
Abstract
Iodine is an essential component of the hormones produced by the thyroid gland and is, therefore, essential for mammalian life. A landmark trial in the early 20th century definitively demonstrated that iodine supplementation could prevent what was then known as “endemic goiter.” Subsequent studies over the next decades demonstrated that iodine deficiency causes a spectrum of disease, including not just goiter, but also cretinism, intellectual impairment, and adverse obstetric outcomes. Salt iodization, first used in Switzerland and the United States in the1920s, has become the mainstay of iodine deficiency prevention efforts. The dramatic reduction in the global prevalence of iodine deficiency disorders (IDD) over the past 30 years represents an outstanding and under-recognized public health achievement. This narrative review provides an overview of critical scientific discoveries and advances in public health nutrition related to the prevention of IDD in the United States and worldwide. This review was written to commemorate the centennial of the founding of the American Thyroid Association.
Introduction
Iodine is an essential component of thyroid hormones and is essential for mammalian life. This narrative review provides an overview of critical scientific discoveries and advances in public health nutrition related to the prevention of iodine deficiency disorders (IDD) in the United States and worldwide, with a focus on the past century (Fig. 1). This review was written to commemorate the centennial of the founding of the American Thyroid Association (ATA).

A timeline of important milestones in understanding and combating the effects of iodine deficiency, 1915–2022.
Discoveries in the 19th Century
In 1811, Courtois accidentally discovered iodine while producing saltpeter for gunpowder for Napoleon's army. He added sulfuric acid to burnt seaweed ash and produced a dark violet vapor that crystallized on cold surfaces. Gay-Lussac subsequently identified it as a new element and named it “iodine,” from the Greek for violet. 1 Coindet, a Geneva physician, learned of iodine's discovery and in 1813 suggested that the historical treatment of goiter with seaweed or sponges was effective because of their iodine content. He began giving oral iodine tincture (at a starting dose of 16.5 mg/day, which is enormously supraphysiological) to patients and observed shrinking of goiters with treatment. 2
He also provoked some cases of iodine-induced thyrotoxicosis, which led to a backlash and persistent concerns that iodine treatment was inherently unsafe. 3 Boussingault, a French chemist working in South America, was the first to propose the use of iodine-containing salt to prevent goiter. 4 Chatin measured iodine in food and drinking water samples from across western Europe and concluded, in 1851, that inadequate drinking water iodine levels were the main cause of endemic goiter. 5 In response, French authorities began distributing iodine tablets and salt together with other prophylactic measures in three regions with high goiter rates. A survey of 5000 children from the region of Haute-Savoie found that this iodine treatment led to the shrinking or disappearance of 80% of goiters. 1
By the late 1800s, scientists realized that cretinism only occurred in areas of endemic goiter but were perplexed by the fact that many patients with cretinism had an atrophic or absent thyroid gland, the opposite of goiter. In 1874, Gull was the first to describe thyroid atrophy in a myxedematous patient. 6 Then, in 1878, the term “myxedema” was coined by Ord. 7 Myxedema resembled cretinism but was seen only in adults, usually women. It was characterized by slowness in thought and movement, facial swelling, and “spade-like hands with skin resembling dry leather.” Building on the work of Gull and Ord, in an 1882 address and subsequent 1883 article coauthored by his cousin, the Swiss surgeon Reverdin described the deleterious phenotype after total thyroidectomy as “myxoedème opératoire.” 8,9
In 1883, Swiss surgeon (and later Nobel laureate) Kocher described the results of 200 thyroidectomies (including 19 of the same cases reported by the Reverdins), terming post-thyroidectomy changes “cachexia strumipriva,” and noting the development of a phenotype similar to cretinism in a patient whose thyroid had been resected at age 11. 10 Semon, a British laryngologist, stated in 1883 that “there appeared to be three conditions closely allied to each other, and having in common either absence or probably complete degeneration of the thyroid body: namely, cretinism, myxoedema, and the state after total removal of the thyroid body.” 11 In response, the Clinical Society of London established a committee that concluded, in 1888, that cretinism and myxedema were due to the “the annihilation of the function of the thyroid body.” 12
In the 1890s, Portuguese and British physicians began successfully treating myxedema with animal thyroid extracts. 13 –15 In 1896, the link between goiter, myxedema, and iodine was established when Baumann and Roos in Germany analyzed animal thyroid glands and isolated a residual insoluble fraction that was ∼10% iodine. 16 They described this compound, which was effective in treating both goiter and myxedema, as “thyroiodine,” and correctly postulated that the iodine had activity only when incorporated into an organic molecule. 17
The History of Iodine Deficiency in the United States
A century ago, when the American Society for Goiter (later the ATA) was founded, endemic goiter was a substantial and highly visible public health problem in the United States. Examination of World War I military draftees demonstrated high goiter rates, particularly in the upper Northwest and Great Lakes regions, where up to 31% of candidates were disqualified from military service because their necks were too large to fit into a uniform. 18,19 Surveys carried out by the U.S. Public Health Service in the 1920s revealed goiter rates up to 70–100% in schoolchildren from parts of Minnesota, Michigan, and Wisconsin. 18 Starting in the 1920s, McClendon, a physiologist at the University of Minnesota, mapped iodine present in foods and drinking water in different regions across the United States, demonstrating that iodine intakes correlated inversely with goiter prevalence. 20
Marine and Kimball
Marine developed an interest in goiter while training as a pathologist in Cleveland, Ohio, at the U.S. “goiter belt” epicenter. Starting in 1907 he did a series of experiments in dogs, pigs, cattle, and fish demonstrating that thyroidal iodine content varied inversely with the amount of hyperplasia. 21 Between 1917 and 1920, together with medical student Kimball, Marine conducted a landmark clinical trial in adolescent girls from Akron, Ohio (Fig. 2). 22 A total of 2190 girls who were treated with 200–400 mg sodium iodide taken in drinking water for 10 days twice annually were compared with 2305 girls who declined study participation. Goiter developed or worsened in only 0.2% of treated girls compared with 14% of controls. In a 1924 Harvey lecture at the New York Academy of Medicine, Marine recommended iodized salt as the best way to prevent both endemic goiter and cretinism at the population level. 23
Several key figures in global efforts to eliminate iodine deficiency disorders. From left to right: David Marine, Oliver Perry Kimball, John Stanbury, Sir Basil Hetzel, and John Dunn. (Photos of David Marine and Oliver P. Kimball courtesy of the National Library of Medicine; photo of Sir Basil Hetzel courtesy of the Iodine Global Network).
Salt Iodization in the United States: History and Effects
Marine noted that in the decade after his Akron trial, “many kinds of iodine medication, including candies, tablets and chewing-gum, ran wild.” 21 However, ultimately it was iodized salt rather than iodized chewing gum that became the preferred intervention, largely due to the efforts of Cowie, a pediatrician and the chair of the Michigan State Medical Society. Salt is an excellent vehicle for iodine fortification because it is consumed by all population groups, most individuals ingest stable amounts of salt from day to day, and the salt iodization process is inexpensive and relatively simple to implement and monitor. 24
With guidance from Marine and Kimball, Cowie spearheaded a remarkable effort to combat iodine deficiency goiter by convening stakeholders including physicians, salt producers, and grocers. 25 In 1923, Hale, a chemist at the Dow Chemical Company in Michigan, developed the methodology for mass iodized salt production, after which, in 1924, table salt iodized at 100 mg/kg was introduced in Michigan on a voluntary basis. Cowie's group developed statewide educational campaigns to create a market for the new iodized salt. These efforts initially met with vehement opposition.
Kimball later recalled that the U.S. Food and Drug Administration “initially insisted that iodized salt cartons be labeled with a skull and crossbones because iodine is a poison” and that “the experiment was at first resisted by the goiter surgeons.” 26 However, in late 1924, the Morton Salt Company became the first U.S. producer to distribute iodized salt nationally. For the next two decades the Endemic Goiter Committee of the American Public Health Association (which included Marine and McClendon among its members) worked on public health education campaigns supporting salt iodization. 22 In 1948, the committee tried, without success, to pass U.S. legislation mandating iodized salt use. Although this effort failed in the United States it led to mandatory salt iodization in Canada.
An early effect of salt iodization was a transient rise in toxic nodular goiter incidence (similar to the thyrotoxicosis induced by Coindet's iodine treatments a century earlier). In 1926, Hartsock, a thyroid surgeon at the Cleveland Clinic and a leading opponent of salt iodization, reported cases of hyperthyroidism in men, which appeared to have been triggered by initiation of iodized salt use. 27 In 1934, McClure reported that although there had been a transient rise in goiter surgeries performed in Michigan hospitals for three years after salt iodization, there was a subsequent rapid 60% decline in goiter surgeries. 28
It has been recently estimated that from 1925 to 1942 there may have been as many as 10,000 excess deaths in the United States due to iodine-induced hyperthyroidism. 29 However, salt iodization also clearly conferred major benefits. By 1951, when Brush and Altland performed a survey of Michigan schoolchildren, the prevalence of goiter had declined from 38.6% in 1924 to only 1.4%. 30 Using military data collected during World Wars I and II to compare the cognitive ability of cohorts born before and after salt iodization, it has been estimated that for the quarter of the U.S. population most deficient in iodine this intervention raised IQ by ∼15 points. 29
The History of Salt Iodization in Switzerland
As early studies led to salt iodization in the United States, parallel efforts were taking place in Switzerland. The iodized salt program in Switzerland was established in 1922. Before its introduction, mountainous areas of Switzerland were affected by severe endemic goiter and cretinism. In 1800, a census of the Canton Valais ordered by Napoleon reported 4000 individuals with cretinism among 70,000 inhabitants. 1 In 1915, Hunziker, in Zurich, stated that goiter was an adaptation to low dietary iodine intake and suggested that small quantities of iodine added to the food supply would prevent the condition. 31 In 1918, a dose–response trial of iodine to treat goiter was done by Bayard in Grächen, a small village at the base of the famous Matterhorn mountain. For six months, Bayard gave iodized salt fortified at three different concentrations to families in the village.
He reported that as little as 30 μg/day of iodine reduced goiter and that diffuse goiters in children were more responsive than the nodular forms in adults. 32 von Fellenberg subsequently performed an iodine balance study that suggested that as little as 17 μg/day resulted in positive iodine balance. 33 Based on the data from Marine and Kimball, in 1919, Klinger recommended providing iodized salt for the general population and iodine supplements in Swiss schools. 1 The Swiss Goiter Committee was formed in 1922 in an advisory capacity to the Federal Office of Health. Iodized salt was introduced in the Appenzell region in 1922, thanks to the efforts of the surgeon Eggenberger, who successfully urged the local authorities to allow the sale of iodized salt. Within a few years after the introduction of iodized salt, newborn goiter and most childhood goiter had disappeared, and no new infants had been born with cretinism. 34
Scientific Developments from the 1940s Onward
In 1948, Wolff and Chaikoff, working at the University of California, Berkeley, first documented the homeostatic mechanism whereby a large dose of iodine transiently inhibits iodine organification in the thyroid gland. 35 Failure of the acute Wolff–Chaikoff effect may lead to iodine-induced hyperthyroidism (the Jod-Basedow phenomenon), the cause of the transient increase in rates of hyperthyroidism seen in the United States and elsewhere shortly after the initiation of salt iodization. More recent data from Denmark demonstrated that although there was a marked increase in the incidence of thyrotoxicosis after salt iodization, rates decreased to baseline by 7–8 years and after 16 years had decreased to 33% below baseline. 36
Starting in the 1950s, Stanbury (the 1969 ATA president for whom the ATA's Stanbury Thyroid Physiology Medal is named) was an important contributor to the science of iodine metabolism as well as to iodine deficiency prevention efforts (Fig. 2). He worked first at Massachusetts General Hospital and later at the Massachusetts Institute of Technology. His interest in radioisotopic studies of iodine kinetics led to him to investigate patients with inherited forms of thyroid dysfunction, including familial iodotyrosine deiodinase deficiency (the first thyroid disorder linked to a specific enzyme defect). 37
In 1952, he traveled to western Argentina to carry out the first collaborative international study of endemic goiter. 38 While working in Argentina, Stanbury used radioisotopic studies to demonstrate that there is increased thyroidal iodine avidity in iodine-deficient individuals and to confirm that the Jod-Basedow phenomenon in patients with long-standing iodine deficiency was caused by excess iodine. 39 His further studies in severely iodine-deficient populations in South America ultimately demonstrated that iodine deficiency impaired neurological development.
In 1952, the World Health Organization's Goiter Study Group (with Kimball as a member) developed a roadmap for global programs for the investigation and prevention of endemic goiter. 40 Subsequent to this effort, in 1958 Kelly and Snellen reviewed the world literature (>900 articles) and concluded that the world prevalence of endemic goiter at the time was close to 200 million (Fig. 2). 18
In the late 1960s, Hetzel, an Australian physician, performed a landmark trial in an area of severe iodine deficiency in Papua New Guinea. 41 In this study, alternate families received saline or iodized oil injection. Iodine supplementation of pregnant women resulted in a 73% reduction in the prevalence of endemic cretinism at 4 years of age. In studies by Belgian investigators performed in Zaire in the 1970s, 42 –44 pregnant women were randomized to receive iodized oil injection or a vitamin injection, and psychomotor development scores were measured in their children at about 6 years of age. There were significantly higher scores in the iodine group and far fewer children with low psychomotor scores.
In a study of iodized oil in area of severe iodine deficiency in China, participants were children from birth to 3 years and pregnant women. 45 Untreated children 1–3 years of age, who were studied when first seen, served as controls. The developmental quotient at 2 years of age was significantly higher in the offspring of the treated mothers and in the treated children, compared with the untreated children. 43 Several controlled studies of iodized oil given to pregnant women in the Andes led by Pretell and Stanbury showed similar benefits on the reduction of cretinism and goiter, and improved cognitive development in the offspring. 46 –48
In 1983, Hetzel coined the term “iodine deficiency disorders.” 49 This terminology emphasized that iodine deficiency causes a spectrum of disorders, including decreased IQ with its profound effects on social and economic development, rather than just endemic goiter or cretinism (Fig. 2). Dunn (the recipient of the ATA's 1968 Van Meter prize and 1997 Paul Starr Award) traveled with his mentor, Stanbury, to South America in the 1960s and became interested in iodine deficiency. He went on to develop methods to assess population iodine status and to control the iodine content of salt, and he became active in the development of international collaborative efforts to eliminate iodine deficiency. 50
The International Council for the Control of Iodine Deficiency Disorders (ICCIDD; now the Iodine Global Network), 51 an expert consultative group, held its inaugural meeting in 1986 in Katmandu, Nepal. Stanbury was the initial chair, Hetzel the executive director, and Dunn the Secretary (and later executive director). With funding from entities including the United Nations Children's Fund (UNICEF), the World Health Association (WHO), and U.S. Agency for International Development, ICCIDD provided technical assistance to national salt iodization programs. Largely because of advocacy from the ICCIDD and its partners, in 1990 the World Health Assembly established the elimination of IDD as a major public health goal for all countries.
Global Progress Toward Elimination of Iodine Deficiency
For the past three decades many iodized salt programs have been introduced to improve population iodine intakes. In 2022, 126 countries had legislation mandating salt iodization and another 21 had legislation allowing voluntary salt iodization. 52 UNICEF estimates that 88% of the global population currently uses iodized salt. 53 Iodine nutrition in populations is typically assessed by measuring urinary iodine concentrations (UIC) in representative cross-sectional national surveys. UIC is a good biomarker for iodine exposure because it reflects recent iodine intake from all sources (including foods such as seafood, dairy, and eggs as well as iodized salt). For the past 15 years, UIC surveys have been carried out in 152 out of 194 countries.
The number of countries with adequate iodine intake has increased from 67 in 2003 to 117 in 2022 (Fig. 3), reflecting the effectiveness of salt iodization. In contrast, excess iodine intakes have occurred in some previously iodine-deficient areas. Thirteen countries currently have excessive iodine intakes (median UIC >300 μg/L). Because a rapid increase in iodine intake may precipitate transient increase in hyperthyroidism (as seen in the United States in the 1920s), it is critical that iodized salt programs be regularly monitored to prevent both iodine deficiency and excess. 54 A modeling study recently estimated the impact of iodized salt programs: the global prevalence of clinical IDD (as assessed by the total goiter rate) fell from 13.1% to 3.2%, while IDD has been prevented in 20.5 million newborns annually. 55 The resulting improvement in cognitive development has likely provided a $33 billion global economic benefit.
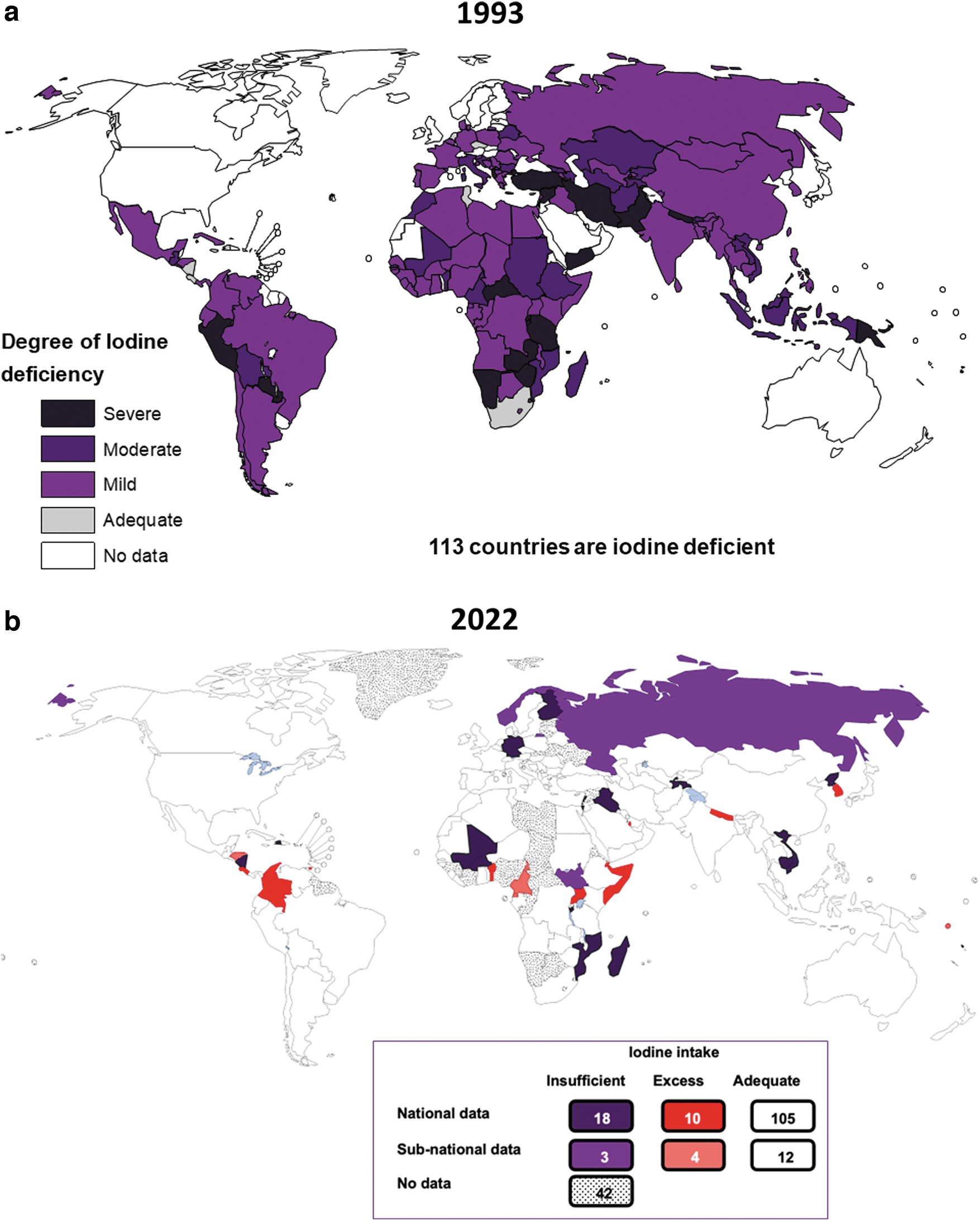
Global iodine status in 1993 (
Conclusions
Studies for the past century have demonstrated that iodine deficiency causes a spectrum of disease, including goiter, cretinism, intellectual impairment, and adverse obstetric outcomes. Salt iodization, first used in Switzerland and the United States in the 1920s, has become the mainstay of iodine deficiency prevention efforts. The dramatic global reduction in IDD over the past century represents an under-recognized public health achievement.
However, work remains to be done. In some regions there has been backsliding—once iodine sufficiency has been achieved resources are diverted to other public health priorities and gains are not sustained. Since the introduction of universal salt iodization in most countries, severe iodine deficiency has been largely eradicated worldwide, but mild to moderate iodine deficiency remains prevalent, especially in pregnant women, who are at highest risk of adverse outcomes from IDD. Future studies are needed to understand how to sustain progress and to optimize iodine nutrition for the most vulnerable population groups.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: draft article preparation by E.N.P. and M.B.Z. Both authors reviewed and approved the final version of the article.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
No funding was received for this article.