
Abstract
Background:
When the antithyroid drugs were discovered in the early 1940s, they were immediately recognized as a revolutionary new treatment for hyperthyroidism. Although much has been learned about their mechanism of action and clinical utility, they continue to be used today in much the same way as they have been since their introduction.
Summary:
In 1995, Dr. Clark Sawin gave an address on the history of antithyroid drug development at the 11th International Thyroid Congress in Toronto, Ontario, Canada. In his review, Dr. Sawin recounted the original observations by Drs. Julia and Cosmo Mackenzie and Curt Richter at the Johns Hopkins University School of Medicine, and how their work ultimately led to Dr. Edwin (Ted) B. Astwood's seminal 1943 report on the use of thiourea and thiouracil in the Journal of the American Medical Association. He also described the development of propylthiouracil and methimazole as less toxic alternatives. He concluded his remarks by noting the often-serendipitous pathway of drug development and the role of pharmaceutical companies in the process.
Conclusions:
Antithyroid drugs remain a cornerstone of thyroid therapeutics. It is informative to review the process by which they came into use, as this is a seminal part of the history of thyroid disease in the 20th century. This knowledge may also spark additional research leading to new pharmacotherapies for patients with hyperthyroidism.
Introductory Note by David S. Cooper
Clark T. Sawin, MD (Fig. 1), was a Boston native, graduating from Brandeis University in 1954 and from Tufts University School of Medicine in 1958. He completed a fellowship in Endocrinology at the Tufts New England Medical Center Hospitals in Boston, under the direction of Edwin (Ted) Bennett Astwood, MD, the father of antithyroid drug therapy. Dr. Sawin was a Professor Medicine at Tufts University School of Medicine and Boston University School of Medicine. During his productive clinical research career, he made many important contributions to thyroidology, particularly in the areas of subclinical thyroid dysfunction and thyroid disease in older persons. In 1998, he moved from Boston to Washington, DC where he served in The Office of the Medical Inspector, Veterans Health Administration, Department of Veteran's Affairs, leading efforts to improve veterans' endocrine care, especially in the realm of diabetes.
Clark T. Sawin, MD (May 23, 1934 to August 11, 2004) (with permission from Ms. Leslie Sawin).
However, medical history was his passion, with a special interest in the history of Endocrinology. He initiated the “Historical Vignette” lecture series at the annual meetings of the American Thyroid Association, a tradition that continues to this day. At the time of his death in 2004, Dr. Sawin was the President of the American Thyroid Association. After his death, to continue Dr. Sawin's work in Endocrinology history, his family established the Clark T. Sawin History Resource Center at the American Thyroid Association and the Clark T. Sawin Memorial Library and Resource Center at The Endocrine Society.
Dr. Sawin had been one of my mentors when I was a student at Tufts Medical School in the early 1970s, and we became good friends. He presented a lecture on the history of antithyroid drug development on September 13, 1995 at the 11th International Thyroid Congress in Toronto, Canada. At my request, he sent me a typed copy of his lecture in 1996, which I have had in my files for the last 26 years. The lecture, which follows, was written to be delivered orally by Dr. Sawin, and has never been published. Some of the content is based on a brief history of Dr. Astwood's work that Dr. Sawin published in 1993. 1 The address was meant to be heard rather than read, and I have edited the typescript to be more appropriate for print media, and I have added photos of the individuals discussed in the lecture and a few editorial comments. Dr. Sawin's original lecture notes did not include a bibliography, and I have taken the liberty of adding one based on my knowledge of the literature on antithyroid drugs. I hope that all of these efforts would meet with Dr. Sawin's approval.
The Origin of Antithyroid Drugs by Clark T. Sawin, MD
In 1944 the world was in turmoil. War was prevalent and caused many to leave their homes—and it was to get worse until it ended in 1945. But my story today is not of the second World War, but of another event that spanned the same years, 1941 to 1945. And that is the discovery and development of antithyroid drugs for the treatment of hyperthyroidism.
In 1941, Elmer V. McCollum had been the Chairman of biochemistry at Johns Hopkins' School of Hygiene and Public Health for more than 20 years. He was widely recognized as the foremost nutritional biochemist of his time. In his laboratory were two young married investigators, Julia Frances (nee Buzz) (Fig. 2) and Cosmo Glenn Mackenzie (Fig. 3). * Julia had a BA from Colorado College and a nursing degree from Johns Hopkins School of Nursing. Cosmo had a BA degree from Johns Hopkins, and both subsequently earned DSc degrees from Johns Hopkins. Both were Assistant Professors of biochemistry, and both were experts in vitamin E and the effects of its deficiency in rabbits. In mid-1941, in an attempt to make rats deficient in this vitamin as well, they administered a new sulfa drug, sulfaguanidine, to alter the bacterial flora in the gut. Not much happened to the rats' nutritional state but, to her great surprise, Julia found huge thyroid glands in the rats at autopsy. Rather than discard the rats or ignore the whole experiment as an anomaly, they set out to explain this peculiar finding.

Julia B. Mackenzie, ScD (April 1911 to November 1, 1999) (provided by Dr. Julia Mackenzie).

Cosmo G. Mackenzie, ScD (May 22, 1907 to October 24, 1999) (provided by the Alan Mason Chesney Medical Archives of the Johns Hopkins Medical Institutions).
The rats' thyroids were microscopically hyperplastic, so the Mackenzies took the histologic slides to Dr. Arnold Rich, the well-known pathologist at Johns Hopkins (e.g., acute interstitial pneumonia [the Hamman-Rich syndrome] was partly named after him), who immediately diagnosed hyperthyroidism (at the time, hyperplasia was often considered synonymous with hyperfunction and excessive hormonal secretion). The Mackenzies demurred because the rats showed no outward signs to suggest thyroid overactivity. Rich also told them that Curt Richter, a behavioral scientist in the Johns Hopkins' Psychiatry department, had recently shown him quite similar slides from rats who had been given phenylthiourea as part of taste preference experiments designed to develop more effective rat poisons. The Mackenzies met with Richter to discuss the problem. Richter later noted the phenylthiourea-induced goiter in passing in a short article on gray hair in rats in December, 1941. 2 He did not pursue the problem, as his main interest was in rat behavior and, later, in how to kill rats roaming the streets of Baltimore. †
The Mackenzies published their initial findings in November, 1941, 3 and continued to seek an explanation for why their rats developed goiters. They recognized the decidedly unusual nature of the goiter—it was caused by a specific chemical and, in contrast to other experimental goiters, it occurred despite the presence of sufficient iodine in the rats' diets. Finally, they were concerned about the millions of patients already being treated with sulfa drugs. ‡
By the end of December, 1941, they had written an abstract for the forthcoming April, 1942, American Federation for Clinical Research (AFCR) meeting in Boston, in which they showed that several sulfa drugs caused goiters in rats, as did thiourea itself (Fig. 4). By April, when Julia presented the abstract, they were able to show that these drugs caused the rats' basal metabolic rate (BMR) to decrease rather than increase, thus excluding hyperthyroidism. They also showed that the drugs did not block thyroxine's (T4s) effect on the BMR, thus excluding a peripheral effect. She proposed that the drugs probably decreased thyroid hormone formation and that this led to goiter by increasing pituitary function. At the end of her talk, Edwin (Ted) B. Astwood commented that he had confirmed that sulfaguanidine caused goiter in rats, and agreed with the Mackenzies' findings.
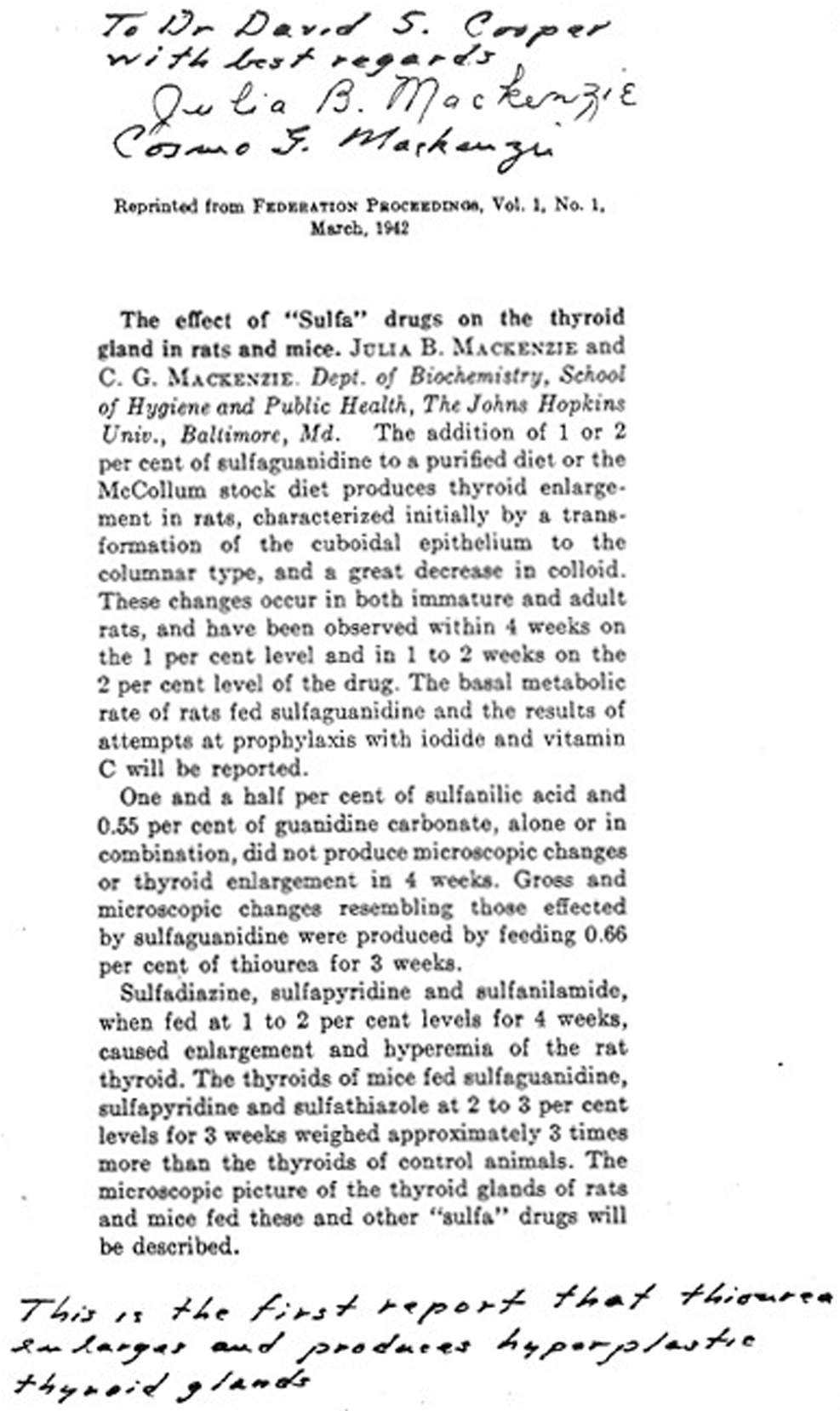
Abstract from the 1942 American Federation for Clinical Research meeting, provided to the author (D.S.C) by Drs. Mackenzie in 1983.
Ted Astwood was a rising star in American Endocrinology (Fig. 5). He had trained at McGill (where he earned his MD degree), at Johns Hopkins (where he completed a gynecologic endocrinology fellowship studying hormonal control of mammary gland development), and at Harvard (earning a PhD in Pharmacology). Astwood had known the Mackenzies for several years, having met them in the mid-1930s during his fellowship at Johns Hopkins. In 1942 at age 32, he was on the staff at Boston's Peter Bent Brigham Hospital and an Assistant Professor of Pharmacotherapy at Harvard Medical School, where he was studying the effects of adrenocorticotropic hormone (ACTH) in hypophysectomized rats; he was also the Editor-in-Chief of the journal, Endocrinology.

Edwin B. Astwood (December 29, 1909 to February 17, 1976) in 1954 when he received the Lasker Award (with permission of the Lasker Foundation).
Although he presented two articles on ACTH at that 1942 AFCR meeting, he immediately stopped most of his work on ACTH in December, 1941, after he learned of the Mackenzies' work at a Harvard Medical School seminar. Until that time he had never done any work related to the thyroid gland, but he subsequently shifted his efforts mainly to studying the thyroid; in fact, he later received permission to divert his National Research Council grant of $2500 from studying ACTH to explaining the drug-induced rat goiters that had been described by the Mackenzies. His rationale was twofold: first, he wanted to explain the underlying mechanism, and second, when it became fairly clear that the goiter was due to blockade of thyroid hormone synthesis, because it might be a therapy for hyperthyroidism. It is of interest that just after that AFCR meeting in April of 1942, Cosmo Mackenzie was asked by a science journalist if he would say that thiourea might be a treatment for hyperthyroidism. He declined, stating that there was no evidence for this in humans.
By October of 1942, both the Mackenzies and Astwood had concluded that sulfaguanidine did indeed most likely block thyroid hormone synthesis. Their articles were essentially contemporaneous and were published, back-to-back in February, 1943, in the same issue of Endocrinology, with the Mackenzies' article placed first (by Editor-in-Chief Astwood). 4,5 Publication was delayed somewhat because Astwood was waiting for the Mackenzies' article. He had been encouraging them to submit it for several months, but writing it was difficult for them because Cosmo, who had enlisted in 1941, was now a member of the United States Army Air Forces studying high altitude physiology.
Both articles took a truly modern approach; that is, they embraced the concept that the thyroid gland fed back on the pituitary to inhibit its secretion, an idea then not universally accepted. Both articles showed that these drugs caused goiter despite adequate amounts of dietary iodine, that they decreased the BMR, that they did not block the metabolic effects of T4, and that both thyroid hormone and hypophysectomy prevented the drugs from causing goiter, and thus, the pituitary was needed for the effect. Both concluded by inference, as none of the data gave direct proof, that the drugs probably acted directly on the thyroid gland to block thyroid function, and that the goiter occurred because of increased pituitary thyrotropin (TSH) secretion.
In March, 1942, Astwood had decided to study thiourea as a potential treatment for hyperthyroidism. First, he took one dose himself, without anything terrible happening; then, he gave it to a few patients without hyperthyroidism and to a few patients with hyperthyroidism. Absolutely nothing happened. Finally, in July 1942, he gave thiourea to one hyperthyroid patient for a long enough time, namely, more than for a few days, and the patient improved remarkably. At the same time he was also studying dozens of synthetic thiourea analogs in collaboration with Richard Roblin of the American Cyanamid/Lederle company. They found a less toxic drug which did not cause the terrible breath odor imparted by thiourea. Astwood gave large doses of this new drug, thiouracil, to two more hyperthyroid patients in October and December, 1942. The first patient receiving thiourea developed a rash, and one of the thiouracil-treated patients developed agranulocytosis, but all survived and all became euthyroid.
The report of these three patients, published in JAMA on May 8, 1943, was a landmark. 6,7 While investigators in New Zealand were on the same track and had proposed a clinical trial of thiourea in April, 1943 (summarized in Hercus 8 ), Astwood had provided for the first time a consistently effective medical therapy for hyperthyroidism. The efficacy was rapidly confirmed both in Boston 9 and Europe. 10 Astwood also found that overtreatment could cause severe hypothyroidism and, because a few patients stopped the drug when they felt better, he serendipitously found that some patients remained in remission with no further treatment. 11
Still, the toxic effects of thiouracil were worrisome. A trial with thiobarbital was disastrous; it turned out to be more toxic than any of the other compounds that had been tested. 12 In 1945, Astwood and Vanderlaan had moved from Harvard to Tufts University Medical School. By late 1945, their team had studied a total of 315 different compounds, 13 most made by the American Cynamid/Lederle company, and found among a series of thiouracil derivatives an effective compound which had fewer side effects. This compound, 6-n-propylthiouracil (PTU), remains to this day the major antithyroid drug used in the United States, although methimazole, also discovered by Stanley and Astwood, 14 and the methimazole prodrug, carbimazole, are also widely used. § Thiouracil was approved by the FDA in 1946 but was withdrawn from the market by the drug companies when PTU was approved by the FDA in 1947.
Concluding remarks
What I have given you is only a sketch of the whole story. Nevertheless, some points of interest are: This successful therapy was devised without understanding the precise intracellular mechanism of the drugs' action, without knowing their pharmacokinetics, without knowing the etiology of hyperthyroidism, and without any hormonal assays in either the rats or the patients. Still, physiologic understanding of the thyroid-pituitary feedback system was a major underpinning to the success of this work, even though it turned out that excessive TSH was not the cause of hyperthyroidism. Nevertheless, as Astwood himself said in 1945: “…the development was by no means a simple process but one marked by many unprofitable detours.” It was ever thus in science and medicine. Note that the work was all done before the National Science Foundation existed and before the explosive growth of the NIH. Were it not for private contributions to the National Research Council and separate support from the Rockefeller Foundation, it is unlikely the Mackenzies or Astwood would have done what they did. Further, this successful therapy would not have come when it did were it not for a close collaboration of the investigators with an interested pharmaceutical company, which in this case occurred without any patents or ownership in the company accruing to the investigators.
Finally, it is worth noting that Astwood always acknowledged the Mackenzies as having started him on his way.
Afterword by David S. Cooper
Astwood continued to make important observations related to antithyroid drug therapy (he coined the term “antithyroid compound” 11 ), including the seminal concept of remission after discontinuation of antithyroid drug therapy, 15 a phenomenon also observed earlier by Williams et al. 16 Astwood also documented the use of antithyroid drugs in pregnancy 17 and continued his work on these compounds into the 1960s. 18 His fervent hope was that drug therapy for Graves' disease would eventually replace radioiodine and surgery as treatments, and stated at the end of his Harvey Lecture in 1945: “When means are found to prevent the occurrence of toxic reactions from antithyroid drugs, or when a compound is discovered which does not give rise to side effects, then it will be possible to treat all cases of hyperthyroidism by medical means”. 11
In recognition of his work with antithyroid drugs, Astwood received the prestigious Lasker Award in 1954 and the Koch medal from the Endocrine Society in 1967. Astwood retired from his academic position at Tufts Medical School in 1972 and returned to his native Bermuda to practice general internal medicine until his death in 1976. An appreciation of Astwood's contributions and his philosophy of life can be found in a tribute by one of his most esteemed fellows, Dr. Jerome Hershman. 19
Cosmo Mackenzie did not pursue thyroid research after World War II. In 1950, he became Professor of Biochemistry and Chairman of the Department of Biochemistry at the University of Colorado School of Medicine. He was elected a Fellow of the New York Academy of Sciences and of the American Association for the Advancement of Sciences. He served as editor for the Journal of Nutrition and the Proceedings of the Society for Experimental Biology and Medicine. He died in 1999 at the age of 92. Dr. Julia Mackenzie became Professor of Biochemistry and Professor of Anatomy at the University of Colorado School of Medicine and worked with her husband in a variety of areas, including vitamin E biochemistry and lipid metabolism in cultured mammalian cells. She also died in 1999.
Final thoughts
The thionamide antithyroid drugs are among a group of compounds, such as lidocaine, phenobarbital, thiazides, and penicillin, that are still important therapies today, despite having been developed 75–100 years ago. It is interesting and perhaps surprising that there is still much to learn about the antithyroid drugs, including the optimal duration of therapy, management of side effects, and their optimal use in pregnancy. The timeline in Box 1 reviews the story of the antithyroid drugs from the original observations in the early 1940s over the last 7 decades to new data from the 21st century.
Timeline of Important Discoveries and Clinical Uses Related to the Thionamide Antithyroid Drugs
This is not a complete list of references, and I regret that space limitations prevent an exhaustive bibliography.
ATD, antithyroid drug; PTU, 6-n-propylthiouracil; T4, thyroxine; TSH, thyrotropin.
Researchers are exploring new therapies for Graves' disease, which are directed at the underlying pathophysiology: an immune dysregulation leading to the presence of stimulating antibodies directed at the thyrocyte TSH receptor. 20 While these exciting potential treatments represent the future, it is hard to imagine a scenario in which the thionamide antithyroid drugs will not be used to treat thyrotoxicosis, at least as initial therapy, while awaiting the salutary effects of more specific treatments.
Footnotes
Acknowledgments
I would like to thank Ms. Leslie Sawin, Dr. Sawin's wife, for granting permission for me to publish Dr. Sawin's lecture; I also would like to thank the Lasker Foundation for permission to publish Dr. Astwood's photograph; Mr. Timothy Wisniewski of the Alan Mason Chesney Medical Archives of the Johns Hopkins Medical Institutions for providing the photograph of Dr. Cosmo Mackenzie; and Mr. Thomas Sherlock and the University of Colorado Medical Center for his assistance in providing historical information about the Mackenzies.
Authors' Contributions
David S. Cooper is responsible for writing the commentary and background information regarding Dr. Sawin and his lecture, as well as the brief history of events occurring in the years after the development of antithyroid drugs. Clark T. Sawin wrote the text of the lecture that he delivered in 1995 to the International Thyroid Congress.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.