate that ablation of small remnants—and especially those remote from the primary tumor—lowers the rate of recurrent cancer” (60).
By the 1980s, most patients with well-differentiated thyroid cancer (WDTC) larger than 1.5 cm received postoperative RAI in the United States and Europe. However, since 1999 this practice has declined in the United States. For example, data from California report that RAI for localized disease declined from 54.6% (1999) to 29.6% by 2015 (61), whereas at the Mayo Clinic it declined from 62% in 1990 to 25% in 2020 (62).
The decline in RAI for thyroid cancer was likely fueled by several concerns: the very low risk of death in low-risk patients, the uncertain benefit of RAI in preventing recurrences (63), and the concern about second primary malignancies related to high-dose RAI (64). In addition, acute RAI side effects (nausea and vomiting [rare] and painful salivary glands) and chronic side effects (permanent dry mouth, nasolacrimal gland dysfunction, recurrent sialadenitis, and delayed reproduction) need consideration. These issues led the ATA to argue against RAI for low-risk thyroid cancer (65), whereas European nuclear medicine specialists did not support this approach (66), refusing to endorse the ATA guidelines.
A randomized phase 3 trial assessed evidence for recurrence after adjunctive radioiodine remnant ablation for low-risk patients compared with no radioiodine; after 3 years no radioiodine was noninferior to radioiodine (55). Nonetheless, despite increasing evidence for little efficacy in low-risk patients, the controversy continues. In the absence of randomized controlled trials, the data support the use of radioiodine for intermediate and high-risk patients (63). The recent Martinique Conferences are an attempt to bridge the divide (67).
What is the Legacy of RAI?
The early history of RAI is a model for remarkably efficient translational research, from bench (1938) to bedside (1941) in less than three years. It is also a model for interinstitutional research cooperation. RAI remains an important therapeutic option for hyperthyroidism including postsurgical recurrent hyperthyroidism. RAI is effective in shrinking obstructing goiters when surgery is to be avoided (68).
The term theranostics (use of the same or similar radioactive compound for diagnosis and therapy (69) is new, but RAI is the paradigm for a theranostic approach to disease. Desire to image the thyroid was the major impetus for the specialty of nuclear medicine, although other radionuclide imaging preceded RAI. Along with estrogen for prostate cancer (1941), RAI was one of the first targeted therapies for cancer.
What Might the (Distant) Future Bring for RAI?
Ideal therapy for Graves' disease would specifically (and safely) inhibit the production of TRAb, thus protecting the “innocent bystander” (thyroid) and effectively treating the hyperthyroidism, potentially making RAI obsolete for that purpose.
Ongoing and future studies will determine who will truly benefit from RAI treatment for thyroid cancer. In addition, future advances will determine whether RAI use will increase as we explore ways to “redifferentiate” WDTC cancers (70) that frequently have lost their ability to concentrate iodine, or whether radioiodine use will decrease as advanced targeted therapies become more effective and less toxic.
Coda
In October 2021 (80 years after the initial RAI treatment), largely due to the efforts of his daughter, Barbara Hertz (71), the American Chemical Society honored Dr. Hertz and the medical use of RAI with a National Historical Chemical landmark designation at the MGH. Based on the legacy of RAI, it is ironic that when Hertz submitted his study for the American Goiter Association Van Meter Award (1946), he received only honorable mention.
Footnotes
Authors' Contributions
Both authors researched, wrote portions of this article, and reviewed the entire article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.