
Abstract
Objective:
Differentiated thyroid cancer (DTC) is associated with an excellent prognosis, but patients with distant metastatic DTC have a 10-year disease-specific survival (DSS) of just 50%. The incidence of distant metastatic DTC has steadily increased in the United States since the 1980s. The aim of this study was to examine trends in survival and treatment for patients with distant metastatic DTC.
Methods:
In this population-based, retrospective cohort study, patients with distant metastatic DTC were identified from the Surveillance, Epidemiology, and End Results-13 cancer registry program. Multivariable logistic and Cox regression analyses were used to examine factors associated with DSS and management. Annual percentage changes in treatment patterns were calculated using log-linear regression.
Results:
During 1992–2018, 1991 patients (69.7% white, 58.0% female, 47.5% aged ≥65 years) were diagnosed with distant metastatic DTC. Papillary thyroid cancer was the most common histological type (74.5%). While the 10-year DSS for overall DTC increased over time (95.4% for patients diagnosed in 1992–1998, 96.6% in 1999–2008, and 97.3% in 2009–2018; p < 0.01), 10-year DSS for DTC with distant metastases did not change (50.2%, 47.3%, and 52.4%, respectively; p = 0.48). Ten-year DSS rates were reduced for patients aged ≥65 years (28.1%), patients undergoing nonsurgical treatment with external beam radiation therapy and/or systemic therapy (6.0%), and patients undergoing no/unknown treatment (32.8%). On multivariable analysis, oncocytic carcinoma, age 65–79 and ≥80 years, male sex, node-positive disease, larger tumor size, nonsurgical treatment, and no/unknown treatment were associated with increased risk of thyroid cancer death. Between 1992 and 2018, the rate of nonsurgical treatment increased, on average, 1.3% per year (1992–1998: 22.9% vs. 2009–2018: 25.6%; p = 0.03), and the rate of patients receiving no/unknown treatment increased 1.9% per year (1992–1998: 11.3% vs. 2009–2018: 15.6%; p = 0.01). Patients aged 65–79 and ≥80 years were more likely than younger patients to receive nonsurgical management or no/unknown treatment.
Conclusion:
Patients diagnosed with distant metastatic DTC have experienced no improvement in DSS over the past three decades. An increasing proportion of patients diagnosed with distant metastatic DTC are receiving nonsurgical treatment or no/unknown treatment over time; the proportion was highest among the oldest patients.
Introduction
Differentiated thyroid cancer (DTC), including papillary thyroid cancer (PTC), follicular thyroid cancer (FTC), and oncocytic carcinoma, is generally associated with an excellent prognosis. However, patients with distant metastatic DTC historically have had substantially lower 10-year disease-specific survival (DSS) compared with patients with non-metastatic DTC (44% vs. 98%, respectively). 1 Since the 1980s, there has been a steady increase in the incidence of distant metastatic DTC in the United States. 2
The American Thyroid Association (ATA) guidelines regarding the appropriate management of distant metastatic DTC describe a hierarchy of treatment strategies beginning with surgical excision of locoregional disease, followed by radioactive iodine (131I), external beam radiation therapy (EBRT), and consideration of systemic therapy with conventional chemotherapy or kinase inhibitors for 131I-resistant tumors. 3 These recommendations reflect the body of evidence documenting superior outcomes among patients treated with surgery and 131I, and the more recent emergence of promising novel kinase inhibitor therapies such as sorafenib in 2013 and lenvatinib in 2015. 4 –7 An initial trial of sorafenib demonstrated a considerable increase in progression-free survival, from under 6 months in the control group to 10.8 months among patients treated with sorafenib. 6 Before the emergence of these targeted therapies, previous iterations of the ATA guidelines had noted doxorubicin as the main option for systemic therapy despite its having limited efficacy. 8
Despite these advances in targeted therapies for 131I-resistant tumors, the incidence-based mortality for advanced-stage DTC has increased over the past two decades. 2 Notably, incidence-based mortality is a population-level measure that provides a breakdown of mortality by variables associated with cancer occurrence. 9 There is a lack of evidence regarding contemporary trends in DSS from distant metastatic DTC that could reflect the recent evolution in available treatments.
The aim of this study was to examine trends in treatment and survival for patients with distant metastatic DTC.
Methods
Data source
In this population-based, retrospective cohort study, patients with thyroid cancer diagnosed between 1992 and 2018 were identified from the Surveillance, Epidemiology, and End Results-13 (SEER-13) cancer registry program of the National Cancer Institute. 10 The SEER-13 data file contains information from 13 high-quality, population-based cancer registries in 10 states and covers 14% of the U.S. population. Date of last available follow-up was December 31, 2018.
Tumor characteristics
DTC cases were identified using the International Classification of Diseases for Oncology, third edition, and classified according to histological type: 11 PTC (histological codes 8050, 8260, 8337, 8340–8344, 8350, 8450–8460), FTC (8330–8335), and oncocytic carcinoma (8290). According to a recent update of the World Health Organization classification of thyroid neoplasms, histologies previously known as Hürthle cell cancer are termed oncocytic carcinoma. 12 Aggressive variants included the diffuse sclerosing variant (8350), tall cell variant (8344), and insular thyroid cancer (8337). 13,14
The definition of distant metastatic disease was based on the presence or absence of distant organ or extracervical lymph node metastases. For cases diagnosed between 1992 and 2003, the Extent of Disease-10 (EOD-10) codes for distant organ metastases and metastases in distant lymph nodes were used. 15 The American Joint Committee on Cancer (AJCC)-derived TNM staging variables were used for cases diagnosed between 2004 and 2018. 16,17 These codes were combined to categorize all cases diagnosed between 1992 and 2018 by M-stage.
Nodal status was defined between 1992 and 2018 by similarly combining the EOD-10 nodes for patients diagnosed from 1992 to 2003 and the AJCC-derived N-stage variables from 2004 to 2018. 15 –17
Tumor size has been captured in SEER since 1983. Cases diagnosed between 1992 and 2018 were categorized by tumor size using three different schemata: 3 EOD-10 size codes for 1992–2003, Collaborative Staging codes for 2004–2015, and Tumor Size Summary codes for 2016–2018.
Study patients were divided into three different groups based on the year of diagnosis: patients diagnosed during 1992–1998, 1999–2008, and 2009–2018.
Demographic and clinical characteristics
Demographic characteristics and treatment information of interest are shown in Table 1. SEER captures treatment data by reviewing medical records. When multiple surgical procedures are coded, SEER reports the most invasive, extensive, or definitive initial treatment procedure. 18 Surgical procedure was determined using codes from the Site-Specific Surgery (1992–1997) and RX Summ—Surgery Primary Site (1998–2018) SEER variables. Patients coded as having “lobectomy, isthmectomy and partial removal of contralateral lobe (near total thyroidectomy),” “subtotal or near total thyroidectomy,” or “total thyroidectomy” were considered to have had total thyroidectomy (TTx). Patients coded as having “lobectomy with or without isthmusectomy” were considered to have undergone lobectomy.
Demographic and Clinical Characteristics of Patients Diagnosed with Distant Metastatic Differentiated Thyroid Cancer Between 1992 and 2018
Analysis of variance for continuous variables; chi-squared tests for categorical variables.
±, with or without; 131I, radioactive iodine treatment; chemo, systemic therapy; DTC, differentiated thyroid cancer; EBRT, external beam radiation treatment; FTC, follicular thyroid cancer; LND, lymph node dissection; PTC, papillary thyroid cancer; TTx, total/subtotal thyroidectomy.
Patients who underwent “no cancer-directed surgery of primary site” were coded as having no surgery. Patients receiving radiation therapy were captured using the radiation recode variable. Patients who had “internal (radioactive implants & radioisotopes)” radiation therapy were determined to have had 131I. The chemotherapy recode variable was used to identify patients receiving systemic therapy (chemo). Patients were then categorized into the corresponding treatment groups (Table 1). Patients who received “non-surgical treatment” included all patients who did not undergo cancer-directed surgery, including patients receiving no/unknown treatment, EBRT, systemic therapy, or any other treatment.
Statistical analyses
Demographic, clinical, and pathological characteristics of patients with distant metastatic DTC were compared between patients diagnosed during 1992–1998, 1999–2008, and 2009–2018 using analysis of variance for continuous variables and chi-squared tests for categorical variables. Kaplan–Meier analysis was used to estimate the probability of DSS of DTC overall and distant metastatic DTC beyond a certain time point (e.g., 10 years) and to display the estimated DSS function; unadjusted comparisons between two or more survival curves were made using the log-rank test. In patients with distant metastatic DTC, multivariable logistic and Cox regression models were used to evaluate the associations of specific demographic and clinical factors with nonsurgical or no/unknown treatment and risk of thyroid cancer death, respectively.
Covariates included time period of diagnosis, patient age, sex, race/ethnicity, marital status, number of malignant tumors per patient, treatment, lymph node dissection, DTC histology, tumor size, and N-stage. Patients with missing information on covariates were excluded from analysis. A two-sided alpha of 0.05 was used in all analyses to define statistical significance. Statistical analyses were performed using Stata/BC version 16.1 (StataCorp LLC, College Station, TX). Moreover, a propensity score (PS) analysis to adjust for potential confounding variables was performed. 19,20 Patients undergoing surgical and nonsurgical treatment were matched using optimal full PS matching. The PSMATCH Procedure in SAS version 9.4 was used to perform optimal full PS matching. The National Cancer Institute's Joinpoint Regression Analysis program (version 4.9.1.0) was used to calculate annual percentage changes in treatment patterns. 21 This study was granted an exemption by our institutional review board due to use of de-identified data.
Results
Demographic, clinical, and pathological characteristics
A total of 1991 patients with a diagnosis of distant metastatic DTC between 1992 and 2018 were identified in the SEER database (Fig. 1). Of those, 69.7% were white and 58.0% female. The most common histological type was PTC (74.5%), and 46.5% of patients had cervical lymph node metastases. The proportion of aggressive histological variants with distant metastases was 3.7%. TTx followed by 131I was the most frequent treatment approach (46.2%).
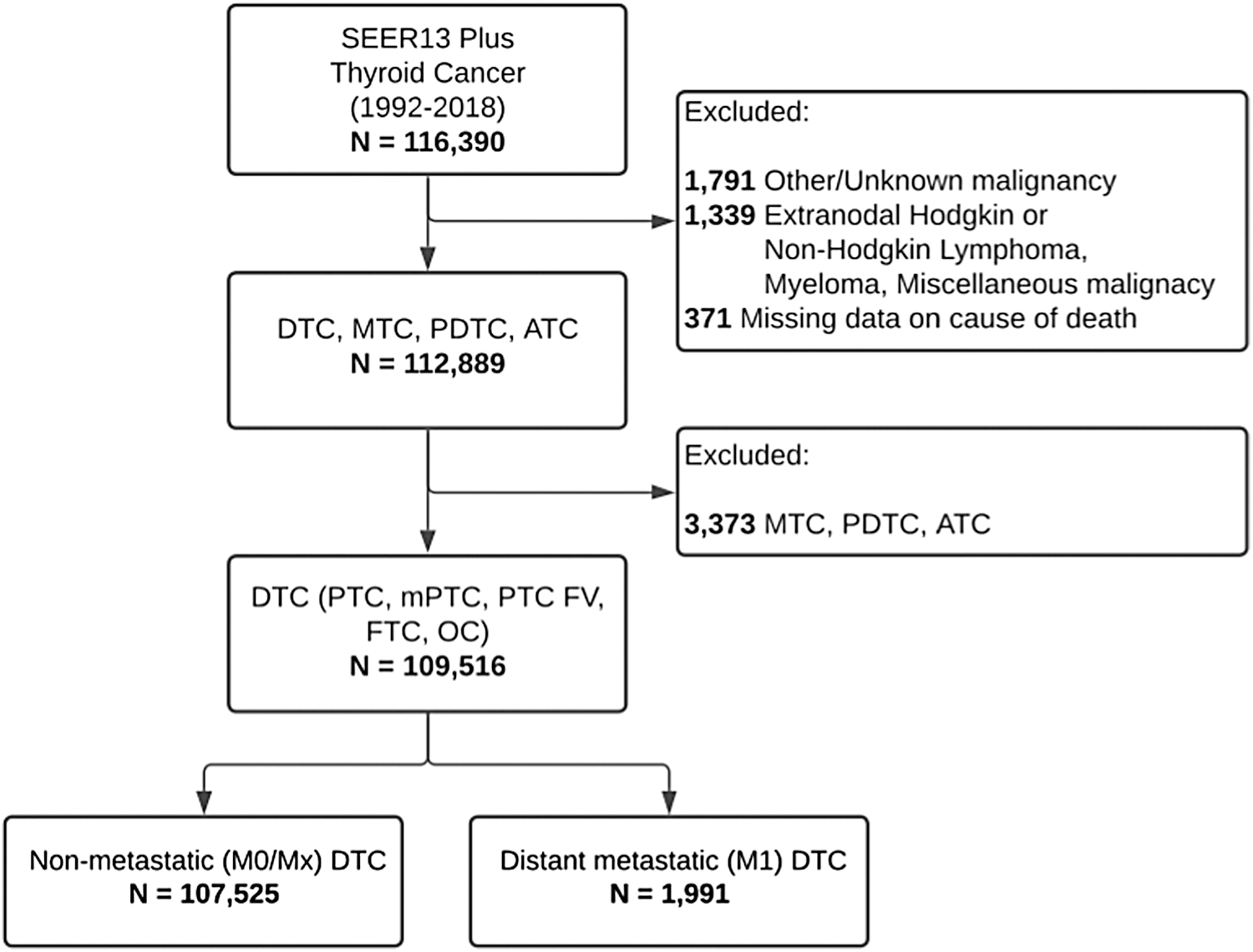
Participant flow diagram. ATC, anaplastic thyroid cancer; DTC, differentiated thyroid cancer; FTC, follicular thyroid cancer; mPTC, microscopic papillary thyroid cancer; MTC, medullary thyroid cancer; OC, oncocytic carcinoma; PDTC, poorly differentiated thyroid cancer; PTC, papillary thyroid cancer; PTC FV, follicular variant of papillary thyroid cancer; SEER-13, Surveillance, Epidemiology, and End Results-13.
The unadjusted variations in demographic, clinical, and pathological variables over time are shown in Table 1. There was no significant difference in the rate of female patients, in marital status, and in the number of malignant tumors per patient. Lymph node dissection, tumor size, and N-stage categories all differed significantly overall by time period (p < 0.01).
Survival analysis
Of all DTC patients, 3.1% (n = 3394) died from thyroid cancer, compared with 43.1% (n = 858) with distant metastatic DTC. The median survival time for DTC overall was 92 months (interquartile range [IQR]: 41–162) compared with 41 months (IQR: 11–99) for distant metastatic DTC. While the 10-year DSS for DTC of all stages differed significantly over time (patients diagnosed in 1992–1998: 95.4%, 1999–2008: 96.6%, 2009–2008: 97.3%; p < 0.01), 10-year DSS for distant metastatic DTC did not change (50.2%, 47.3%, and 52.4%, respectively; p = 0.48) (Fig. 2). The 10-year DSS rates were reduced among patients aged 65–79 years (32.7%) and ≥80 years (10.7%), in patients who underwent EBRT and/or systemic therapy only (6.0%), and in patients who underwent no/unknown treatment (32.8%). Patients who underwent TTx followed by 131I and those who underwent TTx alone had the highest 10-year DSS rates of 64.4% and 56.9%, respectively (Fig. 3).
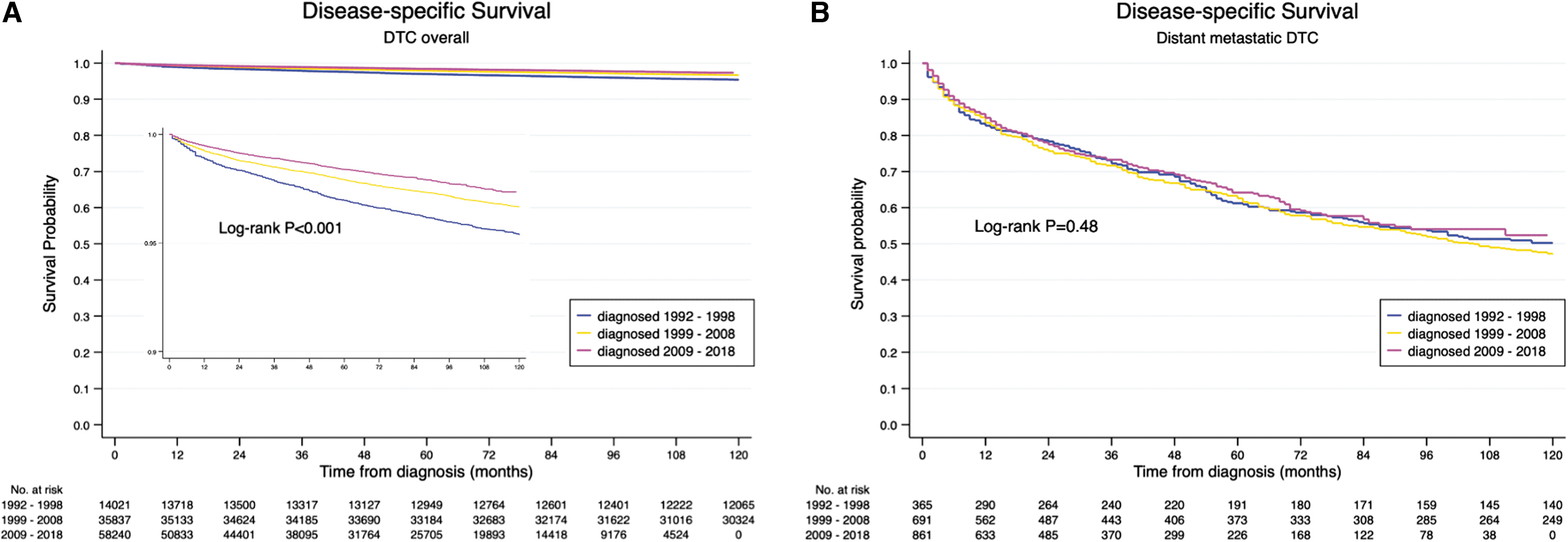
Disease-specific survival of (
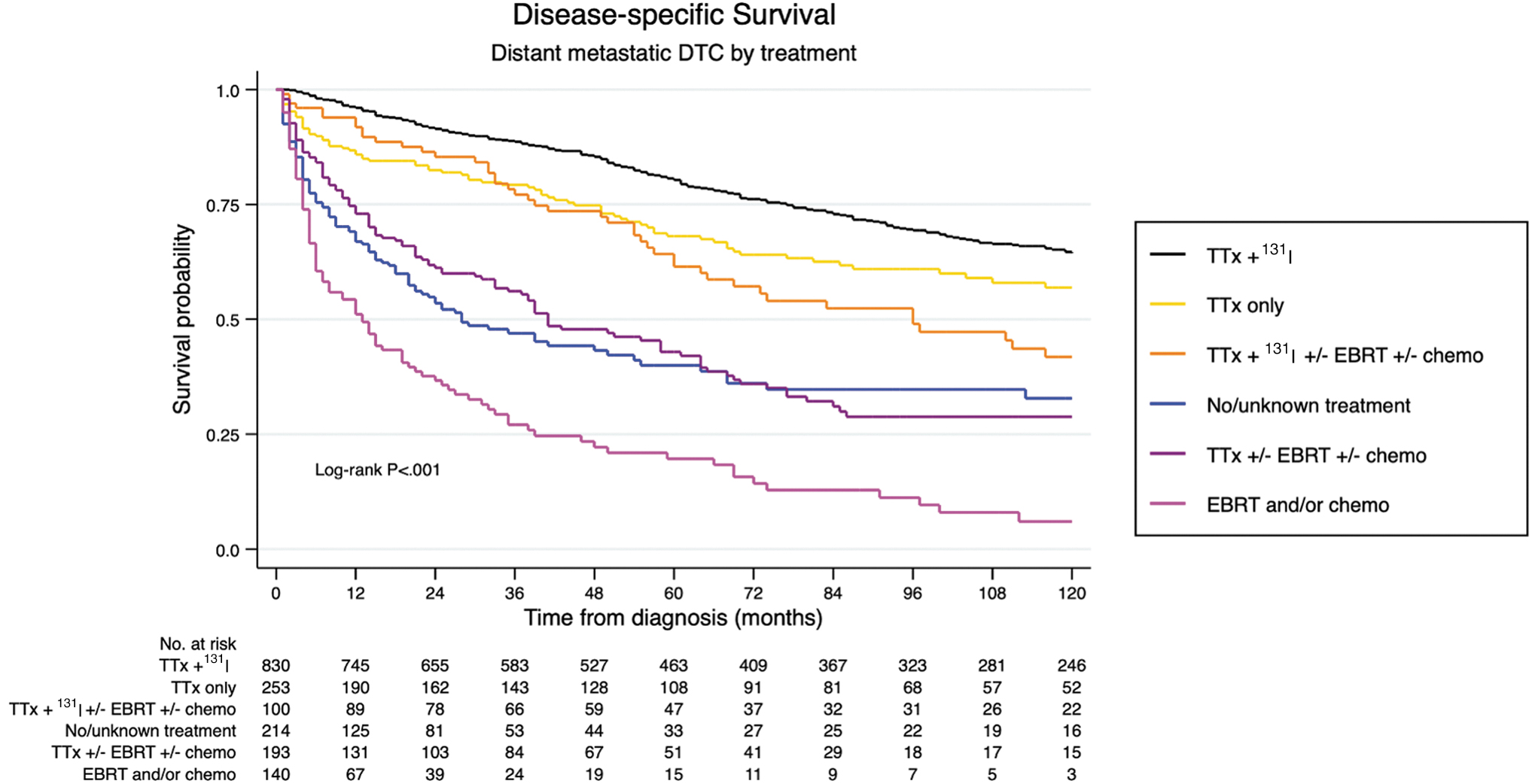
Disease-specific survival of distant metastatic DTC by treatment between 1992 and 2018. 131I, radioactive iodine treatment; chemo, systemic therapy; EBRT, external beam radiation treatment; TTx, total/subtotal thyroidectomy.
After multivariable adjustment, oncocytic carcinoma compared with PTC (hazard ratio [HR] = 2.07 [95% confidence interval {CI} 1.51–2.83]), age 65–79 (HR = 1.95 [CI 1.63–2.33]), age ≥80 (HR = 3.04 [CI 2.38–3.87]), male sex (HR = 1.44 [CI 1.24–1.71]), cervical lymph node-positive disease (HR = 1.42 [CI 1.15–1.74]), tumor size >4 cm compared with ≤1 cm (HR = 2.33 [CI 1.65–3.28]), no/unknown treatment compared with TTx (HR = 2.26 [CI 1.65–3.09]), and EBRT and/or systemic therapy compared with TTx (HR = 3.33 [CI 2.42–4.59]) were associated with an increased risk of thyroid cancer death (Table 2). TTx followed by 131I compared with TTx only (HR = 0.67 [CI 0.52–0.87]) and lymph node dissection compared with no lymph node dissection (HR = 0.78 [CI 0.62–0.97]) were associated with a lower risk of thyroid cancer death.
Multivariable-Adjusted Cox Proportional Hazard Regression of Death from Thyroid Cancer Among Patients Diagnosed with Distant Metastatic Differentiated Thyroid Cancer Between 1992 and 2018
Multivariable Cox regression adjusted for: time period of diagnosis, patient age, sex, race/ethnicity, marital status, number of malignant tumors per patient, median annually household income, area of residency, treatment, LND, DTC histology, tumor size, and N-stage.
Reference categories: diagnosis 1992–1998, patient age <65 years, female sex, white race/ethnicity, married marital status, one malignant tumor per patient, <$50,000 median annually household income, metropolitan area of residency, total thyroidectomy, no LND, PTC, tumor size ≤1 cm, and N0.
aHR, adjusted hazard ratio; CI, 95% confidence interval.
Treatment trends
The rate of nonsurgical treatment increased, on average, 1.3% per year (22.9% in 1992–1998 vs. 25.6% in 2009–2018; p = 0.03), and the rate of patients undergoing no/unknown treatment for distant metastatic DTC increased 1.9% per year (11.3% in 1992–1998 vs. 15.6% in 2009–2018; p = 0.01) (Fig. 4). The proportion of patients receiving systemic therapy increased 2.0% per year (1992–1998: 7.4%, 2009–2018: 8.7%; p = 0.04). After multivariable adjustment, patients aged 65–79 and ≥80 years were more likely to undergo nonsurgical treatment (odds ratio [OR] = 1.96 [CI 1.41–2.71]; OR = 3.90 [CI 2.59–5.85], respectively) and patients ≥80 years more likely to undergo no/unknown treatment (OR = 3.68 [CI 2.48–5.46]) (Tables 3 and 4).
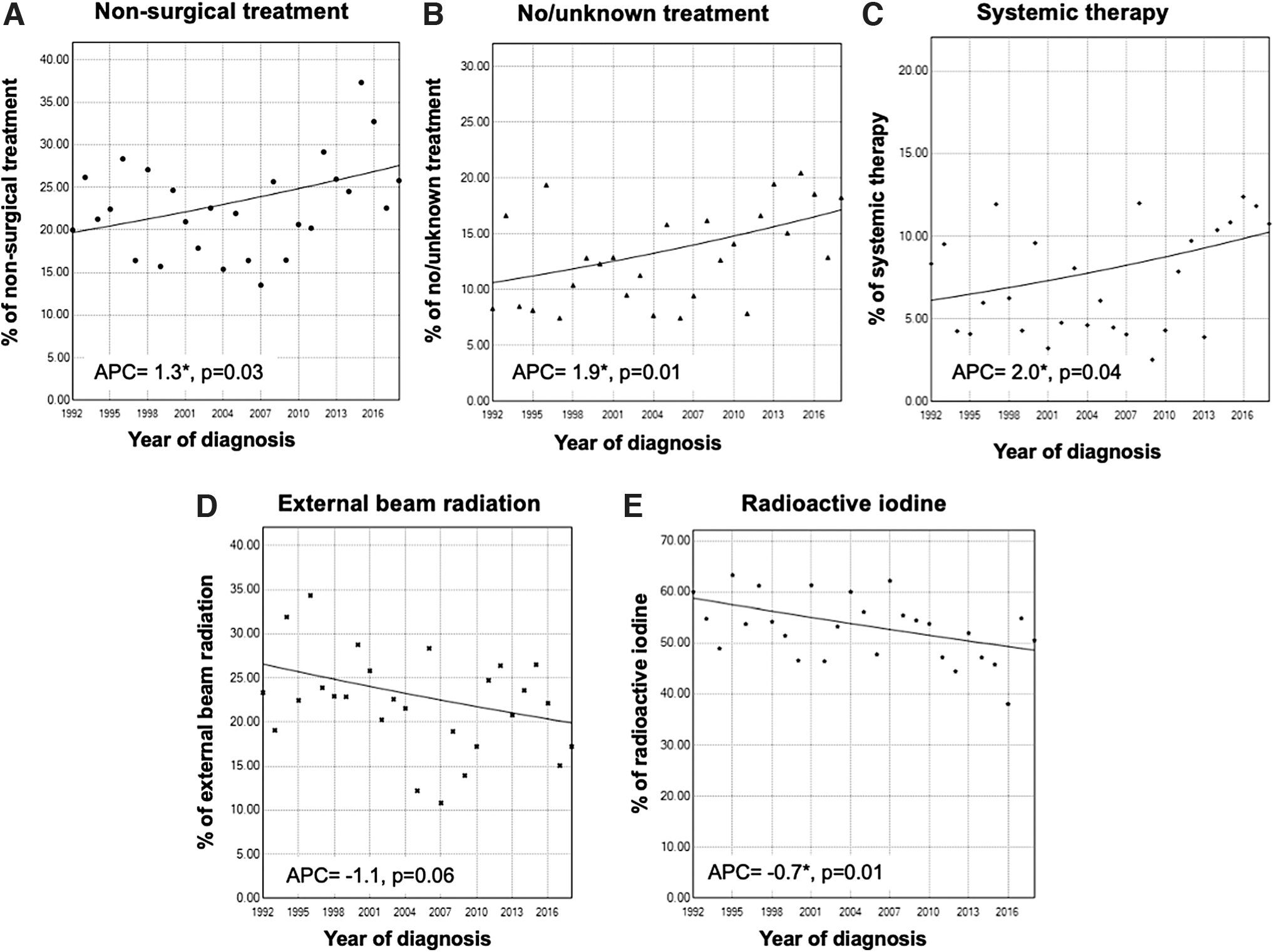
Treatment trends of distant metastatic DTC between 1992 and 2018 (
Multivariable-Adjusted Odds of Nonsurgical Treatment for Distant Metastatic Differentiated Thyroid Cancer Between 1992 and 2018
Multivariable logistic regression adjusted for: time period of diagnosis, patient age, sex, race/ethnicity, marital status, number of malignant tumors per patient, median annually household income, area of residency, DTC histology, tumor size, N-stage, radiation therapy, and systemic therapy.
Reference categories: diagnosis 1992–1998, patient age <65 years, female sex, white race/ethnicity, married marital status, one malignant tumor/patient, <$50,000 median annually household income, metropolitan area of residency, PTC, tumor size ≤1 cm, N0, no radiation, and no systemic therapy.
Multivariable-Adjusted Odds of No/Unknown Treatment for Distant Metastatic Differentiated Thyroid Cancer Between 1992 and 2018
Multivariable logistic regression adjusted for: time period of diagnosis, patient age, sex, race/ethnicity, marital status, number of malignant tumors per patient, median annually household income, area of residency, DTC histology, tumor size, and N-stage.
Reference categories: diagnosis 1992–1998, patient age <65 years, female sex, white race/ethnicity, married marital status, one malignant tumor per patient, <$50,000 median annually household income, metropolitan area of residency, PTC, tumor size ≤1 cm, and N0.
Sensitivity analysis
A sensitivity analysis grouping patients in 5-year intervals showed similar survival rates for DTC overall and distant metastatic DTC (Supplementary Fig. S1). To address potential selection bias, we conducted a subgroup analysis of patients with more extensive primary tumors, that is, N1-stage and/or tumor size >4 cm (Supplementary Fig. S2) that showed similar survival rates by treatment compared with the main cohort. Sample balance after PS matching is shown in Supplementary Table S1, all covariates used in matching met sample balance criteria.
Patients undergoing nonsurgical treatment had significantly higher risk of death from thyroid cancer (log-rank test p < 0.001; Cox model HR = 4.36 [CI 3.32–5.73]). DSS analysis by treatment of the matched patient cohort (Supplementary Fig. S3) showed similar results compared with the main cohort. In addition, DSS rates of patients with more extensive versus localized primary tumors are displayed in Supplementary Figure S4. A trend analysis of the proportion of patients with DTC and distant metastases and DTC-Mx stage among all new DTC diagnoses per year is presented in Supplementary Figure S5.
Discussion
The 10-year DSS for DTC overall increased between 1992 and 2018, likely because of earlier diagnoses at less advanced stages. In contrast, there was no significant change in the 10-year DSS for patients presenting with DTC and distant metastases. In parallel, there was an increase in the proportion of patients undergoing nonsurgical treatment or receiving no/unknown treatment for distant metastatic DTC. Patients aged 65–79 and ≥80 years were more likely than younger patients to receive nonsurgical treatment. Patient age, nonsurgical treatment, and no/unknown treatment were associated with decreased survival.
The observed increase in the proportion of patients receiving nonsurgical treatment likely contributes to the lack of improvement in the 10-year DSS. The current standard of care for DTC with distant metastases is resection of locoregional disease, if surgically accessible, followed by 131I. 3 Unlike many cancers in other organ systems, distant DTC metastases do not preclude resection of the primary tumor because DTC metastases may respond to 131I administration. 3 In a study of 49 patients with distant metastatic DTC at the time of diagnosis, only histology and iodine avidity were significantly associated with improved survival after adjustment for patient age. 22
In a study of 444 patients, 10-year overall survival was 56% among patients with 131I uptake compared with 10% among those without uptake. 5 Among patients without 131I uptake, distant metastasectomy can be considered in selected patients. 23,24 In the present study, TTx with or without 131I ablation was associated with decreased risk of death and higher DSS rates. Together with previously published literature, these results support a continued central role for the surgical management of distant metastatic DTC.
The reasons for the increase in patients receiving nonsurgical treatment are unclear. It is possible that some of the tumors were not resectable because of extensive extrathyroidal extension into critical structures. In SEER, the variable that codes for extrathyroidal tumor extension (EOD-extension) is the same one that defines distant metastatic disease for cases diagnosed from 1992 to 2003; hence, it was not possible to determine extrathyroidal extension for all patients. However, larger tumors with nodal metastases are more likely to preclude surgical resection if they extensively involve certain critical structures such as the aerodigestive tract or major arteries, and this can be used as a surrogate for resectability of the primary tumor. In the present study, tumor size >4 cm and nodal metastases were not associated with an increased likelihood of nonsurgical treatment, suggesting that the observed trend of increased nonsurgical treatment is unlikely to be limited to unresectable tumors.
Among patients with unresectable primary tumors or tumors that are not 131I-avid, EBRT and systemic therapy are potential treatment options. 3 According to this analysis, treatment with systemic therapy increased over time. Before 2013, systemic therapy for non-131I-avid distant metastatic DTC was limited to cytotoxic chemotherapy, with doxorubicin as the most commonly used agent despite limited efficacy. 7,25 –27 More recently, the tyrosine kinase inhibitors sorafenib and lenvatinib have been approved by the U.S. Food and Drug Administration (FDA)-approved for the treatment of 131I-refractory DTC and have been shown to improve progression-free survival. 7,28,29 Given the short follow-up of patients diagnosed after FDA approval of sorafenib and lenvatinib, it is unlikely that potentially higher use had an impact on survival rates.
Furthermore, in our study, it was not possible to draw conclusions about the efficacy of these treatments, especially considering the limitations of SEER, that is, it was an observational study and not a randomized trial, so selection bias/confounding cannot be excluded. Also, SEER does not capture information on type of systemic therapy. However, increasing availability and experience with targeted treatments may change treatment strategies and lead to improved survival. So, this could be reexamined again when longer follow-up has been accrued.
Although systemic therapy with conventional chemotherapy or targeted tyrosine kinase inhibitors are potential options for patients with unresectable DTC, after multivariable adjustment, the risk of thyroid cancer death was higher among patients who received nonsurgical treatment with EBRT and/or systemic therapy and those who received no/unknown treatment. The reason for this could be selection bias. For example, it is possible that among patients with unresectable disease, those with greater disease burden received EBRT and/or systemic therapy, while those with less extensive disease elected to undergo an active surveillance approach given the risk of adverse events. Since SEER does not capture information on the molecular profile of the tumors, this powerful predictor of prognosis could not be considered in multivariable adjustment.
Between 1992 and 2018, patients aged 65–79 and ≥80 years were more likely to receive nonsurgical treatment. Patient age at diagnosis is an important prognostic factor for DTC. 30,31 In a study of 3664 patients with DTC, there was a 37-fold increase in the risk of thyroid cancer death among patients aged >70 years compared with patients aged <40 years. 30 The proportion of patients undergoing nonsurgical treatment was highest among patients aged ≥80 years, which has been shown previously to be not limited to patients with distant metastatic disease. 32 However, the compromised prognosis associated with diagnosis at an older age should not prevent older patients from receiving potentially life-prolonging or life-saving therapies for which they may be eligible. Because SEER has no information on comorbidities, this could not be considered a possible reason for the higher likelihood of nonsurgical or no/unknown treatment at older age.
There are limitations to this study. SEER is a retrospective database, and coding errors are possible. Although SEER includes data regarding systemic therapy use, there are no data on what agent was used. For example, it is unknown whether patients received conventional chemotherapy or targeted therapy with a tyrosine kinase inhibitor. SEER does not include data on why a treatment modality was chosen; it is unknown whether patients who were not treated were offered therapy but declined it. SEER only reports data on radiation and systemic therapy given as first-course treatments, including systemic therapy in clinical trials. 33,34 Consequently, it is unknown whether patients may have received these treatments later in their disease course, such as after disease recurrence or progression.
A recent publication comparing SEER with SEER-Medicare data for other cancer types found an overall sensitivity of 80% for SEER-radiotherapy data and 68% for SEER-chemotherapy data, with an overall positive predictive value of >85% for all treatments. 35 Therefore, underestimation of radiotherapy, such as EBRT and 131I, and systemic therapy is expected, whereas overestimation is less likely. According to the SEER treatment data limitations, it is possible that some of the patients may have had radiation treatment or systemic therapy that was not captured in the SEER records, especially if the treatment was received outside a hospital setting; surgery information, in contrast, is expected to be largely complete. 34 As a result, it is unlikely that there is significant impact on our main conclusion, which is the lack of improvement in survival of distant metastatic DTC, likely due to an increase in nonsurgical treatment.
It was not possible to precisely determine all aspects of nonsurgical treatment approaches because therapies such as radiofrequency, ethanol, or ablation techniques are not specifically coded in SEER. It is likely that, at least in part, tumor size was not coded if patients did not undergo surgery. Cancer registries such as SEER use algorithms to process causes of death from death certificates to identify a single, disease-specific, underlying cause of death. To minimize misattribution, the algorithm introduced in 2010 by Howlader et al was used for all cases diagnosed from 1992 to 2018. 36,37 Despite these limitations, SEER includes data from a large diverse population across the United States and is an important resource to study epidemiological trends.
Conclusion
While earlier diagnoses at less advanced stages may have led to an improvement in DSS for DTC overall over the past three decades, there has been no improvement in DSS for patients presenting with DTC and distant metastases. A growing proportion of patients are receiving nonsurgical treatment or no/unknown treatment over time. Future studies are needed to understand the lack of improvement in DSS for distant metastatic DTC, including investigation of possible changes in tumor biology and factors affecting patient access to surgical and systemic treatments.
Footnotes
Acknowledgment
A.M.S. is part of the Biostatistics Core that is generously supported by the UCSF Department of Surgery.
Authors' Contributions
A.W.: Conceptualization, methodology, software, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization, and project administration. P.C.C.: Software, resources, data curation, writing—original draft, and writing—review and editing. L.C.: Methodology, software, formal analysis, investigation, writing—original draft, writing—review and editing, and visualization. A.M.S.: Methodology, formal analysis, and writing—review and editing. C.M.K.: Conceptualization, resources, writing—review and editing, and supervision. S.A.R.: Conceptualization, resources, writing—review and editing, and supervision. J.A.S.: Conceptualization, resources, writing—review and editing, and supervision.
Disclaimer
These contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
Data Access,Responsibility,and Analysis
A.W. performed the statistical analyses and had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
J.A.S. is a member of the Data Monitoring Committee of the Medullary Thyroid Cancer Consortium Registry supported by Novo Nordisk, Astra Zeneca, and Eli Lilly. Institutional research funding is received from Exelixis and Eli Lilly. All other authors declare no conflicts of interest.
Funding Information
A.W. received funding from the Swiss Cancer League (KLS-5112-08-2020), B. Braun foundation (BBST-D-20-00009), and Martin Allgöwer Foundation. P.C.C. was supported by the National Center for Advancing Translational Sciences, National Institutes of Health (UCSF-CTSI Grant No. TL1 TR001871) and the National Cancer Institute, National Institutes of Health (Grant No. T32CA25107001).
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5