
Abstract
Background:
The 2016 American Thyroid Association guidelines recommend that hyperthyroid patients should be euthyroid before thyroidectomy. This recommendation is based on low-quality evidence. In this retrospective cohort study, we compare peri- and post-operative outcomes of patients with hyperthyroidism who were controlled versus uncontrolled at the time of thyroidectomy.
Methods:
A retrospective cohort study was performed on 275 hyperthyroidism patients at a single institution from December 2015 to November 2022. Patients were defined as hyperthyroid if they had a diagnosis of hyperthyroidism with at least one suppressed thyrotropin (TSH). Patients were considered uncontrolled if triiodothyronine or thyroxine (T4) was elevated immediately before surgery. Patient demographics, perioperative data, and postoperative outcomes were compared with Chi-square and Wilcoxon Rank Sum tests, as appropriate.
Results:
Of the 275 patients, 84.3% were women and 51.3% were uncontrolled at time of surgery. Controlled patients had higher median [interquartile range] TSH (0.4 [0.0, 2.4] mIU/L vs. 0.0 [0.0, 0.0] mIU/L, p < 0.001) and lower free T4 (fT4) (0.9 [0.7, 1.1] ng/dL vs. 3.1 [1.9, 4.4] ng/dL, p < 0.001), respectively. Uncontrolled patients were more likely to be diagnosed with Grave's disease (85.1% vs. 67.9%, p < 0.001) and to undergo surgery due to medication intolerance (12.1% vs. 6%) or history of thyroid storm (6.4% vs. 1.5%) (p = 0.008). Uncontrolled patients were also more likely to take a larger number of preoperative medications (2.3 vs. 1.4, p < 0.001). No patient in either group experienced thyroid storm precipitated by surgery. Controlled patients had shorter operative times (7.3% vs. 19.8% <1 hour, p < 0.014) and decreased median estimated blood loss (15.0 [5.0, 30.0] mL vs. 20.0 [10.0, 50.0] mL, p = 0.002). Both groups experienced similar, low rates of postoperative complications, apart from an increase in temporary hypocalcemia in the uncontrolled group (13.4% vs. 4.7%, p = 0.013).
Conclusion:
Our study is the largest to date examining the postoperative outcomes of patients with uncontrolled hyperthyroidism who undergo thyroidectomy. Our results affirm that thyroidectomy in actively thyrotoxic patients is safe and will not precipitate thyroid storm.
Introduction
While only 1
Use of antithyroid medications such as methimazole and propylthiouracil is associated with known side effects of hepatotoxicity, agranulocytosis and congenital defects. Radioactive iodine is contraindicated in patients with thyroid eye disease and in patients who are pregnant, desire a pregnancy in the near future, or are unable to maintain 6 feet of distance from pregnant women or infants in their household. 5 In addition to the aforementioned side-effects, medical and radioactive therapies often require weeks to months (if ever) to achieve biochemical and symptomatic resolution, and may even require repeated treatments. 6
With regard to surgical intervention, a 2017 National Inpatient Sample Study showed that surgery for Graves' disease in the hands of high-volume surgeons results in excellent postoperative outcomes and low complication rates. 7 If surgical intervention is deemed most appropriate, the 2016 American Thyroid Association Guidelines state that hyperthyroid patients should be rendered euthyroid before surgery to prevent thyroid storm (strong recommendation, low-quality evidence). 2
This recommendation is further supported by the 2020 American Association of Endocrine Surgeons (AAES) Guidelines for the Definitive Management of Thyroid Disease. 8 These recommendations are based on low quality and limited evidence. It is hypothesized that storm is likely precipitated by gland manipulation, leading to excess hormone release into the patient's bloodstream. 9 It has also been suggested that anesthesia itself can precipitate thyroid storm, though data on this are limited. 10
While achieving the euthyroid state is ideal, patient-related factors, such as allergies to medications, drug side effects, refractory disease, compliance with therapy, and the urgency in which definitive therapy is needed, are critical in determining whether or not hyperthyroidism can be controlled preoperatively. Due to the medically underserved nature of our patient population and our position as the only high-volume, quaternary academic referral center in the state, many of our patients are unable to achieve euthyroid status.
Questions remain regarding the safety and efficacy of surgery in the actively hyperthyroid state. With this in mind, we compared peri- and post-operative outcomes for patients with both controlled and uncontrolled hyperthyroidism at the time of thyroidectomy. Our hypothesis was that surgery could be performed before achieving euthyroid state in hyperthyroid patients without compromising postoperative outcomes.
Methods
After Institutional Review Board approval was obtained, we performed a retrospective cohort study of 275 consecutive hyperthyroidism patients undergoing thyroidectomy from December 2015 to November 2022. Inclusion criteria included undergoing thyroidectomy at our institution, being >18 years of age, and having a diagnosis of hyperthyroidism documented in the medical record. In addition to a documented diagnosis, the included patients had either a suppressed preoperative thyrotropin (TSH) or triiodothyronine (T3)/thyroxine (T4) elevation (Fig. 1).
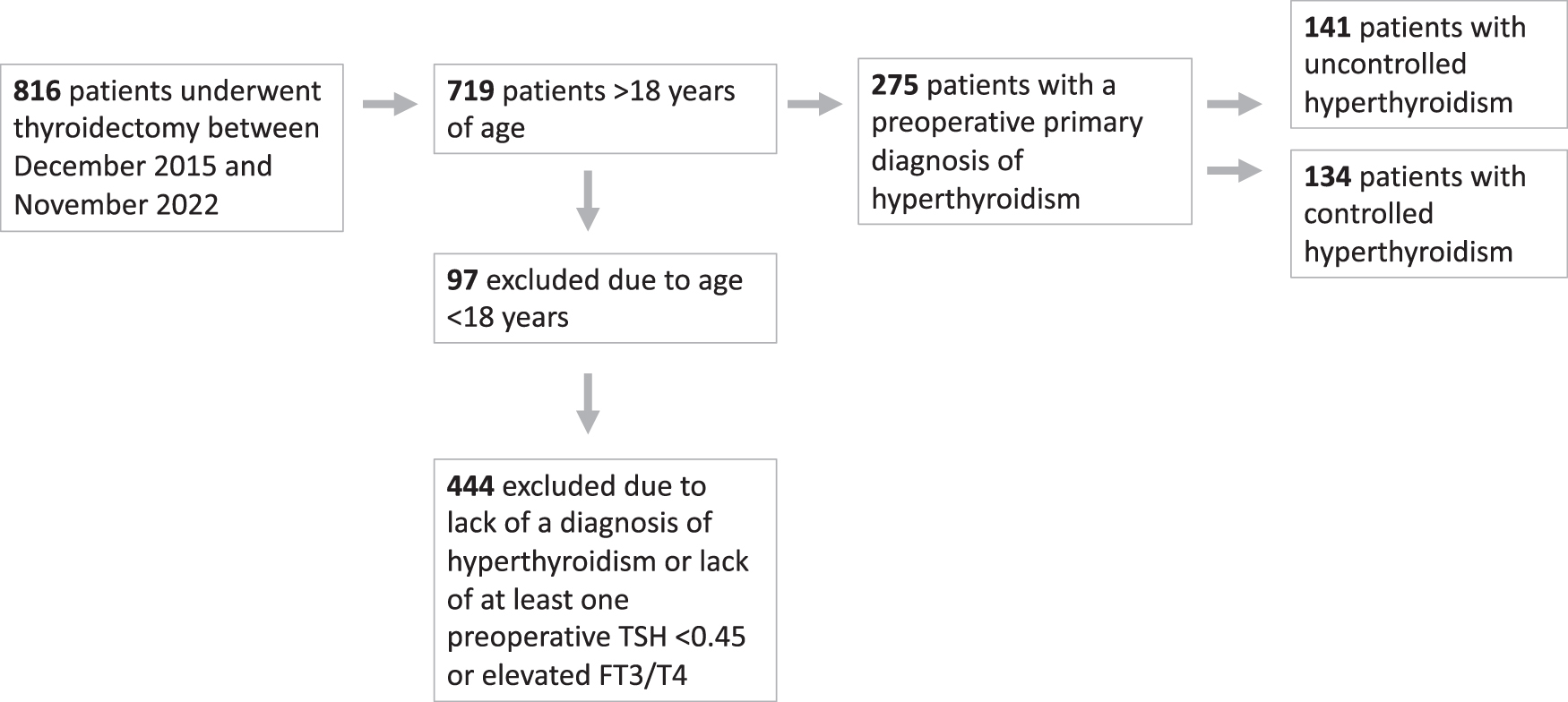
Participant flow diagram.
Four faculty surgeons participated in this study, all of whom are high-volume endocrine surgeons. Patients were defined as uncontrolled if T3 or T4 was elevated immediately before surgery (normal = 2.8–4.4 pg/mL, 0.58–1.64 ng/dL, respectively). Electronic medical records were examined to classify patient demographics, disease etiology, patient-reported reason for surgery, preoperative medication(s), operation length, intraoperative blood loss, and postoperative outcomes.
Temporary hypocalcemia was defined as calcium <8.4 mg/dL (range 8.4–10.2), normalizing by 6 months postoperatively, and liberated from calcium supplementation. Permanent hypocalcemia was defined as continued need for calcium supplementation by most recent postoperative visit, >6 months post operatively. Similarly temporary hoarseness was defined as patient-reported voice changes, with resolution achieved by 6 months postoperatively.
Permanent hoarseness was defined as patient-reported voice changes without resolution at the most recent follow-up, >6 months postoperatively. Hematoma was classified as those patients requiring operative evacuation. We defined thyroid storm according the to the Japan Thyroid Association Definition and Diagnostic Criteria, which includes (1) the presence of thyrotoxicosis with elevated levels of free T3 (fT3) or T4 in addition to (2) evidence of end-organ failure, resulting from breakdown of physiologic compensation mechanisms.
Some stigmata of thyroid storm can include derangements in the central nervous system, fever, tachycardia or arrythmia, congestive heart failure, or gastrointestinal and hepatobiliary manifestations. 8,11
Patient demographics and outcomes were summarized using medians and interquartile ranges for continuous data, as all values exhibited a non-normal distribution. Counts and percentages were used to describe categorical data. We made comparisons between groups using Wilcoxon Rank Sum test and Chi-square tests, as appropriate. Comparison of OR time between groups was performed using a Cochran–Mantel–Haenszel test stratified by surgeon performing the case.
Missing data were minimal in our cohort with respect to TSH, calcium, and fT4, which were missing for 5 (2%), 11 (4%), and 3 (1%) records, respectively. A larger proportion of fT3 was missing, comprising 124 (45%) of patient records; however, since either fT4 or fT3 was used as a marker of hyperthyroidism, we deemed this acceptable. R (version 4.2.1, 2022) software was used for data analysis. Associations were considered significant at p < 0.05.
Results
Of the 275 patients, 84.3% were women and 51.3% were uncontrolled at time of surgery. Controlled patients had higher median TSH (0.4 [0.0, 2.4] mIU/L vs. 0.0 [0.0, 0.0] mIU/L, p < 0.001) and lower fT4 (0.9 [0.7, 1.1] ng/dL vs. 3.1 [1.9, 4.4] ng/dL, p < 0.001), respectively. Uncontrolled patients were more likely to be diagnosed with Grave's disease (85.1% vs. 67.9%, p < 0.001) and to undergo surgery due to medication intolerance (12.1% vs. 6.0%) or history of thyroid storm (6.4% vs. 1.5%, p = 0.008).
Uncontrolled patients were also more likely to take a larger number of preoperative medications [2.3 (±1.0) vs. 1.4 (±0.8), p < 0.001]. Preoperatively, uncontrolled patients were more commonly prescribed anti-thyroid medication (89.4% vs. 72.4%, p = 0.009), beta-blockers (61.0% vs. 45.5%, p < 0.001), steroids (31.2% vs. 7.5%, p < 0.001), and Lugol's solution (7.8% vs. 2.2%, p = 0.036) (Table 1).
Demographics
SD, standard deviation; T3, triiodothyronine; T4, thyroxine; TSH, thyrotropin.
Eleven patients already admitted to the hospital and found to be in thyroid storm before operation were included in postoperative outcomes assessment, nine of whom were uncontrolled at the time of surgery. Of those patients not already in thyroid storm, no patient in either the controlled or uncontrolled groups progressed to storm during the perioperative period.
Controlled patients had shorter operative times (19.8% vs. 7.3% <1 hour, p = 0.014) and decreased median estimated blood loss (15.0 [5.0, 30.0] mL vs. 20.0 [10.0, 50.0] mL, p = 0.002). When controlled for surgeon performing the case, the association between controlled status and operative time was statistically significant (p < 0.001).
Both groups experienced similar, low rates of postoperative complications. Temporary hypocalcemia was more prevalent in the uncontrolled group (13.4% vs. 4.7%, p = 0.013). Permanent hypocalcemia was experienced by 0 patients in the controlled group, and 4 patients in the uncontrolled group (p = 0.137). Temporary hoarseness was noted in 6.6% of the control group and 5.0% of the uncontrolled group (p = 0.531). Permanent hoarseness was noted in 1 patient from each group (p = 0.967) (Table 2). Laryngeal exams to assess vocal cords are not routinely performed at our institution, and they are reserved for patients with voice symptoms or who have had prior anterior neck surgery.
Operative Characteristics and Patient-Related Complications
Additional subgroup analyses were performed comparing demographics and operative complications in the highest quartile of uncontrolled patients (>3.12 ng/dL fT4 preoperatively) versus hyperthyroid patients in the remaining 3 quartiles. An additional analysis was also performed looking at uncontrolled patients (>3.12 ng/dL fT4 preoperatively) versus patients who were controlled before surgery. The results of these sub-analyses were consistent with the conclusions of our original analysis (Supplementary Tables S1–S4).
Discussion
Thyroid storm is a life-threatening complication of hyperthyroidism. Though its exact origins and pathophysiology are poorly understood, it is postulated that a physiologic insult precipitates the transformation of simple thyrotoxicosis to an overwhelming release of thyroid hormone. 8 Historically, the trauma from surgical thyroidectomy was thought to represent such a potential insult. As a result of these widely adopted hypotheses, the 2016 American Thyroid Association guidelines state “If surgery is chosen as treatment for Graves' Disease, patients should be rendered euthyroid prior to the procedure.” 2
However, evidence to support this recommendation is lacking in the literature. To further complicate decision making, the 2020 American Association of Endocrine Surgery guidelines for thyroid surgery state that thyroid storm is a potential risk of surgery, even if the patient is rendered euthyroid before operative intervention. It is postulated that storm in these cases is likely precipitated by gland manipulation, leading to excess hormone release into the patient's bloodstream. 9 Regardless of the degree of preoperative control of hyperthyroidism, careful perioperative management of these patients is crucial to achieve optimal outcomes. 12
Early operation on hyperthyroid patients has been shown to improve biochemical recovery and has not been associated with increased complications in previous studies. 9,12 –14
We hypothesized that delaying operation in this patient population to achieve euthyroid state would result in increased cost and distress in patients due to continual symptomatology, chronic medical therapy, and even inpatient hospitalizations. Importantly, a euthyroid state may not be achievable in many patients for a variety of reasons, including (but not limited to) medication intolerance or non-adherence.
Surgical referral could be restricted based on current guidelines, as endocrinologists and primary care doctors may be reluctant to consult a surgeon without achieving euthyroid state. In addition, we hypothesized that medically underserved populations would have more difficulty achieving euthyroid state due to issues of access and affordability of treatment, though data in this regard are limited. This is anecdotally the case in our patient population, as >15% of Alabaman's live below the poverty line.
Patients in lower socioeconomic strata have been shown to have greater incidence of clinical manifestations best treated with surgery, such as ophthalmopathy and higher severity of disease, 15 thus demonstrating that this is a group that could benefit especially from timely referral to surgical care.
In 2021, our group performed a small study demonstrating the safety of operating on Graves' disease patients who were hyperthyroid at the time of operation. No patients in our study developed overt thyroid storm as a result of surgery. 16 This conclusion was also borne out in a similar retrospective cohort study by Al Jassim et al. in 2018. 12 Their findings similarly show that no biochemically hyperthyroid patients converted to thyroid storm in the perioperative period. 12
A 2018 study by Short et al. of 151 patients undergoing thyroidectomy with primary hyperthyroidism (57 who were uncontrolled at time of operation) supported these conclusions. The only difference found between the preoperatively euthyroid and hyperthyroid groups was increased use of intraoperative beta blockade on hyperthyroid patients. 17
A 2021 systematic review examining surgery for primary hyperthyroidism examined 26 retrospective and prospective cohort studies, of which 4 were judged to have moderate risk of bias, 1 had high risk of bias, 2 had serious risk of bias, and 1 had critical risk of bias. Twelve of those studies included data on preoperatively controlled versus uncontrolled hyperthyroid patients. Thyroid storm did not occur in either group in any of the literature reviewed. 18
We have, with this retrospective review, contributed the largest study to date demonstrating the safety of operating in the hyperthyroid state. In our 275-patient cohort, more than half were actively hyperthyroid at the time of operation, with no significant difference in low rates of permanent postoperative complications or incidence of thyroid storm.
Though perioperative complications such as blood loss and operative time were increased in uncontrolled hyperthyroid patients, one could argue this as an expected, but surmountable technical challenge to the surgeon that has little to no effect on clinically important patient outcome. The experienced surgeon will attest that hyperactive glands are often goitrous, woody/inflamed, and demonstrate increased vascularity, making the administration of a saturated iodine solution (Lugol's) to decrease vascular supply an attractive choice to some clinicians. 19,20
Admittedly, administration of Lugol's solution is not routine practice at our institution, as our patient population is often non adherent to preoperative administration. In addition, some data demonstrate that it does not change surgical outcome or surgeon perception of case difficulty. 21
The uncontrolled hyperthyroid cohort exhibited a significant but temporary increase in rates of postoperative hypocalcemia (13.4% vs. 4.7%). We postulate that the degree of postoperative hungry bone syndrome is more severe in the uncontrolled group and accounts for much of the observed hypocalcemia rather than hypoparathyroidism alone. 22 These data regarding elevated risk of temporary hypocalcemia are important for the operating surgeon to appropriately counsel the patient and to ensure preoperative preparation with oral calcium and/or vitamin D supplementation, whenever possible. 23
As inherent to any retrospective, single institution study, our findings are not without limitation. Our patient referral pattern necessitates open communication with our colleagues providing anesthetic care for these complex cases. In addition, it is our practice to routinely administer steroids on anesthetic induction to reduce conversion of circulating fT4 to T3. The results of this study may not be generalizable in settings without access to skilled and experienced anesthesiologists, leading to selection bias in our reporting.
Careful perioperative management is crucial and significantly contributes to patient safety and outcomes. 13 In addition, our retrospective review is hindered by limitations in data capture, as not all hemodynamic variables and perioperative challenges are reflected in the anesthesia record. Our data are also limited to patients who were eligible for surgical intervention, one potential source of selection bias in our study.
Lastly, in this study, we used the Japanese Thyroid Association (JTA) criteria 11 to define thyroid storm rather than the Burch Wartofsky Point Scale (BWPS). 24 Our institution has historically favored the JTA in clinical practice over the BWPS since biochemical evidence of hyperthyroidism is not formally included in the diagnostic algorithm. Given this institutional practice, sufficient data are not available to calculate the BWPS score (e.g., patients were noted to be tachycardic [heart rate (HR) >100] or not, but whether the HR was 110, 120, or 130 was not recorded). It is known that the JTA is less sensitive than the BWPS in diagnosing thyroid storm, and potential underdiagnosis of this condition in our dataset is a limitation of our study. 2
Future work will be aimed at better characterizing the intraoperative hemodynamic changes that take place in controlled and uncontrolled hyperthyroid patients. This will allow us to better evaluate the unique needs of this patient population and establish best practices for operative intervention on uncontrolled hyperthyroid patients. In addition, confirmatory prospective research would contribute substantially to our knowledge of this complex clinical question, and help guide our practice.
Conclusions
Thyroidectomy can be performed safely and without precipitating thyroid storm in actively hyperthyroid patients. Therefore, surgical evaluation of hyperthyroid patients should not be limited to only those in the euthyroid state.
Footnotes
Authors' Contributions
J.F.: Conceptualization, data collection, analysis, writing, review, and editing (lead); P.Z.: analysis, writing, review, and editing (equal); A.A.: data collection, analysis, review, and editing (supporting); C.M.L.: analysis, review, and editing (supporting); R.A.: data collection, analysis, review, and editing (supporting); A.G.: analysis, writing, review, and editing (supporting); K.R.: analysis, writing, review, and editing (supporting); J.P. and H.C.: conceptualization, analysis, writing, review, and editing (supporting); B.L.: conceptualization (lead), analysis, writing, review, and editing (supporting).
Ethical Approval
All research activities related to this manuscript adhere to the legal and ethical requirements of the United States of America and the Institutional Review Board.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4