
Abstract
Background:
Iodine-induced thyroid dysfunction is a potential risk among susceptible individuals. Iodinated contrast media is a common source of an acute iodine load used in the health care setting and is frequently required for diagnostic computed tomography scans, coronary angiograms, and other radiologic studies. However, the epidemiologic risks of iodine-thyroid dysfunction have not been fully established in the United States.
Methods:
This population-based retrospective cohort study used the U.S. Veterans Health Administration database between 1998 and 2021 and included adults aged ≥18 years with a serum thyrotropin (TSH) measurement. Multivariable logistic regression was used to ascertain the risk of incident thyroid dysfunction (defined by repeated measurements of serum thyroid function) following iodine exposure, adjusting for age, sex, race/ethnicity, baseline serum TSH concentration, and duration between baseline and follow-up TSH concentration.
Results:
The cohort was composed of N = 4,253,119 veterans (mean ± SD = 63.5 ± 14.3 years; 92.9% men; 65.6% non-Hispanic Whites) with 8,729,155 corresponding pairs of serum TSH measurements, from which there were 499,897 TSH pairs with intervening iodine exposure. Thyroid dysfunction occurred in 4.8% of those pairs who had received iodine contrast and 3.6% of those without iodine exposure. Iodinated exposure was associated with an increased risk of thyroid dysfunction (odds ratio [OR] = 1.39, 95% confidence intervals [CI] = 1.37–1.41, p < 0.001) and consistent for all types of serum thyroid dysfunction (overt or subclinical hypo-/hyperthyroidism). Men were at higher risk for the development of thyroid dysfunction than women (men: OR = 1.42, 95% CI = 1.40–1.44; women: OR = 1.16, 95% CI = 1.11–1.21; p-for-interaction <0.001).
Conclusions:
In this largest analysis of U.S. adults to date, iodine exposure was associated with only clinically small absolute increased risks of thyroid dysfunction, particularly in men. These findings suggest that screening of thyroid function following iodinated contrast administration should be targeted to high-risk individuals.
Introduction
Iodine is a micronutrient essential for thyroid hormone production, with 150 μg per day as the recommended intake for adults in the United States. Iodinated contrast media is commonly used in several types of radiologic studies. Since computed tomography (CT) scans were first introduced in the 1970s, their annual use has climbed to >70 million scans in the United States, 1 while >1 million coronary angiograms are performed annually in the United States for cardiac catheterization procedures. 2 A single dose of iodinated contrast administered for CT scans, coronary angiography, and other radiologic procedures can contain up to 13,500 μg of free iodine and 15–60 g of bound iodine, which is equivalent to several hundred times the recommended daily iodine intake. 3 Following exposure to an iodinated contrast agent, iodine stores in the body remain raised up to several months 4 to provide a continuous supply of iodine, thereby increasing the risk of iodine-induced serum thyroid dysfunction.
Although most individuals are able to adapt to the high iodine load, certain susceptible subgroups (e.g., those with a history of thyroid disease and/or thyroid nodules) are at risk for thyroid dysfunction (i.e., hypothyroidism or hyperthyroidism). 5 This can occur after only a single exposure to an iodine-rich substance, as a result of two well-established physiologic principles in thyroidology: the failure to escape from the acute Wolff–Chaikoff effect (resulting in hypothyroidism) and the Jod–Basedow phenomenon (resulting in hyperthyroidism). 5 Small series have shown that subjects exposed to high amounts of iodine have mildly low serum thyroid hormone levels and compensatory increased serum thyrotropin (TSH) to the upper limit of the normal range. 6 –8 Similarly, iodine-induced hyperthyroidism might be transient or permanent, and risk factors include nontoxic or diffuse nodular goiter, latent Graves' disease, and chronic iodine deficiency. 5 The risks of iodine-induced thyroid dysfunction are particularly pertinent in older individuals, in whom the adverse effects of hyperthyroidism and hypothyroidism may worsen underlying health conditions.
The U.S. Veteran population is at high risk for the adverse effects of thyroid dysfunction, given this group's older age and high prevalence of comorbidities 9 ; yet the association between routine medical iodine exposure and serum thyroid dysfunction has not been examined in this group. Moreover, thyroid dysfunction is an established risk factor for multiple adverse cardiovascular outcomes, including atrial fibrillation, congestive heart failure, and cardiovascular mortality 10 –12 potentially exacerbating the elevated cardiovascular disease burden present in the Veteran population. 13 In this large population-based study of the Veterans Health Administration (VHA), we investigated the association between exposure to an iodine load and incident thyroid dysfunction employing repeated measurements of serum thyroid function.
Methods
A population-based retrospective cohort study was performed using the Veterans Affairs Corporate Data Warehouse (CDW) database, the national repository of clinical and administrative records from all U.S. VHA inpatients and outpatients, for the period from March 10, 1988 to October 20, 2021. The study sample included adults (age ≥18 years) with at least one pair of serum TSH measurements, consisting of a normal baseline TSH and a subsequent TSH within the ensuing year. Each subject was eligible to contribute ≥1 pair of TSH measurements (maximum pairs = 29) to the analyses, depending on the number and results of serum TSH levels recorded. Subjects with a history of hypothyroidism, hyperthyroidism, thyroid surgery, thyroid cancer, radioactive iodine treatment, use of thyroid hormone or anti-thyroid medications, and use of other medications that may alter serum thyroid function were excluded (Supplementary Table S1). Pregnancy was not considered exclusionary owing to its potentially incomplete capture in the dataset. Data were also extracted and cross-referenced against the Veterans Affairs (VA) Observation Medical Partnership Database 14 to increase the capture of non-VA medications and electronic medical records that may not be present in CDW. 15 The flow of study sample selection is given in Supplementary Figure S1.
Exposure and outcome ascertainment
Iodine exposure was determined using International Classification of Diseases, Ninth Revision (ICD-9) and ICD-10 codes of radiologic procedures requiring iodinated contrast media (Supplementary Table S2). We extracted TSH pairs, characterized by a normal baseline TSH followed by a subsequent TSH at least 30 days later and up to one year. Each patient could contribute multiple TSH pairs, but any individual with an abnormal serum TSH following iodine exposure was then censored from the ability to contribute any subsequent available TSH values (Fig. 1). The primary outcome was serum thyroid dysfunction, as defined by an abnormal TSH following a normal baseline TSH within one year (each VHA site has its own site-specific TSH reference range used to classify values as normal or abnormal). Secondary analyses were performed to stratify the subtypes of thyroid dysfunction (overt hypothyroidism, subclinical hypothyroidism, overt hyperthyroidism, and subclinical hyperthyroidism), according to reference VA site-specific serum peripheral thyroid hormone (thyroxine [T4] and triiodothyronine [T3]) levels available ≤90 days after an abnormal TSH result.

Extraction of TSH pairs using four patient examples. TSH pairs were defined by any normal baseline TSH and a subsequent TSH within one year. As given in the examples in this figure, each patient can have ≥1 TSH pairs based on the number of TSH measurements and incident thyroid dysfunction. For Patient A, one pair was extracted because they had one follow-up TSH measurement within a year. For Patient B, two pairs were extracted, and the second pair had an event (i.e., thyroid dysfunction) under the absence of iodine contrast exposure. For Patient C, two pairs were also extracted, and the second pair had an event under the presence of iodine contrast exposure. For Patient D, one pair was extracted of the two possible follow-up TSH measurements within a year, as the first pair had an event. TSH, thyrotropin.
Covariates
Covariates included sex, race/ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, and non-Hispanic other races), age at baseline TSH, duration between the baseline and the subsequent TSH (30–89, 90–179, 180–269, 270–365 days), and estimated glomerular filtration rate (eGFR) at baseline TSH 16 as calculated using the most recent blood urea nitrogen, serum creatinine, and serum albumin measurements 3 months before the baseline TSH and until the subsequent TSH.
Statistical analyses
Summary statistics were generated to describe the study cohort. To estimate the adjusted odds ratio (OR) or relative risk ratio (RRR) with 95% confidence interval (CI) of the association between iodinated contrast exposure and incident thyroid dysfunction (including all subtypes of overt and subclinical thyroid dysfunction), we used multivariable binary and polytomous logistic regression models using generalized estimating equations. This flexible statistical modeling allowed us to account for the correlation of responses (i.e., repeated measures) within each individual. 17 The model covariates included sex, race/ethnicity, age, and baseline TSH (Model 1). In Model 2, we additionally included the duration between the baseline and subsequent serum TSH (our primary model).
We computed the E-value to identify the minimum strength of the association between an unmeasured confounder and both the treatment and the outcome, conditional on the measured covariates, to explain away the observed association between iodinated contrast use and increased risk of thyroid dysfunction. 18 To provide the absolute risks based on the regression models, we also predicted the adjusted probability of the outcomes in each exposure group using the marginal standardization form of predictive margins (i.e., fixing individual characteristics at each level of the categories and averaged over our national sample). 19
To evaluate the heterogeneity in the association by demographic characteristics, we also stratified the analyses by sex (male, female), age (<65 years, ≥65 years), and race/ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, and non-Hispanic others). In these stratified analyses, we combined subclinical and overt thyroid dysfunction (i.e., hypothyroidism and hyperthyroidism) to ensure a sufficient number of events in each analysis.
We also conducted the following four sensitivity analyses. First, given the relationship of renal function with urinary iodine excretion and therefore thyroid dysfunction, we further adjusted for calculated eGFR among patients with available component data (n = 4,333,072 pairs [50%]; mean ± SD = 72.3 ± 19.1 mL·min−1/1.73 m2). Second, to assess whether the association differs by the duration between iodine exposure and thyroid hormone measurement, we reanalyzed the data using the two shorter thresholds of the duration (i.e., up to 3 months and up to 6 months) instead of 12 months defined in our main analysis. Third, to minimize the influence of multiple iodine contrast exposures within a short time frame, we reanalyzed the data restricting samples to the first TSH pair for each individual (i.e., only one TSH pair per person). Finally, we reanalyzed the data further excluding the participants with other drugs that might alter thyroid function (i.e., multikinase inhibitors, immune checkpoint inhibitors, and immunomodulators) and those with eGFR <30 mL·min−1/1.73 m2 who are not generally recommended to receive iodinated contrast media.
Statistical significance was defined as two-sided α < 0.05. All analyses were performed with SAS version 9.4 (SAS Institute, Inc., Cary, NC). The study was approved by the Veterans Affairs Greater Los Angeles Healthcare System Institutional Review Board.
Results
There were N = 4,253,119 patients (mean ± SD age at baseline TSH measurement is 63.5 ± 14.3 years; 92.9% men, 65.6% non-Hispanic White) in the study to provide 8,729,155 pairs of serum TSH (mean number of pairs of TSH measurements per patient is 2.1; Table 1), from which 499,681 pairs of TSH had intervening iodine exposure (iodine received at 145.6 ± 94.4 days [mean ± SD] from the baseline TSH) (Supplementary Fig. S1).
Demographic Characteristics of the Study Cohort
This was calculated among TSH pairs with intervening iodine contrast exposure.
TSH, thyrotropin.
Following a normal baseline serum TSH, thyroid dysfunction developed within one year in 4.8% of those pairs who had received iodine contrast, compared with 3.6% in those who had not. In our primary analysis using a generalized estimating equation model, iodinated contrast use was associated with an increased risk of thyroid dysfunction (adjusted OR = 1.39, 95% CI = 1.37–1.41, p < 0.001) (Table 2; Model 1). The increased risk of iodine-induced thyroid dysfunction remained significant (OR = 1.38, 95% CI = 1.36–1.40, p < 0.001) after additionally adjusting for the duration between the baseline and subsequent serum TSH (Table 2; Model 2). The predictive probabilities of thyroid dysfunction among iodine exposed group and unexposed group were 4.6% and 3.4%, respectively (Supplementary Table S3).
Associations of Iodinated Contrast Exposure and Risk of Thyroid Dysfunction
A TSH pair was defined as a normal baseline TSH followed by a subsequent TSH within one year. Each patient could have had ≥2 TSH pairs.
Multivariable binominal and polytomous logistic regression models using generalized estimating equations were used to account for the correlations between repeated measures within each patient (i.e., adjusting for time-invariant individual-level characteristics). Model 1 included sex, race/ethnicity, age, and baseline TSH within each TSH pair.
Model 2 additionally included the duration between the baseline serum TSH and subsequent TSH following iodine exposure (our primary model).
E-value represents the minimum strength of association of an unmeasured confounder with both the treatment and outcome, conditional on the measured covariates, to explain away the observed associations between iodinated contrast use and thyroid dysfunction. Numbers in the parenthesis represent the E-value for the lower bound of 95% CI.
Secondary outcomes were defined based on the reference VA site-specific serum peripheral thyroid hormone T4 and T3 levels among patients with T4 and T3 available ≤90 days after a TSH result.
CI, confidence interval; T3, triiodothyronine; T4, thyroxine; VA, Veterans Affairs.
For the secondary outcomes, iodinated contrast use was associated with increased risk of all types of serum thyroid dysfunction: overt hypothyroidism, RRR = 1.71, 95% CI = 1.56–1.89, p < 0.001; subclinical hypothyroidism, RRR = 1.40, 95% CI = 1.35–1.45, p < 0.001; overt hyperthyroidism, RRR = 1.65, 95% CI = 1.40–1.95, p < 0.001; and subclinical hyperthyroidism, RRR = 1.71, 95% CI = 1.64–1.79, p < 0.001 (Table 2). Examination of the E-value showed that an unmeasured confounder would need to be associated with both the iodinated contrast use and incident thyroid dysfunction with an OR (or RRR) >2.0, conditional on measured covariates, to explain away the observed association.
In the stratified analyses, the association between iodinated contrast use and increased risk of overall thyroid dysfunction was stronger among older Veterans (age ≥65 years, OR = 1.44, 95% CI = 1.41–1.47; age <65 years, OR = 1.37, 95% CI = 1.34–1.40; p-value for the interaction between age and thyroid dysfunction is 0.049) and men (men: OR = 1.42, 95% CI = 1.40–1.44; women: OR = 1.16, 95% CI = 1.11–1.21; p-value for the interaction between sex and thyroid dysfunction is <0.001; Fig. 2). The age difference was most prominent for hyperthyroidism (age ≥65 years, RRR = 2.04, 95% CI = 1.90–2.18; age <65 years, RRR = 1.53, 95% CI = 1.46–1.62; p-value for the interaction between age and hyperthyroidism is <0.001; Fig. 3).

Association of iodinated contrast exposure and risk of overall thyroid dysfunction by age, sex, and race/ethnicity. Multivariable binary logistic regression models using a generalized estimating equation approach and adjusted for sex, race/ethnicity, age, baseline TSH within each TSH pair, and the duration between the baseline serum TSH and subsequent TSH following iodine exposure. OR, odds ratio.
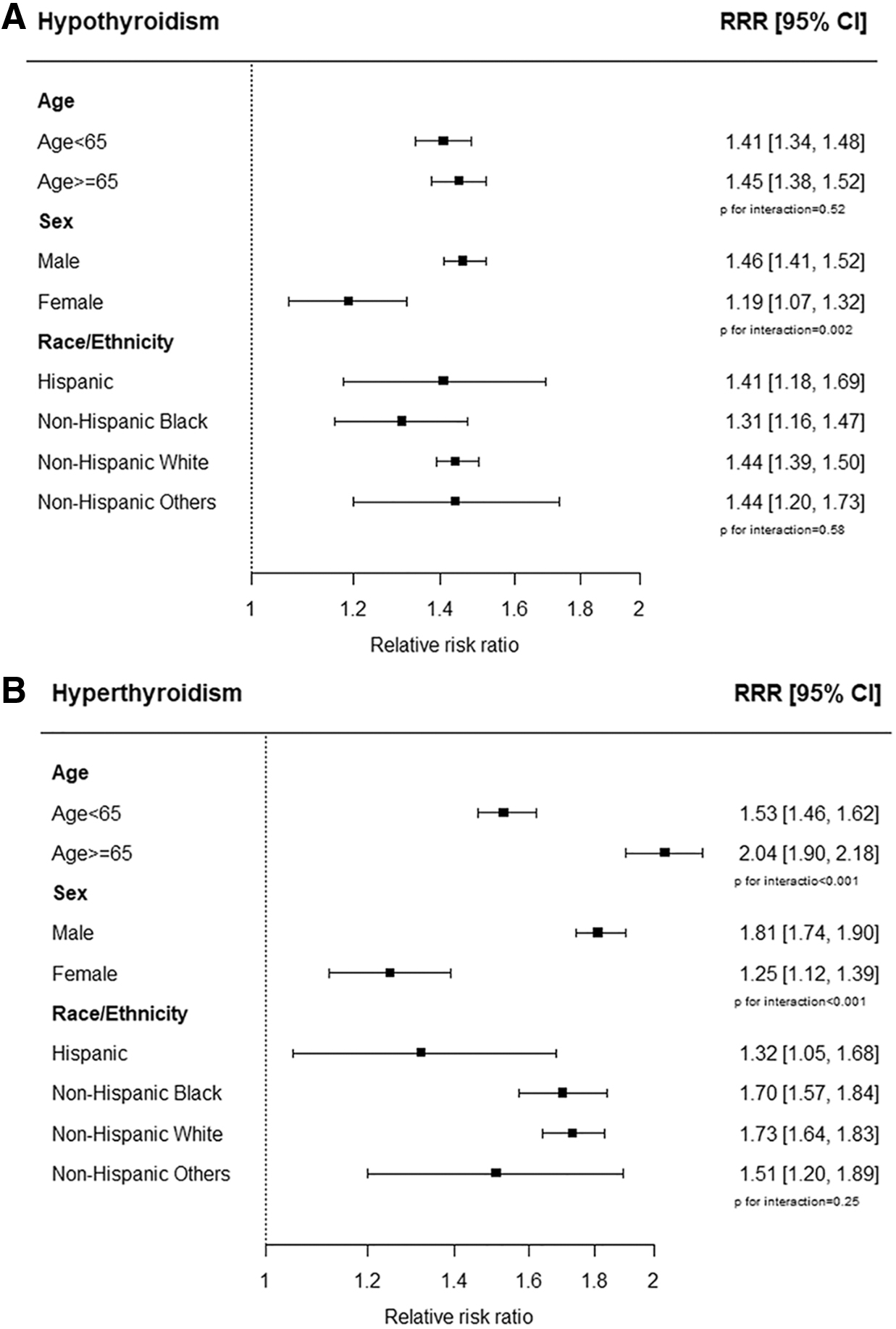
Association of iodinated contrast exposure and risk of hypothyroidism and hyperthyroidism by age, sex, and race/ethnicity. Hypothyroidism included both subclinical or overt hypothyroidism, and hyperthyroidism included both subclinical or overt hyperthyroidism. Multivariable polytomous logistic regression models using a generalized estimating equation approach and adjusted for sex, race/ethnicity, age, baseline TSH within each TSH pair, and the duration between the baseline serum TSH and subsequent TSH following iodine exposure. RRR, relative risk ratio.
The sex difference was observed for both hypothyroidism (men: RRR = 1.46, 95% CI = 1.41–1.52; women: RRR = 1.19, 95% CI = 1.07–1.32; p-value for the interaction between sex and hypothyroidism is 0.002; Fig. 3A) and hyperthyroidism (men: RRR = 1.81, 95% CI = 1.74–1.90; women: RRR = 1.25, 95% CI = 1.12–1.39; p-value for the interaction between sex and hyperthyroidism is 0.001; Fig. 3B). Although there was a lower OR for overall thyroid dysfunction among Hispanic individuals than other race/ethnicity groups, such heterogeneity across race/ethnicity was not observed in the association between iodinated contrast use and increased risk of hypothyroidism and hyperthyroidism (Fig. 3).
These findings remained consistent in our sensitivity analyses: (i) after adjustment for eGFR (Supplementary Table S4), (ii) using two shorter thresholds of the duration between iodine exposure and thyroid hormone measurement (i.e., up to 3 months and up to 6 months from iodine exposure; Supplementary Table S5), (iii) restricting samples to only the first TSH pair for each individual (Supplementary Table S6), and (iv) excluding samples with multikinase inhibitors, immune checkpoint inhibitors, and immunomodulators, and those with eGFR <30 mL·min−1/1.73 m2 (Supplementary Table S7).
Discussion
Findings from this study of the largest integrated health care system in the United States showed that iodinated contrast media exposure was associated with only a clinically small absolute increased risk of incident thyroid dysfunction. In this cohort of primarily older non-Hispanic White men, risks were highest in male Veterans. Although the difference in the overall risk of iodine-induced thyroid dysfunction was clinically small between sex, older Veterans were more likely to develop hyperthyroidism after the iodine exposure than younger Veterans. Given that radiologic iodine contrast is necessary for diagnosis and follow-up of several diseases, our findings suggest that monitoring thyroid function following its administration may be beneficial only in those at highest risk.
These data add to previous observational studies underscoring the risks of iodine-induced hypothyroidism and hyperthyroidism, disorders that have a reported prevalence ranging from 1% to 15% and are highest in regions of endemic iodine deficiency. 20 A recent systematic review and meta-analysis of 29 included studies between 1946 and 2018 showed that the risk of iodine-induced hyperthyroidism is extremely low (0.1%; 95% CI = 0–0.6%). 21 However, to date, a nationwide population-level assessment of the associations between iodine exposure and thyroid dysfunction has not previously been performed in the United States.
One of the largest studies in the United States was a case–control study of medical records from two hospitals in Boston over a 20-year period. 22 In that study, Rhee et al reported that patients without preexisting known hypothyroidism or hyperthyroidism had two- to three-fold increased risks of developing either incident hyperthyroidism (including overt hyperthyroidism) or overt hypothyroidism at a median of 9 months following iodinated contrast administration, compared with patients who did not receive the high iodine load. Similar studies have replicated these associations following iodinated contrast administration in a large community-based Boston area health maintenance organization, 23 an institutional study in Italy of patients who underwent coronary angiography, 24 in children younger than age 4 years in northern California, 25 and in our study of Los Angeles area children younger than age 18 years. 26
In the general adult population of Taiwan, patients with iodinated contrast exposure similarly had a significantly increased risk of developing thyroid dysfunction (hazard ratio [HR] = 1.46; 95% CI = 1.29–1.66). 27 In their subgroup analyses, both the risks for incident hyperthyroidism (HR = 1.22; 95% CI = 1.04–1.44) and hypothyroidism (HR = 2.00; 95% CI = 1.65–2.44) were increased even after adjusting for age, sex, urbanization, Charlson comorbidity index, use of medications that can alter thyroid function, diabetes mellitus, rheumatoid arthritis, depression, chronic kidney disease, anemia, Sjogren's syndrome, and systemic lupus erythematosus. 27 Similar findings were also reported in a subsequent nationwide study of patients with nodular goiter from the Taiwan National Health Insurance Research Database. 28
The European Thyroid Association advocates for an individualized approach to the prevention and treatment of iodine-induced thyroid dysfunction, based on a patient's age, clinical symptoms, the presence of any preexisting thyroid diseases, coexisting morbidities, and iodine intake. 20,29 The Contrast Media Safety Committee of the European Society of Urogenital Radiology recommends that only high-risk patients be monitored for thyroid dysfunction following iodinated contrast use, 29 guidance that may not necessarily be generalizeable owing to the historically iodine deficient status of many European countries. 30 In the United States, the Food and Drug Administration recently issued guidance that newborns and children up to age 3 years should universally be assessed for thyroid dysfunction within 3 weeks of iodine contrast exposure, 31 recommendations that have been controversial and may require further supporting data. 32
At present, there are no clinical recommendations for the screening or follow-up of at-risk adults receiving an acute iodine load (such as that delivered via iodinated contrast media) in the United States, but the American Thyroid Association has advised that iodine supplements containing >500 μg iodine per daily dose be avoided, 33 in alignment with the U.S. Institute of Medicine's Tolerable Upper Limit for iodine set at 1100 μg/day. 34 We believe that the findings from this study inform the gaps in knowledge on this topic, and reassuringly affirm that large-scale population thyroid function screening is likely to be beneficial in only targeted high-risk groups.
Strengths of this study include its large sample size and use of a highly detailed demographic, medical/surgical, laboratory, radiologic, and pharmacy database. The VHA is the largest integrated health care system in the United States. Iodinated contrast use is commonly used for radiologic procedures among Veterans 35,36 and thyroid disorders, including thyroid nodules, thyroiditis, hypothyroidism, and hyperthyroidism were commonly seen in a study of nearly 4.5 million Veterans. 37 The large sample size of VHA data allowed us to evaluate the heterogeneity in the association between iodine exposure and incident thyroid disorders by age, sex, and race. In a stratified analysis, we found a higher magnitude of the association among men than women. While this might be partially owing to the difference in the baseline prevalence of thyroid disorders between sex, further molecular and epidemiological studies are needed to elucidate the underlying mechanisms of potential sex heterogeneity.
There are some limitations of our study. First, owing to the nature of observational studies, our findings contained unmeasured confounding and lack of information regarding severity and duration of thyroid dysfunction. However, our sensitivity analysis employing the E-value assessment indicated that unmeasured confounders would need to be reasonably associated with the outcome (OR >2.0) to explain away the observed association. Moreover, repeated measurements of individual-level data resulted in our use of generalized estimating equation models to take into account unmeasured time-invariant individual characteristics. Second, there are potential misclassifications owing to miscoding of inclusion and exclusion criteria and of procedural iodine use that are inherent in any database analysis.
The inability to have excluded pregnancy in the dataset is also inconsequential, given the predominantly older male composition of our study sample. Although individuals with underlying thyroid dysregulation, such as those with autoimmune thyroid disease, are at increased risk of iodine-induced thyroid dysfunction, 5 serum thyroid antibody data were available in only 10,334 (0.0002%) subjects, in part owing to their known higher prevalence among women, 38 and thus were not included in the analyses of this predominantly (92.9%) male population. We also could not exclude the possibility that nonthyroidal illness might influence serum thyroid hormone levels among critically ill patients. However, we had already excluded discordant TSH and peripheral thyroid hormone levels when the latter were available, and most importantly, the results of all the secondary outcomes (i.e., when overt or subclinical thyroid dysfunction could be analyzed from available serum T3 and T4 levels) remained consistent with the primary models.
The relative higher prevalence of overall thyroid dysfunction (4.61%) [our primary outcome], and the cumulative prevalence of overt and subclinical hypo- and hyperthyroidism (0.647%) [our secondary outcomes], may in part reflect the resolving nature of a type of nonthyroidal illness, in which the abnormal serum TSH initially observed after iodine exposure is further characterized by available serum T3 and T4 levels queried up to 60 days after the abnormal TSH. Finally, because this study was based on a cohort of primarily older non-Hispanic White men, these results may potentially not be extended to other populations. Further prospective studies including non-VA populations would be needed to validate our findings and establish the causality. Although the use of any iodinated contrast dose confers several hundredfold the daily iodine requirements for normal thyroid hormone synthesis, additional research may also examine the potential dose–response of these associations.
In summary, these findings suggest that excess iodine exposure in routine clinical settings represents a potentially modifiable risk, and the risks of thyroid dysfunction and its associated comorbidities should be weighed against the need for iodinated contrast use that is commonly obtained. Furthermore, should radiologic iodine contrast use be necessary, serum thyroid function should be selectively monitored in the one year following its administration among highly susceptible patients, particularly men.
Footnotes
Authors' Contributions
K.I.: conceptualization, methodology, writing (initial draft, review, editing); R.G.: formal analysis, writing (review, editing); M.L.L.: methodology, writing (review, editing); R.E.: writing (review, editing); N.V.N.: writing (review, editing); J.W.C.: writing (review, editing); M.T.B.: writing (review, editing); A.M.L.: conceptualization, writing (initial draft, review, editing).
Author Disclosure Statement
None of the authors have any relevant disclosures.
Funding Information
This work was supported by Merit Review Award 5|01CX0011845 (AML) from the U.S. Department of Veterans Affairs Clinical Sciences Research and Development Service. No funding was received by K.I., R.G., M.L.L., R.E., N.V.N, J.W.C., and M.T.B.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Figure S1