
Abstract
Background:
Several toxicities are recorded during treatment of advanced thyroid cancer (TC) with antiangiogenic drugs, including lenvatinib (LEN). Hypocalcemia was reported in registration studies, but little data are available from real-life cohorts. The aim of our study was to describe the incidence, characteristics, and the management of hypocalcemia in patients on LEN treatment.
Methods:
This is a retrospective cohort study of consecutive patients with advanced TC, treated with LEN for at least six months at a single tertiary center in Italy. Phosphocalcic metabolism was evaluated during treatment.
Results:
We included 25 patients treated for a mean of 29 ± 19 months (range 6–68 months). Hypocalcemia occurred in 6 of the 25 patients (24% [95% confidence interval 9.36–45.13%]), being of grade ≥3 in 2 of the 25 patients (8%), and recurrent in 4 of 6 patients (67%). The median time to hypocalcemia onset was 3 months (range 0.5–13 months) from starting LEN. No differences were found between patients who developed or not hypocalcemia regarding either starting/mean dose of LEN or clinicopathological characteristics. During the hypocalcemic crisis, the 2 patients with grade ≥3 hypocalcemia had low magnesium and low or inappropriately normal parathormone (PTH) levels, while 2 of 3 patients with grade 2 hypocalcemia had a secondary hyperparathyroidism. Hypocalcemia was managed with calcium oral supplementation in most cases, although up to 10% of patients required intravenous calcium treatment and transient LEN withdrawal.
Conclusions:
In this relatively small cohort, we observed an incidence of hypocalcemia of 24%, which is higher than that reported in the registration trial (6.9%). Both PTH-dependent and PTH-independent mechanisms explained hypocalcemia in the present cohort. Monitoring of serum calcium levels is strongly advised during the first year of LEN treatment, as hypocalcemia may be severe. More research is needed to confirm our findings and inform possible risk factors for hypocalcemia in advanced TC patients treated with LEN.
Introduction
Patients with progressive radioactive iodine (RAI)-refractory thyroid cancer (TC), in whom local treatment is not feasible, may undergo systemic therapy with tyrosine kinase inhibitors (TKIs). TKIs are directed against multiple targets 1,2 or single specific targets, such as dabrafenib and trametinib (targeting BRAF and MEK), larotrectinib and entrectinib (targeting NTRK fusions), and selpercatinib (a RET kinase inhibitor). 3
Three antiangiogenic drugs are currently used for the treatment of progressive RAI-refractory TC: lenvatinib (LEN), sorafenib, and cabozantinib, the latter only as a second-line treatment. Multikinase inhibitors (MKIs) should be administered lifelong, until evidence of progression. 1 In the phase III trials, these drugs were shown to prolong progression-free survival (PFS) and improve response rate but were affected by several and various toxicities. In particular, the SELECT study showed a median PFS of 18.3 months versus 3.6 months, with an objective response rate of 65%. 4
Importantly, almost all patients reported at least one adverse event (AE), the majority had a transient LEN interruption and a dose reduction, and around 15% of patients discontinued the treatment. Among various toxicities, hypocalcemia was reported in 6.9% of patients taking LEN, and it was responsible for dose adjustment in four patients (1.5%). 4 Hypocalcemia was reported also in the COSMIC-3115 and in the DECISION 6 trials being reported in 23% and 19% of patients treated with cabozantinib and sorafenib, respectively. However, only few real-life studies evaluated this specific MKI side effect. 7 –9
The aim of our study was to report the incidence of hypocalcemia in a real-life setting of LEN treatment for TC. Other objectives were to describe the characteristics and treatment of hypocalcemia. We explored the potential underlying etiological mechanisms of hypocalcemia in this clinical setting.
Materials and Methods
Patients
This is a retrospective cohort study. We evaluated consecutive patients with progressive, locally advanced, or metastatic differentiated TC who received LEN treatment during the period July 2016–April 2022 and were followed up at our tertiary center in Italy. Patients were included if sequential data on the calcium–phosphorus metabolism were available (Supplementary Fig. S1). Only 1 patient was excluded due to lack of biochemical data (deceased after 45 days of treatment). Among the 25 included patients, all but 3 underwent total thyroidectomy, with or without lymphadenectomy, and RAI treatment and were RAI-refractory with progressive disease at the time of LEN initiation. Among the remaining 3 patients, 2 underwent lobectomy and/or debulking surgery due to neoplastic infiltration of contiguous organs, while 1 patient refused to be operated on. Tumors were staged according to the eighth edition of TNM staging. 10 The functional status of patients was assessed by the ECOG performance status scale. 11
The study was performed in accordance with the ethical standards of the Institutional Research Committee and with the 1964 Declaration of Helsinki. All patients were enrolled in a protocol approved by the ethical committee of the Istituto Auxologico Italiano and provided informed consent to the use of their anonymized clinical data for research purposes (study code approval: 2022_03_08_03).
Biochemical and bone mineral density evaluations
Serum Ca levels were corrected for albumin according to the formula: corrected Ca (cCa) = [0.02 × (normal albumin − patient's albumin)] + serum Ca levels. Blood examinations along with serum Ca evaluation were performed every 2–3 months. Serum Ca was measured using Cobas c-701/702 system (Roche Diagnostics GmbH, Mannheim, Germany). Serum albumin, phosphorous, magnesium, creatinine, and alkaline phosphatases were measured by standard techniques. Serum intact parathormone (PTH) levels were measured using the Elecsys Roche (Cobas e-801) electrochemiluminescence assay (Roche Diagnostics GmbH) (reference interval 1.38–6.79 pmol/L).
Bone mineral density (BMD) was evaluated in 16 patients (9 females, 8 of whom menopausal, and 7 males) by dual-energy X-ray absorptiometry (GE Lunar Prodigy, GE Healthcare Lunar or Hologic Horizon, Hologic Corp., Bedford, MA) at lumbar spine, total femur, and femoral neck and expressed as standard deviation units in relation to the young (T-score) and age-matched (Z-score) reference healthy population. In 7 women and in 1 man, the BMD evaluation was performed before the start of LEN; in 7 men and 1 woman, the BMD was evaluated during LEN treatment. Vitamin D levels were measured at baseline, and patients with vitamin D levels <75 nmol/L were supplemented with cholecalciferol.
Adverse events
AEs were recorded on Electronic Hospital Records and were classified according to the Common Terminology Criteria for Adverse Events version 5.0. 12 In particular, grade 1 and grade 2 hypocalcemia was defined by serum cCa ranges of 2.00 to 2.02 mmol/L and 1.75 to <2.00 mmol/L, respectively; grade 3 by serum cCa of 1.50 to <1.75 mmol/L or hospitalization requirement; grade 4 by serum cCa <1.50 mmol/L or complication with life-threatening symptoms.
Statistical analyses
We described quantitative data as mean ± standard deviation (SD), and median with range, depending on normality of distribution (as evaluated by the Shapiro–Wilk test). Categorical variables were expressed by the absolute number and percentage. The incidence and 95% confidence interval [CI] were estimated using the Clopper and Pearson method. Statistical group comparisons were performed using the Mann–Whitney U test and Student's t test for respective nonparametric and parametric continuous variables. Categorical variables were compared using the χ 2 test or the Fisher's exact test. We defined the p-value for statistical significance as <0.05. All statistical analyses were performed using MedCalc Statistical Software version 19.2.0 (MedCalc Software bvba, Ostend, Belgium).
Results
Clinical features of the cohort and incidence of hypocalcemia
The baseline characteristics of the 25 patients are summarized in Table 1. Most patients were treated by total thyroidectomy, 2 patients had lobectomy, and 1 patient was not submitted to surgery. Postsurgical hypoparathyroidism was recorded in 3 of the 24 patients submitted to surgery (12.5%). The prevalent histotype was papillary (50%), follicular tumors were the 37.5%, and poorly differentiated cases were the 12.5% of cases. Most patients had stage I or II TC as assessed by the eighth edition of the AJCC Cancer Staging Manual (35% and 50%, respectively) at initial diagnosis.
Clinical Characteristics of the Cohort (N = 25) at the Time of the Start of Lenvatinib Treatment
One patient not submitted to surgery not calculated.
LEN, lenvatinib; mets, metastases; SD, standard deviation; TKI, tyrosine kinase inhibitor.
Locoregional and/or distant metastases to the lung and/or bone were detected in 80% and 76% of cases, respectively, either at diagnosis and/or during the follow-up. The majority of patients had an ECOG status 0 or 1 (60% and 32%, respectively), being ECOG 2 the 8% of cases. The mean LEN initial dose was of 16.9 mg (range 4–24 mg), and all the included patients received this treatment for at least 6 months and for a mean ± SD of 29 ± 19.9 months (range 6–68 months). Hypocalcemia occurred in 6 of the 25 patients, corresponding to an incidence of 24% [CI 9.36–45.13%], and it was of grade ≥3 in 2 of the 25 patients (8%). The median time to hypocalcemia occurrence after LEN start was of 3 months (mean 5 months and range 0.5–13 months).
Comparison between patients who developed or not hypocalcemia
In hypocalcemic patients, cCa levels recorded during the follow-up widely fluctuated within the normal range, frequently dropping below the lower limit, while in eucalcemic patients, they were more stable and always in the normal range (Fig. 1). We evaluated the clinical characteristics of the patients who developed hypocalcemia during LEN treatment in comparison to those who remained eucalcemic during treatment (Table 2). No significant differences were found among the two groups in terms of clinical features, such as gender (female patients 50% vs. 57.9% in hypocalcemic and eucalcemic groups, respectively), and age at initial surgery (60.7 years vs. 58.1 years).
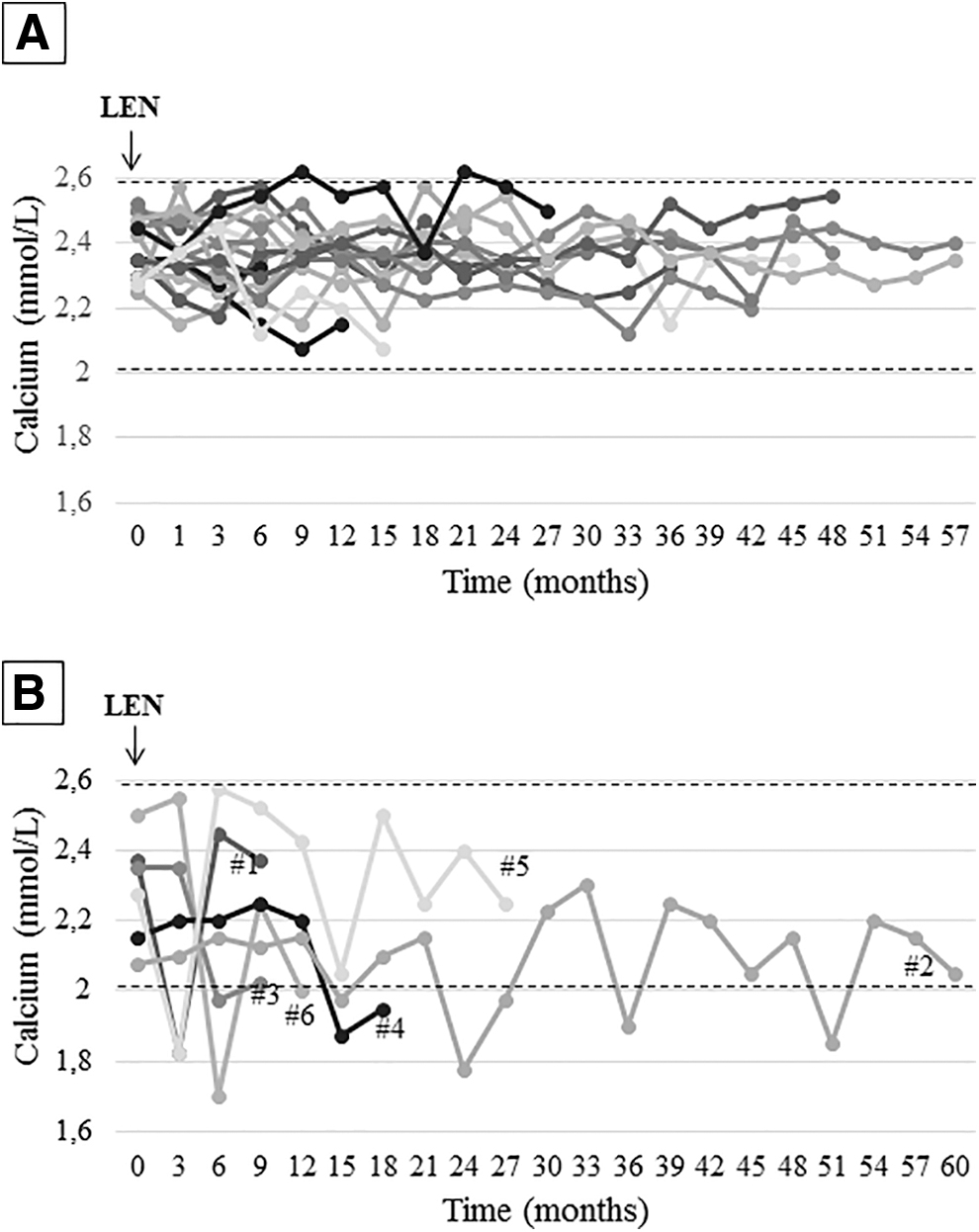
Calcium levels (corrected for albumin, cCa) at baseline and during LEN treatment in eucalcemic cases (
Comparison of the Clinical Characteristics of Hypocalcemic and Eucalcemic Patients
One patient not submitted to surgery not calculated.
Papillary histotype was more frequent in the group of patients who had hypocalcemia (83.3% vs. 38.9%), although the difference was not statistically significant (p = 0.09). No significant differences were observed for patients with hypocalcemia compared with those with no hypocalcemia regarding the age at start of LEN treatment (70.4 years vs. 66.5 years), the starting dose (17.7 mg/day vs. 16.6 mg/day), the mean dose of LEN treatment (14 mg/day vs. 13.5 mg/day), and the duration of LEN treatment: 23 ± 20.7 (range 6–60) months versus 31 ± 19.7 (range 6–68) months.
Factors potentially contributing to the development of hypocalcemia tended to be more frequent in the hypocalcemic group. In particular, diarrhea, vomiting/nausea, and weight loss tended to be more frequent in the hypocalcemic group (100% vs. 78.9%, 33.3% vs. 26.3%, and 83.3% vs. 47.3%, respectively). The number of patients who had a central neck dissection (60% vs. 30.8%), the presence of postsurgical hypoparathyroidism (16.7% vs. 11.1%), previous treatment with calcium before starting LEN (33.3% vs. 26.3%), and the presence of bone metastases at the time of LEN initiation (33.3% vs. 21.1%) also tended to be more frequent in patients with hypocalcemia compared with those who did not have hypocalcemia. However, none of the risk factors were statistically significantly different between the groups (Table 2).
A BMD evaluation was available in 16 patients (9 female, 8 of whom menopausal, and 7 male): osteoporosis was reported in 3 of 4 (75%) patients who experienced at least one episode of hypocalcemia and in 4 of 12 (33.3%) patients in the other group (Table 2). Three of these 16 patients had bone metastases, and osteoporosis was documented in 2 of them. Importantly, bisphosphonates or denosumab were given, concomitantly to LEN, in 2 of 6 patients who developed hypocalcemia and in 1 of 19 eucalcemic patients (33.3% vs. 5%).
Characteristics and management of hypocalcemia
Hypocalcemia was of grade 3 in 2 of 6 cases, who transiently interrupted LEN and were treated with intravenous Ca treatment, with normalization of serum Ca levels. The 4 patients with grade 2 hypocalcemia received oral Ca supplementation and one of them withdrew LEN for other concomitant AEs.
The biochemical evaluation recorded at each hypocalcemic episode is reported in Table 3. In the 6 patients, serum PTH levels ranged between 1.34 and 10.33 pmol/L (n.r. 1.38–6.79). Among cases with a CTCAE grade 3 hypocalcemia, patient 1 had inappropriately normal PTH levels (4.97 pmol/L), while patient 2 had low PTH levels (1.34 pmol/L) at the first episode and an inappropriately normal PTH level (4.19 pmol/L) at a following hypocalcemia (data not shown). This latter patient was submitted to a loboisthmectomy and a debulking intervention on the other thyroid lobe, because of massive infiltration to the striated muscles, esophagus, and vascular and lymphatic vessels, as we previously reported. 13 Among the 4 patients who developed a grade 2 hypocalcemia, 1 patient had an inappropriately normal PTH levels during hypocalcemia (3.08 pmol/L) and 2 patients had slightly high PTH levels (7.67 and 10.33 pmol/L).
Summary of the Biochemical Findings During the First Episode of Hypocalcemia
AP, alkaline phosphatase; cCa, corrected calcium; K, potassium; Mg, magnesium; P, phosphorus; PTH, parathormone.
Only patient 5 had a permanent postsurgical hypoparathyroidism, and he was on Ca replacement therapy at the time of hypocalcemia onset. Serum phosphorus, creatinine, urea, alkaline phosphatases, and potassium levels were usually normal in these patients during the hypocalcemic crises. Magnesium ranged between 0.41 and 0.91 mmol/L. It was low in the 2 patients (0.41 and 0.58 mmol/L, n.r. 0.66–1.07) who recorded grade 3 hypocalcemia and in 1 patient (0.49 mmol/L) with grade 2 hypocalcemia, while the other 3 patients had normal magnesium levels (0.70, 0.82, and 0.91 mmol/L). Four patients had recurrent hypocalcemia, despite concomitant calcium and vitamin D supplementation. All the new hypocalcemic episodes were milder compared with the first one, with the exception of that occurred in patient 6, who recorded another grade 2 hypocalcemia, but with cCa levels lower (1.88 mmol/L) than those found at the first episode (1.98 mmol/L).
Grade 3 hypocalcemia was acutely managed with intravenous calcium infusions, and then, the two patients were treated by the oral administration of a calcium carbonate dose ranging from 1 to 3 g/day, calcitriol 0.5–0.75 μg/day, and cholecalciferol 50,000 IU/month. Three of the 4 patients with grade 2 hypocalcemia received calcium carbonate 0.5–1 g/day and calcitriol 0.25–0.5 μg/day, while patient 3 withdrew LEN for other concomitant AEs and serum Ca normalized without calcium supplementation.
Discussion
In the present real-life study, a high incidence of hypocalcemia (24% [CI 9.36–45.13%]) was observed during LEN treatment, and it was grade ≥3 in 8% of patients. This incidence, although observed in a small series, is higher than that reported in the registration SELECT study, in which 6.9% and 2.7% of patients complained of all-grade and grade ≥3 hypocalcemia, respectively. 4 A lower incidence (10% and 3% all-grade and grade ≥3) was also reported in the only available real-life study reporting data on both the phosphocalcic metabolism and the incidence of hypocalcemia. 9
Differences between registration trials and real-life studies have been reported for the incidence of other AEs occurring upon MKIs treatment, 14 –17 and further, real-life studies will likely give more insights into the actual incidence of this LEN toxicity. Frequent serum calcium measurements are advised in patients on LEN treatment, as we demonstrated: (1) the cCa levels widely fluctuates within and below the normal range and this may be missed with sporadic assessments; (2) symptoms related to a mild Ca reduction may be vague and may be confused with the other AEs.
The possible causes underlying LEN-induced hypocalcemia in these patients may be PTH-dependent or PTH-independent, as summarized in Figure 2. PTH-dependent hypocalcemia may be caused by iatrogenic hypoparathyroidism or hypomagnesemia. In our series, postsurgical hypoparathyroidism was more frequent in hypocalcemic patients, although they were eucalcemic on Ca chronic treatment before starting LEN. It is thus possible to hypothesize that a postsurgical mild hypoparathyroidism leading to borderline/normal Ca and PTH levels could be perturbed by minor events (dehydration, malabsorption) leading to clinically evident hypocalcaemia.
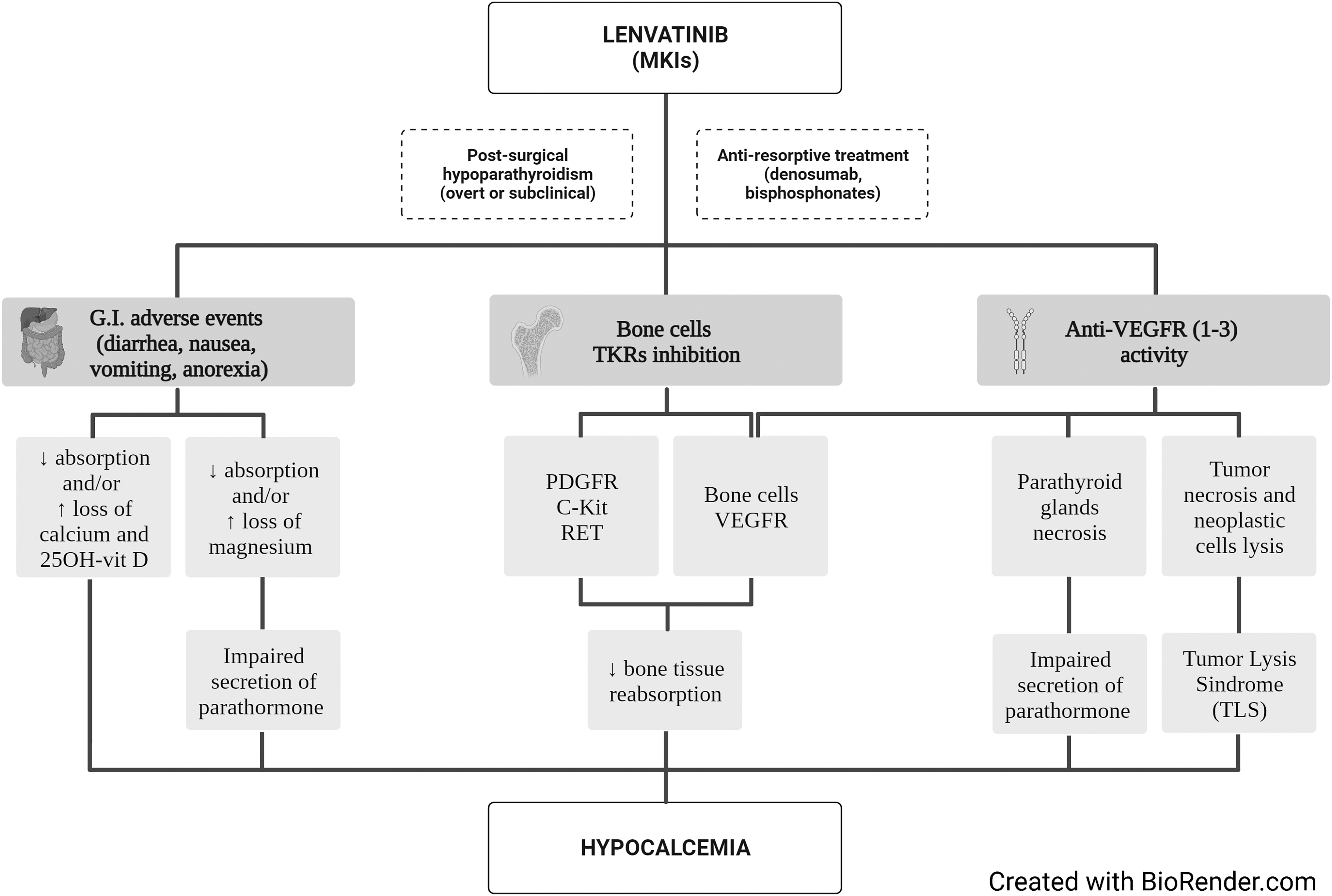
The possible mechanisms at the basis of hypocalcemia in patients with advanced thyroid cancer treated with LEN (or other multikinase inhibitors). Dashed squares indicate possible precipitating factors in patients with borderline calcium levels.
Another precipitating factor in patients with borderline/normal cCa levels could be the treatment with bisphosphonates or denosumab for osteoporosis and/or bone metastases, which was concomitant to LEN in 2 of the 6 patients who developed hypocalcemia. Concerning hypomagnesemia, the reduction of serum magnesium is known to impair PTH secretion by means of an altered stimulation of the Ca sensing receptor, thus leading to hypocalcemia. 18 Another possible cause of PTH-dependent hypocalcemia could be the direct damage of the parathyroid glands since antiangiogenetic drugs such as MKIs were already reported to significantly reduce the vasculature density in endocrine organs. 19 During hypocalcemia, the lack of a PTH increase as a response to the low Ca levels, that is, an “inappropriately” normal PTH, indicates a parathyroid impairment due to either a postsurgical hypoparathyroidism or an iatrogenic cause.
Alternatively, PTH-independent hypocalcemia may be caused by reduced absorption or increased loss of Ca and 25-OH vitamin D. 18,20 Many patients taking MKIs complain of nausea, vomiting, anorexia, and diarrhea, 4 –6 which may lead to Ca and 25-OH vitamin D malabsorption, which is the most common causes of PTH-independent hypocalcemia. 18 Another reason of PTH-independent hypocalcemia is the tumor lysis syndrome (TLS), a rare oncological emergency due to the sudden death of tumor cells and the subsequent release of several metabolites into the blood stream. Among these, the phosphate ion, whose concentration is up to four times higher in malignant than in normal cells. Hyperphosphatemia can contribute to Ca-phosphate salt formation and potentially cause secondary hypocalcemia.
Although more frequently associated with lymphomas and leukemia, TLS may also occur during systemic treatment (i.e., steroids, chemotherapy, and radiotherapy) for solid tumors 21 and has been described during sorafenib 22 and LEN 23 treatment for hepatocellular carcinoma. In our series, this condition could be excluded since the reduction of the tumor masses was slow and neither impaired renal function nor hyperkalemia and hyperuricemia, which are typical of the TLS, were recorded. Finally, MKIs act on several kinases, such as VEGF, PDGFR, c-KIT, and RET, which are also expressed by bone cells (i.e., osteoclasts and osteoblasts), and a potential off-target effect on bone metabolism and calcium levels has been reported. 24
In our cohort, different mechanisms may have contributed to hypocalcemia. The 2 patients with grade ≥3 hypocalcemia had low or inappropriately normal serum PTH levels, indicating a PTH-dependent mechanism, although we cannot exclude the contribution of PTH-independent mechanisms, in particular Ca malabsorption and hypomagnesemia because of gastrointestinal side effects. The same mechanism was likely at the basis of the grade 2 hypocalcemia recorded only two weeks after LEN start in a patient with postsurgical hypoparathyroidism, although well compensated with Ca and calcitriol. Different PTH levels were detected in the remaining 3 patients with grade 2 hypocalcemia. One of them had inappropriately normal PTH levels, while two patients had a secondary hyperparathyroidism, indicating that hypocalcemia was due to PTH-independent mechanisms
There were no significant differences to be considered as risk factors between patients who developed or did not develop hypocalcemia: the rate of postsurgical hypoparathyroidism was similar, and also age, gender, presence of bone metastases. Interestingly, the frequency of osteoporosis was higher, although not significantly, in patients who developed hypocalcemia (75% vs. 33.3%, p = 0.16). This finding did not reach the statistical significance likely due to the relatively small number of cases included but warrants further evaluation in a larger cohort to better understand the potential impact of osteoporosis on MKI-induced hypocalcemia. However, it seems reasonable to evaluate Ca-phosphorus metabolism more carefully in osteoporotic cases on LEN.
Since there was no difference neither in the LEN starting dose nor in the dose during treatment, the occurrence of hypocalcemia seems to be LEN dose-independent.
Finally, in 4 of 6 patients, hypocalcemia developed within the first three months of treatment, and in the remaining 2 cases after 1 year from the start of the TKI. This is similar to what reported for other toxicities in the SELECT study 25 and strengthen the indication to strictly follow patients treated with MKIs especially during the first six months of therapy. 2 Nevertheless, as for other AEs, hypocalcemia may recur during LEN treatment, and Ca levels should be routinely monitored during treatment.
This study has several limitations. First, this was a retrospective study, and it was subject to incomplete relevant biochemical data, such as measurements of 24-hour calcium, C-terminal telopeptide, or vitamin D. Second, the study is limited by a relatively small sample size, and group comparisons are statistically underpowered. Confirmation of our findings is needed in other similar or larger cohorts.
In conclusion, hypocalcemia may occur not infrequently early in the course of LEN treatment for advanced TC. In the present series, hypocalcemia was observed in approximately one in four patients, and this did not appear to be related to LEN dose. Both PTH-dependent and PTH-independent mechanisms were observed to explain hypocalcemia in this setting. As hypocalcemia may be a life-threatening AE, monitoring of Ca levels following the start of LEN treatment is strongly advised. We recommend specific caution during the first year of treatment and/or when concomitant precipitating factors, such as osteoporosis, antiresorptive treatments, and gastrointestinal toxicities, are present. Oral Ca supplementation may correct hypocalcemia if promptly diagnosed; however, up to 10% of patients may have a severe hypocalcemia requiring intravenous treatment and LEN transient interruption. Further studies are needed to gain more insights into the characterization of this toxicity and associated risk factors.
Footnotes
Authors' Contributions
S.D.L.: Conceptualization, data collection, formal analysis, and writing and editing. M.T. and C.M.: Data collection, formal analysis, and editing; C.C. and N.G.: Data collection and editing. L.F.: Conceptualization, supervision, and writing. All the authors were responsible for the final approval of the article.
Author Disclosure Statement
L.F. is consultant for Eisai and Ipsen; the other authors have no conflicts of interests to disclose.
Funding Information
This study was partially funded by the Italian Ministry of Health (THY-CANC ID 2.773.026).
Supplementary Material
Supplementary Figure S1