
Abstract
Papillary thyroid carcinoma (PTC) is the most common type of thyroid cancer, usually with an indolent course. ALK fusions are rare in PTC but may give rise to a more aggressive behavior. We report a novel ALK fusion, CCDC149–ALK, not previously described in PTC, detected by next-generation sequencing in a 30-year-old woman with progressive widely metastatic radioiodine-refractory (RAIR) disease to lung, muscle, and brain. The patient was started on alectinib, a second-generation anaplastic lymphoma kinase (ALK) inhibitor. Within eight weeks, her palpable disease had completely regressed, and the serum thyroglobulin decreased dramatically. Restaging imaging demonstrated an objective partial response. Our case highlights the role of ALK fusions in thyroid cancer and highlights its clinical significance in PTC. We recommend deep mutational sequencing in BRAFV600E -negative RAIR PTC to identify targetable genetic alterations, including gene fusions, that may result in dramatic therapeutic benefits.
Case
Our patient had an enlarging thyroid nodule with two indeterminate biopsies over 2 years at the age of 22 years. She has been otherwise in good health without exposure to irradiation, chemotherapy, nor nuclear plants. Her family does not have known hereditary cancer syndrome. In 2012, at age 30 years, a right hemithyroidectomy and isthmectomy were performed for its large size. There were 4 distinct nodules ranging from 1.5 to 2.0 cm. Pathology analysis confirmed a classical papillary thyroid carcinoma (PTC) with minimal extrathyroidal extension without evidence of lymphatic, vascular, or perineural invasion (Fig. 1A).
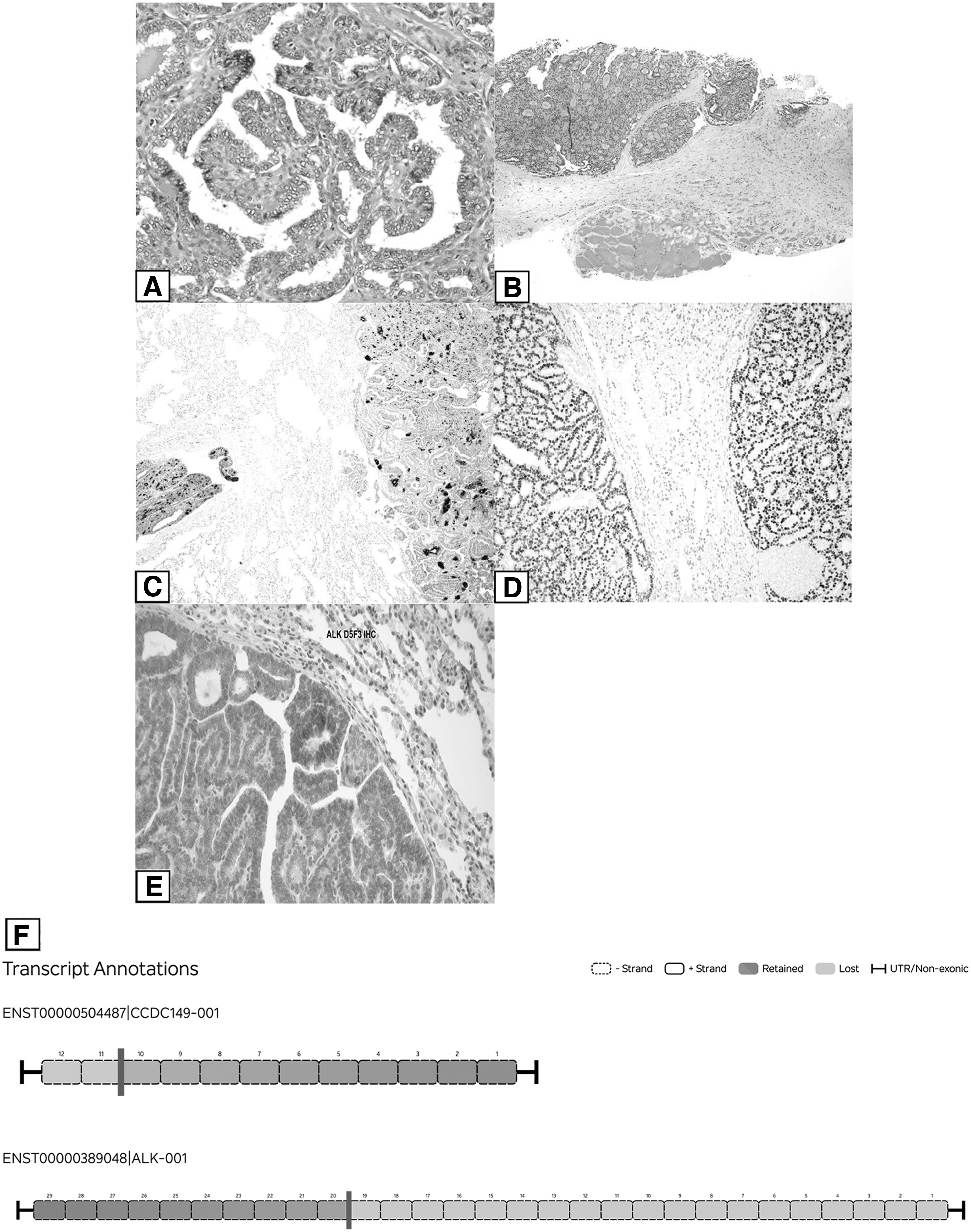
Histological and immunohistochemical features. Primary tumor in the thyroid demonstrated nuclear features of papillary thyroid carcinoma and architectural papillae (
One paratracheal lymph node was negative for carcinoma. After her initial surgery, she subsequently had left completion thyroidectomy, negative for malignancy, but with one perithyroidal lymph node positive for a microscopic focus of metastatic disease. She received 50 mCi of radioactive iodine (131I) for remnant ablation. Recombinant human thyrotropin (rhTSH)-stimulated radioactive iodine (RAI) whole body scan in 2014 did not demonstrate any abnormal uptake. Her TSH was suppressed.
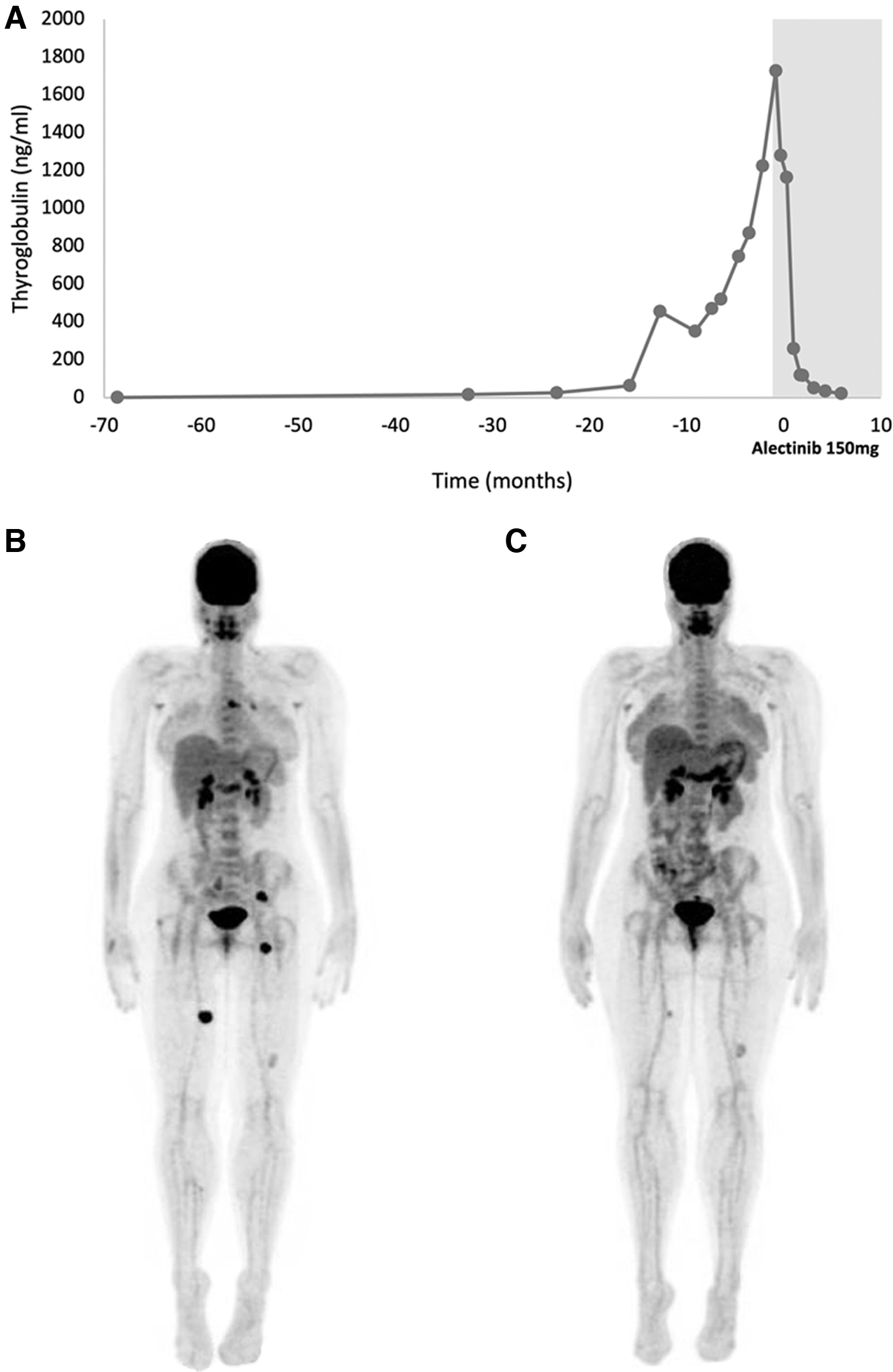
Suppressed thyroglobulin (Tg) remained elevated and continued to uptrend from 6 to 26 ng/mL in 2019 (Fig. 2A). RhTSH scan did not demonstrate any abnormal uptake. When she was admitted for pneumonia in January 2020, lung nodules were seen on chest X-ray. Positron emission tomography-computed tomography (PET-CT) revealed F-fluorodeoxyglucose-avid nodularity in right inferior thyroid, bilateral axillary, left hilar and subcarinal lymph nodes, and left lower and bilateral upper lung.
(
In February 2020, she had a stimulated Tg of 456 ng/mL with a TSH of 129 mIU/L. Repeat CT imaging in April 2020 revealed increased size of lung nodules and suppressed Tg was now 352 ng/mL (Fig. 2A). In July 2020, she underwent robotic left lower and upper lobe wedge resections. Pathology analysis reported metastatic PTC. Despite the resection, Tg was rising to 471 ng/mL (Fig. 2A). She was empirically treated with RAI 208 mCi after rhTSH stimulation in October 2020. Post-therapy whole body scan showed iodine activity in the right lung, two small lesions in the hilum, and the mediastinum, all likely representing metastatic disease.
In January 2021, she developed right-sided weakness and numbness. Brain MRI showed a left parietal and a right occipital lesion. Tg was 1729 ng/mL (Fig. 2A). She underwent craniotomy and resection of the two metastatic lesions confirmed by pathology analysis followed by stereotactic radiosurgery. In February 2021, PET-CT detected metastatic disease with several intramuscular nodules in the left posterior pelvis and right posterior medial thigh, and biopsy of a thigh nodule was performed (Fig. 2B). Histology analysis confirmed metastatic thyroid carcinoma, predominantly follicular patterned, with nodular and focally papillary architecture, and intratumoral fibrosis without dedifferentiation (Fig. 1B).
Immunostaining was positive for Tg (Fig. 1C), PAX-8 (Fig. 1D), and anaplastic lymphoma kinase (ALK) stain in the cell cytoplasm (Fig. 1E). Next-generation sequencing (NGS) of 648 gene panel was performed by Tempus Labs, Inc., and one of the brain lesions, identified a CCDC149–ALK fusion (Fig. 1F). The fusion was confirmed on lung and muscle metastatic samples, as well as in the primary thyroid tumor. No other genetic alterations were identified.
The patient was started on alectinib, a tyrosine kinase receptor inhibitor of ALK, 600 mg twice daily on March 6, 2021. 1 Alectinib caused mild facial edema and rash, which resolved with hydrochlorothiazide and emollient. Within eight weeks, a palpable left flank mass was shrinking, and her appetite and energy were restored. Tg level within 8 weeks decreased to 120 ng/mL (Fig. 2A). PET-CT on July 12, 2021, resulted in either marked improvement or resolution of all known target lesions consistent with partial response by RECIST v1.1 (Fig. 2C). At the time of this report, the patient continues to tolerate alectinib without significant toxicity and with sustained response 13 months after initiating treatment.
Discussion
PTC is the most common thyroid cancer, and indeed, the most common endocrine malignancy. Its incidence has increased from 4.8 to 14.9 per 100,000, primarily due to early detection of subclinical disease with imaging and biopsy, as supported by a stable death rate of 0.5 per 100,000 per year. Women are more affected than men with 2.5:1 ratio, and it occurs during fourth and fifth decades of life. PTC typically has an excellent prognosis after surgery with or without RAI treatment; however, this prognosis may be altered by an aggressive PTC variant. 2,3
The 2022 WHO classification of endocrine tumors creates a new subtype of high-grade thyroid carcinomas, namely differentiated high-grade thyroid carcinomas. 4 These carcinomas retain features of the differentiated carcinoma; here, PTC, but with increased number of mitoses (≥5 per 2 mm2) and necrosis. Given the primary carcinoma is classified as a PTC lacking such high-grade features, and as the lung metastasis retains the differentiated status, there are no overt morphological features to suggest progression toward a revised high-grade phenotype. The presence of tumor metastatic to lung indicates aggressive nonstandard tumor biology.
Genomic profiling has become an increasingly helpful adjuvant diagnostic tool, indicating tumor prognosis and providing mechanistic therapeutic options. PTC usually has an indolent course with a low tumor mutational burden. The most common driver mutations in thyroid cancers are typically point mutations in BRAFV600E or NRAS/HRAS, involving the mitogen-activated protein kinase (MAPK) pathway. Chromosomal rearrangements involving RET, NTRK, ALK, and other genes are mutually exclusive with BRAFV600E and NRAS/HRAS mutations in thyroid cancer, and they have historically been more frequently reported in pediatric and young adults. 5
They may be associated with aggressive clinical course and refractoriness to RAI. 3,6 Recently, Chu et al described kinase fusion-positive thyroid carcinomas showing characteristic morphological features, namely multinodular growth, prominent intratumoral fibrosis/sclerosis, predominantly follicular architecture with glomeruloid structures, and lymphovascular invasion. 7 Furthermore, once BRAFV600E mutation has been excluded by immunohistochemistry or NGS, the likelihood is high that carcinoma is kinase fusion positive. 8
Translocation of ALK with different 5′ fusion partners is seen across diverse cancer types, resulting in oncogenesis through activation of tyrosine kinase involving diverse cellular signaling pathways and upregulation of transcription. 9 ALK is affected in diverse cancers, but most notable significance is the discovery of EML4–ALK rearrangement in lung cancer and the clinical impact from ALK targeting therapies. 1,10 Its clinical significance has been suggested beyond lung cancer. 11
Since the development of crizotinib in 2011, ALK-inhibiting therapies (ALKi) have been expanding. 12 Crizotinib is a tyrosine kinase inhibitor of ALK, ROS-1, and c-MET. After crizotinib, relapsed cancers are found to have secondary ALK mutations leading to crizotinib resistance. Second-generation ALKi—ceritinib, alectinib, brigatinib, and ensartinib—were developed and demonstrated 10–20 times higher potency than crizotinib, better central nervous system penetration, and superior progression-free survival (PFS). 1,13 –15 Third-generation ALKi, lorlatinib, has even higher potency, PFS benefit, and activity against crizotinib-resistant mutations including G1202R. 16,17
ALK rearrangements—most commonly EML4–ALK and STRN–ALK—have been described in 2.2% of PTC. 17 Although prior retrospective analysis has suggested a rather indolent course for ALK rearranged PTC, recent cases have shown otherwise. 18 EML4–ALK and STRN–ALK fusions are more commonly seen with infiltrative thyroid follicular growth, suggestive of dedifferentiation and associated with increased mortality. 19 Another case of EML4–ALK PTC presented with distant metastasis, however, the rarity of ALK rearrangements limits a definitive answer. Literature describes clinical responses to ALKi for thyroid cancer harboring ALK fusions. 20 –22
Aydemirli et al have described a patient with EML4–ALK rearranged PTC who responded to lenvatinib, crizotinib, and then lorlatinib. 20 CCDC6–ALK fusion has been reported in one case of pediatric medullary thyroid carcinoma, who also had clinical, radiographic, and serological response to alectinib, leading to survival of patient beyond 280 days. 21 CCDC149–ALK fusion has been reported in poorly differentiated thyroid carcinoma. 23,24
To our knowledge, ours is the first reported case to describe and target CCDC149–ALK fusion in PTC. The repeated NGS fusion assay of CCDC149–ALK in all disease sites, response to alectinib, and lack of other oncogenes confirm this novel fusion to be the driver mutation in our patient's cancer. CCDC149 is a coiled coil family gene located in chromosome 4 with fusion, including CCDC149 exons 1–10 and ALK exons 20–29. Interestingly, both protein and RNA sequence levels of CCDC149 are expressed in the thyroid gland. 24 The exact function and distribution of expression of CCDC149 are still being studied, with its relevance in the thyroid is unclear, but we suspect its effect as a fusion partner to be similar to CCDC6–ALK where it can enhance ALK activity.
Our young patient had an unexpectedly aggressive course of PTC with extensive metastasis to lung, soft tissue of the extremities, and brain despite standard therapies of surgical resection and RAI. She has experienced an early and deep response on alectinib and remains on treatment. Limitations of our report is limited to a single case report, but with ongoing response of >13 months, we believe the clinical significance is credible.
In patients with advanced radioiodine-refractory PTC who may need systemic therapy, we recommend molecular diagnostic testing that may identify targetable mutations with the potential for therapeutic benefit. We also recommend early recognition of brain as a potential metastatic site for aggressive PTC is warranted when Tg level is rising.
Footnotes
Acknowledgment
We thank Samuel G. Lee for his assistance in data presentation.
Authors' Contributions
H.L contributed to writing original draft, visualization, review, and editing. V.K. carried out writing original draft (supporting), visualization, review, and editing. C.N. carried out review and editing. P.M.S. was involved in writing original (supporting), review, and editing. M.V. and L.J.W. were in charge of review and editing. A.M. was in charge of conceptualization, investigation, project administration, review, and editing. W.S. was involved in supervision, project administration, review, and editing.
Ethics
Patient provided verbal, not a written consent, per our institutions' policy for an anonymous case report. Institutional review board review is not required for a case report in our institution.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.