
Abstract
Introduction:
Thyroid incidentalomas are frequently identified thyroid nodules viewed on nonthyroid dedicated imaging studies. Clinical guidelines recommend evaluation of all thyroid incidentalomas to risk stratify for cancer. This study examined how thyroid incidentalomas are reported on chest computed tomography (CT) and determined the association of reporting location with likelihood of evaluation and risk of long-term outcomes.
Methods:
Retrospective cohort of 1460 previously identified Veterans with thyroid incidentalomas on chest CT from a single VA institution between 1995 and 2016. Reporting of the incidentaloma was categorized as either in the body of the report alone or in the impression. Demographic data, vital status, thyroid ultrasound, endocrinology consult, thyroid nodule fine needle aspiration, thyroid surgery, thyroid cancer diagnosis, and death from thyroid cancer were abstracted.
Results:
Among the 1460 Veterans (mean age 70.4 years and 94.9% male) in the cohort, 707 incidentalomas (48.4%) were reported in the impression and 753 (51.6%) were reported in the body section. Veterans with thyroid incidentalomas reported in the impression versus body were significantly more likely to be evaluated within 6 months (35.5% vs. 5.1%; p ≤ 0.001), 12 months (38.5% vs. 6.5%; p ≤ 0.001), and at any time during the follow-up period (47.8% vs. 13.2%; p ≤ 0.001). Veterans with thyroid incidentalomas reported in the impression versus body were more likely to undergo thyroidectomy (18 [2.6%] vs. 6 [0.8%]; p = 0.009), but there was no difference in the proportion of Veterans diagnosed with thyroid cancer (11 [1.6%] vs. 6 [0.8%]; p = 0.18), thyroid-cancer related mortality (4 [0.6%] vs. 1 [0.1%]; p = 0.16), or all-cause mortality (63.2% vs. 66.5%; p = 0.19).
Conclusions:
Thyroid incidentalomas on chest CT are inconsistently reported and often receive no subsequent evaluation. The location of reporting affects whether clinical evaluation is performed, yet reporting does not affect the proportion of Veterans who died of any cause and may have little effect on the proportion of Veterans who received a diagnosis of thyroid cancer or died from thyroid cancer. These findings suggest that the guideline recommendation to evaluate all thyroid incidentalomas should be reevaluated.
Introduction
Incidentalomas are unanticipated findings of a nodule or mass on imaging studies. They can cause substantial patient anxiety, although most do not represent serious or life-threatening conditions. 1 Thyroid incidentalomas are thyroid nodules seen on nonthyroid dedicated imaging studies, including chest computed tomography (CT), cervical spine magnetic resonance imaging (MRI), carotid ultrasound (US), and chest X-ray. Thyroid incidentalomas are present on neck CT in 16% of patients 2 but are inconsistently reported, 3,4 with prior studies reporting variable prevalence of incidental thyroid nodules from <1% 5,6 to 5–6%. 7 Thyroid incidentalomas are more common with advancing age, reflecting the natural history of thyroid nodules. 7 Advances in imaging technology, especially the widespread and growing use of chest CT for lung cancer screening, 8 have increased reporting of thyroid incidentalomas over the past two decades. 7
Most thyroid nodules, and therefore thyroid incidentalomas, are benign. Even so, thyroid nodules, including thyroid incidentalomas, may be considered for further evaluation because a small percentage will be malignant. Previous fine needle aspiration (FNA) studies of incidental thyroid nodules found 12.5% malignant, 2 similar to the 7–15% reported prevalence of malignancy among all thyroid nodules. 9 The 2015 American Thyroid Association (ATA) guidelines for thyroid nodules and thyroid cancer recommend evaluation of all suspected thyroid nodules, whether identified incidentally or not, using thyroid US to risk stratify the nodule and make decisions on whether to perform FNA. 9 This was rated a strong recommendation by the ATA task force based on high-quality evidence. 9 Conversely, the American College of Radiology recommends evaluation of only a subset of incidental thyroid nodules identified on CT or MRI based on patient age and nodule size, suggesting US for nodules ≥1 cm if age <35 years and for nodules ≥1.5 cm if age ≥35 years. 10
Despite these recommendations, prior studies have reported high variability in how radiologists report incidental thyroid nodules on CT, 3 and neither guideline recommends how incidental thyroid nodules should be reported. A radiology report consists of two sections, the body and the impression. The body of the report consists of all findings, normal and abnormal, while the impression summarizes the key or important findings of the imaging study. Often, providers only read the impression of a radiology report and not the entire body, leading to the possibility of missed findings if they are only reported in the body section. This introduces the possibility of missed nodules and lack of subsequent evaluation.
An enhanced understanding of the reporting, evaluation, and outcomes of thyroid incidentalomas is needed to provide better evidence-based guidance regarding the clinical evaluation of thyroid incidentalomas. The present study utilized an existing database of previously identified individuals with reported thyroid incidentalomas on chest CT scans to determine whether the location (the body or impression section of the radiology report) of the incidentaloma was associated with the likelihood of subsequent evaluation and whether differences in reporting location was associated with eventual thyroid surgery, thyroid cancer, or death from thyroid cancer.
Methods
This is a retrospective cohort study using electronic medical record data from 1650 previously identified Veterans with incidental thyroid nodule on chest CT (755 chest CT with contrast, 895 chest CT without contrast). A detailed description of the methodology used to identify these Veterans has previously been published. 7 In summary, a natural language processing (NLP) technique was developed by identifying the word “thyroid” within radiology reports, excluding those which reported “normal” or “unremarkable” thyroids, and performing a manual review to verify positive reports. This method was validated and found to have a 99.6% negative predictive value. 7
We previously used this method to identify reported incidental thyroid nodules in either the body or the impression section of radiology reports (chest CT, neck MRI, and carotid US) within our institution between 1995 and 2016. A total of 98,054 radiology reports were potentially eligible for inclusion in this study. After duplicate scans were removed, a total of 30,339 chest CT scans were reviewed; of these, 1650 scans in unique patients reported a thyroid incidentaloma. 7 Of the 1650 Veterans reviewed, 190 Veterans were excluded for having thyroid incidentaloma evaluation before their index date (Fig. 1).
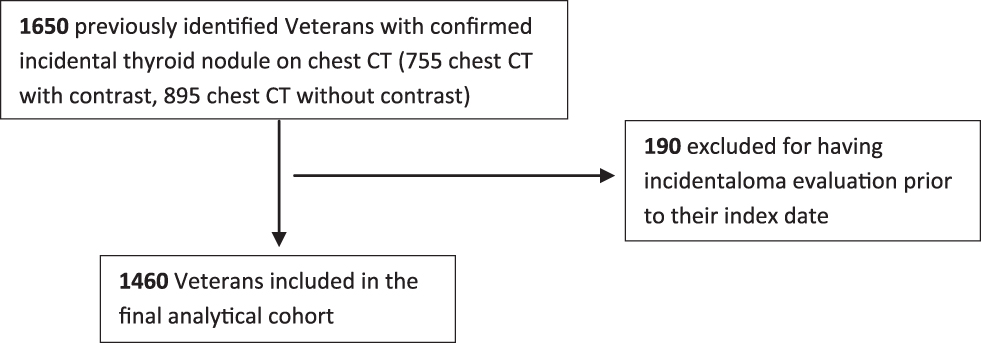
Participant flow diagram.
The index date was defined as the date of the Chest CT scan that reported the thyroid incidentaloma. Reporting of the incidentaloma on the radiology report was categorized as appearing either in the body of the report alone or in the impression section of the report. Demographic data included sex and age at index date. Vital status, including date of death if deceased, thyroid US, endocrinology consult for thyroid nodule, thyroid nodule FNA, thyroid surgery, thyroid cancer diagnosis, and death from thyroid cancer, was abstracted from the electronic health record. Thyroid incidentaloma evaluation was defined as a composite of any of the following: dedicated thyroid US, endocrinology consult for thyroid nodules, or thyroid nodule FNA.
Thyroid cancer diagnosis was based on surgical pathology reports and ICD codes. To determine death from thyroid cancer, records of all deceased Veterans with documented thyroid cancer were reviewed independently by two study team members to adjudicate whether thyroid cancer was the cause of death. Reviewers were blinded to the reporting location of the incidentaloma. Veterans who underwent thyroid nodule evaluation with thyroid US, endocrinology consult for thyroid nodule, or thyroid nodule FNA before their index date were excluded from the analyses. Post hoc analysis of Veterans stratified by mean age (≤70 years compared to >70 years) was performed to assess whether the association of reporting location with likelihood of evaluation and risk of long-term outcomes varied by age group. This project was conducted as a quality improvement initiative. It was reviewed by the Minneapolis VA Institutional Review Board and determined that the board's approval was not required.
Statistical analysis
Table 1 includes demographics and descriptive evaluation data. For continuous variables, mean (SD) and/or median (IQR) are reported. For categorical data, percentages and raw numbers are reported. Continuous measures were compared by reporting method and did not meet parametric assumptions; therefore, the Wald test for medians (quantile regression) was utilized to compare medians. Categorical variables were compared by reporting method utilizing chi-square tests. The Mann–Whitney U test was utilized to compare the non-normally distributed time to evaluation variables.
Characteristics and Evaluation of Veterans with Thyroid Incidentalomas in Overall Cohort and by Radiology Reporting Method
FNA, fine needle aspiration; US, ultrasound.
Results
A total of 1460 Veterans were included in the final analytical cohort. The mean (SD) age of Veterans was 70.4 (10.9) years, and 1386 (94.9%) were male (Table 1). Of the 1460 Veterans, 707 incidentalomas (48.4%) were reported in the impression section of the radiology report, and 753 (51.6%) were reported in the body of the report only. There was no significant difference in age (p = 0.32) or sex (p = 0.32) of Veterans by radiology reporting method.
Overall, 29.9% (437 of 1460) Veterans received any evaluation of their thyroid incidentaloma. The mean time to any thyroid nodule evaluation (thyroid US, endocrinology consult, or thyroid nodule FNA) was 14.5 (SD 28.5) months, and the median time was 1.7 (IQR 0.5, 13.8) months. The time to evaluation for thyroid incidentalomas reported in the impression section of the radiology report was significantly shorter than that for incidentalomas reported in the body of the report alone (mean time = 12.2 months vs. 22.3 months; p = 0.002; median time = 1.3 months vs. 12.7 months; p ≤ 0.001).
In addition, compared with those reported in the body of the report alone, significantly more of the incidentalomas reported in the impression section were evaluated within the subsequent 6 months (35.5% vs. 5.1%; p ≤ 0.001), 12 months (38.5% vs. 6.5%; p ≤ 0.001), and at any time during the entire follow-up period (47.8% vs. 13.2%; p ≤ 0.001) (Table 1). Among Veterans ≤70 years compared to >70 years of age there was no difference in the proportion of incidentalomas reported in the impression section (49.9% vs. 50.1%; p = 0.19). Veterans ≤70 years compared to >70 years appeared more likely to receive evaluation. However, among both age groups, there was a similar effect of reporting location on the likelihood of subsequent evaluation (Supplementary Tables S1 and S2).
Veterans with thyroid incidentalomas reported in the impression versus body location of the radiology report were more likely to undergo thyroidectomy (18 [2.6%] vs. 6 [0.8%]; p = 0.009). Among the 1460 Veterans, 17 (1.2%) received a diagnosis of thyroid cancer. While the proportion of Veterans receiving a thyroid cancer diagnosis was ∼2-fold higher among Veterans with incidentalomas reported in the impression versus body location of the radiology report, this difference was not significant (11 [1.6%] vs. 6 [0.8%]; p = 0.18). In addition, there were no significant differences between Veterans with thyroid incidentalomas reported in the impression versus those with incidentalomas reported in the body of the report alone in the proportion of Veterans with thyroid-cancer related mortality (4 [0.6%] vs. 1 [0.1%]; p = 0.16) or all-cause mortality (63.2% vs. 66.5%; p = 0.19) (Table 2). Of the 17 Veterans diagnosed with thyroid cancer, the mean time to any evaluation was 9.1 (SD 13.6) months.
Long-Term Outcomes Based on Radiology Reporting Method
Of the five Veterans who died of thyroid cancer the mean time to any evaluation was 0.5 (SD 0.6) months. Of these five Veterans, four had high risk pathology, including two Veterans with medullary carcinoma, one with tall cell variant papillary carcinoma, and one with widely invasive follicular carcinoma. The remaining Veteran had Stage III T4aN1bM0 papillary carcinoma.
Discussion
We found that fewer than half of thyroid incidentalomas are reported in the impression section of chest CT reports and that reporting location is significantly associated with the likelihood of subsequent evaluation. Incidentalomas reported in the impression section versus those reported in the body of the report alone are more likely to be further evaluated with thyroid US, endocrinology consult, and thyroid nodule FNA and are evaluated significantly sooner. However, we found no significant differences between thyroid incidentalomas reported in the impression section compared to incidentalomas reported only in the body of the report with respect to proportion receiving a thyroid cancer diagnosis, experiencing thyroid-cancer related death, or all-cause mortality.
Prior studies have reported that 16% of chest CT scans have a visible thyroid incidentaloma 2 with 5–6% of all chest CT scans reporting this incidental finding. 7 The common visualization of thyroid nodules on chest CT scans, coupled with the increasing use of chest CT due to lung nodule tracking, lung cancer screening, and receiving care and evaluations in the emergency department, 7,11 will likely increase prevalence of thyroid incidentalomas. Thyroid incidentalomas have also been reported on chest X-ray, carotid US, and cervical spine MRI, 5,7 and incidentalomas are not unique to the thyroid gland. For example, Incidental pulmonary nodules have also been reported to be an increasingly common consequence of routine medical care 12 and variably reported in the impression section. 13
Our results are consistent with prior studies noting high variability in how radiologists report thyroid incidentalomas. 3 We observed a significant association between reporting the thyroid incidentaloma in the impression section of the radiology report and a greater likelihood of receiving a subsequent evaluation. We found that thyroid incidentalomas reported in the impression section were more likely to be further evaluated with nearly half being evaluated compared to only 13% when reported in the body of the report alone. Our study does not address the cause of this difference, but errors of omission seem likely. Providers are less likely to be aware of incidentalomas only reported in the body of the report, and this approach has been suggested as a way to influence the ordering providers evaluation decision. 4 This strategy, if true, is a clear violation of patient autonomy, the right of patients to make decisions about their medical care, and missed results also lead to potential medical-legal liability.
As is the case with many abnormal results or laboratory or imaging studies, it may be prudent to first inform patients of any findings of incidentalomas and then engage in shared clinical decision-making regarding the benefits, potential harms, and possible outcomes of further evaluation. Widespread evaluation of thyroid incidentalomas in older adults has been reported to not be cost-effective 14 and may initiate a cascade of clinical care, including thyroid US, thyroid nodule FNA, thyroidectomy, and potential lifelong thyroid hormone replacement and monitoring. The decision to evaluate, or not evaluate, a thyroid incidentaloma should be made with the patient with consideration of life expectancy, his/her preferences, and health care priorities, as opposed to a universal reflex to evaluate all incidental nodules. Interestedly, 7.9% of our Veterans with a reported incidentaloma received evaluation over 12 months after it was initially reported. While this evaluation may have been triggered by a new event, such as another imaging study or abnormal physical examination, data are not available in our study to test this hypothesis.
Despite the effect of thyroid incidentaloma reporting location on likelihood of subsequent evaluation, we did not observe significant differences between Veterans with thyroid incidentalomas reported in the impression section compared with those with incidentalomas reported only in the body of the report in clinically relevant outcomes, including diagnosis of thyroid cancer, death from thyroid cancer, or all-cause mortality. Thyroid cancer was very rare in our cohort with only 17 (1.2%) Veterans being diagnosed with thyroid cancer. Autopsy studies have shown that 11% of patients have incidental papillary thyroid cancer upon death, 15 and it is possible that there were many Veterans in our cohort with undiagnosed, clinically silent thyroid cancer.
The lack of differences in clinically relevant outcomes argues against the need to evaluate all thyroid incidentalomas as currently recommended by the ATA. 9 Furthermore, the evaluation of all thyroid incidentalomas in real-world practice will lead to increased clinical and economic burden, yet our results suggest that this practice may not result in improved clinical outcomes. Our findings lend credence to the U.S. Preventative Services Task Force recommendation against screening for thyroid cancer due to the increased harms yet lack of benefit from the overdiagnosis of thyroid cancer. 16
The major limitation of our study is its retrospective cohort design. Thus, we are unable to analyze why providers evaluate certain thyroid incidentalomas but not others nor were we able to examine patient, provider, or facility level factors that influenced time to evaluation. There is likely selection bias present in the Veterans who received further evaluation. For example, a provider may be more likely to further evaluate a thyroid incidentaloma in a younger or healthier patient compared to an older patient with multiple medical comorbidities due to the competing risk of nonthyroid cancer related mortality. Another potential explanation for whether or not an evaluation is performed is an error of omission, where providers simply do not see and are therefore unaware of the thyroid incidentaloma. This likely explains the difference seen in evaluation based on reporting location.
Our study has several strengths, including the NLP method to identify thyroid incidentalomas on chest CT, large sample size, and nearly complete follow-up for data on subsequent evaluation and long-term clinical outcomes. However, there are limitations. Our study population was predominately older males, and the findings need confirmation in a broader patient population. Despite this limitation, the majority of thyroid studies have a female predominance, and our study provides increased knowledge in a predominately male cohort. Nodule size and other characteristics were not consistently reported on chest CT, and we were unable to analyze the effects of nodule size or other features on subsequent reporting and evaluation. Finally, outcomes, including thyroid surgery, thyroid cancer diagnosis, and thyroid cancer death, were rare events, and therefore, our study was underpowered for these outcomes.
In conclusion, thyroid incidentalomas on chest CT are inconsistently reported and often receive no further evaluation. The location of the reporting in the radiology report impacts whether or not clinical evaluation with thyroid US, endocrinology consult, and FNA is subsequently performed. However, there was no significant difference between Veterans with thyroid incidentalomas reported in the impression versus body section of the report in the proportion who subsequently received diagnosis of thyroid cancer, died from thyroid cancer, or died of any cause. Further research is warranted to determine how to best standardize the reporting of thyroid incidentalomas and to evaluate the effect of evaluating versus not evaluating thyroid incidentalomas on risk of adverse clinical outcomes to better inform future clinical practice guidelines.
Footnotes
Authors' Contributions
T.D.: Study conception (lead), writing—original draft (lead), data collection (supportive). A.G.: Data collection (lead), data analysis (lead), writing—review and editing (equal). K.E.: Study conception (supportive), methodology (lead), writing—review and editing (equal). C.J.B.: Study conception (supportive), writing—review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2