
Abstract
Purpose:
Disparities in the diagnosis and treatment of patients with differentiated thyroid cancer (DTC) have been described. This review includes the most recent literature on existing diagnostic and treatment disparities in the United States and proposes practical clinical and policy ideas for improving the gap in the treatment of DTC.
Methodology:
We performed a comprehensive literature review to include key articles related to DTC and disparities of treatment, diagnosis, and outcomes for disadvantaged patient populations.
Results:
Vulnerable patient populations with DTC have been extensively studied, and the literature shows that clear disparities of diagnosis and treatment exist. Socioeconomically disadvantaged patients, uninsured, rural, elderly, and patients belonging to minoritized racial and ethnic groups are more likely to present with advanced disease at presentation. These same vulnerable patient populations are less likely to have access to high-volume surgeons, less likely to be treated according to guidelines, and receive less aggressive treatment (such as radioactive iodine) compared with white patients. Further, these patients experience financial toxicity more so than their counterparts.
Conclusions:
Disparities of care exist for certain vulnerable patient populations with DTC. Approaches to rectify these should be multipronged and involve improving access to high-volume specialists with ongoing use of telehealth consults, language concordant care, an emphasis on guideline-directed therapies, ensuring continuity of care and long-term follow-up with better community partnerships, engage diverse patients in national guideline-writing committees of prominent societies and reducing the financial burden of cancer treatments at the state and national policy level.
Introduction
Differentiated thyroid cancers (DTC) are relatively indolent and more often surgically curable than most other solid tumors. 1 In fact, many argue that in wealthy nations such as the United States, patients with these tumors are overtreated, leading to reduced quality of life without any survival benefit. 2 –4 Thus, the treatment of DTC is a nuanced balance between identifying more aggressive disease before it becomes incurable, and avoiding overtreatment of indolent tumors. 5
Further, many of these patients require multidisciplinary approaches, including surgery, adjuvant treatments such as radioactive iodine (RAI), and lifelong surveillance for recurrence. Therefore, DTC patients may be particularly vulnerable to disparities in both access to care—which may paradoxically result in overdiagnosis and overtreatment of advantaged groups and underdiagnosis and undertreatment of vulnerable populations—and differences in utilization of care, leading to inadequate treatment for patients with aggressive disease.
Interest in studying health care disparities has grown within the thyroidology community along with increasing awareness of the harm caused by these discrepancies in care. The National Institute on Minority Health and Health Disparities (NIMHD) defines health care disparities as differences that affect disadvantaged populations, resulting in higher population incidence and/or prevalence of a given disease or its risk factors; higher rates of disease symptoms or reduced daily functioning; premature or excessive mortality; or greater burden of disease within a given population. 6 In particular, much recent research pertaining to disparities in care for patients with thyroid disease has focused on the disparities in the diagnosis, treatment, and outcomes of patients with thyroid cancer. 7
Health Care Disparities and Incidence of Thyroid Cancer
Several studies have identified access to health care, often mediated by insurance coverage, as a direct correlate of thyroid cancer incidence. 8,9 Harari et al studied the California Cancer registry and found that patients with lower socioeconomic status, particularly Black patients, had more advanced disease at diagnosis than their wealthy white counterparts. 10 A similar pattern was identified in the National Cancer Database; uninsured and socioeconomically disadvantaged patients had higher rates of extrathyroidal extension, lymphovascular invasion, distant metastases, and positive margins after surgery than patients with private insurance. 11
In a separate analysis, these authors also showed that thyroid cancer incidence was strongly correlated with the percentage of the population that was insured on a state-by-state basis; the more insured people in a state, the higher the incidence of thyroid cancer. 11 These disparities may exist even down to the individual hospital level. One study of two affiliated hospitals in New York City found that patients treated at a private university hospital were nearly twice as likely to have DTC detected by imaging as patients at a public hospital. 12
Importantly, discrepancies in incidence are not entirely explained by insurance status alone. Perhaps unsurprisingly, the incidence of thyroid cancer in Canada also seems to be correlated with access to care, despite universal health coverage. 13 Two Canadian studies also found that socioeconomically disadvantaged and rural patients were more likely to have advanced thyroid cancer at diagnosis. 13,14 In the United States, patients living in rural areas are also less likely to be diagnosed with thyroid cancer than urban counterparts. 15 The authors of these studies note that other barriers, such as availability of transportation and distance to the nearest health care facility, possible individual mistrust in the health care system, and competing life priorities based on socioeconomic factors, are likely major contributors to access to care.
Limited English language proficiency and health care literacy also have a significant impact on access to care, in turn reducing the odds that a patient may be diagnosed with thyroid cancer. Limited English proficiency increases the likelihood that patients do not have a primary care provider and have not had a preventative visit in the previous year. 16 Further, in the United States, there is significant variability in the availability of interpreter services to help reduce the obstacles that non-English speakers face when seeking care. 17 For example, in one study of Hispanic women diagnosed with thyroid cancer, those with lower English proficiency were less likely to report that they had adequate access to information about thyroid cancer. 18
Therefore, it is likely that socioeconomic status, rural location, distance from the nearest health care facility, English proficiency, health care literacy, and insurance status all play a role in the likelihood of a given patient being diagnosed with DTC.
Disparities in Extent of Treatment for DTCs
These same factors—socioeconomic and insurance status, race, and ethnicity—are also all associated with the extent of treatment for DTC patients. Patients who are uninsured or under-insured are less likely to be treated with total thyroidectomy, formal lymphadenectomy, and adjuvant RAI than patients with private insurance. In fact, with regards to adjuvant RAI, these disparities increase with the increasing stage of disease. 11 Lower socioeconomic status and education level are also directly correlated with lower likelihood of adjuvant RAI treatment. 19
Likewise, these factors may contribute to the financial toxicity associated with thyroid cancer treatment. A study of patients in the North American Thyroid Cancer Survivorship Study found that female sex, low income, low education level, and treatment in the United States (as opposed to Canada) were all independently associated with financial toxicity as measured by the COST-PRO score. 20 Chen et al used the Los Angeles Surveillance Epidemiology and End Results (SEER) database and their own survey data to study financial toxicity among Hispanic women with thyroid cancer.
They included 273 patients who completed their survey (an 80% response rate); they found that more than 30% of them reported being at least “a little” or “somewhat” worse-off financially following their diagnosis, and nearly 40% had to use personal savings to pay for their care. 21
Financial toxicity disproportionately impacts all thyroid cancer patients. 22 Fenn et al found that more than 30% of patients with thyroid cancer reported “a lot” of financial problems following their diagnoses, more than patients with breast, lung, colorectal, ovarian, and other cancers. 23 Paradoxically, this disproportionate degree of financial toxicity relative to other solid tumors may be due to the indolent disease course and subsequent need for long-term surveillance and follow-up. This may explain why patients with thyroid cancer had quality-of-life scores similar to others with more aggressive types of cancer, and worse than those with breast cancer. 24
Ramsey et al from the University of Washington used the Western Washington SEER Cancer Registry to determine the rates of bankruptcy among patients with a variety of cancer types. They found that in a propensity-matched model, thyroid cancer patients had a rate of filing for bankruptcy protection that was similar to other cancers in the model other than lung cancer; ∼40% of patients who ultimately filed for bankruptcy did so in the first 5 years after diagnosis. Younger age, female sex, locoregional or advanced disease, and non-white race were all independently associated with an increased likelihood of becoming bankrupt following a cancer diagnosis. 25
Perhaps most concerning, however, is that disadvantaged patients are more likely to receive care that is inconsistent with major professional society guidelines. Wenaas et al studied nearly 2500 patients with AJCC stage III or IV thyroid cancer from the SEER database to assess compliance with the 2006 American Thyroid Association (ATA) guidelines. Specifically, they considered less than near-total thyroidectomy, no lymphadenectomy, and no adjuvant RAI to be non-compliant treatment.
They found that Black patients, those older than 65 years of age, and patients with lower income or who were single were less likely to be treated in accordance with the ATA guidelines. 26 Subsequently, Shah et al performed a much larger scale analysis of the National Cancer Database, including more than 250,000 patients with any stage thyroid cancer, and found that Black patients were less likely to undergo an appropriate extent of thyroidectomy, again according to ATA guidelines. They also found that Black, Asian, and Hispanic patients were less likely to be treated with RAI than their white counterparts. 27
These studies demonstrate the impact that socioeconomic factors, race, and ethnicity have on the provision of care to thyroid cancer patients. Under certain circumstances, less aggressive treatment may improve outcomes given the indolent nature of most thyroid cancers. Thus, ironically, disparities in treatments may occasionally reduce overtreatment and overdiagnosis. Unfortunately, however, there are substantial data to suggest that although in some instances overtreatment may be reduced, outcomes are generally significantly worse for disadvantaged patients.
Thyroid cancer patients with low income, who are uninsured or underinsured, and who belong to minoritized racial or ethnic groups are more likely to present with advanced disease, receive less aggressive treatment that often differs from guideline recommendations, and experience subsequent financial toxicity more often than wealthy, insured, white patients. Most importantly, these translate to worse survival for some disadvantaged patients.
A recent analysis of more than 45,000 patients with thyroid cancer in the SEER database also found that after adjusting for socioeconomic, tumor, and treatment-related variables, Black patients with thyroid cancer had higher five-year mortality than white patients. 28
Disparities in Access to Expert Care for Patients with DTC
It has been well documented in the literature that disparities in access to subspecialty care are more pronounced for certain individuals who identify as racial and/or ethnic minorities across multiple medical conditions, including cardiovascular disease, diabetes, and cancer. 29 The reasons are multifactorial but these patients often have less access to preventative care, lack of insurance or the means to pay for costly procedural care (such as surgery), and lack of postoperative care/follow-up (Fig. 1).
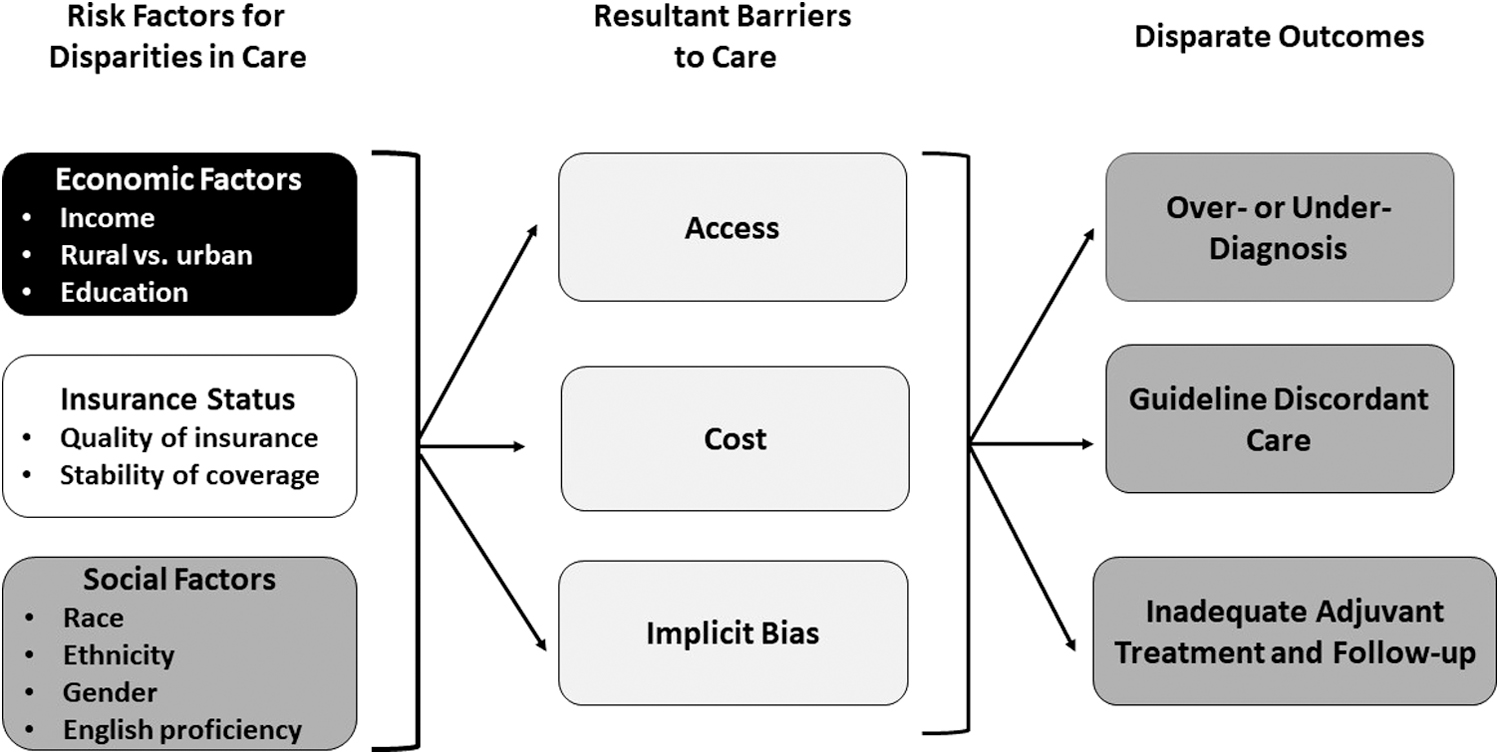
Cascading factors contributing to disparities in thyroid cancer care.
This can lead to delays in diagnosis and more advanced disease at presentation, as well as loss to long-term follow-up that prohibits appropriate treatment and surveillance. 10,11,19,21,27 Further, a recent study demonstrated that minority patients were more likely than white patients to be informed of their thyroid cancer diagnosis by their primary care provider, rather than an endocrinologist or surgeon. However, in the same study, only 66% of primary care physicians reported feeling comfortable discussing a thyroid cancer diagnosis with their patients. 30 Importantly, this may also affect referral to high-volume thyroid surgeons. 31
These disparities in access to care are relevant for racially and/or ethnically minoritized patients with DTC and are perhaps confounded by the fact that access to a high-volume thyroid surgeon leads to better overall outcomes, including fewer surgical complications and a lower postoperative mortality rate. 32 Al-Qurayshi et al studied patients undergoing thyroid or parathyroid surgery for primary malignancy and found that patients from communities with poor health indicators and those of Black and Hispanic backgrounds were more likely to be treated by low-volume surgeons, and that this group of patients also had a higher risk of postoperative complications. 33
Noureldine et al studied outcomes among more than 100,00 patients of different race and ethnicities undergoing thyroid (83%) or parathyroid (17%) surgery in the National Inpatient Sample and found that Black patients were less likely to have access to intermediate and high-volume surgeons compared with white patients, and that Hispanic patients had the least access to high-volume surgeons. Further, they calculated same-admission complications based on post-operative secondary diagnoses and procedures and found that Black patients had higher overall complications compared with white patients.
Black patients also had a longer mean length of stay, higher in-hospital mortality, and higher mean total charges 34 ; these findings are similar to the results of another study examining racial differences in clinical and economic outcomes for patients undergoing thyroidectomy. 35
Another vulnerable group of patients who have had less access to expert, high-volume care are elderly patients. In a study of the National Cancer Database encompassing >30,000 patients undergoing thyroidectomy for thyroid cancer, Youngwirth et al found that elderly (over 65 years), along with Black and uninsured patients were more likely to be treated at low-volume institutions and had higher rates of incomplete resections (such as macro- and microscopically positive margins), which were associated with compromised survival. 36
Papaleontiou et al surveyed members of the Endocrine Society, American College of Physicians, and American Academy of Family Practice with questions assessing the physicians' referral patterns in several different sample case scenarios involving elderly (>65 years old) patients. They found that among the 269 physicians surveyed (35% response-rate), endocrinology specialists and those treating >10 thyroid cancer patients per year were more likely to refer to a more distant high-volume surgeon rather than a local surgeon, regardless of patient age. 31 The clinicians cited patient preference (68%), transportation difficulties (63%), and confidence in the local surgeon (54%) as the main reasons for referring elderly patients to local surgeons rather than distant specialists.
Minding the Gap: Reducing Disparities
The reasons underlying disparities of care for underserved and vulnerable patients with DTC are complex and multifactorial. A multipronged approach is needed to improve access to care, reinforce guideline-directed therapies, and ensure stable and improved insurance coverage to increase continuity of care and reduce financial toxicity for vulnerable patient populations (Table 1).
Proposal for a Multi-Pronged Approach to Reducing Disparities in Care for Disadvantaged and Vulnerable Patients with Thyroid Cancer
Telemedicine has the potential to become a key tool to reducing disparities in thyroid cancer care. During the COVID-19 pandemic, the ability to perform virtual consultation across state lines improved access to care for underserved populations and could be a continued method of cultivating access to high-volume physicians for underserved patients and patients in rural areas. However, ensuring equity in telehealth care also requires vigilance, as disadvantaged patients may be less likely to have access to technology and/or the knowledge necessary to use it. These factors have already been suggested to exacerbate disparities in care for chronically ill patients via telehealth. 37
Fortunately, there is evidence that the expansion of telehealth services has improved access to care for some patients. In a recent study examining racial/ethnic and socioeconomic disparities using telemedicine during the pandemic, it was shown that Black patients used telemedicine more often than white patients during the second half of the pandemic. 38 Further, for patients undergoing thyroid surgery, Schumm et al found that satisfaction using telemedicine is high and equivalent to in-person visits. 39
These authors also assessed surgeon communication during visits using the Communication Assessment Tool, a post-visit patient survey instrument, and found no significant difference in patient-reported communication effectiveness between virtual and in-person visits. Telemedicine may also facilitate the use of interpreters for patients with limited English proficiency. In addition, the ability to join the visit remotely may allow other family members to participate in a thyroid cancer patient's care, reducing the effect of poor health literacy by spreading knowledge among a broader support group.
Telemedicine consults to high-volume thyroidologists and surgeons may help provide state-of-the-art recommendations, which could then be translated into practice at a more local level for easy access. Thus, the use of a telemedicine platform might be an efficient and relatively inexpensive method of improving access to care for underserved patients with DTC.
Thyroid cancer requires long-term surveillance and has a high rate of recurrence that can require serial imaging and laboratory testing, additional surgery, or other percutaneous interventional procedures. Establishing continuity with a high-volume specialist for this type of long-term surveillance can be challenging; especially without reliable, consistent, health insurance. Lack of health insurance is associated not only with advanced disease at diagnosis, but also with less aggressive treatment after diagnosis and guideline discordant care. Thus, any approaches to reduce disparities in thyroid cancer care that do not broaden access to stable, affordable health insurance are unlikely to be successful.
Expanding access to insurance alone is necessary but not sufficient to address the financial toxicity caused by thyroid cancer care. Travel expenses, time off work, child- or eldercare are just a few of the costly impediments for patients to easily reach the necessary treatment centers, appointments, etc. These real-life concerns are currently rarely covered or supplemented by any insurance and have associated high out-of-pocket expenses that can be insurmountable for certain patients.
Although medical-related costs can be tax deductible, they are only so once they exceed 7.5% of annual gross income. 40 Certain insurances such as Medi-Cal do pay for medical and non-medical travel expenses for low-income patients; however, there are a limited number of patients who may qualify for such benefits. 41 Better policies around patient-centered coverage for cancer care will specifically need to be implemented to allow for more equitable health care for most patients.
Finally, numerous studies have shown an independent effect of patient race and ethnicity on treatment and outcomes for thyroid cancer patients. Sadly, this reflects persistent systemic racial bias in medicine. These innate biases may be more subtle and more difficult to directly address than other sources of health care disparities but are no less important. Increasing emphasis on diversifying the medical field may help to alleviate the problem through increased representation in the long term.
Promoting community relations between health care professionals and vulnerable communities by establishing language and race/ethnicity-concordant affordable health programs may also help provide more culturally competent, grass-roots care.
Highlighting racial and ethnic disparities may inspire self-reflection and reduce implicit bias for health professionals. New training programs, such as the Cultural Complication Curriculum developed at the University of Michigan and the Anti-Oppressive Curriculum at the University of California San Francisco, have great potential to educate medical trainees, faculty, and staff about their own biases and how to overcome them. 42,43
In addition, we strongly advocate for emphasis on guideline-directed care, independent of patient race or ethnicity, to standardize treatments and reduce subjective decision making that may perpetuate these disparities. National professional guideline-writing committees, such as the American Thyroid Association, may be able to include diverse patients who can bring their lived experiences and help guidelines be encompassing of vulnerable patients and communities.
Minority groups are also frequently under-represented in clinical trials. 44,45 Strikingly, a recent analysis of 230 cancer clinical trials between 2008 and 2018 showed that representation for Black and Hispanic patients reflected only 22% and 44% of expected participation based on cancer incidence. 44 Representation did not change over the study period. Significant efforts are needed to address these disparities in cancer trial representation to ensure that treatments offered are effective and safe for all patients. Participation in clinical trials also offers the potential for increased access to affordable care as well, as both treatment and follow-up are typically provided at no cost to participants.
Finally, all researchers and publishers should be held to higher standards in dealing with race and racism in scholarly work. Boyd et al wrote easy-to-follow standards for scientific writing, which included naming race specifically in study design; naming racism specifically as a risk factor; never offering genetic interpretations of race in studies; and citing experts of color, among others. 46
Conclusion
Disparities of care have been shown to exist for disadvantaged and underserved patients with DTC, which leads to worse outcomes for this patient population. The solution to this problem should be multidimensional and involve improving access to high-volume specialists, emphasis on guideline-directed therapies, community engagement, ensuring continuity of care and long-term follow-up, and reducing the financial burden of cancer treatments.
Footnotes
Authors' Contributions
S.D.: has made a substantial contribution to the acquisition and analysis of the data presented, drafting of the article, and approved the version to be published concept or design of the article. T.M.U.: has made a substantial contribution to the acquisition and analysis of the data presented, drafting of the article, and approved the version to be published. S.R.: has made substantial contribution to the conceptual design, data analysis, editing and revision of the article, and approved the version to be published. The authors have agreed to be accountable for all aspects of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.