
Abstract
From low-resolution images in the 1960s to current high-resolution technology, ultrasound has proven to be the initial imaging modality of choice for thyroid application. Point-of-care ultrasound has brought the technology to the thyroid specialist. Combined with physical examination, it provides real-time information regarding goiter, thyroid nodules, and thyroid cancer. Ultrasound-guided fine-needle aspiration biopsy has become the accepted norm, with biopsies rarely performed using palpation alone. Advantages of ultrasound-guided biopsy include precise placement of the needle within the nodule, selective sampling of areas with suspicious features, and accurate direction of the biopsy needle to actively growing viable cells in the periphery of the nodule. Education of endocrinologists in thyroid ultrasound began in the late 1990s and by 2016 more than 6000 clinicians had completed an ultrasound course. Concurrent with this rapid expansion of use of thyroid ultrasound was a rise in the diagnosis of small papillary carcinomas, which might have otherwise remained indolent and undetected. The 2009 American Thyroid Association Guidelines for the Management of Thyroid Nodules and Thyroid Cancer recommended biopsy for all solid hypoechoic nodules measuring larger than 1 cm. Attempting to decrease the frequency of biopsies of low-risk nodules, subsequent guidelines have focused on identifying and selectively biopsying those thyroid nodules at higher risk of clinically significant carcinoma based on ultrasound appearance. A major role for thyroid ultrasound has been in both preoperative staging and mapping to help determine the extent of surgery, as well as postoperative monitoring for locoregional soft tissue or lymph node metastases. With the recognition that the increase in papillary carcinoma was predominantly a result of early diagnosis of small often indolent cancers, active surveillance has become a promising management strategy for papillary thyroid microcarcinomas. Thyroid ultrasound is essential to active surveillance of thyroid cancer. Easy access to high-quality ultrasound studies is a requirement for a successful active surveillance program. Thyroid ultrasound has been used to facilitate interventional procedures, including treatment of thyroid nodules, treatment of recurrent thyroid cancer, and therapy of papillary thyroid microcarcinoma.
Introduction
The thyroid is well suited to ultrasound study because of its superficial location, vascularity, size, and echotexture. 1 Ultrasound of the thyroid was not available before the 1960s. Now it is the modality of choice for most thyroid imaging, and “point-of-care” ultrasound has made it accessible to the thyroid specialist. It has a proven value in evaluation of goiter and thyroiditis, thyroid nodules, population evaluation for iodine deficiency, and as an adjunct to thyroid biopsy. Comprehensive cervical ultrasound is essential in pre- and postoperative thyroid cancer care. Ultrasound skills are a prerequisite for interventional procedures, including alcohol and thermal ablation. Consistent high-quality thyroid ultrasound is indispensable in the active surveillance of thyroid cancer.
An article published in 2004 reviewed the development of ultrasound technology. 1 Since then, there have been minor refinements in technology, but significant changes in utilization and application of thyroid ultrasound. This article will discuss the rapid growth of thyroid ultrasound for the past two decades, its role in the overdiagnosis of thyroid cancer, and resulting efforts to use thyroid ultrasound in a more appropriate and rational manner. It will focus on the central role of ultrasound in the management of thyroid cancer.
Early Use of Ultrasound
Medical ultrasound was developed based on technology used in sonar navigation, using a “pulse-echo” technique. Early in the 1950s, the first medical applications of imaging by pulse-echo reflection were performed. Later in that decade John Julian Wild reported the observation that gastric malignant tumors were more echogenic than normal gastric tissue. 1 Early in the 1960s the first studies utilizing two-dimensional B-mode ultrasound scanning in gynecology were published.
Ultrasound for Thyroid Imaging
The earliest use of ultrasound for thyroid imaging began in the late 1960s. In 1967, Fujimoto et al reported data on 184 patients studied with low-resolution B-Mode ultrasound and reported that abnormal thyroid tissue showed increased echogenicity. Areas of absent echoes suggested cystic composition and a pattern of strong internal echoes within a thyroid nodule was felt to correspond to carcinoma. 2
In 1971, Manfred Blum published a series of A-mode ultrasound images, demonstrating the ability of ultrasound to distinguish solid from cystic nodules and accurately measure their dimensions. 3
Development of grayscale display provided greatly improved images, and in 1974 Crocker et al published a report on the grayscale imaging of thyroid cancer. Despite very low-resolution images they described “low amplitude sparse and disordered echos” characteristic of thyroid malignancy. 4 Subsequent postacquisition processing of the image, including edge enhancement and noise reduction, greatly improved the quality of the displayed image. Compound spatial imaging became available early in the 21st century. This technology combines multiple images obtained from different angles and reconstructs them into a single image.
The result is much less noise, sharper definition, and a more realistic appearing ultrasound displayed (Fig. 1). Additional advances in technology, including higher frequency transducers and more rapid frame rates have further improved image quality. While the development of matrix array transducers has both improved image quality and enabled three-dimensional (3D) image acquisition, 3D imaging has not demonstrated clinical advantage and has not entered common use. Similarly, elastography and contrast-enhanced ultrasound remain promising techniques, but have not yet been proven to be practical in clinical use.
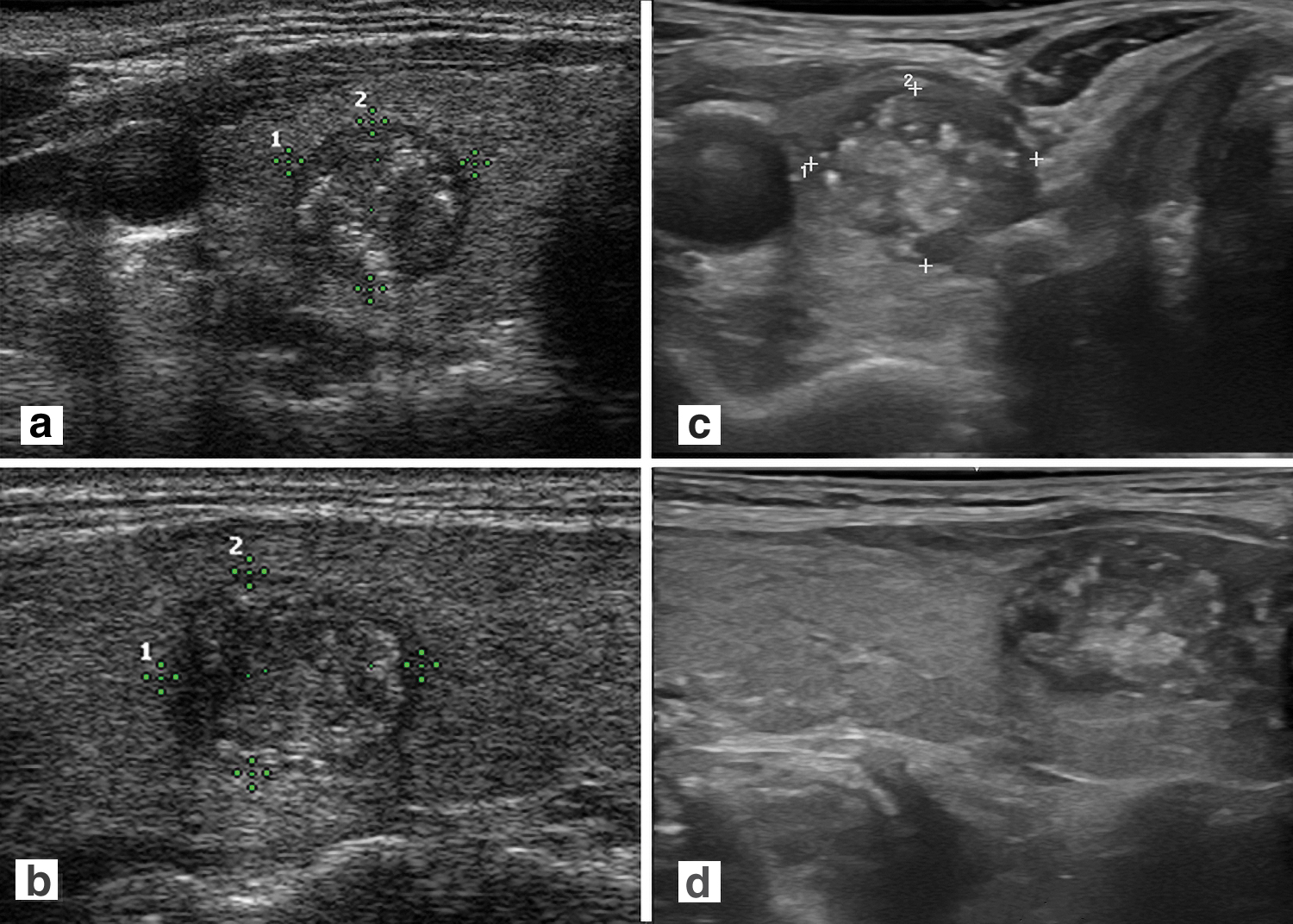
Compound spatial imaging. (
Ultrasound Guidance for Fine-Needle Aspiration of Thyroid Nodules
In 1977, Walfish et al recommended combining ultrasound guidance with fine-needle aspiration biopsy. 5 In the majority of patients with a prior “nondiagnostic” biopsy, an adequate sample could be obtained when ultrasound-guided biopsy was performed. 6 Advantages of ultrasound-guided biopsy include precise placement of the needle within the nodule and accurate direction of the biopsy needle to actively growing viable cells in the periphery of the nodule. Ultrasound guidance enables targeting of the solid components of complex nodules, allows selective sampling of areas with suspicious features, and helps avoid introducing the needle through large blood vessels. Ultrasound-guided fine-needle aspiration biopsy has become the standard, with biopsies rarely performed using palpation alone.
Point-of-Care Thyroid Ultrasound Performed by Endocrinologists
Despite growth of point-of-care ultrasound in obstetrics and gynecology, before the turn of the century thyroid ultrasound imaging remained in the domain of radiology. Radiology reports were often sparse, rarely providing three dimensional measurements, and often lacking details regarding the characteristics of nodules, or the presence or absence of lymphadenopathy.
In 2000, Susan Mandel and her colleagues reported that thyroid ultrasound altered the clinical management in 63% of patients referred to the thyroid nodule clinic at the Brigham and Women's Hospital. 7
In 2004, Baskin wrote an editorial titled “Thyroid Ultrasound—just do it.” 8 Citing the above report, 7 the editorial reviewed indications for ultrasound imaging and discussed the value of combining ultrasound with fine-needle aspiration biopsy. Encouraging point-of-care thyroid ultrasound, he stated that “clinicians must become proficient in the use of ultrasound and ultrasound-guided FNA as extensions of the physical examination. We cannot afford to deprive our patients of the many benefits of these procedures.”
Education and Expansion of Use
Point-of-care thyroid ultrasound performed by endocrinologists grew rapidly in the late 20th century. Education in thyroid ultrasound began at several major medical centers and the American Association of Clinical Endocrinologists (AACE) offered the first educational course specific to thyroid ultrasound in 1998. Under the direction of Baskin and Daniel Duick, 53 endocrinologists were taught to perform diagnostic ultrasound and ultrasound-guided fine-needle aspiration biopsy. Three hundred endocrinologists were trained for the next two years. 9 With the support of its CEO, Donald C. Jones, AACE took the lead in thyroid ultrasound education, offering multiple two-day courses every year, as well as short courses linked to the annual meeting. The Endocrine Society and American Thyroid Association also began holding short courses at their annual meetings.
Endocrine University was established in 2002 by AACE. A four-day course, including two days of didactic and “hands on” instruction in thyroid ultrasound and biopsy was provided to senior endocrine fellows. Held at the Mayo Clinic in Rochester, Minnesota, under the direction of Gharib, 10 more than 3000 endocrine fellows have attended Endocrine University and received training in thyroid ultrasound. By 2016, more than 6000 participants had completed an AACE ultrasound course. 9
Cautionary Tales—Overdiagnosis of Thyroid Cancer
In 2008, Cronan opined in Radiology, “Thyroid Nodules: Is it time to turn off the ultrasound machines?” 11 addressing the controversy of evaluating nonpalpable nodules with ultrasound. With technology now permitting detection of 2–3 mm nodules, the editorial discussed the impact of identifying small nodules. Acknowledging that 67% of the population evaluated with ultrasound have a small incidental nodule, he indicated that this would represent a potential reservoir of 150 million Americans with thyroid nodules. He noted that there had been a 2.4-fold increase in the reported incidence of thyroid nodules for the prior three decades, and a 3-fold increase in thyroid aspiration biopsies between 1995 and 2005.
Despite most guidelines at that time recommending biopsy only if nodules exceeded 1 cm, he stated that he was routinely asked to perform biopsy on 5–10 mm nodules. He projected that if all thyroid nodules in the American population were evaluated, and all cancers detected were treated, the surgical cost alone “would conservatively reach 30 billion dollars.”(sic) It became clear that rather than turning off ultrasound machines, guidelines were needed regarding the evaluation of sub-centimeter nodules and diagnosis of subclinical thyroid cancer.
The overdiagnosis of thyroid cancer was addressed in landmark articles by Davies and Welsh in 2006 and 2014. In 2006, they reported on the increasing incidence of thyroid cancer in the United States, noting that there had been a doubling of thyroid cancer diagnoses in the prior decade, while the mortality rate for thyroid cancer had not significantly changed. Eighty-seven percent of the increase was due to tumors 2 cm or smaller, many nonpalpable and found either by ultrasound screening or as an incidental lesion on CT or MRI. 12
In a subsequent 2014 report they again analyzed the results of Surveillance, Epidemiology, and End Results (SEER) data, indicating that there had been close to a threefold increase in incidence of thyroid cancer between 1975 and 2009. Despite the increase in cancer diagnosis the mortality rate had remained stable and extremely low (Fig. 2). 13 Figure 2, graciously provided by Davies, extends the data, and appears to show stabilization of the incidence of thyroid cancer diagnoses for the past decade since their prior report.
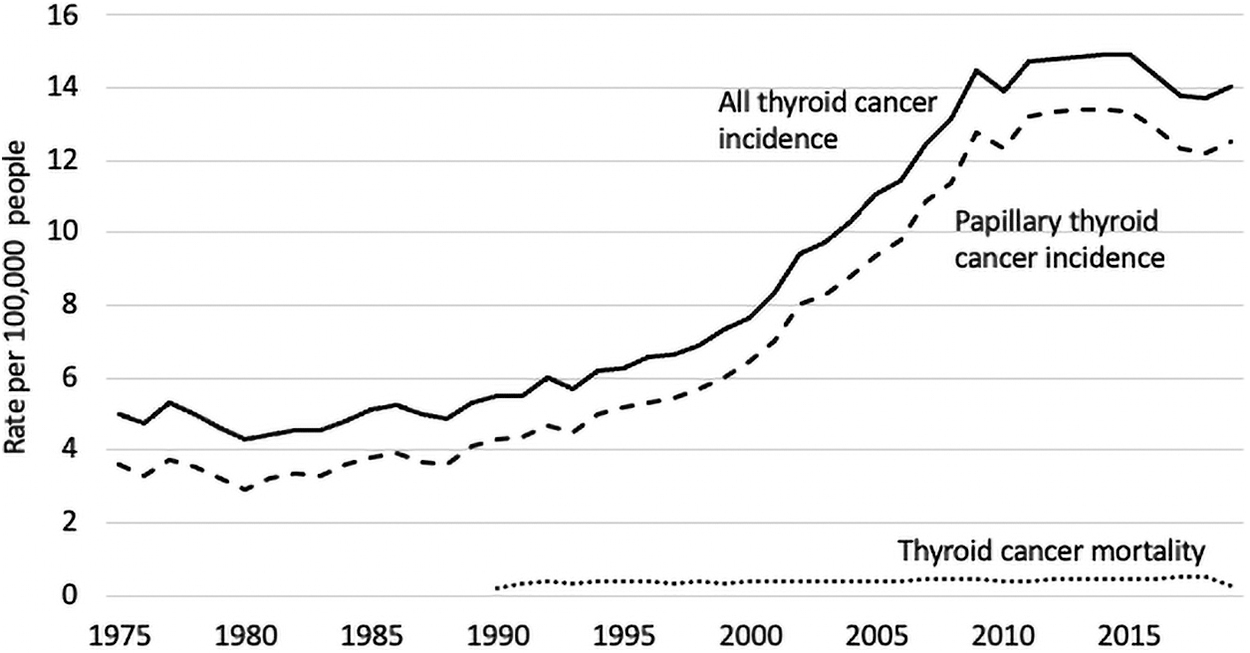
Thyroid Cancer Incidence and Mortality in the United States, 1975–2019. This illustrates a rapid rise in diagnosis of thyroid cancer between 1995 and 2009, while the mortality remained low and essentially unchanged. Most of the increase in carcinoma diagnosed was due to small papillary carcinomas. There appears to be stabilization of the increase for the past decade, following improved guidelines for biopsy of thyroid nodules. Data are from The SEER Program (
In 2014, Ahn et al reported on an “epidemic” of thyroid cancer in South Korea. They indicated that following institution of fee-for-service thyroid cancer screening with ultrasound, the number of patients undergoing surgery for thyroid cancer in South Korea rose from ∼1000 in 2001 to over 11,000 in 2012. 14 In March 2014, a physician coalition for prevention of overdiagnosis of thyroid cancer called for a cessation of ultrasound screening for thyroid cancer, with a 35% drop in thyroid cancer surgery in only 1 year. 15
Analyzing data from the SEER database, Haymart et al reported that increased use of thyroid ultrasound was associated with an increase in thyroid cancer diagnosis, including localized papillary thyroid cancer with size ≤1 cm. They estimated that between 2002 and 2013 at least 6594 patients over the age of 64 years in the United States were diagnosed with thyroid cancer due to increased use of thyroid ultrasound. 16
Improved Guidance for Use of Thyroid Ultrasound
With the recognition that thyroid cancer incidence was rising faster than any other cancer type in the United States, and epidemiological evidence indicating that the majority of cases were small indolent subclinical papillary carcinomas unlikely to result in morbidity or mortality, efforts were made to mitigate the problem of overdiagnosis. 17 Guidelines from the United States Preventative Services Task Force recommended against screening for thyroid cancer by ultrasound or palpation. 18 Nonetheless, it was apparent that more specific ultrasound guidelines were needed to address the escalating diagnosis and surgery of small thyroid cancers.
The 2009 American Thyroid Association Guidelines for the management of Thyroid Nodules and Thyroid Cancer recommended that biopsy be performed on all nodules over 5 mm in patients with a history suggesting a high risk for thyroid cancer. Biopsy was otherwise recommended for all solid hypoechoic nodules measuring larger than 1 cm. 19 AACE, in collaboration with Associazione Medici Endocrinologi, and European Thyroid Association published guidelines in 2010 recommending biopsy of nodules of any size with marked hypoechogenicity, irregular margins, anteroposterior dimension greater than transverse dimension, microcalcifications, or “chaotic arrangement of intramodular vascular images.” 20 In 2011, the Korean Society for Thyroid Radiology recommended biopsy of all nodules exhibiting any feature suspicious for malignancy, acknowledging that nodules smaller than 5 mm are difficult to biopsy. 21
It was apparent that the approach to thyroid nodules and cancer should be aimed at detecting clinically significant lesions rather than identifying all incidental and indolent lesions. Between 2015 and 2017 several sets of guidelines were developed in an attempt to identify those thyroid nodules at higher risk of clinically significant carcinoma based on ultrasound appearance. These guidelines took two distinct approaches: pattern recognition and quantitative scoring systems based on structural criteria.
The nodule section of the 2015 American Thyroid Association Guidelines for the Management of Thyroid Nodules and Thyroid Cancer, led by Haugen and Mandel, proposed a novel pattern recognition approach, dividing nodule patterns into five categories: high, intermediate, low, very low suspicion, and benign, with size criteria for biopsy in each category. Biopsy of nodules <1 cm was not recommended, even with suspicious criteria or high-risk history. 22
In 2009, Horvath et al proposed a Thyroid Imaging Reporting and Data System (TI-RADS), based on the concepts of the breast imaging system of the American College of Radiology. 23 There have been at least seven TI-RADS proposed: Chilian TI-RADS, Kwak TI-RADS, Korean TI-RADS, European-TI-RADS, American College of Radiology (ACR)-TI-RADS, and Chinese TI-RADS. As with the 2015 ATA Guidelines described earlier, each of these systems utilizes features of nodules such as composition, shape, echogenicity, vascularity, margins, and inclusions/calcifications to predict the probability of malignancy, and provide guidance regarding the need for biopsy. 24
In 2017, the American College of Radiology modified prior systems and proposed the ACR TI-RADS. Assigning points for five criteria of composition, echogenicity, shape, margins, and presence of echogenic foci, nodules were categorized as benign, not suspicious, mildly suspicious, moderately suspicious, or highly suspicious, with criteria for the size of the nodule prompting biopsy. Similarly, biopsy was recommended of high suspicion nodules only if the size exceeded 1 cm, with recommendation that sub-centimeter nodules be followed with sequential ultrasound examinations. 25
The Korean TI-RADS used a similar algorithm beginning with the composition of the nodule (solid, partially cystic, purely cystic, or spongiform) with the presence or absence of any suspicious ultrasonographic features, including microcalcifications, nonparallel orientation, speculated, or microlobulated margins. Nodules were divided into high, intermediate, or low suspicion, and benign categories. Again, each category was then assigned a size cutoff for biopsy, with recommendation to biopsy high suspicion nodules only if larger than 1 cm, but “selective biopsy” of smaller nodules, including those with suspicious cervical lymph nodes or suspicion of extrathyroidal extension. 26 In 2021, the Korean Society of Thyroid Radiology guidelines were revised, with changes in the nodule size thresholds for biopsy, and addition of more precise guidance regarding diagnosis of suspicious lymph nodes and extrathyroidal extension. 27
Studies to validate and compare each of the leading guidelines demonstrate good performance of each in reducing biopsies of benign nodules, and either performing biopsy or active surveillance of malignant nodules. 24,28
Several organizations have promoted guidelines to standardize the performance of ultrasound examination and the reporting of thyroid, parathyroid, and comprehensive cervical ultrasound examinations. The American Institute of Ultrasound Medicine has periodically published such guidelines. Of note, in the 2013 revision a recommendation first appeared that all cervical ultrasound examinations should include a brief investigation of the lateral neck for the presence or absence of suspicious or abnormal appearing lymph nodes. 29
With the recognition that high-quality ultrasound imaging is necessary for long-term management of thyroid nodules and thyroid cancer, the Thyroid Head and Neck Cancer Foundation (THANC) developed a consensus statement on ultrasound evaluation of thyroid nodules and lymph nodes, aiming to standardize thyroid and cervical ultrasound reports with regard to content, terminology, and organization. 30 Recommendations were made regarding the performance and recording of thyroid ultrasound examinations, including characterization of the thyroid, clinically significant nodules, and cervical lymph nodes.
Central Role of Ultrasound in Active Surveillance of Thyroid Cancer
With the recognition that the increase in papillary carcinoma was predominantly a result of early diagnosis of small often indolent cancers, active surveillance became a promising management strategy for papillary thyroid microcarcinomas. 31 In active surveillance, delaying surgery in favor of observation with serial ultrasound requires precise ultrasound measurements of nodules, as well as determination of the absence of involved cervical lymph nodes. Initial trials of active surveillance from Japan indicated that nonsurgical management of papillary thyroid microcarcinoma was safe and cost-effective when compared with immediate surgery with postsurgical surveillance. Reports from Ito et al in 2003 were promising 31 and supported by subsequent long-term studies. 32,33 Active surveillance of select sub-centimeter cancers was incorporated into the 2015 ATA guidelines. 22
A successful active surveillance program requires availability of high-quality ultrasound studies. Studies are typically repeated initially at six-month intervals, and precise measurements are needed along with skilled evaluation of the cervical lymph node basins. Appropriate tumor characteristics and location, and the absence of suspicious cervical lymph nodes are essential criteria for active surveillance (Fig. 3). As stated by Ito, “The quality and consistency of ultrasound for longitudinal evaluation of the thyroid and cervical node basins is a significant factor in active surveillance and poses a challenge for the implementation of this type of program outside of high-volume thyroid centers.” 31
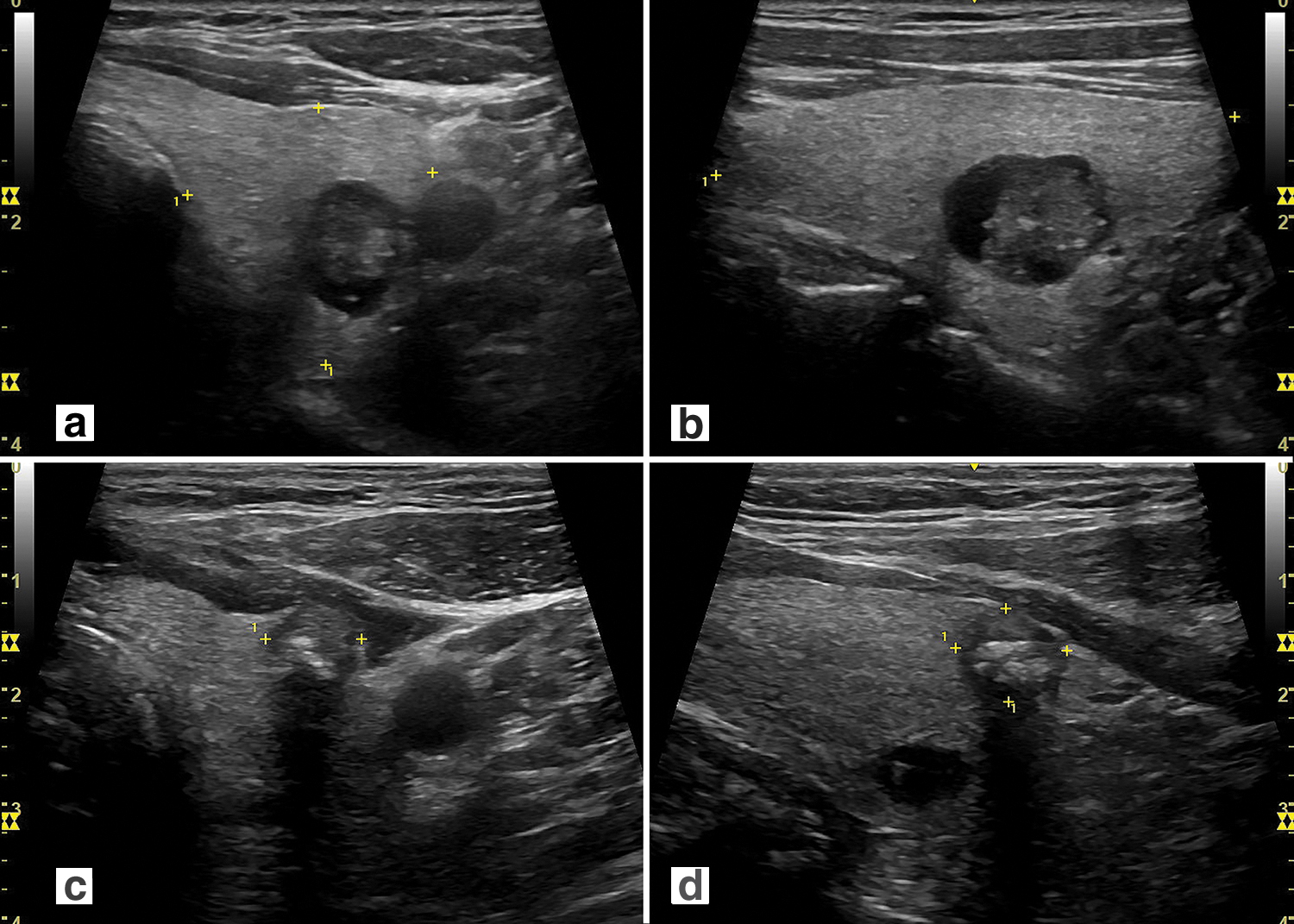
Ideal and inappropriate candidates for active surveillance. The distinction between ideal, appropriate, and inappropriate candidates for active surveillance includes ultrasound characteristics, as well as patient characteristics and characteristics of the medical team. (
The Thyroid Cancer Care Collaborative offered guidance in selection of appropriate candidates, monitoring, and record keeping for patients entering active surveillance. Providing an imaging and cytology module, they helped form a framework for active surveillance. 34 Subsequently, Tuttle et al reported on 291 patients enrolled in an active surveillance program at Memorial Sloan Kettering Cancer Center. 35 Classifying patients as “ideal, appropriate, or inappropriate” for active surveillance 36 (Fig. 3), they increased the maximum acceptable tumor dimension to 1.5 cm. They stressed the importance of availability of ultrasound expertise as a prerequisite for such a program. In a subsequent article reviewing active surveillance, the importance of patient selection and of a multidisciplinary team was emphasized. 37
Recently, an investigation of clinician acceptance of active surveillance found that while most endocrinologists support its use, it is vastly underutilized, with concerns regarding lack of sufficient long-term evidence and medicolegal concerns remaining significant barriers. 38
Thyroid Ultrasound in Pre- and Postoperative Surveillance of Thyroid Cancer
An essential role for thyroid ultrasound has been in both preoperative staging and mapping to determine the extent of surgery, and postoperative monitoring for locoregional soft tissue or lymph node metastases.
In 2003, investigators at the MD Anderson Cancer Center reported performance of a preoperative comprehensive cervical ultrasound examination in patients undergoing surgery for thyroid cancer, in whom clinical evaluation suggested that the neck was free of metastatic disease. Abnormal lymph nodes or soft tissue metastases were detected by ultrasound in 39% of patients, altering the operative procedure in these patients, greatly improving the probability of complete resection at surgery. 39 The following year a retrospective study performed by the same group reported that in patients undergoing reoperation for persistent or recurrent thyroid cancer, reoperation was judged to have been possibly preventable in 39% in whom incomplete initial surgery was performed without an adequate preoperative ultrasound study. 40
Similarly, in 2006 clinicians at the Mayo Clinic reported that preoperative ultrasound detected nonpalpable lymph node metastasis in 32.9% of 702 patients undergoing ultrasound papillary thyroid cancer surgery. 41
The 2009 and 2015 ATA guidelines recommend a comprehensive cervical ultrasound examination be performed in all patients undergoing surgery for suspicion of thyroid cancer. 19,22 Such studies should include details of the tumor, including location within the gland and evidence of the presence or absence of extracapsular or extrathyroidal extension. A comprehensive cervical lymph node survey should be performed in all thyroid cancer cases. The 2015 guidelines additionally recommended cross-sectional imaging studies (CT and MRI) for patients with clinical suspicion for advanced disease, including invasive primary tumor, or clinically apparent lymph node involvement. 22 A preoperative map should be prepared, illustrating size and location of the thyroid lesion(s) and abnormal or suspicious lymph nodes (Fig. 4).
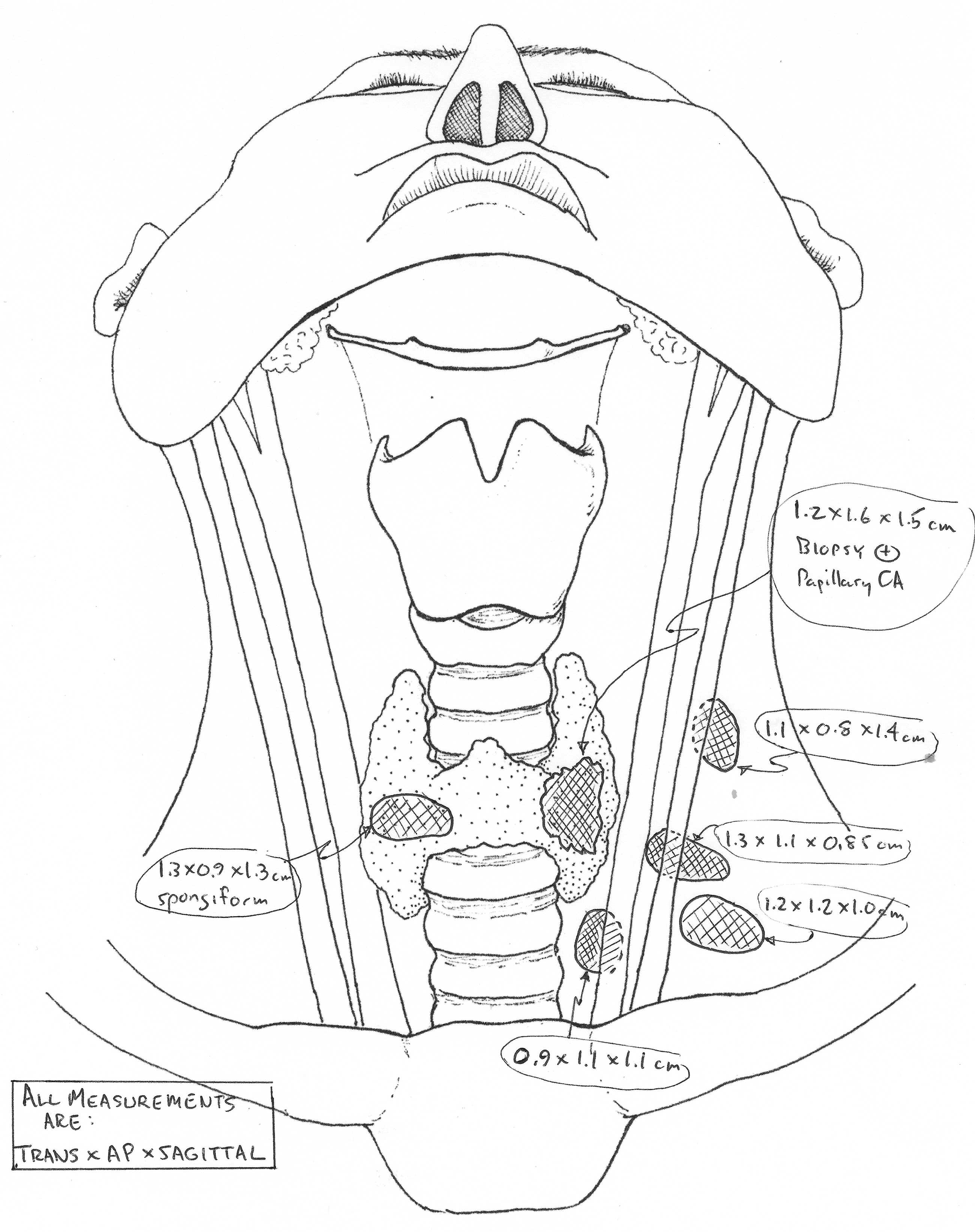
This map has been prepared using ultrasound and CT images obtained in the preoperative evaluation. It demonstrates the primary thyroid lesion, as well as involved cervical lymph nodes. Preparation of such a map allows detailed preoperative surgical planning.
The 2015 ATA guidelines recommended that after surgery for well-differentiated thyroid cancer, cervical ultrasound to evaluate the thyroid bed and central and lateral cervical node compartment should be performed at 6–12 months, and then periodically, depending on the patient's risk for recurrent disease and thyroglobulin status, and indicated that suspicious lymph nodes greater than 8–10 mm in the smallest diameter should undergo biopsy only “if a positive result would change management.” Per these guidelines, “Non-suspicious and small nodes (less than 8–10 mm in the smallest diameter) can be monitored with neck ultrasound.” 22
With the demonstrated value of ultrasound in detection of cervical lymph node metastases, the management of recurrent/persistent nodal disease was addressed in 2015 by the American Thyroid Association surgical affairs committee writing task force. 42 Similar recommendations were presented in a Head and Neck Society consensus statement in 2016. 43 Both of these articles clearly indicated that ultrasound is the initial imaging study of choice for detection of structural recurrence, discussed active surveillance of select nodal disease, and suggested that a multidisciplinary approach is essential to management decisions. As with active surveillance of thyroid nodules and thyroid microcarcinoma, high-quality ultrasound performed by experienced operators is essential to active surveillance of recurrent disease.
Interventional Uses of Thyroid Ultrasound
Thyroid ultrasound has been used to facilitate interventional procedures, including treatment of thyroid nodules and recurrent thyroid cancer, and therapy of papillary thyroid microcarcinoma.
The earliest ultrasound-assisted interventional procedure was alcohol ablation of hyperfunctioning thyroid nodules. However, it became clear that the predominant role for alcohol ablation was in large cystic nodules. Subsequently, thermal ablation, including laser and radio frequency ablation was introduced. Papini et al described long-term efficacy of ultrasound-guided laser ablation for benign thyroid nodules in 2014. 44 The European Thyroid Association published guidelines for thermal ablation of benign thyroid nodules in 2020. 45
The guidelines recommended restricting procedures to benign lesions with either symptomatic or cosmetic concerns. The Asian Conference on Tumor Ablation Task Force published similar guidelines in 2021. 46 Both guidelines emphasized the importance of ultrasound in patient selection, recommended that nodules with high-risk ultrasonographic features not be considered for procedure, and recommended one or two benign biopsies be obtained before intervention. Both guidelines also stated that experience with microwave ablation and high-intensity focused ultrasound was insufficient to recommend their current use. The European guidelines commented on nearly similar clinical efficacy and safety of laser and radiofrequency ultrasound-guided procedures. 45
With the safety and efficacy of thermal ablation for benign thyroid nodules demonstrated, studies have been performed evaluating nonsurgical treatment of papillary thyroid microcarcinoma. Reports have shown long-term efficacy of ultrasound-guided laser ablation for papillary thyroid microcarcinoma 47 and comparable four-year clinical outcome between radio frequency ablation and thyroid lobectomy for low-risk papillary thyroid microcarcinoma. 48
Recently, a consensus statement was issued by the American Head and Neck Society Endocrine Surgery Section with the Asia Pacific Society of Thyroid Surgery, Associazione Medici Endocrinologi, British Association of Endocrine and Thyroid Surgeons, European Thyroid Association, Italian Society of Endocrine Surgery Units, Korean Society of Thyroid Radiology, Latin American Thyroid Society, and Thyroid Nodules Therapies Association. It discussed the indications, techniques, complications, and expectation of successful treatment, and recommended follow-up for percutaneous ablation techniques. It provided a manual for best practice application of ablation techniques. It emphasized that advanced training in ultrasound and an “…established skill set in the performance of ultrasound and ultrasound guided procedures is a prerequisite for the safe application of ultrasound guided ablation technologies.” 49
Certification and Endocrine Certification in Neck Ultrasound
In 2006, several commercial insurance plans indicated that they would not reimburse providers for the performance of thyroid ultrasound unless they were certified either by American Institute of Ultrasound in Medicine (AIUM) or the ACR. A subsequent joint venture between AACE and AIUM resulted in development of the Endocrine Certification in Neck Ultrasound (ECNU) program in 2007. Certification was provided through AACE, with agreement by AIUM. Certification required completion of a written examination, documentation of appropriate case volume, and a case-based validation of competency with submission of relevant cases to be reviewed and critiqued by ECNU-certified physicians.
The ECNU handbook included guidelines for reporting thyroid ultrasound results utilizing standards from ACR and AIUM. These included indications for the procedure, descriptions of the overall thyroid, and nodules, all measurements reported in three dimensions, the presence or absence of involved suspicious cervical lymph nodes, and recommendation of action based on the study.
Physicians were certified under the ECNU program for the next 13 years. However, in December 2019, AACE restructured their thyroid education program and announced that they would no longer offer certification or recertification to individual physicians. 50 All physicians previously certified received permanent certification with the prior 10-year recertification requirement rescinded. Currently, practices, departments, or institutions can be can be recognized by either AIUM or the ACR if clinician-performed ultrasounds fall under the auspices of the radiology department.
The issues of continuing education in thyroid ultrasound, certification, and validation of competency remain significant challenges for the future of clinician-performed point-of-care thyroid ultrasound.
Conclusion
From its first availability in the 1960s with low-resolution images, to current high-resolution imaging, ultrasound has a crucial role in the evaluation and treatment of thyroid disorders. It is invaluable to endocrinologists as an extension of the physical examination, providing real-time information regarding goiter and thyroid nodules. It is a proven adjunct to fine-needle aspiration biopsy. Comprehensive central and lateral cervical ultrasound evaluation is essential before thyroid cancer surgery, and in the subsequent follow-up of thyroid cancer patients.
Active surveillance of papillary microcarcinoma or evaluation for thyroid cancer requires precise measurements of lesions and skill at cervical lymph node evaluation. Thyroid ultrasound is instrumental to interventional studies, including chemical and thermal ablation of benign and malignant thyroid tumors as well as recurrent thyroid cancer. While overuse of thyroid ultrasound may have played a role in the overdiagnosis of small indolent clinically insignificant thyroid cancers, recent data suggest that improved guidelines may have resulted in a stabilization of the prior rise in incidence (Fig. 2).
Moving into the future, radiomics (quantification and extraction of minable data from images) and artificial intelligence/machine learning will clearly play a large role in minimizing user dependence as a limiting feature of ultrasound imaging. As we transition from an old paradigm of seeking and destroying all thyroid cancer, to a new paradigm of finding and selectively treating significant thyroid cancer, ultrasound will continue to play a critical role.
Footnotes
Dedication
Dedicated to the memory of Daniel Duick, MD, FACP, MACE, ECNU (1941-2022). A great clinician, teacher, and mentor.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.