
Abstract
Background:
A history of thyroid and nonthyroid malignancies has traditionally been an exclusion criterion in patients with anaplastic thyroid cancer (ATC) seeking to enroll in clinical trials. In this study, we examined the impact of prior malignancies on overall survival (OS) in patients diagnosed with ATC.
Methods:
In our retrospective cohort study, we identified 451 patients with ATC treated at MD Anderson between 2000 and 2019. Clinical and pathological information was obtained through chart review. Survival analyses were conducted using the Kaplan–Meier method and multivariable Cox proportional hazard models.
Results:
A history of clinically documented differentiated thyroid cancer (DTC) was reported in 14% of patients with ATC (n = 62), most commonly papillary thyroid cancer (81%, n = 50). The median time from diagnosis of prior DTC to ATC diagnosis was 3.5 years (range: 6 months to 35 years). Concomitant DTC was found on pathology in a higher proportion of patients (52%, n = 234). A history of nonthyroid cancer was reported in 23% of patients (n = 102), where 19% (n = 87) had one, 2% (n = 10) had two, and 1% (n = 5) had three prior cancers. The median time from diagnosis of prior nonthyroid cancer to ATC diagnosis was 8 years (range: 3 months to 53 years). The most common prior nonthyroid cancers were nonmelanoma skin (28.4%), prostate (19.6%), and breast cancers (16.7%). In a subgroup analysis performed in patients with available tumor mutation information (n = 183), the frequency of detected tumor driver mutations (BRAF, RAS, TP53) was not significantly different between patients with ATC with and without a history of nonthyroid cancer. On multivariate analysis after adjusting for age and overall stage, prior DTC, concomitant DTC, and prior nonthyroid cancers, all had no significant impact on OS.
Conclusions:
The presence of prior malignancy does not significantly impact OS in patients with ATC. Revision of eligibility criteria for enrollment of patients with ATC into clinical trials is warranted.
Introduction
Anaplastic thyroid cancer (ATC) is a rare and aggressive thyroid malignancy that has been associated with a history of differentiated thyroid cancer (DTC). 1 Although ATC accounts for only 1–2% of all thyroid cancers, it contributes to more than 40% of thyroid cancer-related deaths. 2 ATC had a historical median survival of 3 to 5 months and a 1-year survival rate of less than 10–20%. 3,4 In recent years, the survival outcomes of patients with ATC have significantly improved. 5 In our recent retrospective review of 479 patients, we found that the median overall survival (OS) was 16 months for all patients with ATC and 24 months for patients with BRAFV600E -mutant ATC. 5,6 Utilization of intensive multimodality treatment and prioritization of clinical trial enrollment have been key factors in improving outcomes.
While clinical trial enrollment has improved over time, only a fraction of patients (21%) were eligible and enrolled in trials, suggesting that there are important barriers that need to be addressed. 5 A cancer history is a common exclusion criterion for clinical trials in oncology, which was recently addressed in December 2021 in the revised guidance on eligibility criteria for cancer clinical trials issued by the National Cancer Institute. 7 In fact, the landmark clinical trial of dabrafenib and trametinib in patients with BRAFV600E-mutated ATC excluded individuals with a history of malignancy within three years of ATC diagnosis. 8
With the population of cancer survivors increasing steadily in the United States over the past few decades, improved survival has also led to an increased risk of developing additional malignancies. 9 –11 Literature suggests that men and women in cancer remission are 11% and 17%, respectively, more likely to develop a second primary cancer compared with the general population. 12 Zivaljevic et al reported a history of nonthyroid cancer to be independently and significantly associated with ATC development. 13 However, to our knowledge, the prevalence and prognostic value of prior nonthyroid cancers in the setting of ATC have not been systematically reported in the literature.
Moreover, there is growing evidence suggesting that ATC arises from differentiated thyroid cancer (DTC) through the accumulation of additional mutations. 14,15 Indeed, a significant portion of ATC tumors have been shown to harbor a concomitant DTC component on histopathology. 16 However, previous studies have shown inconsistent results regarding prognosis among individuals with a history of DTC or concomitant DTC. 16,17 These controversies suggest that a more comprehensive study with a large patient cohort is needed to elucidate the true prognostic implications of thyroid cancer history in patients diagnosed with ATC.
The main objective of this study was to evaluate the prevalence of prior malignancies, including both thyroid and nonthyroid cancers, in patients with ATC and to investigate whether a history of cancer impacts OS in patients with ATC.
Methods
Approval for the study was obtained from the MD Anderson Institutional Review Board (IRB) (IRB ID: IRB00005015). A waiver of informed consent was granted by the IRB as the study was determined to have minimal risk using existing information derived from patient care. We conducted a retrospective cohort study and evaluated patients seen at the MD Anderson Cancer Center for pathologically proven ATC between February 1, 2000, and March 20, 2019. All patients were 18 years of age or older at the time of diagnosis. ATC diagnosis was made by fine needle aspiration, core biopsy, or on surgical pathology and verified by a specialized head and neck pathologist.
Patients referred from outside institutions had their pathology rereviewed and confirmed at MD Anderson. The date of ATC diagnosis was noted as the date of specimen collection of pathologically confirmed ATC. Patients were excluded from analysis if no pathology report confirmed ATC. Patients who presented to MD Anderson and sought care elsewhere were excluded if no follow-up data were available.
The overall stage of ATC and prior DTC was determined based on the American Joint Committee on Cancer (AJCC) 7th edition staging criteria. Cancer history was obtained from electronic medical records through a retrospective chart review. Prior thyroid cancer included papillary thyroid cancer (PTC), follicular thyroid cancer (FTC), poorly differentiated thyroid cancer (PDTC), and oncocytic carcinoma diagnosed greater than six months before the diagnosis of ATC. For patients with two primary thyroid cancer types, the predominant subtype on pathology was used for further analyses. All cancers with an oncocytic component were classified as oncocytic carcinoma. Concomitant thyroid cancer on histopathology is defined as the presence of DTC in the setting of ATC as identified by a pathologist.
A history of cancer was defined as a clinically reported history of nonthyroid cancer greater than one month before the diagnosis of ATC. Nonmelanoma skin cancers included basal cell and squamous cell carcinoma; lung cancers included small-cell and nonsmall-cell variants; head and neck cancers include salivary gland carcinoma as well as squamous cell carcinoma of the oral cavity, submandibular nodes, and larynx.
The time from prior cancer to ATC diagnosis is defined as the number of years between the prior cancer diagnosis and ATC diagnosis. The primary outcome of interest was OS. OS was defined as the time interval from the date of ATC diagnosis to the date of death from any cause. The last date of follow-up was defined as the date of death for deceased patients, or the date of last follow-up at MD Anderson for living patients. The duration of follow-up was calculated from the date of diagnosis until the date of last known follow-up. Patients known to be alive were censored at the time of last contact. Patients with nonmelanoma skin cancers were excluded from the survival analysis.
We performed retrospective chart review to ascertain the treatment modalities used. Multimodal treatment of ATC was defined as having received treatment from two or more of the following categories, surgery, radiotherapy, or systemic treatment, which include BRAF-directed therapy, immunotherapy, and cytotoxic chemotherapy.
Tumor materials used for mutation testing were obtained from fine needle biopsy, core biopsy, excisional biopsy, or surgical resection. DNA was extracted from unstained sections of tissue or cytology slides as previously described. 18,19 Tumor mutational profiles were determined by next-generation sequencing in a Clinical Laboratory Improvement Amendments-certified institutional laboratory using targeted panels as previously described. 6 Tumor mutation burden (TMB) was calculated as the number of nonsynonymous mutations per mega base covered. High TMB was defined as TMB that was higher than group median value, while low TMB was TMB that was lower than group median value.
Statistical analysis was performed using SAS. Survival estimates were calculated using the Kaplan–Meier method. The log-rank test was used to compare survival curves across groups. Descriptive statistics were used to summarize demographic and clinicopathologic characteristics of included patients. Cox proportional hazards models were used to assess the association between cancer history and OS. Multivariable models adjusting for known clinical predictors of OS, age, and overall TNM stage were utilized. 20,21 A two-tale p-value of <0.05 was designated as statistically significant.
Results
Patient demographics
A flowchart of included patients is shown in Figure 1. Baseline characteristics of the study population are summarized in Table 1. The median age of ATC diagnosis was 66 ± 11.4 years. Fifty-six percent of individuals (n = 250) were stage IVC at the time of diagnosis. Median OS for the entire cohort was 8.4 months with a 1-year survival rate of 39% and a 2-year survival rate of 22%.
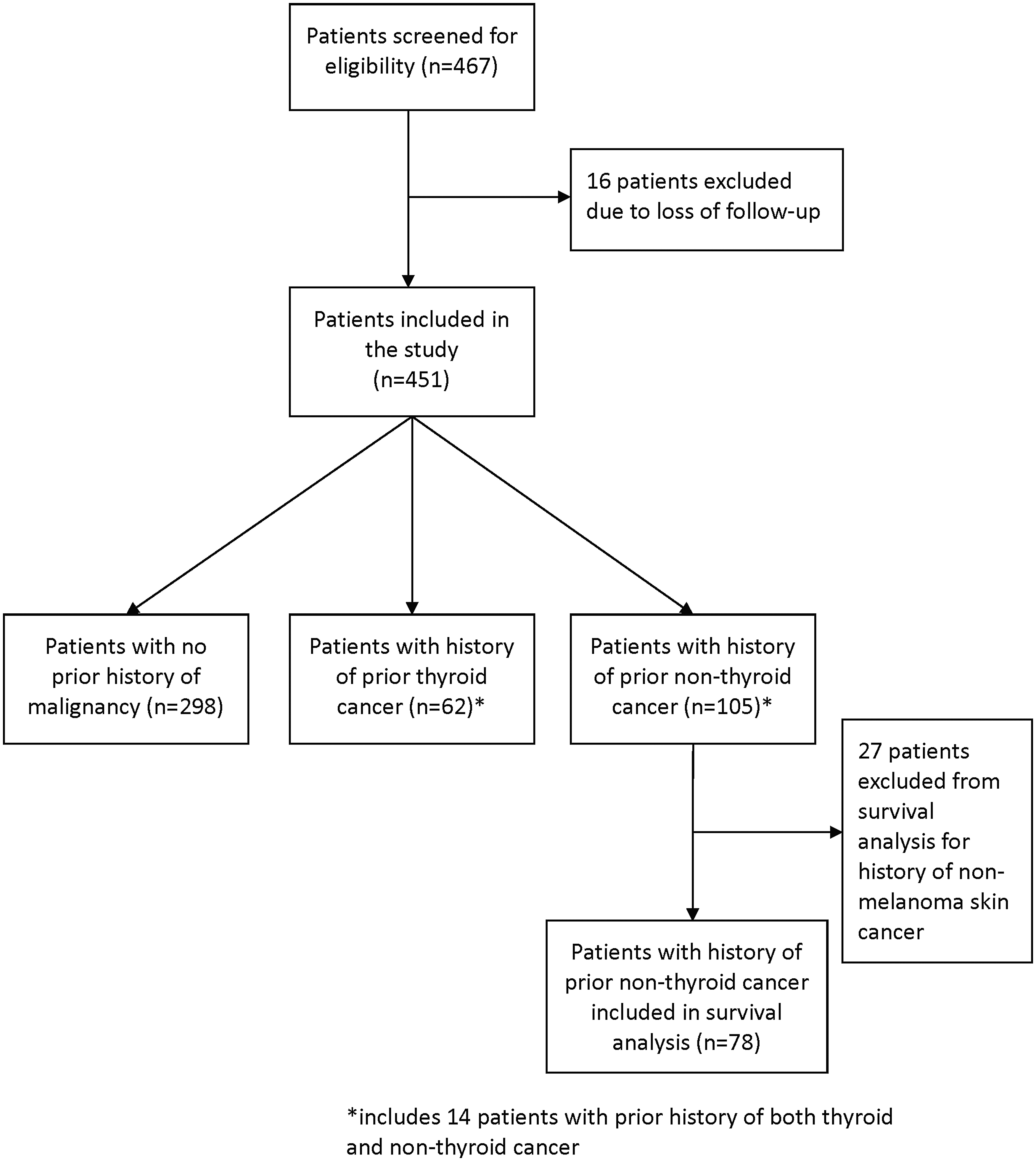
Diagram of included patients.
Baseline Characteristics of Individuals with Anaplastic Thyroid Cancer (N = 451)
FTC, follicular thyroid cancer; IQR, interquartile range; PDTC, poorly differentiated thyroid cancer; PTC, papillary thyroid cancer; SD, standard deviation.
History of DTC
A history of DTC was reported in 14% (n = 62) of the patients in our cohort (Table 1). The median time from the diagnosis of prior DTC to ATC diagnosis was 3.5 years, with a range of 6 months to 35 years. PTC (81%, n = 50) was the most commonly reported type of prior DTC, followed by FTC (10%, n = 6), PDTC (6%, n = 4), and oncocytic carcinoma (3%, n = 2) (Table 1).
Clinicopathological characteristics of the 62 cases of prior DTC are summarized in Table 2. Among individuals with available staging information of their prior DTC (n = 34), most presented with stage T3 or T4 (74%, n = 25), N1 (82%, n = 28), and M0 (97%, n = 33) disease. The majority of patients (n = 22 of 34, 65%) had extrathyroidal extension (T3b, T4a, T4b). In addition, treatment modalities received for prior DTC included surgery (n = 61 of 62, 98%), radioactive iodine (n = 46 of 62, 74%), external beam radiation (n = 18 of 62, 29%), chemotherapy (n = 5 of 62, 8%), and targeted therapy (n = 4 of 62, 6%). The time from prior DTC to ATC diagnosis among patients who received different treatment modalities for prior DTC is summarized in Supplementary Table S1.
Clinicopathological Data on Patients with Anaplastic Thyroid Cancer with a History of Differentiated Thyroid Cancer (N = 62)
There was no significance difference in the average time to ATC transformation by DTC treatment modality. Among the 52 patients with available data on DTC recurrence status, 41 patients (79%) had reported recurrence of DTC before ATC diagnosis. Only nine patients had known mutation information for their prior DTC. Eight patients had a BRAFV600E mutation, and one patient harbored TP53 and NRAS mutations. The majority of patients with prior DTC (81%, n = 50) presented with distant metastasis at the time of ATC diagnosis. These findings suggest that the majority of transformations occurred at the distant site.
On pathology reports, concomitant DTC was found in 52% (n = 232) of patients at the time of pathologic ATC diagnosis (Table 3). Among these patients, concomitant PTC was the most common concomitant DTC, identified in 65% (n = 153) of patients. This was followed by FTC (26%, n = 60), PDTC (7%, n = 17), and oncocytic carcinoma (2%, n = 4) (Table 3). The prevalence of prior DTC type among patients with concomitant DTC is summarized in Table 3. A history of both DTC and nonthyroid cancer was reported in 3% (n = 14) of patients with ATC. The most common DTC in this cohort was PTC (n = 13), followed by FTC (n = 2) and PDTC (n = 1). One patient had PTC with a PDTC component, and another had PTC with an FTC component.
Prevalence of Clinically Documented Prior Thyroid Cancer Among Patients with Concomitant Differentiated Thyroid Cancer Identified on Histopathology (N = 232, 52%)
History of nonthyroid cancer
Twenty-three percent of patients with ATC (n = 102) reported a history of clinically documented nonthyroid cancer. Of these individuals, 19% (n = 87) had one, 2% (n = 10) had two, and 1% (n = 5) had three prior cancers. Median time from diagnosis of prior nonthyroid cancer to ATC diagnosis was 8 years, with a range of 3 months to 53 years and a mean of 11.1 years ±10.8 years (standard deviation). The anatomical locations of the prior cancers are listed in Supplementary Figure S1. The most common cancers were nonmelanoma skin (28.4%, n = 29), prostate (19.6%, n = 20), and breast (16.7%, n = 17). The most common cancers in females (n = 45) were breast (33.3%, n = 15), nonmelanoma skin (22.2%, n = 10), and colorectal (8.9%, n = 4).
The most common cancers in males (n = 57) were prostate (35.1%, n = 20), nonmelanoma skin (33.3%, n = 19), and lymphoma (15.8%, n = 9). An analysis of the prevalence of cancer history by age of ATC diagnosis revealed a general increase in the prevalence of nonthyroid cancer with age. However, a similar trend was not observed for a history of thyroid cancer (Supplementary Fig. S2). A history of external beam radiation therapy for a prior cancer diagnosis was reported in 23 patients (23%). Among individuals with prior head and neck cancer (n = 6), 67% (n = 4) had received prior radiation therapy.
We performed a subgroup analysis in individuals for whom tumor genomics data were available (n = 183). Specifically, we looked at rates of driver mutations in genes including the RAS family (NRAS, KRAS, HRAS), BRAF, and TP53 (Table 4). BRAFV600E and RAS mutations are mutually exclusive. BRAFV600E mutations were found in 34% (n = 15) and 40% (n = 56) of individuals with and without a history of nonthyroid cancer, respectively; RAS mutations in 18% (n = 8) and 25% (n = 35), respectively; and TP53 mutations in 55% (n = 24) and 51% (n = 70), respectively.
Driver Mutation Profiles on Subset of Patients (N = 183) Who Had Undergone Next-Generation Sequencing Using Either Tumor Tissue or Liquid Biopsy at the Time of Anaplastic Thyroid Cancer Diagnosis
Chi-square test.
TMB, tumor mutation burden; WT, wild type.
No significant differences in the prevalence of the aforementioned driver mutations were noted when comparing patients with and without a history of nonthyroid cancer. TMB was high in 29% (n = 10) versus 32% (n = 35) of individuals with and without a history of cancer, respectively. The type of TP53 mutation was not significantly different between groups (Table 4).
A history of nonthyroid cancer did not significantly impact the treatment regimens undergone for ATC (p = 0.81). The vast majority of patients received multimodal treatment—86% and 79%, respectively, for patients with and without a history of cancer.
Overall survival
The median survival, as well as one- and two-year survival rates for patients, is summarized in Table 5. On Kaplan–Meier analysis, a history of DTC had no significant effect on OS (log rank p = 0.66), while concomitant DTC on pathology was associated with significantly improved OS (log rank p = 0.009) (Fig. 2A, B). However, after adjusting for age and overall stage using multivariate Cox regression analyses, neither a history of DTC nor the presence of concomitant DTC on pathology had a significant association with OS (adjusted hazard ratio [aHR], 0.91; [confidence interval; CI 0.67–1.23]; p = 0.53; and aHR, 0.83 [CI 0.67–1.04]; p = 0.1, respectively) (Table 6).

Overall survival in patients with ATC by
Survival Outcomes of Patients in Different Cohorts
RT, radiation therapy.
Multivariable Cox Regression Analysis for Overall Survival
Adjusting for age and overall stage.
HR, hazards ratio.
A history of nonthyroid cancer (patients with nonmelanoma skin cancer were excluded from this analysis) did not impact OS in either the Kaplan–Meier (log rank p = 0.67) or in the multivariate Cox regression analyses (aHR, 0.85 [CI 0.63–1.14]; p = 0.28) (Fig. 2C and Table 6). Similarly, the number of prior cancers had no significant impact on OS (log rank p = 0.58; aHR, 1.03 [CI 0.52–2.04]; p = 0.94) (Fig. 2D and Table 6). A history of radiation treatment did not significantly impact OS (aHR, 0.84 [CI 0.47–1.49], p = 0.54) (Fig. 2E and Table 6). Finally, the time from diagnosis of prior nonthyroid cancer to ATC diagnosis also did not impact OS (aHR, 1.02 [CI 0.51–2.02]; p = 0.96) (Fig. 2F and Table 6).
Discussion
In our cohort of 451 patients with ATC, 14% reported a history of DTC and 51% had evidence of concomitant DTC at the time of ATC diagnosis. The incidence of concomitant DTC among our cohort is likely underestimated as the identification of concomitant DTC requires surgical specimen or excisional biopsy, which was not available in all patients. In addition, among the individuals with concomitant PTC on pathology in our cohort, only 18% had received a prior diagnosis of PTC. We believe it is possible that the true incidence of prior DTC (14%) is likely underreported, or that the initial DTC lesion was clinically occult or had undergone rapid transformation to ATC before it became clinically apparent.
The prevalence of reported prior DTC and concomitant DTC among individuals with ATC varies widely in literature—ranging from 13% to 78%, and from 33% to 82%, respectively. 1,16,17,22 –24 The significant variation may be partially attributable to the rarity of ATC and to the relatively small sample size of some of these studies. Despite the variations in prevalence, the significant association between both prior and concomitant DTC with ATC has been shown consistently, further supporting the hypothesis that ATC arises as a result of anaplastic transformation from prior DTC. 16,17 Interestingly, among individuals with available clinicopathological data of their prior DTC, most patients presented with aggressive DTC.
The majority of patients had extrathyroidal extension (T3b, T4a, or T4b, n = 22 of 34, 65%), nodal metastasis (N1, n = 28 of 34, 82%), and recurrence of DTC before ATC diagnosis (n = 41 of 52, 79%). A high percentage (n = 46 of 62, 74%) of those patients received radioactive iodine. These findings suggest that ATC may be associated with more aggressive phenotypes of DTC. 25 However, we also showed that prior DTC and concomitant DTC did not significantly impact OS in patients with ATC. Our results are consistent with findings of previous studies that reported similar prognosis among patients with and without prior DTC and concomitant DTC. 16,17,26
A history of nonthyroid cancer was reported in 23% of patients in our cohort. Previous studies reported the prevalence of prior cancer in all cancer patients to be in the range of 3.5–36.9%. 27,28 Literature has consistently shown that cancer survivors are at increased susceptibility of developing second primary malignancies, with a lifetime risk of up to 33%. This increased risk may be due to a variety of factors, including genetic syndromes, environmental exposures, late effects of treatment, or increased surveillance due to prior cancer. 11
In our subgroup analyses of patients who have undergone mutation testing, we did not find that patients with prior nonthyroid cancers had different driver mutations or TMB than those without. However, a higher percentage of patients with ATC reported a history of breast cancer (33% vs. 13%) and prostate cancer (35% vs. 13%) compared with the general population. 9,28 Interestingly, we found head and neck cancer to be overrepresented in our cohort (6%) compared with the national average of 3%. 29 Among the patients with a prior head and neck cancer in our cohort (n = 6), 67% (n = 4) of them received prior radiation therapy. Exposure to radiation at a young age is a well-documented risk factor for PTC. 30 However, the relationship between irradiation later in life and the development of ATC has not been demonstrated and needs to be further explored. Future studies are warranted to further delineate these associations as they may have important implications for screening.
With regard to survival outcomes, no significant difference was noted in OS for a reported history of nonthyroid cancer, suggesting that prior cancer was not a significant prognostic factor in the setting of ATC diagnosis. It is possible that this finding may be confounded by enhanced screening measures and earlier detection in patients with a prior cancer diagnosis. 31 However, the effect of prior cancer on OS does not to appear be consistent across all cancer types and stages. No difference in OS was found among patients with locally advanced nonsmall-cell lung cancer and pancreatic cancer. 32,33 On the contrary, other studies reported prior cancers to be associated with worse survival outcomes in patients with early-stage nonsmall-cell lung cancer and larynx cancer. 34,35
Our findings have important implications for both clinical practice and consideration of clinical trial eligibility in patients with ATC who report a history of cancers. First, multimodal treatment has been shown by multiple studies to convey survival benefits in patients with ATC. 36,37 Given that prior cancers had no significant impact on OS, our data support the use of multimodal treatment in patients with ATC regardless of a cancer history. In addition, a cancer history is a common exclusion criterion for clinical trials in oncology. Our study suggests that patients with ATC with prior cancers should not be excluded from clinical trials. We showed no difference in OS not only with regard to a history of malignancies, but also in terms of time interval between prior cancer diagnoses and ATC diagnoses, providing further evidence that this specific patient population should not be excluded in future clinical trials. Given that ATC trials are uncommon and eligible patients remain limited, eliminating this exclusion criterion is very important to maximizing outcomes in this disease.
Our study has several limitations due to its retrospective nature. First, limited information on prior clinicopathological features of prior DTC and treatment details was available from a retrospective chart review as many presented to MD Anderson following ATC diagnosis. This prevented further stratification based on the prior treatment regimen to explore the effect of prior cancer and cancer therapy on the development and prognosis of ATC. Moreover, no conclusions can be derived from the limited sample of patients with molecular testing. Future studies with wider availability of genomic profiling will help determine if specific combinations of somatic mutations are associated with worse outcomes. Second, MD Anderson is a tertiary cancer center that introduces the possibility that patients with improved survival may be selected for. Lastly, the true prevalence of prior cancers cannot be elucidated from this study as it requires a prospective study design.
However, given the rarity and rapid progression ATC, such data are rare and difficult to obtain. To the best of our knowledge, this study represents one of the first and largest single-institution studies to examine the prevalence and OS of ATC patients with a history of nonthyroid cancers.
Footnotes
Authors' Contributions
Y.H.C.: Data curation and writing—original draft (lead). M.C.: Conceptualization and writing—review and editing. J.S.: Data curation, formal analysis, and writing—original draft. L.X.: Formal analysis. M.G.: Data curation. A.M., M.D.W., S.Y.L., R.D., and M.E.Z.: Writing—review and editing. J.R.W.: Conceptualization (lead), methodology (lead), supervision, and writing—review and editing (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Mark Foundation ASPIRE award (J.R.W. and M.E.Z.), the American Thyroid Association grant (J.R.W.), and the MD Anderson Cancer Center Petrick Multidisciplinary Anaplastic Thyroid Cancer Research Fund (J.R.W., R.D., N.B., S.Y.L., M.E.Z., and M.C.). IRB protocol number is PA14-1082.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1